Article Text

Abstract
The success of cardiac surgery has transformed the prospects of children with congenital heart disease with over 90% now surviving to adulthood. The early pioneering surgeons took on significant risk, whilst current surgical practice emphasises safety and consistency. In this article we review important British contributions to the field and consider challenges for the future, specifically how to better manage and reduce the adverse sequelae of congenital cardiac surgery by continuing to innovate safely.
- cardiac surgical procedures
- heart defects, congenital
- heart transplantation
Statistics from Altmetric.com
Introduction
The first successful intracardiac operation in the UK was performed in 1925 by Henry Souttar, accessing the mitral valve via the left atrial appendage and using his forefinger to carry out mitral commissurotomy1 (figure 1). 2 Of the 10 patients undergoing surgery for mitral stenosis between 1922 and 1928, this was one of only two who survived the perioperative period.2 3 Further attempts were abandoned and the risks of cardiac surgery were deemed unjustifiable. In 1946 the cardiologist Maurice Campbell at Guy’s Hospital observed that cyanotic congenital heart disease ‘sometimes seems a dull subject because of the lack of treatment for this condition, so there is a feeling that it does not much matter about the diagnosis’.4
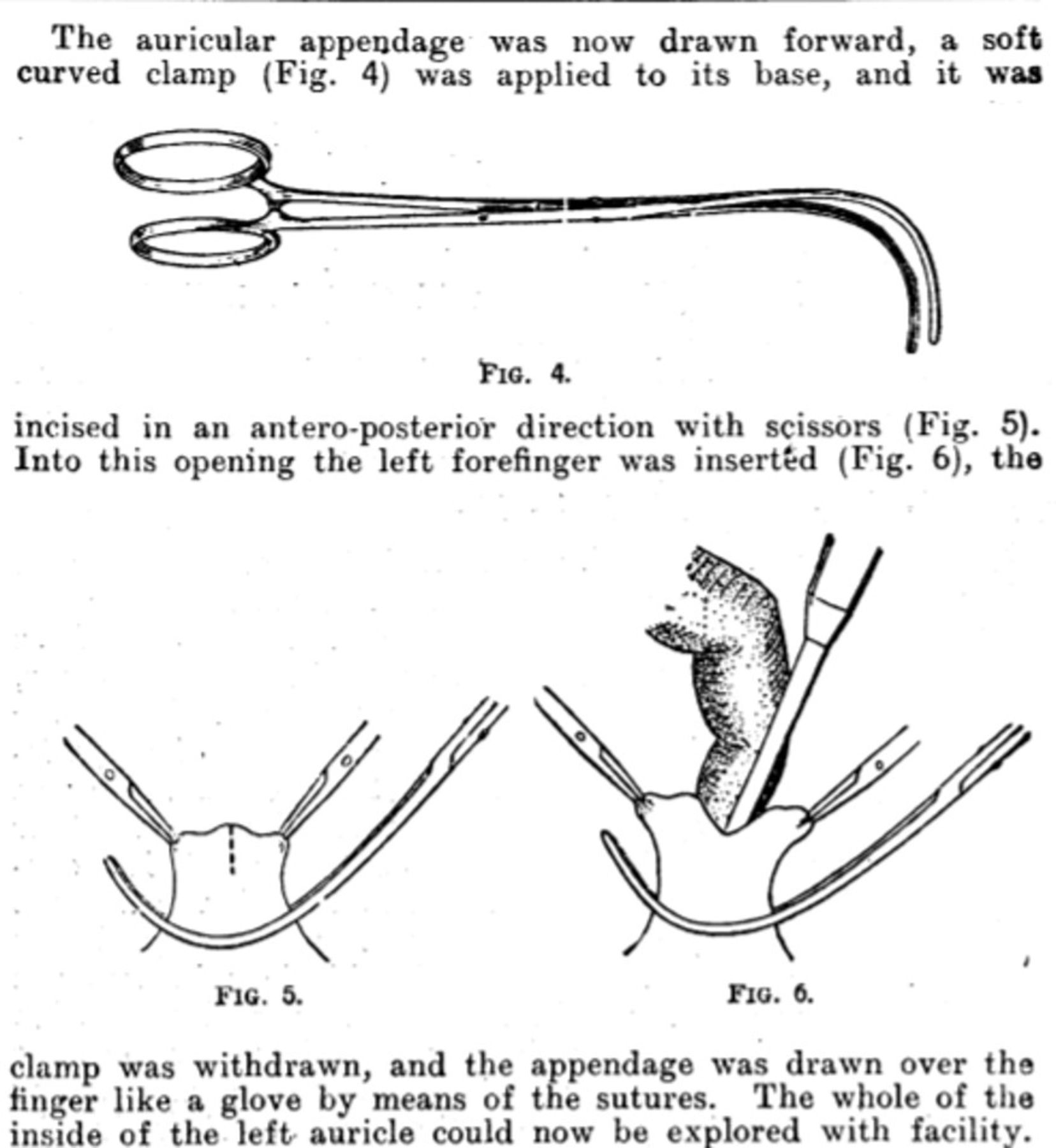
Excerpt from Henry Souttar’s description of the first mitral commissurotomy in the UK. Reproduced from the British Medical Journal, The surgical treatment of mitral stenosis, Souttar, HS. 2:603–6. Copyright 1925 with permission from BMJ Publishing Group. In response to Dwight Harken’s question ‘Why did you not repeat that magnificent operation?’ he wrote: ‘I did not repeat the operation because I could not get another case. Although my patient made an uninterrupted recovery the Physicians declared that it was all nonsense and in fact that the operation was unjustifiable’.49
Set against this background, developments in cardiac surgery and management of congenital heart disease over the past 100 years have been nothing short of astonishing. Testament to this is the emergence of the adult congenital heart disease (ACHD) population, which now exceeds the paediatric congenital heart disease population in Western countries.5 Pioneering surgeons and patients took on significant risk, with frequent setbacks and high early failure rates following introduction of new procedures. Current cardiac surgery emphasises safety, consistency and maximising benefit. Key challenges for the future include how to manage the long-term sequelae of surgery in the ACHD population and how to continue surgical innovation and ‘pioneer safely’ to reduce these sequelae and improve long-term outcomes.
Extracardiac surgery
In 1938 Robert Gross performed the first ligation of a patent ductus arteriosus in Boston,6 heralding the advent of extracardiac surgical procedures (figure 2). The first successful duct ligation in the UK was reported a year later in 1939 by Oswald Tubbs at St Bartholomew’s Hospital.7 This was followed in 1944 by resection of coarctation of the aorta with end-end anastomosis by Crafoord and Nylin8 in Stockholm and the development of the Blalock-Taussig shunt at John Hopkins in Baltimore.9

Timeline of landmark procedures in cardiac surgery and congenital heart disease. ASD atrial septal defect; AVR aortic valve replacement; AVSD atrioventricular septal defect; MVR mitral valve replacement; PDA patent ductus arteriosus; VSD ventricular septal defect.
Closed direct cardiac surgery
Despite the success of these early extracardiac procedures, scepticism remained about the safety of intracardiac surgery. In a ‘proof of concept’ moment, the American surgeon Dwight Harken successfully removed bullets and shrapnel from the hearts of 56 soldiers injured on D-day without a single death.10
This paved the way for a new era of closed direct cardiac surgery in which the cardiologist Maurice Campbell and the surgeon Russell Brock played pivotal roles4 (figure 3). Campbell was an early member of the Cardiac Club and President of the British Cardiac Society from 1956 to 1960. He was also one of the first editors of the British Heart Journal.11 In 1947 Campbell and Brock hosted Alfred Blalock at Guy’s Hospital. During his visit Blalock performed 10 of his shunt operations on cyanotic children with tetralogy of Fallot.4 The prognosis for children with cyanotic congenital heart disease was known to be particularly poor and this transformational procedure demonstrated that it was possible to relieve cyanosis and improve outcome by augmenting pulmonary blood flow. This paradigm shift, combined with Harken’s work supporting the feasibility of intracardiac surgery, inspired Brock, Campbell and Thomas Holmes Sellors to pioneer a new approach to enhancing pulmonary blood flow by direct pulmonary valvotomy12 (figure 4).

Maurice Campbell (left). Reproduced from the British Heart Journal, Maurice Campbell, Shirley Smith, K, 34:1–2. Copyright 1972 with permission from BMJ Publishing Group. Russell Brock (right). Reproduced with kind permission from William Edwards, Curator of the Gordon Museum, GKT Medical School, King’s College London. Brock described the plight of children with cyanosis who ‘have been almost hidden away in all parts of the country, not through any deliberate policy of concealment, but because many are necessarily, from their disability, confined to the house or to their room for the whole or the greater part of their lives’.50

Brock’s pulmonary valve dilator. Reproduced with permission from the British Cardiovascular Society archive. Brock’s eponymous procedure for treatment of pulmonary stenosis comprised right ventriculotomy, infundibular resection and pulmonary valvotomy. In response to objections raised about this direct approach, Brock wrote: ‘By timorous meditation we arouse fear and postpone success… The essential fundamental is the stenosed valve which holds up the passage of blood; the relief of this stenosis must be the ideal to be aimed at’.12
In 1948 Brock and Campbell formed the Peacock Club at Guy’s Hospital, regularly convening cardiologists, surgeons, pathologists and radiologists to discuss cases and research in congenital heart disease.4 This multidisciplinary approach was unusual but came to characterise the management of congenital heart disease in the UK. The minutes of these meetings are held in the British Cardiovascular Society Archive. It is worth recalling that echocardiography did not come into use until the 1960s, so the role of the pathologist in presenting necropsy specimens was crucial in advancing clinicians’ understanding of congenital heart disease.
Cardiopulmonary bypass and the development of open intracardiac surgery
The next challenge was to conceive a method of opening the heart to allow surgeons to operate under direct vision while maintaining end organ perfusion. In 1953 John Gibbon successfully employed his heart-lung machine to facilitate repair of a large atrial septal defect in an 18-year-old patient in Philadelphia.13 Of his first four patients, this was the only survivor.14
In London, Dennis Melrose developed a heart-lung machine using rotating discs to expose a thin layer of blood to oxygen (figure 5). This was used by William Cleland and the Hammersmith Hospital team to perform the first cardiopulmonary bypass operation in the UK in 1953.15 Like Gibbon, their initial foray was not encouraging. The first patient survived a closed aortic valvotomy, but of their six subsequent patients only one survived, and work on human patients came to a temporary halt. Following a visit to Kirklin and Lillehei in the USA, they restarted the programme in 1957, this time with success. Their first patient, a woman with an atrial septal defect, was still alive and well 25 years later.16 They went on to produce the first commercially available heart-lung machine (H Bentall, personal communication, 2021).

Pump oxygenator using the rotating disc principle perfected at the Postgraduate Medical School and first applied clinically in 1954. Reproduced from Postgraduate Medical Journal, Types of heart-lung machines used in extra-corporeal circulation, Melrose, DG, 37:639–645. Copyright 1961 with permission from BMJ Publishing Group. Please note that the subject in the picture is not identified in the original publication.
The development of cardiopulmonary bypass resulted from the convergence of technological, pharmacological and surgical developments extending over many years, including the discovery and clinical application of heparin.17 Further advances followed, with Ken Taylor playing a key role in defining the pathophysiological effects of cardiopulmonary bypass, leading to refinements in the 1980s.18
The use of the heart-lung machine paved the way for increasingly complex intracardiac procedures under direct vision. The next challenge was to find a way of safely inducing reversible cardiac arrest (cardioplegia) to create a motionless and bloodless operating field without causing cardiac ischaemia or risking air embolism.
1955 was pivotal. Dennis Melrose, Hugh Bentall and colleagues at the Hammersmith Hospital had reported reversible cardiac arrest using potassium citrate infusion in dogs.19 Stopping the heart was ethically controversial, but following approval by church leaders, an application for use in humans was approved (H Bentall, personal communication, 2021). This original technique was abandoned in the USA in the 1960s due to concerns about myocardial damage, but the principle was sound. Subsequent work by Braimbridge and Hearse at St Thomas’ Hospital led to a revival of potassium-based cardioplegia and their ‘St Thomas’ Cardioplegic Solution’ is still widely used today.16 20
Expansion of cardiac surgery
The 1960s and 1970s witnessed a vast expansion in cardiac surgery facilitated by advances in cardiopulmonary bypass, circulatory arrest and deep hypothermia. Heart valve technology improved and valve replacements became commonplace. Important work on the preparation of aortic homografts was carried out by Carlos Duran and Alfred Gunning in Oxford. They devised a technique for implanting aortic valves in the subcoronary position in dogs.21 In 1962 Donald Ross performed the first successful subcoronary implantation of an aortic homograft in humans.22 Working alongside the cardiologist Jane Somerville in 1967, he pioneered the eponymous Ross procedure, in which a pulmonary autograft is used to replace a diseased aortic valve and the pulmonary valve is replaced with a homograft23 (figure 6). This remains an incredibly valuable option for young patients requiring aortic valve replacement, with the pulmonary autograft offering improved longevity and potential for growth without need for anticoagulation.

Excerpt from Donald Ross’ seminal publication describing aortic valve replacement with a pulmonary autograft. Reprinted from The Lancet, vol 290, issue 7523, Ross DN, Replacement of mitral and aortic valves with pulmonary autografts, 956–958. Copyright (1967), with permission from Elsevier.
This era also witnessed key advances in the management of transposition of the great arteries (TGA) (figure 7). Senning and Mustard pioneered ‘physiological correction’ with atrial switch in 1959 and 1963, respectively.24 ‘Anatomical correction’ with arterial switch followed in 1975.25

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Schematic representation of transposition of the great arteries (A), ‘physiological correction’ with atrial switch (B) and ‘anatomical correction’ with arterial switch (C). LV left ventricle; RV right ventricle.
The technical demands of the arterial switch were immense, not least because, in addition to switching the great arteries, the coronary arteries had to be detached and reimplanted on to the neoaortic root. Performing such intricate surgery on neonatal hearts and providing appropriate perioperative neonatal care was incredibly challenging. However, if the ventricular septum was intact, waiting for the child to grow ran the risk of the left ventricle ‘deconditioning’ and becoming incapable of supporting systemic circulation. Magdi Yacoub, a recipient of the British Cardiovascular Society Mackenzie Medal, pioneered a two-stage arterial switch at Harefield Hospital in 1977. This comprised pulmonary arterial banding in the neonatal period to prevent deconditioning of the left ventricle, followed by arterial switch at 6 months.26 This was superseded by a single-stage arterial switch performed in the neonatal period, pioneered by Castaneda and Norwood in Boston in 1984.27 In a landmark paper, Marc de Leval, a key exponent of the procedure in the UK, analysed a cluster of failures that he experienced with this difficult technique. He subsequently retrained and demonstrated improvement in his results. This paper highlighted the importance of monitoring personal surgical outcomes and the role of humility in the pursuit of excellence.28
This was brought into sharp relief when concerns were raised about paediatric cardiac surgical results in Bristol in the early 1990s. This led to a 3-year major public enquiry in the English National Health Service. A key plank of the enquiry’s recommendations was that surgeons should know and publish their results.29 This led ultimately to the formation of comprehensive national outcomes databases in adult and congenital cardiac surgery, arrhythmia management and interventional cardiology, with the aim of facilitating quality improvement.
Cardiac transplantation
British surgeons have made a rich and pioneering contribution to heart and lung transplantation. Following the world’s first heart transplant in 1967 in Cape Town, Donald Ross carried out the first heart transplant in the UK. The first patient survived for just 46 days before succumbing to infection. The next two transplants were also unsuccessful due to failure to control rejection.30 Shortly afterwards the UK Government announced a moratorium which lasted more than a decade.
Two things changed in the 1970s. First was the advent of immunosuppressant drugs and transvenous endomyocardial biopsy using a bioptome for the early diagnosis of heart transplant rejection. The latter was developed by the Irish surgeon Philip Caves whilst a visiting research fellow under Norman Shumway at Stanford University.31 Second, in 1976 the Medical Royal Colleges in the UK confirmed that brainstem death, rather than cardiac arrest, could be considered as death of the donor.32
The UK’s heart transplant programme was relaunched in 1979 by Terence English at Papworth Hospital and a few months later by Magdi Yacoub at Harefield Hospital, both of whom had worked with Ross.16 John Wallwork at Papworth Hospital performed Europe’s first successful heart-lung transplant in 1984 and performed the world’s first heart-lung and liver transplant in 1986 alongside Roy Calne, the father of ciclosporin. Tim Higenbottam pioneered endobronchial biopsy for lung transplantation at Papworth Hospital. Chris McGregor performed the first successful lung transplant in the UK in 1987, followed by the first successful infant heart transplant in the UK in 1988, putting the Freeman Hospital in Newcastle on course to be a major international influence.33 Simultaneously, Magdi Yacoub pioneered the ‘Domino procedure’, in which a patient with failing lungs, usually due to cystic fibrosis, received the heart and lungs from a donor, while another patient received the good heart from the first patient.34
In 1988 Great Ormond Street Hospital started paediatric heart transplantation with Marc de Leval and Martin Elliott, initially mentored by and funded through the Papworth network, and rapidly grew to become one of the largest paediatric heart transplantation centres in the world.
Advances in perioperative care
In the early years, perioperative care was provided by the surgeons and anaesthetists in side rooms off cardiac wards and adult intensive care units. The expansion of cardiac surgery stimulated the development of dedicated paediatric cardiac intensive care units, led by specialised intensivists and supported by vital developments in cardiac monitoring, bedside imaging, pharmacology and mechanical ventilation.
The discovery that prostaglandin could be used to maintain patency of the ductus arteriosus in 1973 was revolutionary.35 This allowed time to stabilise neonates with duct-dependent pulmonary circulation and prepare them for a surgical shunt, rather than having to rush them to surgery in unstable condition. It also facilitated surgical repair of lesions with duct-dependent systemic circulation, such as interrupted aortic arch and hypoplastic left heart disease, which are rapidly fatal if untreated.
Advances in imaging
Early surgery was hampered by limited diagnostic techniques, relying principally on clinical skills and catheterisation. Of the first four patients on whom Gibbon operated with his heart-lung machine, two died in relation to inaccurate preoperative diagnoses.14 The advent of echocardiography, first M mode in the 1960s, then two-dimensional echo in the 1970s, facilitated improved accuracy of diagnosis. This was further enhanced in the 1980s by cardiac MRI and cardiac CT. The emergence of antenatal diagnosis with fetal echocardiography in the 1980s enabled careful planning of the delivery and postnatal care of affected children.
Advances in imaging were underpinned by the development of the sequential segmental approach to cardiac morphology, resulting from collaboration between Robert Anderson, Fergus Macartney, Elliot Shinebourne and Michael Tynan in London.36 This made complex congenital heart disease easier to understand and communicate and led ultimately to the development of an international, unified nomenclature, vital for successful registries.37 Rodney Franklin at the Royal Brompton Hospital provided important leadership in this painstaking project.
Adult congenital heart disease
The success of these developments in cardiac surgery created a growing population of adult patients with congenital heart disease. The cardiologist Jane Somerville provided powerful advocacy for these patients, describing their specific medical, social and psychological needs.38 In 1975 she established the first dedicated ward for adolescent patients with congenital heart disease at the National Heart Hospital, named after the eminent cardiologist Paul Wood, and this developed into a dedicated Grown Up Congenital Heart Disease Unit.39 In 2002 she chaired the British Cardiac Society Working Party for Grown Up Congenital Heart Disease, setting out a framework for a national integrated service, centralising care of complex patients into dedicated regional units.40
Percutaneous intervention
Developments in cardiac surgery have been matched by dramatic advances in transcatheter interventions. The development of balloon atrial septostomy by Rashkind and Miller in 196641 was followed by an explosion of new transcatheter interventions in the 1970s and 1980s, including closure of shunts (atrial septal defects, ventricular septal defects and patent ductus arteriosus) and relief of obstructive lesions (valvar stenoses and coarctation). Percutaneous pulmonary valve implantation, an important tool in the management of pulmonary regurgitation following repair of tetralogy of Fallot, was first reported by Philip Bonhoeffer in 2000.42 This was followed by transcatheter aortic valve implantation in 2002.43
Current status and future perspective
The success of paediatric cardiac interventions presents new challenges, namely how to improve the quality and quantity of life for those surviving into adulthood. They currently face reduced life expectancy and increased morbidity from heart failure, arrhythmia, pulmonary vascular disease, endocarditis and repeat surgery. These problems may arise from lesions pertaining to their original diagnosis, or as sequelae of their previous surgery.
In contemplating the future of cardiac surgery and congenital heart disease there are two key challenges to consider.
The first challenge is to improve treatment of the sequelae of cardiac surgery and residual lesions. Heart failure is a major problem and represents the leading cause of death in patients with ACHD.44 Treatment is difficult, particularly in patients with functionally single ventricle and systemic right ventricle, for whom there is currently a paucity of evidence-based therapies. Patients with ACHD face significant barriers to transplantation. Following transplantation they face higher early mortality but better long-term survival compared with patients with other pre-transplant conditions.45 In the UK there is a severe discrepancy between the predicted number of transplants for patients with congenital heart disease and the number of patients with congenital heart disease presenting with advanced heart failure.46 There is a pressing need for improved access to organs and mechanical support.
The second challenge is to reduce the burden of postoperative sequelae and residual lesions. One such success was the replacement of the atrial switch with the arterial switch for treatment of TGA. The atrial switch dramatically improved survival prospects for infants with TGA but conferred unfavourable long-term sequelae, including a systemic right ventricle and high risk of atrial arrhythmias. This was superseded by the technically demanding arterial switch, which in the current era has superior outcomes and has consequently rendered the atrial switch almost obsolete. Nonetheless, for the first 10 years following its introduction, reported mortality was higher with the new arterial switch compared with the established atrial switch.47 In a landmark study, Catherine Bull and colleagues48 at Great Ormond Street demonstrated this period of increased hazard to patients during the introduction and learning of a new procedure. This raises questions as to how we can continue to innovate in order to maximise benefit to the wider population, while minimising risk to the individual.
Conclusion
The outlook for patients with congenital heart disease has transformed over the past 100 years, from a time when no treatment could be offered and few survived until adulthood, to a time when a vast armoury of surgical and transcatheter interventions ensure that few do not survive into adulthood. This presents a set of new challenges for the future.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Acknowledgments
The authors would like to thank Professor Tom Treasure for his constructive critique of the manuscript.
References
Footnotes
Contributors JCE-SL and BK planned the article. JCE-SL wrote the initial draft. BK, MJE and JW contributed original material and critical revisions of the manuscript. BK is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JW is Chairman of the Royal Papworth Hospital NHS Foundation Trust. BK is Chairman of Birmingham Women’s and Children’s NHS Foundation Trust and a trustee of the British Cardiovascular Society.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Commissioned; externally peer reviewed.