Article Text

Statistics from Altmetric.com
Clinical guidelines have become a core element in optimising care for patients with cardiovascular disease. However, the quality of guidelines depends on a rigorous unbiased process that integrates the clinical evidence with input from a range of stakeholders. In this issue of Heart, Garbi1 summarises the National Institute for Health and Care Excellence (NICE) principles and processes for development of clinical guidelines in England. The discussion is divided into four key areas: (1) Guideline development by an independent advisory committee includes aligning recommendations with national health policies, and involvement of patients, patient-advocates, and the public as well as healthcare professionals. (2) Recommendations should be based on relevant, reliable and robust evidence and should include consideration of cost-effectiveness and population benefit. (3) Guidelines should support innovation and reduce healthcare inequalities. (4) Finally, ensuring guideline implementation and providing regular updates are essential.
In the accompanying editorial, Otto, Kudenchuk and Newby2 compare the NICE methodology with the current approach of our cardiovascular professional societies, as well as to established reporting criteria for clinical practice guidelines (figure 1).3 They propose several areas for improvement including cooperative development of a common evidence database; a rigorous transparent process based on established standards; a more diverse group of stakeholders; minimising conflicts of interest; support by information specialists, medical writers and other relevant experts; regular updates; adaptation for regional considerations; and improved methods for dissemination and access. As they conclude: ‘Current cardiovascular society guidelines fall short of best practice. We can and must do better.’

Visual summary of reporting criteria for clinical practice guidelines as detailed in the Appraisal of Guidelines, Research and Evaluation (AGREE) checklist.
In patients with atrial fibrillation (AF) at moderate or high risk of stroke, randomised controlled trials (RCTs) have shown superiority or non-inferiority of non-vitamin K oral anticoagulants (NOACs) over vitamin K anticoagulants (VKA) for prevention of stroke or systemic embolism along with reduced rates of intracranial haemorrhage. However, patients in RCTs may not be representative of the full range of patients seen in clinical practice. In order to address this issue, Camm and colleagues4 used a method called overlap propensity matching to compare the effectiveness of VKA and different NOACs for mortality, stroke/systemic embolism and major bleeding in patients with newly diagnosed AF and an indication for oral anticoagulation. Based on 25 551 patients in the Global Anticoagulant Registry in the FIELD-Atrial Fibrillation (GARFIELD-AF) study, they confirmed that ‘Important benefits in terms of mortality and major bleeding were observed with NOAC versus VKA with no difference among NOAC subtypes’ (figure 2).
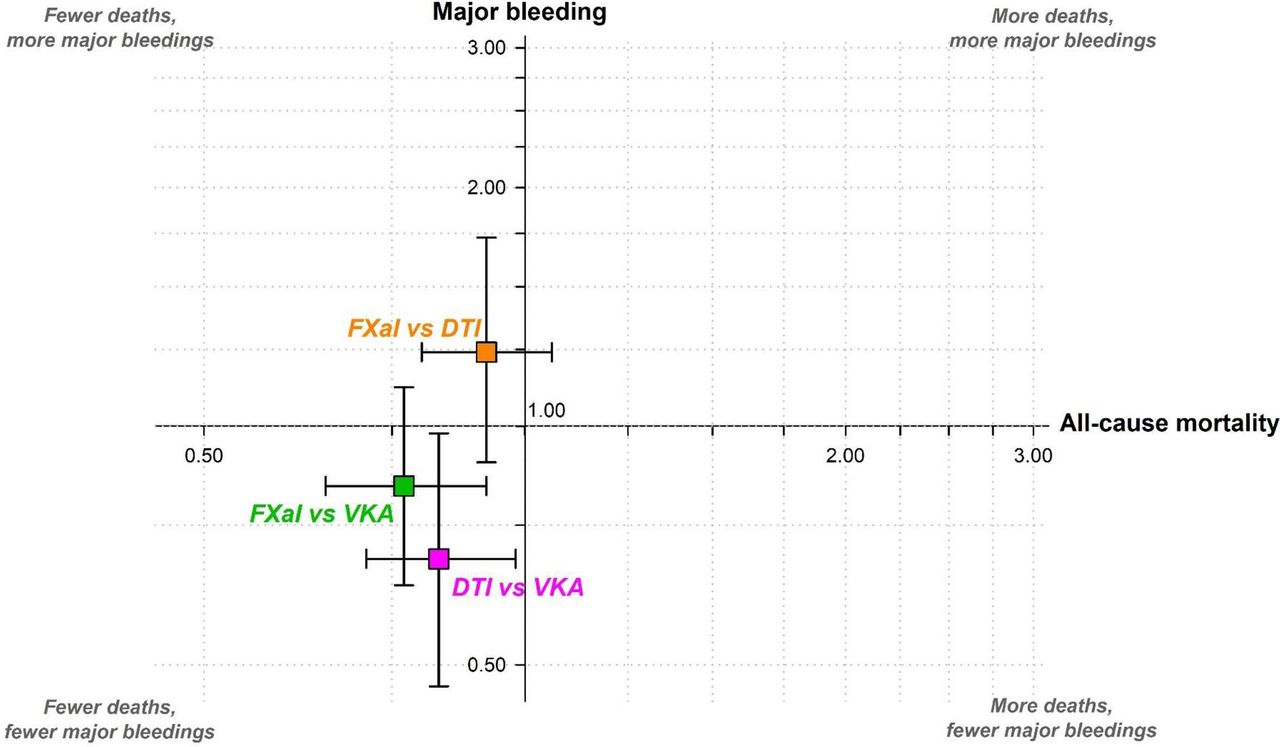
Adjusted* HRs and corresponding 95% CIs for selected outcomes at 2 years of follow-up by OAC treatment at baseline. The reference considered is the treatment reported as second. *Obtained using an overlap-weighted Cox model. Variables included in the weighting scheme are: country and cohort enrolment, sex, age, ethnicity, type of AF, care setting specialty and location, congestive heart failure, acute coronary syndromes, vascular disease, carotid occlusive disease, prior stroke/TIA/SE, prior bleeding, venous thromboembolism, hypertension, hypercholesterolaemia, diabetes, cirrhosis, moderate to severe chronic kidney disease, dementia, hyperthyroidism, hypothyroidism, current smoking, heavy alcohol consumption, body mass index (BMI) heart rate, systolic and diastolic blood pressure at diagnosis and baseline antiplatelet use. DTI, direct thrombin inhibitor; FXaI, factor Xa inhibitors; NOAC, non-vitamin K oral anticoagulants; OAC, oral anticoagulants; SE, systemic embolism; TIA, transient ischaemic attack; VKA, vitamin K antagonists.
In the accompanying editorial, Choi and Lee5 point out the strengths of this study including a clinically diverse international patient cohort with regular audits and a low rate of loss to follow-up, a sophisticated matching method, and results consistent with previous RCTs. However, limitations include the possibility of residual confounders; possible discontinuation or switching of medications during this study period; lack of detailed data on types of major bleeding, and regional or ethnic differences in outcomes; and any effects due to lack of adherence to therapy. As they conclude ‘The GARFIELD-AF registry has reported valuable clinical practice patterns in AF worldwide, but it will also play a role as a pragmatic study for real-world practice-based RCTs.’
The prevalence and outcomes of adults over age 65 years with more than mild mitral regurgitation (MR) or tricuspid regurgitation (TR) was studied in 4755 subjects who had undergone echocardiography in the Oxford Valvular Heart Disease Population Study (OxVALVE).6 Overall, the prevalence of moderate or greater MR was 3.5% and TR was 2.6% with only about half these patients having previously diagnosed valve disease. Subjects with regurgitation identified by screening were less likely to be symptomatic than those with known valve disease. The aetiology of MR was most often primary although 22% had secondary MR due to left ventricular systolic dysfunction (figure 3). Surgical intervention was rarely undertaken (2.4%) during the 64-month median follow-up.
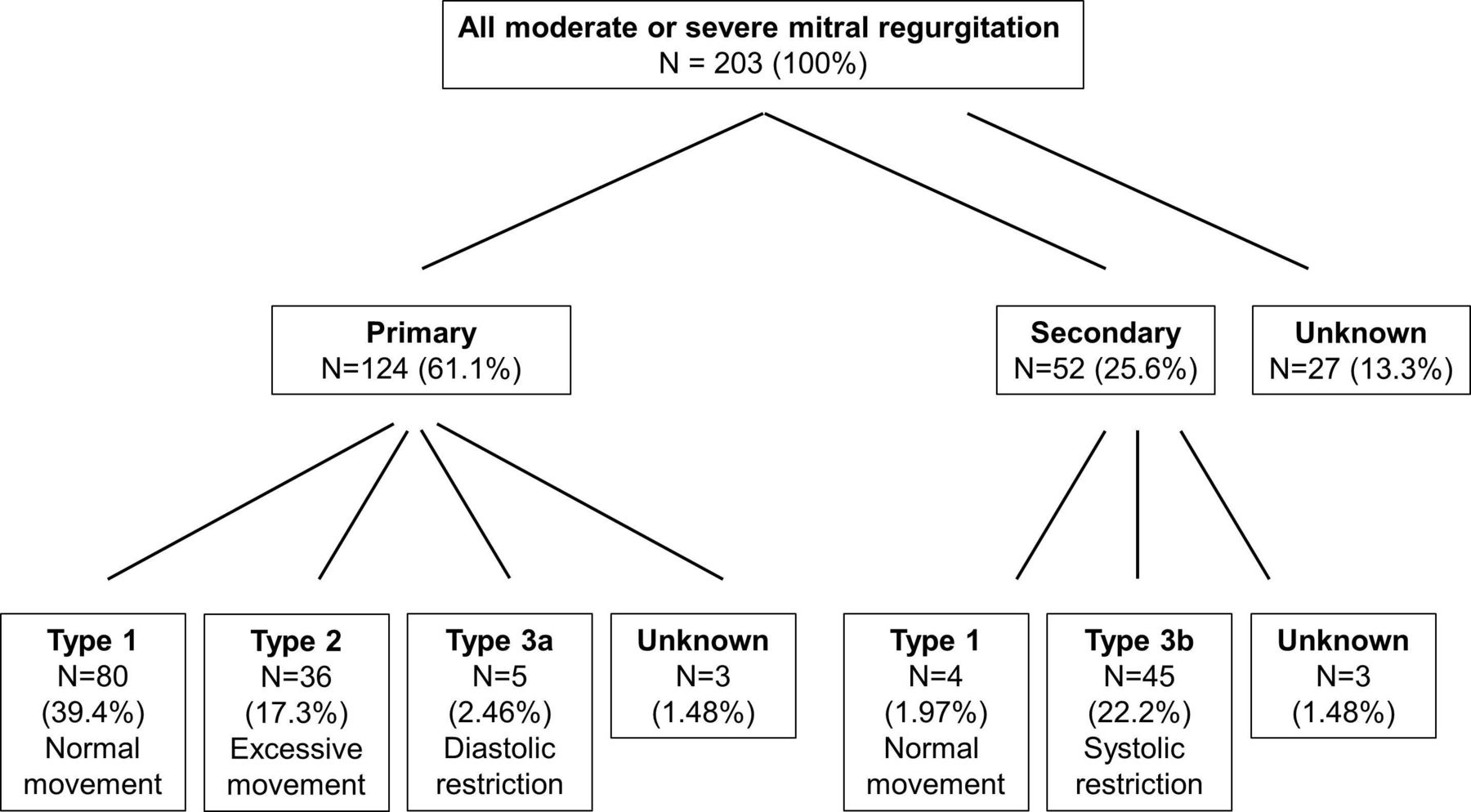
Mechanism of mitral regurgitation (MR). The mechanisms of valve dysfunction in patients with moderate or greater MR are shown, according to Carpentier classification. Type 1, normal leaflet motion and position; type 2, excess leaflet motion; type 3a, restricted leaflet motion in systole and diastole; type 3b, restricted leaflet motion in systole.
In an editorial, Bouleti and Iung7 point out that the prevalence of MR and TR increases even further in those over age 75 years and that the number of patients with secondary MR and a low left ventricular ejection fraction is of concern given the association with impaired long-term survival. They conclude: ‘These findings highlight the need for educational programmes to increase the awareness on heart valve disease, for evaluation of the adherence to guidelines and for the continuous development and evaluation of less invasive interventions targeting elderly patients.’
The Education in Heart article in this issue summarises the recommended approach to screening for cardiovascular disease in healthy individuals.8 A state-of-the-art review article on nuclear cardiology9 provides an overview of myocardial perfusion imaging techniques and clinical applications for ischaemic heart disease, heart failure, and myocardial disease and infection. Newer nuclear imaging approaches include 18F-fluorodeoxyglucose positron emission tomography scans for diagnosis of infective endocarditis, particularly in patients with prosthetic valves, and the use of nuclear approaches as adjuncts for the diagnoses of sarcoidosis and amyloidosis.
Our Cardiology in Focus series continues with an article10 on pregnancy during cardiology training which will be helpful for women considering pregnancy during cardiology training (or as a consultant cardiologist) for those providing training and support to those women (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Concerns of the pregnant cardiologist.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Commissioned; internally peer reviewed.