Article Text

Abstract
Objective Previous studies have suggested endothelial dysfunction in adult patients after repair of aortic coarctation (CoA). It has been proposed to play a key role in the pathogenesis of arterial hypertension in the absence of re-coarctation. We aimed to assess the presence of endothelial dysfunction, the number of endothelial progenitor cells (EPC), and the levels of proinflammatory cytokines associated with endothelial injury in contemporary patients after CoA repair.
Methods For this prospective observational study, 20 CoA patients and 22 healthy controls were recruited. Digital reactive hyperaemia was measured by peripheral arterial tonometry. Flow cytometry was used to quantify EPCs, and a comprehensive panel of laboratory markers of endothelial dysfunction was measured.
Results Half the patients had known arterial hypertension requiring medical treatment. Indices of reactive hyperaemia showed no significant difference between CoA patients (1.96±0.32) and controlss (1.765±0.48) (p=0.82). Circulating EPCs, defined by the number of CD34+, CD34+/KDR+, CD34+/AC133+, CD34+/AC133+/KDR+ or CD34+/CD45− labelled cells were equally not significantly different between the groups. Furthermore, plasma levels of inflammatory mediators and markers of endothelial function (IL-6, IL-8, ICAM1 and VCAM1) were not significantly different between the groups, as were vascular endothelial growth factor levels (p>0.05, for all).
Conclusions By contrast with earlier reports, no clinically significant difference in endothelial function between adult patients with coarctation repair and healthy controls could be demonstrated. Therefore, endothelial dysfunction may not necessarily be present in this population. Further studies are required to identify mechanisms and to develop strategies to avoid arterial hypertension in these patients.
- CONGENITAL HEART DISEASE
- HYPERTENSION
Statistics from Altmetric.com
Introduction
Despite surgical or interventional repair in early life, the prevalence of hypertension in adult patients with aortic coarctation in the absence of re-coarctation remains high, and is associated with an increase in cardiovascular morbidity and mortality.1 As many as 50% of patients aged between 30 years and 40 years may be hypertensive.2 The mechanisms of hypertension in these patients remain largely unclear. As a consequence, coarctation of the aorta is increasingly viewed as a systemic cardiovascular disorder rather than a localised disease of the descending aorta. Endothelial dysfunction is an important component in the development of cardiovascular disease, and has been proposed to play a key role in the pathogenesis of arterial hypertension in patients after coarctation repair.3 Other studies however, have questioned the presence of endothelial dysfunction in this setting.4 ,5 Multiple methods and markers related to endothelial function have been evaluated which are thought to measure different aspects of a complex system. In addition to differences in patient populations, these methodological differences may have contributed significantly to conflicting results.
In this study of endothelial function, a combination of tests on a vascular, cellular and biochemical level was selected. For the non-invasive measurement of endothelial function, we chose peripheral arterial tonometry (PAT) over flow-mediated dilation (FMD). While widely used, measuring FMD requires a considerable amount of operator training and experience which may influence the feasibility and reproducibility of measurements in a clinical setting. Also, protocols, imaging parameters, data analysis and interpretation of results have been quite heterogeneous, complicating the comparability of outcomes.6 Meanwhile, measurements of reactive hyperaemia (RH) by PAT are increasingly being used. The U.S. Food and Drug Administration (FDA)-approved EndoPAT unit features a simple setup and a standardised protocol. Measurements and data analysis are largely automated, easy to perform and have a good reproducibility.7 RH measurements have been shown to correlate with endothelial function as measured by injection of acetylcholine,8 and to independently predict major cardiovascular events.9
Endothelial function is influenced by the balance of endothelial injury and recovery. Proinflammatory cytokines (such as IL-6, IL8 and MCP-1) may impair endothelial function by reducing nitric oxide synthesis in endothelial cells.10 They may also increase production of adhesion molecules (such as VCAM1 and ICAM1) stimulating the migration of leukocytes into the vascular wall in atherogenesis. Measurements have been used for cardiovascular risk prediction.11 Circulating endothelial progenitor cells (EPC) from the bone marrow contribute to the replacement of injured endothelial cells, and their number is related to endothelial function and cardiovascular risk.12 Vascular endothelial growth factor (VEGF) is a potent angiogenic factor stimulating the mobilisation of EPCs from the bone marrow, and reduced levels may be involved in the development of endothelial dysfunction.13
Using this comprehensive panel of previously employed tests, our objective was to study endothelial function, endogenous repair mechanisms and inflammatory injury in a group of contemporary patients after repair of aortic coarctation.
Methods
Study participants
In this prospective observational study, 20 patients with coarctation repair who presented to our adult congenital heart disease centre between July and September 2009 were included. Twenty-two controls were recruited by providing information on the study through leaflets, the department's website and word of mouth (table 1). The protocol was approved by the local ethics committee, and all study participants provided written informed consent.
Patient characteristics
Blood pressure and PAT
Digital reactive hyperaemia was measured with PAT using a commercially available system (Endo-PAT, Itamar Medical, Caesarea, Israel). The examinations were carried out in a quiet room at 25°C with the patient in a supine position and probes placed on both index fingers. A blood pressure cuff was attached to the right arm and patients were allowed to rest and accommodate to temperature conditions for at least 15 min. Blood pressure was measured using an auscultatory sphygmomanometer. After baseline measurements, the blood pressure cuff was inflated to 200 mm Hg or at least 20 mm Hg supra-systolic levels, while the effect of occlusion on tonometry was observed. After exactly 5 min, the cuff was deflated. During the following 10 min of simultaneous tonometry of both index fingers, hyperaemic response was observed. Data were analysed automatically using Endo-PAT-2000-V.3.1.2 (Itamar Medical). The reactive hyperaemia index (RHI) of the occluded arm was calculated as the ratio between postocclusion and preocclusion PAT signals, and normalised to the results of the control arm (figure 1).
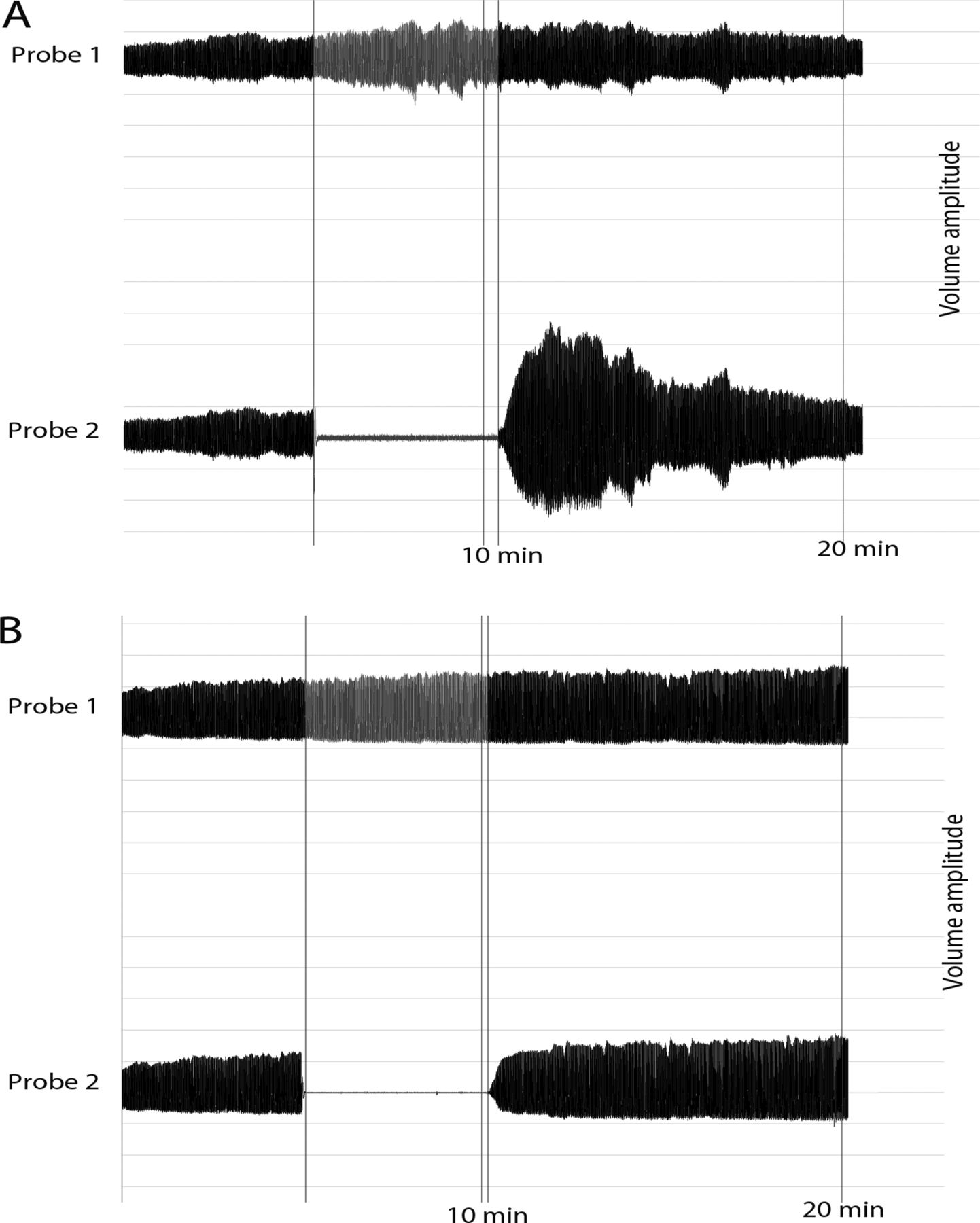
Examples of normal (A) and abnormal (B) peripheral arterial tonometry traces. Traces represent volume changes at the tip of both index fingers over the time course of the recording. During inflation of the blood pressure cuff, blood flow is interrupted in the right index finger (probe 2). In normal individuals, deflation of the cuff leads to marked reactive hyperaemia, while in patients with an impaired endothelial function the increase of the amplitude is much smaller.
Flow cytometric detection of circulating EPCs
Blood was drawn immediately before measurement of digital reactive hyperaemia. Peripheral blood mononuclear cells (PBMNC) were isolated by density centrifugation with Vacutainer CPT cell preparation tubes (BD Biosciences, Oxford, UK) according to the manufacturer's instructions. EPCs were enumerated using established criteria as CD34+ cells coexpressing AC133 and VEGF receptor-2 (VEGFR2/fetal liver kinase 1/KDR) or cells expressing CD34 and not CD45.14 ,15 We incubated 106 PBMNCs with FITC-labelled monoclonal mouse antihuman CD34 (BD Bio-sciences), PE-labelled monoclonal mouse antihuman AC133 (Miltenyi Biotec, Surrey, UK), and allophycocyanin-labelled monoclonal mouse anti-human KDR (R&D Systems, Abingdon, UK) antibodies for 30 min at 4°C according to the manufacturer's instructions, or with appropriate isotype controls. At least 100 000 events were acquired in the lymphomonocytic gate using a FACSCalibur cytometer (Becton Dickinson, Oxford, UK).
Analysis was performed using FCS-Express-3 (De Novo Software, Los Angeles, USA). The number of progenitor cells was calculated as a percentage of all lymphomonocytic cells (figure 2). We also quantified EPCs as lymphomonocytic cells expressing CD34 with low expression of CD45 (PE-labelled monoclonal mouse antihuman CD45, BD Biosciences) as CD45 low/CD34+ EPCs in accordance with previous studies.16

Example of a Fluorescence-activated cell sorting (FACS) cytometric analysis of peripheral blood mononuclear cells in one patient. The number of progenitor cells is calculated as a percentage of all lymphomonocytic cells.
Plasma assays
Plasma levels of interleukin-6 (IL-6), interleukin-8 (IL-8), intercellular adhesion molecule 1 (ICAM-1), vascular cell adhesion molecule 1 (VCAM1), monocyte chemotactic protein-1 (MCP1) and VEGF, were quantified using a bead array cytometric analyser (Luminex System, Luminex Corporation, Austin, Texas, USA) and multiplex bead kits (Bio-Rad Laboratories, Inc., Hercules, California, USA) according to the manufacturer's instructions.
Echocardiographic parameters
A comprehensive standardised echocardiographic evaluation was performed in all patients using a Vivid 7 Ultrasound Machine (GE Healthcare, Little Chalfont, UK). LV mass was calculated from linear dimensions obtained from M-mode images.17 Relative wall thickness was calculated as: (2×posterior wall thickness)/end-diastolic diameter. The aortic arch and descending aorta were visualised from a suprasternal view. Doppler echocardiography was used to measure the peak blood flow velocity (Vmax) at the former coarctation site. Diastolic run-off was defined as continuous forward flow throughout the whole diastole.
Statistical analysis
Data are expressed as mean±SD. Power calculation was performed using G*Power-3.1 (University of Duesseldorf, Department of Psychology, Duesseldorf, Germany) assuming a clinically meaningful difference in mean RHI of 0.4 (22%) on the basis of previous studies8 ,18 and a SD of 0.5 and showed a power (1-β error probability) of 0.83 with the sample size (α error probability 0.05).
Statistical analysis was performed with the Mann–Whitney U test or t test (depending on the distribution of values) and χ2 test were appropriate using GraphPad Prism V.5.0 (GraphPad Software, San Diego, California, USA). For all analyses, a 2-sided value of p<0.05 was considered statistically significant.
Results
Twenty patients with coarctation of the aorta who had undergone surgical treatment in childhood were recruited. The mean age at surgery was 7±6 years. Only five patients were older than 9 years at the time of surgery. Half the patients had known arterial hypertension requiring antihypertensive treatment. Medical treatment had been started at least 3 years prior to enrolment. There was no significant difference in age or Body Mass Index between patients and controls. They also did not significantly differ in gender (χ2 (1, N=42)=1.16, p=0.3) or the number of smokers (χ2 (1, N=42)=2.6, p=0.1). One of the patients had type I diabetes. None of the patients or controls had a history of coronary artery disease or stroke, or had any clinical signs of infection. Details on patient characteristics are presented in table 1.
Systolic ambulatory blood pressure was significantly higher in CoA patients, while diastolic pressure showed no significant difference between patients and controls. At the time of measurements, two patients showed signs of significant residual stenosis (as defined by a blood pressure gradient >20 mm Hg between upper and lower limbs and diastolic run-off), which required subsequent intervention. Two patients had a LV mass index greater than 125 g/m2, and 8 a relative wall thickness above 0.45. The mean values were in the normal range (table 2).
Haemodynamic and echocardiographic parameters
Peripheral arterial tonometry
We could not demonstrate a clinically significant difference in endothelial function as defined by reactive hyperaemia between patients and controls (RH-index 1.96±0.32 vs 1.77±0.48, p=0.82) (figure 3). Also, we found no significant difference in RHI between hypertensive and normotensive patients. When patients were divided in groups with early versus late surgical repair using various age cut-offs, again, no significant difference could be found.

{kind=link}
{kind=link}
{kind=link}
(A) Relationship between reactive hyperaemia indices measured by peripheral arterial tonometry in patients with coarctation repair (CoA, n=20) versus healthy individuals (controls, n=22). (B) Comparison of the number of progenitor cells defined by different criteria and expressed as a percentage of all lymphomonocytic cells in patients with coarctation repair (CoA, n=19) versus healthy controls (n=21). Data are presented in box plots.
Circulating EPC numbers
Circulating EPC numbers, as defined by the number of CD34+, CD34+/KDR+, CD34+/AC133+ or CD34+/AC133+/KDR+ labelled cells did not significantly differ between patients and controls. Similarly progenitor cell numbers, defined as CD34+/CD45− labelled cells, showed no significant difference between CoA patients and controls (figure 3). We could not demonstrate a significant difference in EPC numbers between normotensive and hypertensive patients.
Inflammatory markers
Serum levels of sICAM, IL-6, IL-8 and VEGF did not show a significant difference between patients and controls (p>0.05 for all). Although there was a trend towards an increased level of sVCAM in patients, only levels of MCP-1 showed a significant difference between controls and CoA patients (table 3).
Levels of serum markers
Discussion
Arterial hypertension remains a common problem after coarctation repair, and is a major concern in the long-term outcome of these patients. The pathophysiology of hypertension after successful surgical treatment of aortic coarctation, and in the absence of re-coarctation is still poorly understood. It has been suggested that coarctation of the aorta could represent a primary or secondary systemic vasculopathy rather than an isolated local disease of the aortic isthmus. These changes are thought to be involved in the development of hypertension in the absence of re-coarctation as well as premature cardiovascular events.
A number of observational studies in patients after coarctation repair have proposed endothelial dysfunction as measured by FMD, or a decreased reactivity to nitric oxide of the arterial wall as a key player in this respect.3 ,19–22 Impairment of FMD in these patients has been described with20 and without evidence of increased blood pressures.3 This has lead to the hypothesis that endothelial dysfunction may not simply be the result, but partly the cause of hypertension in the absence of re-coarctation. The findings of persistent impaired endothelial function proximally, but not distally, to the former coarctation site,19 ,23 as well as association of endothelial dysfunction with age at repair,21 suggest that the former pressure gradient across the coarctation may be a mechanism inducing structural and functional changes including endothelial dysfunction. Proinflammatory cytokines and soluble adhesion molecules associated with endothelial function have been found to be increased even in normotensive patients3 ,24 and point towards an ongoing endothelial injury. However, a number of investigators have recently reported preserved endothelium-dependent vascular reactivity in contemporary patients after coarctation repair4 ,5 ,25 and have found serum markers of endothelial dysfunction (Endothelin-1) not to be significantly elevated compared with controls.24
The current study investigated contemporary patients with coarctation repair and adequate blood pressure—albeit with a relatively high proportion of patients on antihypertensive medication. In a study powered to detect previously described meaningful clinical differences in RHI, we could not demonstrate a significant difference in endothelial function as assessed by PAT between patients and healthy controls. Consistent with this finding, numbers of EPCs, soluble forms of adhesion molecules, and all but one serum level of proinflammatory markers did not show a significant difference. The consistent finding of preserved endothelial function on a molecular, cellular and vascular level (investigated for the first time as part of a single study) suggest that a clinically relevant endothelial dysfunction may not be present in our population.
In some regards, the patients included in the current study may represent the better end of the spectrum of patients. The mean age at surgery in our population was 7±6 years. While some investigators have shown evidence for endothelial dysfunction even in patients operated at a very young age,23 others have found normal FMD in patients younger than 9 years of age at coarctation repair.21 Also, LV mass has been shown to relate to the time to correction as well as systolic blood pressure in coarctation patients.20 LV hypertrophy was present in only 10% of our patients.
While a preserved endothelial function in our normotensive patients would be consistent with recent findings of others,4 ,25 the percentage of hypertensive patients was high in our patient group. In these patients, antihypertensive treatment resulted in good blood pressure control, and had been initiated at least 3 years prior to enrolment. It seems possible that early and rigorous use of antihypertensive medication in the current era may have, in part, prevented peripheral vascular and myocardial damage. Two recent prospective drug trials in patients after coarctation repair have provided evidence that impairment of endothelial function may, in fact, be reversible. Four weeks of treatment with an ACE inhibitor26 or a HMG-CoA reductase inhibitor27 resulted in markedly increased FMD, while levels of proinflammatory cytokines and soluble adhesion molecules decreased.
In the light of our results, it appears that other mechanisms of hypertension in the absence of re-coarctation must also be considered: increased stiffness of the aorta and the carotid arteries have been demonstrated by several studies.23 ,24 Aortic coarctation patients have been found to have histological changes of the aortic wall including fibrosis, cystic media necrosis and fragmentation of elastic fibres.28 De-differentiation of arterial smooth muscle and medial thickening have been described in animal models of coarctation, and provide possible explanations for the functional changes. Finally, the elastic properties of the aorta can also be altered by replacing elastic vessel tissue with stiff foreign material. In a study on the impact of aortic stenting in coarctation patients with significant stenosis, those with tube graft implantation showed little improvement in arterial hypertension despite successful reduction of the gradient.29
Study limitations
It might be considered a limitation of this study that measurements of FMD were not included. Considerations of standardisation, reproducibility and feasibility in our clinical setting have led us to choose PAT, which has recently emerged as an alternative technique.
In general, endothelial dysfunction is considered a systemic condition because evidence has been found in many vascular beds from the coronary arteries to the peripheral arteries and the microvasculature. Non-invasive peripheral measurements with FMD and PAT show a correlation with coronary endothelial function, but some differences have to be noted: while FMD is thought to be more related to conduit artery function, PAT may represent microvascular function to a higher degree.30 Also, alterations in vascular structure and function may not be uniformly distributed throughout the vasculature proximal to the former coarctation site. In a recent study using an animal model of coarctation, a progression of vascular remodelling, beginning first in large elastic arteries and delayed in distal vessels was found. It is thus possible that measurements of FMD would have yielded different results in our study. Even though microvascular function has been postulated to be an earlier indicator of cardiovascular risk especially in young patients, the value in coarctation patients remains to be determined.30
Finally, increasing the size of the sample may have exposed more subtle differences between the groups, albeit these may not be of clinical relevance.
Conclusion
By contrast with earlier reports, no clinically significant difference in endothelial function between adult patients with coarctation repair and healthy controls could be demonstrated.
Our findings on a molecular, cellular and vascular level suggest that aortic coarctation may not necessarily be associated with endothelial dysfunction in adult coarctation patients as seen at tertiary centres. Further studies are required to identify mechanisms and to develop strategies to avoid arterial hypertension in these patients.
Key messages
-
What is already known on this subject?
-
The prevalence of arterial hypertension in adult patients with aortic coarctation remains high and is associated with an increase in cardiovascular morbidity and mortality. Endothelial dysfunction has been proposed to play a major role in the pathogenesis of hypertension in the absence of re-coarctation in these patients.
-
What might this study add?
-
The results of the current study demonstrate that endothelial dysfunction – as assessed by peripheral arterial tonometry, numbers of endothelial progenitor cells, soluble forms of adhesion molecules, and serum levels of proinflammatory markers – may not be inevitable in contemporary patients after coarctation repair.
-
How might this impact on clinical practice?
-
Our results are of clinical relevance as they demonstrate that aortic coarctation may not necessarily be associated with endothelial dysfunction in adult coarctation patients, as seen at tertiary centres. This underlines the possible importance of other mechanisms as potential causes of persistent arterial hypertension in the absence of re-coarctation. A better understanding of the involved mechanisms may at some point influence treatment decisions.
References
Footnotes
-
Contributors All authors have made substantial contributions to the manuscript. RMR and G-PD designed the study protocol. RMR, MD, DH and TT performed the measurements and lab work. Data analysis and writing was done by RMR and critically reviewed by G-PD and HB.
-
Funding This study was supported by a research grant from the Fördergemeinschaft Angeborene Herzfehler Universität Münster e.V., Germany and a research grant from the Deutsche Forschungsgemeinschaft, Germany (DFG Th903/7-2).
-
Competing interests None.
-
Ethics approval Local Ethics Committee of the University of Muenster.
-
Provenance and peer review Not commissioned; externally peer reviewed.