Article Text

Abstract
Objective Patients with repaired tetralogy of Fallot (TOF) experience increased rates of mortality and morbidity in adulthood. This study was designed to identify risk factors for death and ventricular tachycardia (VT) in a large contemporary cohort of patients with repaired TOF.
Methods Subjects with repaired TOF from four large congenital heart centres in the USA, Canada and Europe were enrolled. Clinical, ECG, exercise, cardiac magnetic resonance (CMR) and outcome data were analysed.
Results Of the 873 patients (median age 24.4 years), 32 (3.7%) reached the primary outcome (28 deaths, 4 sustained VT; median age at outcome 38 years; median time from CMR to outcome 1.9 years). Cox proportional-hazards regression identified RV mass-to-volume ratio ≥0.3 g/mL (HR, 5.04; 95% CI 2.3 to 11.0; p<0.001), LV EF z score<−2.0 (HR, 3.34; 95% CI 1.59 to 7.01; p=0.001), and history of atrial tachyarrhythmia (HR, 3.65; 95% CI 1.75 to 7.62; p=0.001) as outcome predictors. RV dysfunction was predictive of the outcome similar to LV dysfunction. In subgroup analysis of 315 subjects with echocardiographic assessment of RV systolic pressure, higher pressure (HR 1.39; 95% CI 1.19 to 1.62; p<0.001) was associated with death and sustained VT independent of RV hypertrophy and LV dysfunction.
Conclusions RV hypertrophy, ventricular dysfunction and atrial tachyarrhythmias are predictive of death and sustained VT in adults with repaired TOF. These findings may inform risk stratification and the design of future therapeutic trials.
- Congenital Heart Disease
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Despite significant advances in the early management of tetralogy of Fallot (TOF) and 20-year survival rates exceeding 90%, residual hemodynamic and electrophysiological abnormalities contribute to increasing morbidity and mortality rates beginning in the third decade of life.1–4 Since the first reports of sudden death in survivors of TOF repair from 40 years ago, numerous attempts have been made to define risk factors for adverse clinical outcomes.5 ,6 Most reports, however, suffer from a small sample size of patients predominantly operated in the late 1950s to the early 1970s when surgical techniques were evolving rapidly. Furthermore, the ability to noninvasively assess RV size and function, which are notably affected by sequelae of TOF surgery, was limited and imprecise.7 A previous multicentre cohort study identified QRS duration ≥180 ms as a predictor of death and clinical arrhythmia in patients with repaired TOF.8 However, as with other studies from that era, assessment of the RV was imprecise. More recently, the advent of cardiovascular magnetic resonance (CMR) has allowed accurate and reproducible noninvasive measurements of biventricular size and function and quantification of valvular regurgitation.9–11Several single-centre studies have indicated that severe RV dilatation and RV and/or LV dysfunction measured by CMR are important risk factors for adverse clinical outcomes, superseding the importance of QRS prolongation as a predictor of outcome.12 ,13 These studies, similarly, were hampered by small sample sizes and paucity of hard outcomes.
To overcome these limitations and to determine risk factors for death and sustained ventricular tachycardia (VT) in a large contemporary cohort of TOF repair survivors, we have established the International Multicenter TOF Registry (INDICATOR).14 The goals of this registry, which enrolled contemporarily managed patients from four large congenital heart centres in the USA, Canada and Europe, were to allow risk stratification based on clinical, ECG, exercise and CMR data and to explore whether these risk factors vary according to type of repair.
Methods
Patients
A detailed description of the methodology of the INDICATOR registry, including recruitment protocol, inclusion and exclusion criteria, data collection and data analysis in the core laboratory has been published.14 Briefly, participating centres identified patients fulfilling the following inclusion criteria: (1) repaired TOF; (2) CMR completed between 1997 and 2010; (3) 12-lead ECG within 1 year from CMR; and (4) clinical follow-up ≥1 year or occurrence of a primary outcome. Patients with CMR data that were incomplete or not suitable for quantitative assessment by the CMR core laboratory were excluded. Each participating centre received Institutional Review or Ethical Board approval.
Data collection
De-identified data were sent to the data coordinating centre, which included a data repository, CMR core laboratory and a statistical core centre. The registry collected data on patient demographics (date of birth, gender, race), anatomic type of TOF, associated anomalies, surgical and catheter interventions and clinical outcomes. Clinical history and dates of any arrhythmias were recorded, including atrial ablation prior to a documented outcome and pacemaker or defibrillator implantation after CMR.
The following diagnostic studies were sought at the time of enrolment: CMR, ECG, ambulatory 24-h Holter monitor and exercise stress test. One centre also collected Doppler echocardiographic data to quantify RV systolic pressure based on peak velocities of the tricuspid regurgitation jet and RV outflow. The ECG was analysed for heart rate and QRS duration. The 24-h Holter monitor was analysed for atrial arrhythmia (categorised as supraventricular tachycardia, atrial fibrillation or atrial flutter) and for ventricular ectopy (defined as >100 premature ventricular contractions, >20 couplets or nonsustained VT lasting <30 s).
De-identified digital copies of the CMR examinations were sent to the CMR core laboratory for analysis. The technical details of the CMR imaging protocol, analysis methods and quality assurance procedures have been published.10 ,14 ,15 Measurements included diastolic and systolic RV and LV volumes, mass and pulmonary regurgitation fraction. Calculations included ventricular stroke volumes and EFs. Measurements were adjusted to body surface area and z scores were calculated.
Outcomes
The combined primary outcome was defined as all-cause mortality (classified as sudden cardiac death, heart failure-related death, cardiac other or non-cardiac), aborted sudden cardiac death (defined as resuscitated pulseless cardiac event) or sustained VT (lasting ≥30 s or requiring cardioversion). Participating centres updated the data coordinating centre every 6 months regarding new clinical outcomes, including periodic reviews of available national death registries.
Statistical analysis
Categorical variables were summarised using frequencies and percentages and compared for patients with and without the primary outcome using Fisher's exact test. Continuous variables were summarised using either the mean and SD or median and range; they were compared using the unpaired t test or Wilcoxon rank-sum test. Cox proportional hazards regression was used to evaluate factors associated with time from last CMR until death, aborted sudden cardiac death or sustained VT. Patients who did not experience the primary outcome were censored at the time of last follow-up. Hazard ratios (HR)s are reported with 95% CIs. Harrell's c-index was used to quantify how well the model discriminates between subjects who experienced the outcome and those who did not. The c-index extends the area under the receiver-operator curve (c-statistic) for binary outcomes to the case of censored survival time data; a value of 0.5 indicates that the model has no ability to predict the outcome, while a value of 1.0 indicates that the model perfectly discriminates between subjects with and without the outcome. Stepwise forward selection was used to fit a multivariable model. Once the factors most strongly associated with the primary outcome were identified, cut points were considered for continuous variables. Nagelkerke's R2 was reported for the final models. This value approximates the amount of variability in the outcome explained by the factors in the model. Analyses were repeated for the subgroups of patients with and without RV-to-pulmonary artery (RV-PA) conduits. In order to evaluate the relationship between RV systolic pressure and outcome, a subgroup analysis was performed for patients in whom RV pressure data were available within 1 year of the CMR. A two-sided p value of less than 0.05 was considered to indicate statistical significance. Statistical analyses were performed using Stata V.12 (StataCorp, College Station, Texas, USA).
Results
Study patients
Of the 1265 subjects screened for enrolment, 873 fulfilled entry criteria, and thus, formed the study cohort. Their demographic, anatomic and surgical characteristics are shown in table 1. Selected laboratory data stratified by outcome are listed in table 2.
Demographic, anatomic and surgical characteristics
Arrhythmia, exercise, and CMR data
Of the 873 cohort patients, 32 experienced the primary outcome of death (n=28) or sustained VT (n=4). Median follow-up from first CMR was 4.2 years (15 days to 12.2 years). Outcomes occurred from 4 days to 9.2 years (median 1.9 years) after baseline evaluation at a median age of 38 years (1.7–74.6 years). Of the 28 deaths (median age 41.8 years), 4 (14%) were classified as sudden cardiac death (median age 43 years), 6 (22%) as heart failure-related (median age 53.7 years), 4 (14%) as other cardiac (median age 38.5 years), 9 (32%) as non-cardiac (median age 44.4 years), and 5 (28%) as unknown (median age 32 years). The median age at presentation of sustained VT was 29.3 years.
Predictors of outcomes
Multiple demographic, clinical, ECG, exercise and CMR variables were associated with the outcome on univariable analysis (table 3). Although duration of the QRS complex on ECG was not associated with the outcome when analysed as a continuous variable, QRS duration ≥180 ms was an outcome predictor (HR, 3.17; 95% CI 1.42 to 7.10; p=0.005). Importantly, compared with a model that includes CMR-measured RV mass-to-volume ratio and LV EF, the c-index of a model that includes only QRS duration ≥180 ms was significantly lower (0.85 vs 0.59, p=0.001). Notably, RV end-diastolic volume and RV/LV end-diastolic volume ratio were not associated with the outcome whereas RV and LV EF, RV mass index, and RV mass-to-volume ratio were strongly related to death and sustained VT.
Univariable predictors of outcome
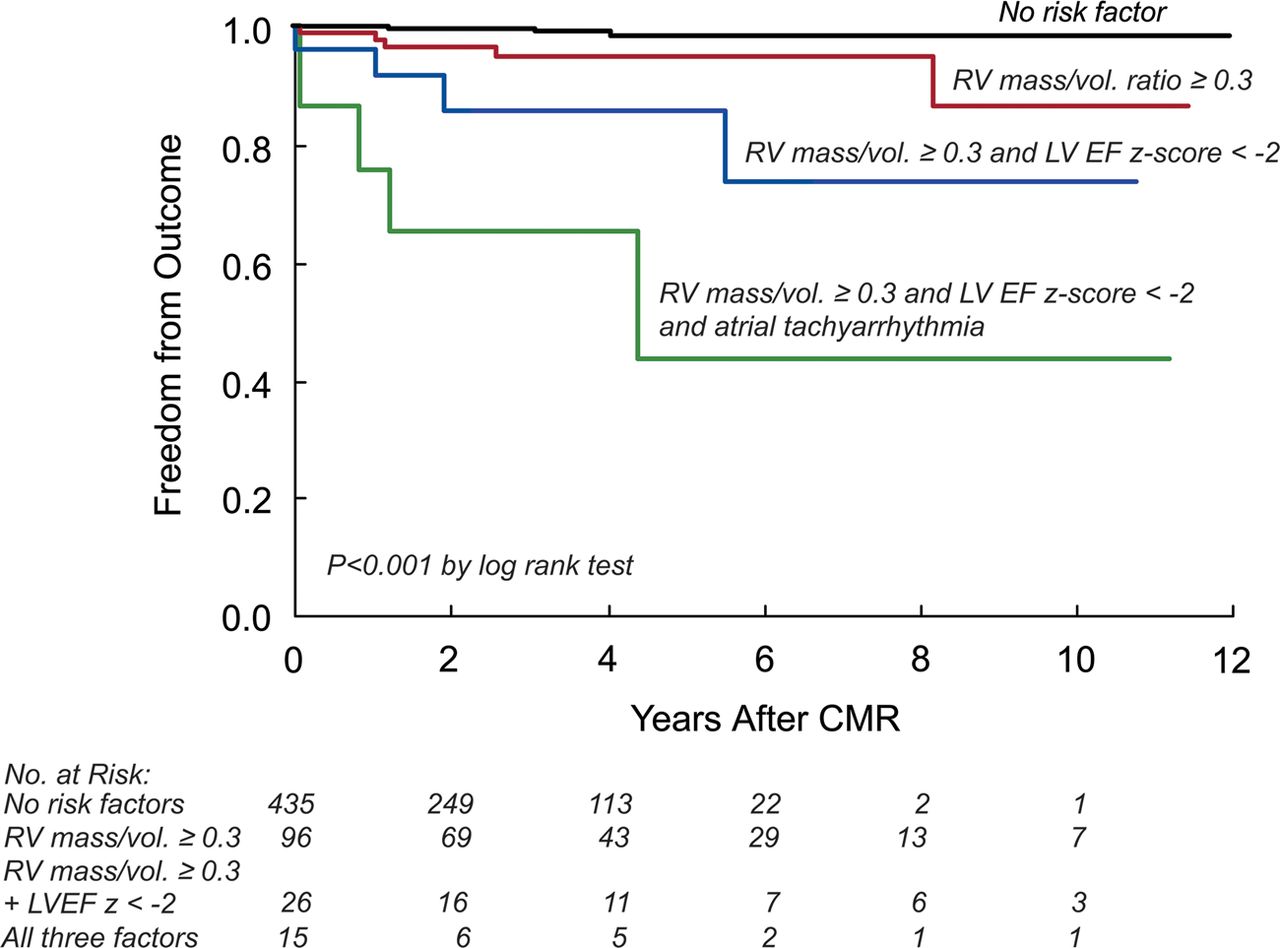
The best predictive model for death and sustained VT by multivariable analysis included RV mass-to-volume ratio ≥0.3 g/mL, LV EF z score <−2.0 (<55% in males and <54% in females), and history of atrial tachyarrhythmias (model c-index 0.832; R2 0.246; table 4). Using Kaplan–Meier analysis, we found that in patients with none of the above predictors, freedom from the outcome was 98% at 5 and 10 years. In contrast, freedom from the outcome at 5 and 10 years was 95% and 86%, respectively, in patients with RV mass-to-volume ratio ≥ 0.3 g/mL; 86% and 74%, respectively, in patients with RV mass-to-volume ratio ≥0.3 g/mL and LV EF z score <−2.0; and 65% and 43%, respectively, in patients with all three risk factors (figure 1). Replacement of LV EF z score <−2.0 with RV EF z score <−2.0 (<48% in males and <50% in females) resulted in only slight decreases in the model's c-index and R2 values. Finally, we found that the above risk factors were associated with the outcome regardless of the type of death. Specifically, multivariable analysis of patients who experienced cardiac death or sustained VT (excluding those with non-cardiac and unknown causes) found the same variables to be associated with the primary outcome with a similar c-index of 0.826 as compared with 0.832 for all outcomes. Similar findings were also noted when the analysis was repeated in patients that experienced cardiac death, excluding the four patients with sustained VT.
Multivariable predictors of outcome
{kind=link}
Kaplan–Meier curves for the outcome ( death and sustained VT) according to risk factors. Access the article online to view this figure in colour.
Subgroup analyses
To determine whether risk factors for the outcome are the same in patients with and without RV-PA conduits placed as part of TOF repair, we performed additional subgroup analyses (table 4). Multivariable Cox regression analysis showed that the same risk factors that were identified in the entire cohort were also predictive in the 724 patients with no conduit. In contrast, among the 149 patients with RV-PA conduit, predictors of outcome included RV mass-to-volume ratio ≥0.5 g/mL and LV end-systolic volume index ≥ 35 mL/m2.
We further analysed interactions between Doppler-derived RV pressure, RV hypertrophy and clinical outcomes among the 315 patients in whom all of these parameters were available. The group with RV pressure data differed from those without this information (n=558) with regard to demographics, clinical and surgical histories, ECG, exercise and CMR parameters (see online supplementary table 1S). Of the 302 patients with Doppler data in the RV outflow tract, 29 (10%) had a peak gradient ≥50 mm Hg, 101 (33%) had a peak gradient between 20 and 49 mm Hg, and 172 (57%) had a peak gradient <20 mm Hg. As expected, RV pressure positively correlated with RV mass index (rs=0.33, p<0.001) and with RV mass-to-volume ratio (rs=0.57, p<0.001). Compared with the 293 patients who did not have the outcome, those who experienced death or sustained VT (n=22) had a significantly higher RV systolic pressure (64±27 mm Hg vs 40±18 mm Hg, p<0.001). Multivariable analysis showed that in addition to lower LV EF z score, both RV mass z score (HR 1.08 for every 1 SD increase; 95% CI 1.02 to 1.14; p=0.008) and RV pressure (HR 1.39 for every 10 mm Hg increase; 95% CI 1.19 to 1.62; p<0.001) were predictive of the outcome (table 4).
Discussion
This large multicentre observational cohort study identified RV hypertrophy, left or RV systolic dysfunction and atrial tachyarrhythmias as predictors of death or sustained VT in young adult patients with repaired TOF. Moreover, we found that patients with two or three concurrent risk factors were at a much greater risk for poor clinical outcome as compared with those having none or a single risk factor. Subgroup analyses showed that patients with a conduit between the RV and the pulmonary arteries have different risk factors than those without a conduit. In selected patients with noninvasive data on RV pressure, both RV hypertension and increased RV mass are independently associated with poor outcomes despite correlations between these variables. Also notable is the lack of association between RV volumes and the study's primary outcome. It is important to note that in contrast to prior studies that focused on RV volumes,11–,13 our study is the first to examine the relationships between CMR and other clinical and laboratory parameters and hard clinical outcomes as opposed to surrogate outcomes.
In this study, we chose all-cause mortality or sustained VT as the composite primary outcome because of their clinical importance. Although half of the deaths in this cohort were classified as other or unknown, all-cause mortality is a key outcome.3 Furthermore, it is often difficult to distinguish between cardiac and non-cardiac death as comorbidities can be induced or exacerbated by poor cardiac status. Our observation that approximately half of the deaths were classified as other or unknown is similar to the findings of Chiu et al3 that 14 of their 29 patients (48%) with repaired TOF died of non-cardiac causes. Importantly, we found that the risk factors identified in this study applied to patients regardless of the type of death. Specifically, the same risk factors were associated with the primary outcome when the analysis was restricted only to those patients who experienced cardiac-related death or sustained VT.
Previous studies on risk factors for adverse clinical outcomes late after TOF repair have identified numerous predictors, which can be divided into three broad categories: (1) patient history (eg, older age at repair); (2) electrophysiologic markers (eg, prolonged QRS duration); and (3) hemodynamic abnormalities resulting from severe chronic pulmonary regurgitation and other sequelae of TOF surgery (eg, ventricular dysfunction).6 ,7 ,16 ,17 Although these studies provided useful insights into risk stratification, most were constrained by relatively small sample sizes, reliance on surrogate outcomes, or lack of accurate tools to evaluate RV size and function.12 ,13 ,18–,20 The importance of our study is underscored by its analysis of data from a large multicentre cohort with clinically important outcomes and its comprehensive collection of variables from all three broad categories. Whereas univariable analysis confirmed several previously noted associations between clinical and laboratory parameters and adverse patient outcomes, multivariable analyses provided new insights.
This study is the first to identify RV hypertrophy as an independent risk factor for death and sustained VT in patients with repaired TOF. Specifically, patients with RV mass-to-volume ratio ≥0.3 were more than five times more likely to experience the outcome as compared with those with a lower ratio. Similar findings were noted with other measures of RV hypertrophy such as mass index and z score. To our knowledge, only one previous study identified RV hypertrophy as a risk factor for adverse clinical outcomes in this patient population.12 Indeed, most studies on the subject, including those with CMR data, have not measured RV mass.11 ,18 ,19 In contrast to patients with congenital heart disease, a large body of literature documents the strongly negative prognostic value of LV hypertrophy in acquired conditions such as essential hypertension and diabetes.21–23 Moreover, a recent study showed that increased RV mass was associated with more than twice the risk of heart failure or death in adult patients enrolled in the Multi-Ethnic Study of Atherosclerosis (MESA).24 Based on studies of the myocardium in these and other acquired cardiovascular diseases, it is reasonable to suspect that the increase in RV mass is due not only to increase in myocyte volume but also due to increase in interstitial volume with increased collagen concentration and gross fibrosis.25 If confirmed, this may be a target for future therapies.
To further explore whether RV hypertrophy is a surrogate of RV hypertension and to determine which parameter better predicts the clinical outcome, we explored these questions in a subgroup of patients with Doppler estimation of RV systolic pressure. As expected, the two variables correlated with each other. Unexpectedly, however, both were associated with the outcome in multivariable analysis. These results suggest that despite a moderate correlation between higher pressure and increased mass, each parameter contributes to risk through different mechanisms or that they synergistically interact via a common pathway. We speculate that the RV hypertrophy observed in our study results from a maladaptive process in response to prolonged volume and/or pressure overload leading to pathological increase in the ratio of interstitial content (primarily collagen and fibroblasts) to myocytes volume. Such maladaptive pathological process has been shown in a variety of diseases affecting the LV.26 Additional factors such as intraventricular and interventricular dyssynchrony may also contribute to mechanical inefficiency of ventricular function and pathological hypertrophy.
From a practical perspective, the findings of our study provide a framework for risk stratification of patients with repaired TOF. It remains speculative whether therapeutic interventions designed to prevent or lessen the risk factors identified in this cohort will lead to improved clinical outcomes, including longer life expectancy and freedom from major arrhythmias. Possible therapeutic interventions include surgical or transcatheter pulmonary valve implantation prior to development of ventricular dysfunction, development of RV hypertrophy or onset of atrial tachyarrhythmias; ablation or other therapies for atrial flutter or fibrillation; early intervention to decrease RV systolic pressure (eg, catheter or surgical treatment of pulmonary artery stenosis); and, finally, pharmacological therapy designed to decrease diffuse myocardial fibrosis.
Our study has several limitations. The cohort is restricted to subjects who have undergone CMR; this limitation is partially mitigated by the routine use of CMR in this patient group at the participating centres. In addition, patients with pacemakers or defibrillators implanted before CMR were excluded. Although we made every effort to ascertain clinical outcomes through regular updates of the registry every 6 months and review of national death registries, it is conceivable that some outcomes were not recorded. Finally, the cutoff values for RV mass-to-volume ratio reported here might not be generalisable as measurement of RV mass may vary by technique.
In conclusion, RV hypertrophy and LV and RV dysfunction measured by CMR, as well as atrial tachyarrhythmias predict death and sustained VT in patients with repaired TOF. The likelihood of a poor outcome increases substantially when multiple risk factors coexist. Elevated RV systolic pressure may confer an additional risk, though the mechanism that distinguishes it from that of RV hypertrophy requires additional study. These findings may inform the design of future trials on therapeutic interventions in this population.
Key messages
-
What is already known about this subject?
-
Patients with repaired tetralogy of Fallot (TOF) experience increased rates of mortality and morbidity beginning in early adulthood but the risk factors for late adverse outcomes are poorly defined.
-
How might this impact on clinical practice?
-
Our findings inform risk stratification and clinical decisions as well as the design of future trials on therapeutic interventions in patients with repaired TOF.
-
What this study adds?
-
We analysed risk factors for adverse clinical outcomes in a large, contemporarily managed cohort of young adult patients with repaired TOF enrolled in the International Multicentre TOF Registry (INdiCaTOR). The results uncover new risk factors for death and sustained ventricular tachycardia, including right ventricular hypertrophy, left and/or right ventricular dysfunction and history of atrial tachyarrhythmias. This information informs risk stratification and clinical decisions in this rapidly growing population of adult patients.
Acknowledgments
We thank Sarah P Evans, BS, and Ioannis Germanakis, MD for their assistance with data processing. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table
Footnotes
-
Contributors AMV: conceived and designed the research, acquired the data, analysed and interpreted the data, drafted the manuscript and approved the final version of the manuscript. GEA: analyzed and interpreted the data, contributed to drafting the manuscript, critically reviewed the manuscript and approved the final version of the manuscript. JS: acquired the data, analysed and interpreted the data, contributed to drafting the manuscript, critically reviewed the manuscript and approved the final version of the manuscript. KG: performed statistical analysis, analysed and interpreted the data, drafted part of the manuscript, critically reviewed the manuscript and approved the final version of the manuscript. RI, ZK: acquired data, critically reviewed the manuscript and approved the final version of the manuscript. MAG, PJK, MJL, BM, AJP, RW, SVB-N, MG: contributed to the study design, contributed to acquisition of data, critically reviewed the manuscript and approved the final version of the manuscript. TG: responsible for all aspects of the research, conceived and designed the research, analysed and interpreted the data, drafted the manuscript and approved the final version of the manuscript.
-
Funding Higgins Family Noninvasive Research Fund at Boston Children's Hospital (TG, AMV, AJP), the Dunlevie Foundation (AMV, JS, MJL, GEA), the Lerner Research award (AMV), NIH/NHLBI 1 R01 HL089269-01A2 (TG), and the British Heart Foundation Fellowship award (SVB-N). SVB-N, MAG and PJK were supported by the NIHR Cardiovascular Biomedical Research Unit of Royal Brompton and Harefield NHS Foundation Trust and Imperial College London. This report is independent research by the National Institute for Health Research Biomedical Research Unit Funding Scheme.
-
Competing interests None.
-
Ethics approval Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.