Article Text

Abstract
Objectives To evaluate the effectiveness of interventions to improve shared decision making (SDM) in cardiology with particular focus on patient-centred outcomes such as decisional conflict.
Methods We searched Embase (OVID), the Cochrane library, PubMed and Web of Science electronic databases from inception to January 2021 for randomised controlled trials that investigated the effects of interventions to increase SDM in cardiology. The primary outcomes were decisional conflict, decisional anxiety, decisional satisfaction or decisional regret; a secondary outcome was knowledge gained by the patients.
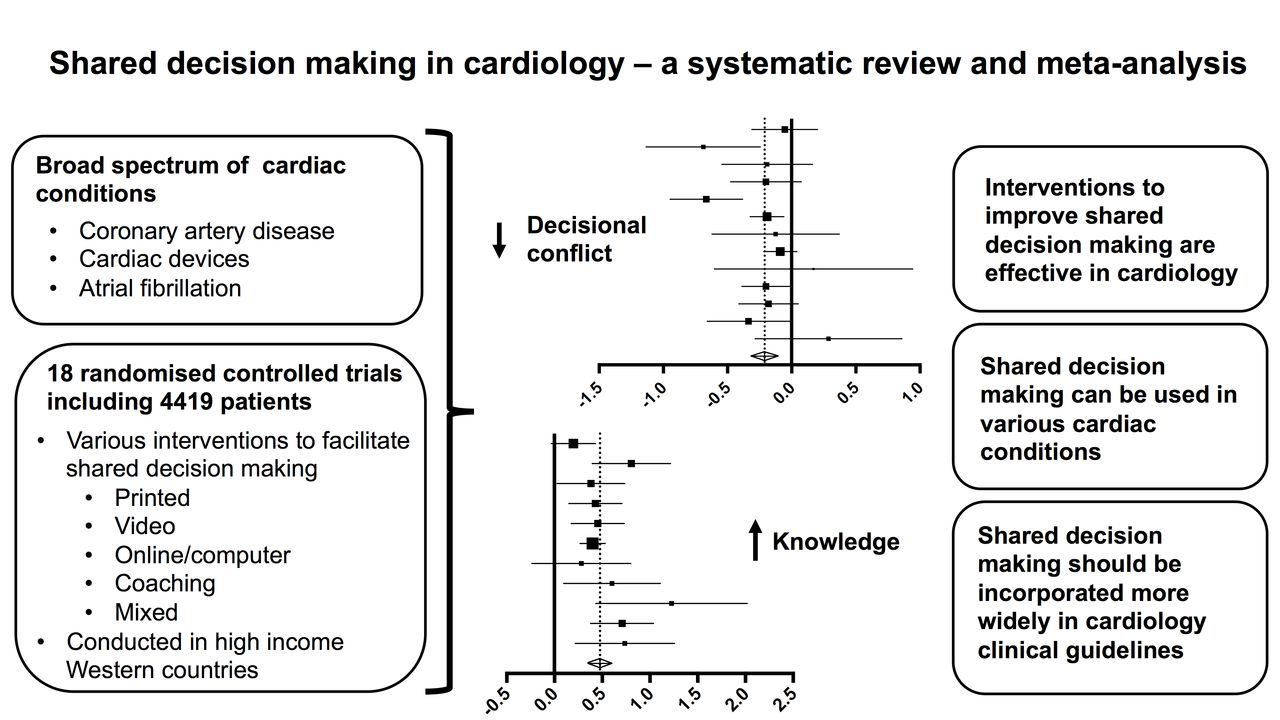
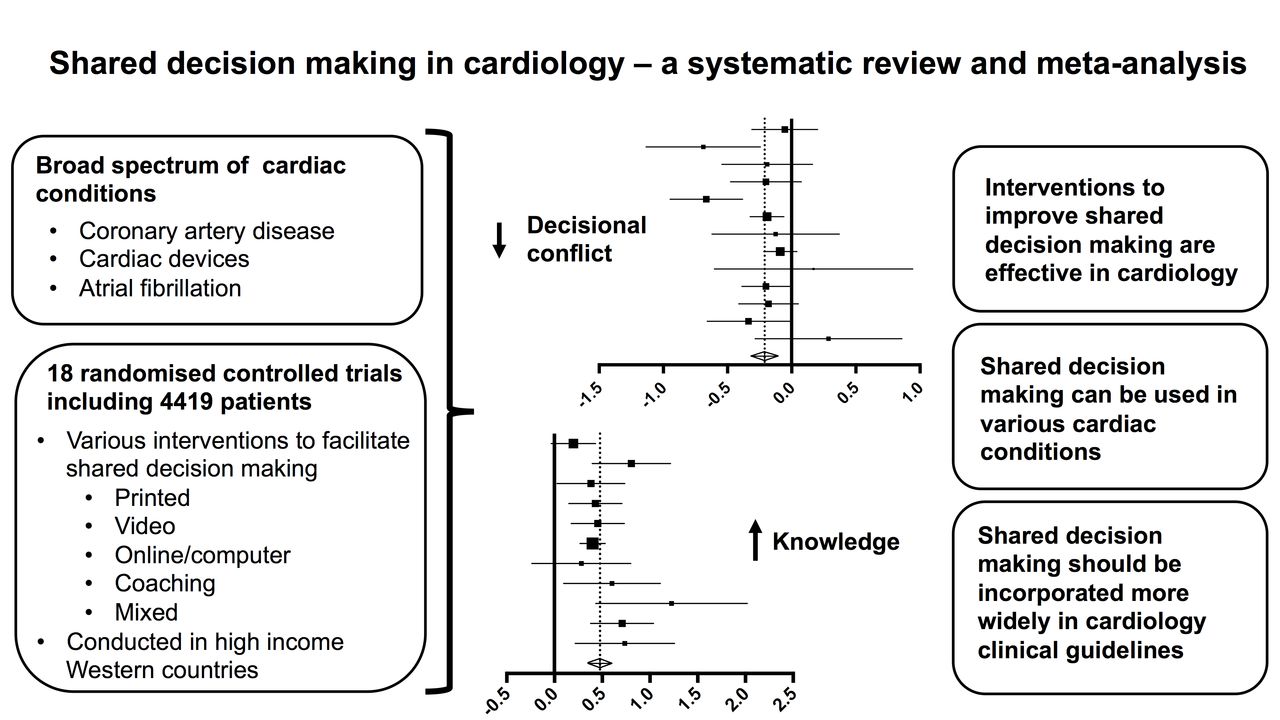
Results Eighteen studies which reported on at least one outcome measure were identified, including a total of 4419 patients. Interventions to increase SDM had a significant effect on reducing decisional conflict (standardised mean difference (SMD) −0.211, 95% CI −0.316 to −0.107) and increasing patient knowledge (SMD 0.476, 95% CI 0.351 to 0.600) compared with standard care.
Conclusions Interventions to increase SDM are effective in reducing decisional conflict and increasing patient knowledge in the field of cardiology. Such interventions are helpful in supporting patient-centred healthcare and should be implemented in wider cardiology practice.
- meta-analysis
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Shared decision making (SDM) is a joint process in which a healthcare professional works together with a person to reach a decision about care. The effectiveness of interventions to increase SDM in various specialties has been demonstrated. SDM has been applied in cardiology, and there are a number of randomised controlled trials (RCTs) testing its effects on a variety of clinical situations.
WHAT THIS STUDY ADDS
We perfomed a systematic review and meta-analysis of the RCTs that examine the application of SDM in cardiology and more specifically its effects on decisional conflict, decisional anxiety, decisional regret, decisional satisfaction and knowledge. This is the first meta-analysis to address this question. Overall, we showed that interventions which aim to increase SDM are effective in cardiology.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Evidence for the effectiveness of SDM in cardiology may help change attitudes towards this patient-centred framework and facilitate its recommendation in clinical guidelines.
Introduction
Shared decision making (SDM) has been defined as ‘an approach where clinicians and patients share the best available evidence when faced with the task of making decisions, and where patients are supported to consider options, to achieve informed preference’.1
SDM is considered desirable and effective as a policy choice to facilitate the right of involvement for patients, to allow patients to take an active role in decisions regarding their health, to reduce overuse of treatment options without clear benefit, to reduce healthcare practice variations, as well as to improve sustainability of the healthcare system by supporting patient ownership of their care.2
Although SDM is specifically recommended for certain clinical scenarios in cardiology, such as implantable cardioverter defibrillator (ICD) insertion,3 the uptake in cardiac clinical guidelines is uneven,4 5 presumably at least partly due to lack of evidence of its effect across the spectrum of cardiology.
We conducted this systematic review and meta-analysis of randomised controlled clinical trials to investigate the effectiveness of interventions to facilitate SDM in cardiology. Accumulating evidence on the effectiveness of SDM in cardiology may help inform clinical guidelines in cardiology and thereby help change attitudes towards this patient-centred approach.
Methods
Protocol
A protocol for this study explicitly stating defined objectives, criteria for study selection, assessment criteria for included studies and data extraction was developed. The protocol was prospectively registered with the International Prospective Register of Systematic Reviews and has been allocated the registration number CRD42021290164 (www.crd.york.ac.uk/prospero). We present our findings according to the reporting guidelines for meta-analyses and systematic reviews of randomised controlled trials (RCTs) as outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (online supplemental file).
Supplemental material
Database search
We searched Embase (OVID), the Cochrane library, Pubmed and Web of Science from Inception to January 2021. Search strategies were adapted from Légaré et al 2 for the SDM aspect of the search, modified to make the search cardiology specific, and adjusted according to requirements of each database (online supplemental file). The search strategy for Embase, as a representative example, is shown as follows:
(shared decision or sharing decision or informed decision or informed choice or decision aid).ti,ab. or ((share* or sharing* or informed*) and (decision* or deciding* or choice*)).ti. (22530).
exp clinical decision making/ or exp decision making/ or exp decision support system/ or exp ethical decision making/ or exp family decision making/ or exp medical decision making/ or exp patient decision making/ or (decision making or decision support or choice behaviour).ti,ab. or ((decision* or choice*) and (making* or support* or behaviour*)).ti. (477532).
exp patient participation/ or (patient participation or consumer participation or patient involvement or consumer involvement).ti,ab. or ((patient* or consumer*) and (involvement* or involving* or participation* or participating*)).ti. (43913).
exp doctor patient relation/ or exp nurse patient relationship/ or exp nurse/ or exp physician/ or (nurse* or physician* or clinician* or doctor* or general practitioners or gps or healthcare professionals or healthcare professionals or healthcare providers or healthcare providers or resident*).ti,ab. (2129607).
exp patient/ or (patient* or consumer* or people*).ti. (4653143).
4 and 5 (587332).
1 or (2 and 3) or (2 and 6) or (3 and 6) (66880).
“random*".ab,kw,ti. (1632000).
(Myocard* or Arrhythm* or Valv* or Fibrill* or Tachycard* or Bradycard* or Heart or Angin* or Coronar* or Ischaemi* or Ischemi* or Card* or Aort* or Mitral or Vascular or Infarct* or Conduction or Channelopathy or “Diastolic dysfunction” or “Systolic dysfunction” or Atri* or Ventric* or Palpitatio* or Arter* or Hypertensi* or Cardiac pac* or Pacemaker or Endocarditis or electrocardiogra* or electrophysiolog*).ab,kw,ti. (4990709).
7 and 8 and 9 (1300).
Study selection and data extraction
Two reviewers (PM and NG-H) independently screened titles and abstracts. Relevant studies were retrieved in full text and assessed for eligibility. Studies which were only available as abstract were excluded. Discrepancies between the two reviewers were resolved by discussion or through involvement of up to two further reviewers (JR and CP). Only RCTs assessing the effects of an intervention to increase SDM in cardiology were included.
Two reviewers used a data collection form to extract available data (PM and NG-H) including clinical setting, study population and geographical location, clinical condition, details on intervention under investigation, as well as endpoints and their associated collection time points. Study methodological quality was assessed independently by two reviewers (PM and NG-H) using a standardised tool.6 Potential bias was classed as high, low or unclear, and discrepancies were resolved through discussion between reviewers.
The primary outcomes of decisional conflict, decisional anxiety, decisional regret and decisional satisfaction were chosen as patient-centred outcome measures as preliminary searches showed these to be the most coherently reported. A summary of the instruments used to assess these outcomes is provided in online supplemental tables S6 and S7. If primary outcomes were reported at multiple follow-ups, data from the last follow-up were used for the meta-analysis. A predefined secondary outcome was knowledge gained by the patient, assessed at the earliest opportunity following intervention. Studies that only reported on the secondary outcome without investigating effects on the primary outcomes were excluded.
Data analysis
Data were analysed in OpenMeta(Analyst) software V.10.12 (developed by the Center for Evidence Synthesis, Brown University, School of Public Health, Rhode Island State, USA) and Meta-Essentials tool for Microsoft excel7 and plotted using GraphPad Prism. A continuous random-effects model was used to calculate summary estimates, and data were presented as standardised mean differences (SMDs) with 95% CIs. Only data available from published studies were used. If studies reported on means with CIs, corresponding SDs were calculated to generate SMDs. Where studies reported only on means and estimation of SD was not possible, data were excluded. Interstudy heterogeneity was assessed using the I2 statistics, where values above 50% were considered significant. We planned to assess publication bias visually and by funnel plot if at least 10 studies reported on any outcome measure.
The following predefined subgroup analyses were planned on the primary outcome decisional conflict if sufficient data were available: (1) different cardiac condition or subspecialty, for example, atrial fibrillation, cardiac device implantation and chest pain/intervention; and (2) different strategies to improve SDM, for example, video format, computer/online information sheets and printed patient information. We planned to conduct sensitivity analyses to test the robustness of the data.
Patients and the public have not been involved in the design and conduct of this systematic review and meta-analysis.
Results
Our search identified 9245 titles and abstracts for screening, of which 159 articles were assessed in full text (figure 1). Eighteen RCTs reporting on 4419 patients were included in this systematic review and meta-analysis (tables 1 and 2, online supplemental table S5). The included trials were modest in size with the exception of Hess et al 8 and Kunneman et al,9 reporting on 898 and 922 patients, respectively. Trials were conducted exclusively in high-income countries, including the USA (Allen et al,10 Case et al,11 Coylewright et al,12 Doll et al,13 Fraenkel et al,14 Hess et al,15 Hess et al,8 Kostick et al,16 Kunneman et al 9 and Thomas et al 17), UK (Thomson et al 18) and Canada (Carroll et al,19 Holbrook et al,20 Lewis et al,21 Man-Son-Hing et al,22 McAlister et al,23 Morgan et al 24 and Schwalm et al 25). No trials were conducted in low-income or middle-income countries.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram.
Characteristics of included studies
Outcomes of included studies
A broad range of clinical conditions in cardiology were covered, including atrial fibrillation and anticoagulation (Fraenkel et al,14 Hoolbrook et al,20 Kunneman et al,9 Man-Son-Hing et al,22 McAlister et al 23 and Thomson et al 18), chest pain and coronary artery disease (Case et al,11 Coylewright et al,12 Doll et al,13 Hess et al,15 Hess 8 et al and Morgan et al 24), cardiac devices and pacemakers (Carroll et al,19 Lewis et al 21 and Thomas et al 17), as well as advanced treatment options, including left ventricular assist devices (Allen et al 10 and Kostick et al 16). Included trials used a variety of formats in patient decision aids to improve SDM, including printed aids (Allen et al,10 Carroll et al,19 Coylewright et al,12 Hess et al,15 Hess et al,8 Holbrook et al,20 Kostick et al,16 Lewis et al,21 McAlister et al,23 Man-Son-Hing et al,22 Morgan et al 24 and Schwalm et al 25), audiotapes (Holbrook et al,20 McAlister et al 23 and Man-Son-Hing et al 22), video (Allen et al,10 Morgan et al 24 and Thomas et al 17), coaching (Lewis et al 21) and online/computer programs (Case et al,11 Doll et al,13 Fraenkel et al,14 Holbrook et al,20 Kunneman et al 9 and Thomson et al 18). Details of reviewers’ structured assessment of methodological quality of included studies6 are shown in table 3.
Risk of bias assessment of included studies
Thirteen RCTs reported data from 3738 patients on decisional conflict using a decision conflict scale that could be included in the meta-analysis. None of the included studies was considered as having low risk of bias across the domains assessed (table 3). Interventions to increase SDM had a significant effect on reducing decisional conflict (SMD −0.211, 95% CI −0.316 to −0.107) compared with standard care (figure 2). A moderate degree of heterogeneity was observed (I2=49.02%), which in part may be explained by the wide range of cardiac conditions and interventions to improve SDM that were included. The largest effects were observed in studies reported by Hess et al 15 and Carroll et al 19 reporting on the use of decision aids in decision making concerning chest pain and ICD insertion, respectively, driving the degree of overall heterogeneity. However, no single clinical condition or intervention to improve SDM was identified that could explain the heterogeneity across studies. Prespecified subgroup analysis, stratified based on clinical condition and examining different formats of patient decision aids suggest effectiveness of SDM across the broad spectrum of cardiology and through the use of various modalities (online supplemental file). Leave-one-out sensitivity analysis confirmed the robustness of the reported data (online supplemental file). Funnel plot analysis did not suggest significant publication bias (figure 3).

Effect of interventions to increase shared decision making on decisional conflict. Standardised mean difference of decisional conflict score is shown. Weights are derived from the random-effects model.

Funnel plots for decisional conflict and knowledge.
Eleven RCTs reported data on 2210 patients on patient knowledge assessed through use of various questionnaires with relevance to the cardiology condition under investigation. There was modest heterogeneity (I2=37.61%) in the included studies, and a significant increase of knowledge was reported (SMD 0.476, 95% CI 0.351 to 0.600, figure 4; funnel plot, figure 3).

Effect of interventions to increase shared decision making on patient knowledge. Standardised mean difference of knowledge score is shown. Weights are derived from the random-effects model.
Decisional regret was quantitatively reported in only two RCTs and decisional satisfaction in three RCTs (table 2 and online supplemental table S5) and meta-analysis was therefore not performed.
Discussion
We found considerable evidence to support the use of interventions to improve SDM in cardiology (figure 5). Use of such interventions reduced decisional conflict and increased patient knowledge. There was not enough evidence to conclude on the effects of such interventions on patient satisfaction or decisional regret.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Graphical summary.
In this protocol-driven, prospectively registered systematic review, we conducted a comprehensive search strategy and included only randomised controlled clinical trials allowing us to report on the highest level of evidence. A broad range of cardiology topics was included in the clinical trials assessed, and we aimed to analyse multiple outcomes with relevance to SDM, thus making the findings of our study relevant to the full clinical spectrum in cardiology. We have analysed and reported our finding according to the PRISMA guidelines.
Despite the methodological design, this systematic review and meta-analysis is not without limitations. Most of the 18 studies included in this systematic review and meta-analysis were modest in size, underpowered to detect potentially small differences between groups, and often included only one or two outcome measures. There was significant heterogeneity in the trials included in this study, which could partly be explained by different cardiac conditions under study. However, no singular cardiac condition or strategy to improve SDM emerged that could explain the heterogeneity alone. Furthermore, despite this heterogeneity, the effect of interventions to increase SDM on one of the main outcome measures (decisional conflict) was consistent across the cardiac conditions studied. Leave-one-out sensitivity analysis supports this conclusion.
The robustness of the present study is supported by the prespecified subgroup analysis, stratified according to clinical condition, demonstrated the effectiveness of SDM across various domains such as chest pain/coronary artery disease/coronary intervention, arrhythmias/atrial fibrillation and cardiac device implantation. The robustness of the effects of the interventions on SDM underscores the generalisability of our findings to the wider field of cardiology and is consistent with findings of similar analyses in other medical and surgical specialties.26–28 It is also noteworthy that the findings of this meta-analysis were robust in a subgroup analysis investigating various formats to support SDM such as printed media, computer aids and other formats. It is, however, less clear whether the findings of our study are also applicable to lower-income and middle-income countries as all included studies were conducted in high-income countries (see table 1). Furthermore, there may also be important effects of culture and language affecting the effectiveness of interventions to improve SDM. Since all our included studies were conducted in the USA, Canada and the UK, our findings may not necessarily be applicable to other high-income countries, for example, in Asia or Europe.
Despite the effectiveness of SDM in improving patient outcomes in general,2 several challenges have been encountered during implementation.29 Major barriers to implementation, both from patients and clinicians, were found to be (1) lack of knowledge and skills, (2) lack of tools and, most importantly, (3) opposing attitudes. Nevertheless, the Making Good Decisions in Collaboration programme also identified possible solutions that may also help in implementation of SDM in cardiovascular care.29 For example, dedicated interactive skills workshops may be used to challenge clinicians’ attitude and highlight the gap between current practice and SDM. Tools to aid decision making could be developed locally, making appropriate information available with relevance to local management pathways and further engaging clinicians with SDM. Similarly, preparing patients to participate in SDM through raising awareness of this method may increase their engagement in this process. Through measurement of decision quality, an improvement in care may be demonstrated following implementation of SDM. Importantly, success of implementation depends on both a collaborative and facilitated approach in each clinical team as well as senior-level support, demonstrating this to be an organisational priority.
Evidence for the effectiveness of SDM in cardiology may help change attitudes towards this patient-centred framework and facilitate its recommendation in clinical guidelines. While this systematic review and meta-analysis adds to the growing evidence of the effectiveness of interventions to increase SDM on patient-centred outcomes, further research on strategies for implementation is urgently needed.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
JR and CP are joint senior authors.
PM and NG-H are joint first authors.
Twitter @DrJReinhold
Contributors PM and NG-H: conceptualisation, methodology, validation, investigation, writing (review and editing), and contributed equally to this paper; JR: conceptualisation, methodology, validation, investigation and writing (original draft), project administration and guarantor; CP: conceptualisation, methodology, validation, investigation, writing (review and editing), project administration and supervision; PM and NG-H: contributed equally to this paper; JR and CP: contributed equally to this paper.
Funding JR and CP received funding from the National Institute for Health and Care Research as part of the clinical lecturer scheme.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.