Article Text

Statistics from Altmetric.com
001 SIROLIMUS ELUTING STENT AND UNPROTECTED LEFT MAIN STENOSIS: THE MULTICENTER E-CYPHER REGISTRY
A. Gershlick, G. Guagliumi, P. Guyon, C. Lotan, J. Schofer, P. Urban, W. Wijns.University Hospitals of Leicester and Others
Background: While treatment of unprotected left main stem (LMS) lesion with PCI remains somewhat controversial, improved outcome through reduced recurrence rates may influence opinion away from the surgical towards the percutaneous approach. The use of sirolimus eluting stents (SES) in LMS, although intuitive, requires careful assessment in real world cases.
Methods: Since April 2002, 220 patients with unprotected LMCA lesions from 79 international centres were prospectively entered in the e-CYPHER database, an ongoing, prospective post marketing, internet based registry. Patient follow up was obtained at 1, 6, and 12 months by patient visit and/or phone contact.
Results: Six month follow up to time of abstract submission is available for 173 patients, with mean age of 66 (SD 11) years. There were 22% diabetics, 28% with prior myocardial infarction (MI), 43% had prior PCI, and 38% prior coronary artery bypass graft (CABG). Main indications for PCI were stable angina (42%), unstable angina (42%), silent ischaemia (8%), and recent or acute MI (4%). Fifty four per cent of patients had three coronary vessels disease. The mean LMS lesion length was 13.1 (SD 7.1) mm and the mean reference coronary vessel diameter was 3.1 (SD 0.4) mm. Overall 1.01 (SD 0.28) SES/LMS lesion were implanted in native (83%) or restenotic lesion (17%). Direct stenting was used in 33%. The combined in-hospital major adverse cardiac events (MACE) rate was 0% with no target vessel failure. At the present time, 6 month follow up has been collected in 163 patients (73%). Incidence of any MACE was reported in 3.7% of cases with 1.8% death, 0.6% MI, and 1.8% target lesion revascularization. Complete 6 month clinical follow up will be available for the presentation.
Conclusion: In this registry SES implantation in LMS lesions appears safe and feasible and, to date, effective for 6 months’ follow up.
002 LOW INCIDENCE OF REVASCULARISATION OF BARE METAL STENTS IN THE ERA OF DRUG ELUTING STENTS: A SINGLE TERTIARY CENTRE EXPERIENCE
H. Jilaihawi, S. Khan, J. Kovac.Glenfield Hospital, Leicester, UK
Background: The use of drug eluting stents has reduced the impact and incidence of both angiographic and clinically significant in-stent restenosis. However, in parallel to this development, there has been an ongoing improvement in bare stent technology. We were keen, therefore to study the incidence and determinants of need for repeat intervention in our patients.
Methods: We studied information contained in our database pertaining to patients undergoing coronary stenting between 1 January 2003 and 7 November 2003. The end point of clinically driven percutaneous target lesion revascularisation (TLR) at 12 months was used, defined as return for intervention to the same lesion within the specified follow up period after the original intervention. This was entered into a multivariate binary logistic regression model with diabetes, clinical instability, total stent length, minimum stent diameter, and individual type of stent (drug eluting Taxus and Cypher stents or the most commonly used bare metal stents including Zeta, Driver, and Sonic) used as covariates.
Results: 1112 patients underwent stenting to an average of 1.4 vessels using a mean total stent length of 23.4 mm and an average minimum diameter of 3.1 mm. The TLR rate was 4.9% of all patients at 12 months (54 cases). It was higher in diabetics (7.3% of 219 patients; p = 0.04), unstable cases (6.7% of 208 patients; p = NS). It was lower in those receiving drug eluting stents (2.8% of 109 patients; p = NS) with respect to bare metal stents, although TLR was low even in those receiving the latter (5.1% of 1003 patients). With regard to specific commonly used bare metal stents there were slight, albeit statistically insignificant, differences. TLR was seen in 5.8% of 467 Zeta cases, 4.9% of 329 Driver, and 5.4% of 93 Sonic cases. In the multivariate model only diabetes was a significant predictor of TLR—perhaps due to the overall low event rate observed.
Conclusion: Clinically significant restenosis with need for revascularisation is currently low in our practice, supporting the argument that more expensive strategies such as drug eluting stents to reduce this phenomenon should be reserved for patients at highest risk, such as diabetics or those with unstable coronary artery disease.
003 REAL WORLD USE OF SIROLIMUS ELUTING STENTS IN SAPHENOUS VEIN GRAFT DISEASE: DATA FROM THE E-CYPHER REGISTRY
A. H. Gershlick, A. Abizaid, G. Guagliumi, P. Guyon, C. Lotan, J. Schofer, A. Seth, J. E. Sousa, P. Urban, W. Wijns.University Hospitals of Leicester and Others
Background: The efficacy of sirolimus eluting stents in the treatment of native vessel disease has been clearly demonstrated in several randomised trials. However there are few data to support the use of SES for the treatment of saphenous graft disease (SVG) stenosis. Restenosis rates in SVG are known to be higher than those in native vessels.
Methods and Results: The international e-CYPHER registry enrolled 14 316 patients to assess the post-marketing performance of sirolimus eluting stent (SES) in “real-world” cases. Six month clinical follow up was captured and analysed by an independent steering committee group. 14 068 patients had lesions in native coronary (Native) and 248 patients had SVG lesions. SVG pts had significantly worse risk profile: patients were older (68 (SD 9.6) v 61 (SD 11) years old; p = 0.0001), more commonly male (82.7% v 77.6%; p = 0.060), more likely to be diabetic (34.3% v 28.5%; p = 0.046), had more hypertension (69.4% v 62.1%; p = 0.020), more hyperlipidemia (80.2% v 62.8%; p = 0.0001), and more often were restenotic lesions (27.8% v 12.1%; p = 0.0001). Direct stenting was more common in the SVG group (43.9% v 33.2%; p = 0.0001). Number of stents per lesion and lesion length was similar in both groups (1.39 (SD 0.7) v 1.34 (SD 0.6); p = 0.273) and 17.1 (SD 10) v 17.2 (SD 8.8); p = 0.782 respectively but reference vessel diameter was larger in SVG group (3.0 (SD 0.37) v 2.86 (SD 0.35); p = 0.0001).
Results: Of 248 patients with SVG and 14 068 with lesions in native vessels, the major adverse cardiac event (MACE) was death 4 (2.0%) v 159 (1.48%), p = 0.54; QMI 2 (1.0%) v 35 (0.33%), p = 0.10; nQMI 2 (1.0%) v 60 (0.56%), p = 0.40; TLR 5 (2.51%) v 132 (1.23%), p = 0.105; TVR 5 (2.51%) v 87 (0.81%), p = 0.009; subacute/late thrombosis 1 (0.5%)/1 (0.5%) v 67 (0.6%)/16 (0.15%), p = 0.74; total MACE 13 (6.53%) v 361 (3.35%), p = 0.014
Conclusions: In the e-CYPHER registry, SES treatment of SVG lesions was associated with a low rate of 6 month TLR (2.5%). The higher MACE rates (6.5%) observed in the SVG group compared with the native group is explained by the higher TVR (non-TLR) rates. This still represents a striking improvement in safety and efficacy when compared with historical bare metal stent data.
004 REAL LIFE IMPACT OF SIROLIMUS ELUTING STENT IMPLANTATION IN TREATING DIABETIC PATIENTS: A 6 MONTH FOLLOW UP REPORT FROM THE INTERNATIONAL E-CYPHER REGISTRY
B. Kevin, A. Gershlick, G. Guagliumi, P. Guyon, C. Lotan, J. Schofer, A. Seth, J. E. Sousa, P. Urban, W. Wijns for the e-CYPHER InvestigatorsHammersmith Hospital, Imperial College and Others
Background: Restenosis and clinical recurrence in diabetic patients undergoing stenting remain a problem, especially in the insulin dependent patients. Limited data have been collected in randomised clinical trials with the use of sirolimus eluting stents (SES) in this high risk group.
Methods: To assess the impact in the real life of SES in treating diabetes, 3506 diabetics/12627 patients entered into the multicentre, international e-CYPHER registry and eligible for follow up at 6 months were analysed. Major adverse cardiac events (MACE) at 180 days after SES placement were adjudicated by an independent endpoint review committee.
Results: Of diabetics, insulin dependent (ID) patients accounted for 34%. Compared with non-insulin-dependent (NID) patients they were more often female (37 v 25%, p<0.001). Diabetics had similar rates of three vessel disease to non-DM (IDD 27% v NID 28% v non-DM 23%); lesion length (17.8 (SD 9.3) v 17.7 (SD 9.3) v 17.1 mm resp); reference vessel diameter (2.8 (SD 0.4) v 2.8 (SD 0.3) v 2.9 (SD 0.3) mm resp) and number of stents implanted (1.4 (SD 0.7) per patient each group). Patients were treated equally with prolonged antiplatelet agents (4.5 months, 95% CI 4.3 to 4.7). Six month follow up was available in 81% of IDD and 84% of NID patients and 85% non-diabetic. Overall diabetic MACE rate at 6 month was: in-hospital, 0.53%; 30 day, 1.89%; 180 days, 4.4% (compared with 2.6% in non-diabetics, 180 days). MACE rates were 5.9% in IDD v 3.3% in NID patients, p = 0.001, including death (3.2% v 1.5%, p = 0.03), myocardial infarction (1.6% v 1.0%, p = 0.2) and target lesion revascularisation (TLR, 1.5% v 1.3%, p = 0.7). Low rates of stent thrombosis (acute, subacute, and late) was observed in both groups (1.0% v 0.7%, p = 0.31).
Conclusion: These results, collected from the largest sample of diabetics patients treated in routine clinical practice with SES, show that the Cypher stent is safe and effective in all types of diabetic patients, as demonstrated by the limited rate of TLR in both IDD and NID groups. However among diabetic patients receiving SES, the IDD cohort continues to have a higher mortality at 6 months.
005 MULTIVESSEL PCI PROCEDURES WITH IMPLANTATION OF SIROLIMUS ELUTING STENTS: A REPORT FROM THE E-CYPHER REGISTRY
A. H. Gershlick, P. Urban, G. Guagliumi, P. Guyon, C. Lotan, J. Schofer, A. Seth, J. E. Sousa, W. Wijns.University Hospitals of Leicester and Others
Introduction: Sirolimus eluting stents (SES) are now widely used, and their efficacy in the treatment of single target lesions has been reliably documented in several randomised clinical trials. Only limited information is available, however, regarding single stage multivessel procedures in routine clinical practice.
Methods: The e-CYPHER registry has currently collected baseline, procedure, and follow up information from 14 316 patients treated in 281 OUS centres with >1 SES. Data were adjudicated by an independent data review committee. 1525 patients (11%) underwent multivessel PCI during the index procedure.
Results: In this subset, mean patient age was 61.7 (SD 11.3) years, 80.4% were male and 34.5% diabetic (11.5% IDD and 23% NIDD). The indication for PCI was: stable angina 43%, unstable angina 35%, acute or recent AMI 10%, and silent ischaemia or another indication 12%. 58% were two vessel and 42% three vessel disease. 2.5% of lesions were in the LMS (0.8% unprotected) and 1.6% in an SVG. 8.3% were in-stent restenotic lesions and 5.5% were total occlusions. Mean estimated reference diameter was 2.8 (SD 0.4) mm and mean lesion length 16.7 (SD 8.9) mm. Each patient on average received 2.6 (SD 0.9) SES to treat 3478 lesions (2.3 lesions/patient) situated in >2 of the three main coronary vessels. Direct stenting was used for 38% of lesions. In-hospital MACE rate was 0.6% (0.1% death, 0.4% AMI, 0.2% emergent TLR). At 6 months, clinical FU was available for 1118 patients (86% of those eligible). 2.2% had died, 1.4% had suffered myocardial infarction, and 1.7% had undergone TLR, for an overall MACE rate of 4.2%. The overall stent thrombosis rate per patient (combining definite and likely events) was 1.16% (0.18% acute, 0.81% subacute, and 0.18% late).
Conclusion: These medium term data are highly encouraging regarding safety of SES in the treatment of multivessel disease, and suggest that the excellent results observed in randomised controlled trials for single lesions can be reproduced for patients requiring more extensive percutaneous revascularisation. The 12 month follow up results will also be presented at the 2005 BCS meeting
006 PERCUTANEOUS CORONARY INTERVENTION WITH DRUG ELUTING STENTS FOR BIFURCATION LESIONS: 6 MONTH RESULTS
K. Vijayalakshmi, B. Kunadian, R. Morley, R. Wright, J. Hall, A. Sutton, M. de Belder.Department of Cardiology, The James Cook University Hospital, Middlesbrough, UK
Background: Complex coronary lesions including bifurcation lesions are associated with a high rate of in-stent restenosis (ISR). Although drug eluting stent (DES) significantly reduces intimal hyperplasia, there are limited outcome data for patients treated with DES for bifurcation lesions.
Methods: Between August 2002 and November 2004, 933 patients underwent percutaneous coronary intervention (PCI) with DES. Bifurcation lesions (BL) were treated in 218 (23%) patients. Of these, 98 (45%) patients had treatment for two bifurcation lesions. Of these, 163 (75%) were men, 94 (43%) patients had stable angina, 38 (17%) patients were diabetic, 54 (25%) had previous myocardial infarction, 8 (4%) had previous CABG, and 31 (14%) had previous PCI. 15 (7%) patients underwent emergency PCI.
Results: In these patients, 373 DES were implanted (1.7 (SD 0.9) stents/patient). PCI was attempted in 303 vessels and 352 lesions (1.61 (SD 0.79) lesions/patient). PCI for BL was performed in 154 (51%) left anterior descending arteries, 19 (6%) right coronary arteries, 5 (2%) left main stem, 9 (3%) obtuse marginal arteries, 5 (2%) diagonal arteries, and 26 (9%) circumflex arteries. Calcified lesions were treated in 121 (56%), chronic total occlusions in 10 (5%), and ISR in 15 (7%) patients. 210 (96%) patients had IIb/IIIa inhibitors. The mean reference diameter was 3 (SD 0.5) mm. The mean (SD) lesion length was 18.9 (SD 11.5) mm. The mean (SD) pre and post PCI minimum lumen diameter was 0.76 (SD 0.4) mm and 3.0 (SD 0.48) mm (p = 0.001). The mean pre and post PCI percentage stenosis was 73.5 (SD 15) and 5.6 (SD 6.9) (p = 0.001). The longest stented segment was 28.5 (SD 13.69) mm. Complete procedural success (all lesions dilated to % DS <50%, no Q-MI, no emergency CABG, patient alive) was obtained in 211 (97%) patients. In hospital MACE occurred in none. Two (0.9%) patients died at 30 day follow up. Six month data were available on 183 (84%) patients. Of these two (0.9%) patients died at 6 month follow up. TVR occured (0%) in none of these patients.
Conclusion: The six month data for patients undergoing percutaneous coronary intervention using DES in bifurcation lesions are favourable. This is associated with a low incidence of MACE and clinically driven target vessel revascularisation (TVR)
007 COMPARISON OF OUTCOMES IN REAL WORLD USE OF SIROLIMUS ELUTING STENTS WITH THE RANDOMISED CONTROLLED CLINICAL TRIALS: CAN THE RESULTS BE REPRODUCED?
A. H. Gershlick, G. Guagliumi, P. Guyon, C. Lotan, J. Schofer, A. Seth, J. E. Sousa, P. Urban, W. Wijns.University Hospitals of Leicester and others
Background: Four randomised, controlled clinical trials have demonstrated the safety and efficacy of the sirolimus eluting coronary stent which are now widely used in routine clinical practice. Only limited information is available however, directly comparing outcome in patients treated in the “real world” with those treated in the controlled environment of clinical research.
Methods: The e-CYPHER registry has enrolled a total of 15 573 patients between April 2002 and July 2004. Of these, baseline, procedure, and 6 month follow up data are available for 14 316 patients. Clinical outcomes at 6 months were compared in those patients enrolled into e-CYPHER (n = 14 316) and those treated in the sirolimus arm of the SIRIUS trial (n = 533).
Results: Patient demographics similar in both groups in terms of age and prior history of cardiac disease; however, there are several striking differences between the two groups.
Characteristic: e-CYPHER/SIRIUS: male, 77.7/72.6; diabetes, 28.6%/24.6%; B2/C lesions, 85%/59%; recent MI, 7%/excluded(-); unstable angina 33.7% (-); prior MI 34%/28.2%; prior revasc 28.6%/26.3%; lesion, >30 mm, 11.7%/(-); lesion, <2.5 mm 8.3%/(-); LMS, 2.2%/(-); ostial, 8.2%/(-); SVG, 2.0%/(-); CTO, 8.8%/(-); ISR, 12.1%/(-); bifurcation, 11.3%/(-).
Although the patients entered into e-CYPHER registry consist of a more “high risk” patient population with more challenging lesions than those treated in SIRIUS, the clinical outcomes are remarkable similar. Major adverse cardiac events are 2.5% for e-CYPHER v 7.1% for SIRIUS. Target lesion revascularisation and target vessel failure also favour e-CYPHER (1.0% v 4.1% and 2.1% v 8.8% respectively).
Conclusion: This retrospective comparison is a clear indication that real world practice can achieve equally impressive results to those from randomised, controlled, clinical trials.
008 INTERRELATION BETWEEN NT-pro BNP, QRS WIDTH, AND SEVERITY OF HEART FAILURE: EUROHEART FAILURE SURVEY
N. K. Khan, P. Velavan, K. Goode, A. S. Rigby, A. L. Clark, F. Follath, M. Komajda, K. Swedberg, J. G. F. Cleland.University of Hull, Kingston upon Hull, UK; University Hospital Zurich, Switzerland; CHU Pitié-Salpetrière, Paris, France; Sahlgrenska Hospital, Göteborg, Sweden
Introduction: QRS width is believed to be an important marker of cardiac dyssynchrony and may also be a marker of severe left ventricular dilatation and systolic dysfunction (LVSD). NT-pro brain natriuretic peptide (BNP) may also be a useful marker to identify heart failure.
Aims: (1) To describe the relation between QRS prolongation and plasma concentrations of N-terminal pro brain natriuretic peptide in patients with suspected heart failure. (2) To describe the relation between these variables and LVSD.
Methods: The EuroHeart Failure survey collected data from patients with suspected heart failure in 115 hospitals from 24 countries across Europe during 2000–2001 for a 6 week period. Patients had various investigations including a standard 12 lead ECG, echocardiogram to assess left ventricular function and measurement of plasma NT-pro BNP levels. We describe a group of 1848 patients who had both ECG and NT-pro BNP testing. Echocardiogram results were available for 1404 of these patients. 61% were men (24% aged >75 years) and 39% were women (39% aged >75 years); NYHA status: Class 1 37%; III/IV 25%; 25% had QRS width of >120 ms; 28% had preserved LV function, 19% had mild, 25% had moderate, and 28% had severe LVSD.
Results: The mean (SE) NT-pro BNP level was significantly increased in patients with QRS prolongation; 1941 (SE 134) pg/ml in patients with QRS <120 ms as compared to 3044 (SE 218) pg/ml in patients with QRS >120 ms (p<0.0001). The greater the width of QRS, the higher was the NT-pro BNP level (r = 0.23; p = 0.00001). Higher NT-pro BNP levels were seen in patients with severe LVSD (3114 (SD 234) pg/ml) when compared with patients with mild LVSD (1911 (SE 260) pg/ml) (p<0.001). On logistic regression analysis, both QRS prolongation and increased NT-pro BNP were predictive of moderate or severe LV dysfunction (wide QRS >120 ms: OR 3.8, 95% CI 2.7 to 5.3; NT-pro BNP >1270 pg/ml: OR 2.3, 95% CI 1.8 to 3.0).
Conclusion: Higher NT-pro BNP levels are observed in patients with suspected heart failure and wide QRS complexes. Both QRS prolongation and increased NT-pro BNP levels are independently associated with moderate or severe LV dysfunction.
009 ANAEMIA PREDISPOSES TO HEART FAILURE IN ACUTE CORONARY SYNDROMES INDEPENDENTLY OF THE SEVERITY OF MYOCARDIAL INJURY
R. A. Archbold, A. Al-Hajiri, A. Suliman, J. Cooper, K. Ranjadayalan, A. D. Timmis.Newham University Hospital NHS Trust, London; University College, London; Barts and The London NHS Trust, London, UK
Background: Anaemia has been identified as a major determinant of outcome in patients with cardiovascular disease, particularly heart failure (LVF). In this study we have examined the relations between haemoglobin concentration ([Hb]), LVF, and mortality in acute coronary syndromes (ACS).
Methods: Cross sectional cohort study of 1693 patients with ACS (43% myocardial infarction). Hospital outcomes (LVF, cardiac death) were analysed by quartiles of admission [Hb] (Q1 <12.6, Q2 12.6–13.7, Q3 13.8–14.8, Q4 >14.8 g/dl).
Results: There was a close inverse relation between the frequency of LVF and admission [Hb], (Q1 21.7%, Q4 11.1%; p (trend) <0.0001), the odds of LVF being 0.45 (95% CI 0.31 to 0.66) for Q4 relative to Q1. Admission [Hb] was also associated with age, renal dysfunction, and ethnicity but despite multiple adjustment for these and other baseline variables, the effect of [Hb] was diminished only slightly, the odds of LVF for Q4 relative to Q1 increasing to 0.53 (0.32–0.88). The association of [Hb] with LVF was not a reflection of the severity of myocardial injury, rates of infarction (52.6% v 40.2%; p = 0.001), and median (IQR) peak CK values (257 (112–834) v 156 (75–509) IU/l; p<0.0001) being higher in Q4 compared with Q1. This may explain why admission [Hb] was not associated with cardiac death, which occurred in 3.1% of Q4 and 3.9% of Q1 patients (p = 0.24).
Conclusion: In patients with ACS, anaemia predisposes to LVF but not cardiac death. Predisposition to LVF appears to be a direct effect of anaemia, and is not attributable to myocardial injury which is paradoxically less severe in patients with anaemia.
010 ELEVATED SERUM GLUCOSE PREDICTS MORTALITY IN PATIENTS ADMITTED TO HOSPITAL WITH A NEW DIAGNOSIS OF HEART FAILURE
J. Newton, I. B. Squire.Department of Cardiovascular Sciences, University of Leicester, UK
Introduction: Heart failure (HF) is characterised by increased sympathetic activity with excess free fatty acids, insulin resistance, and reduced glucose uptake. Markers of increased sympathetic activity can predict mortality. We assessed the relation between serum glucose and mortality in patients with HF.
Methods: Retrospective analysis of 528 patients admitted to hospital with new HF. Demographics, comorbidity, baseline therapy, and examination findings were abstracted from case notes. First serum haemoglobin, sodium, potassium, creatinine, and glucose were recorded.
Results: See figure. 179 (34%) patients were on diabetic therapy on admission or discharge. 103 (58%) of the diabetic patients died compared with 138 (40%) of non-diabetic patients (p<0.0001). Unadjusted survival analysis by glucose quartile demonstrated association between glucose >10 mmol/l and all-cause mortality hazard ratio (HR) 1.773 (95% CI 1.251 to 2.512, p = 0.001). This was significant only in non-diabetic patients (HR 2.675 (1.664 to 4.301, p<0.0001); 0.853 (0.504 to 1.443) in non-diabetics). After adjustment for age, sex, blood pressure, sodium, creatinine, haemoglobin, and prior diuretic use, a serum glucose >10 mmol/l remained significant for all-cause mortality (HR of 2.636 (1.577 to 4.405, p<0.0001)) in non-diabetics.
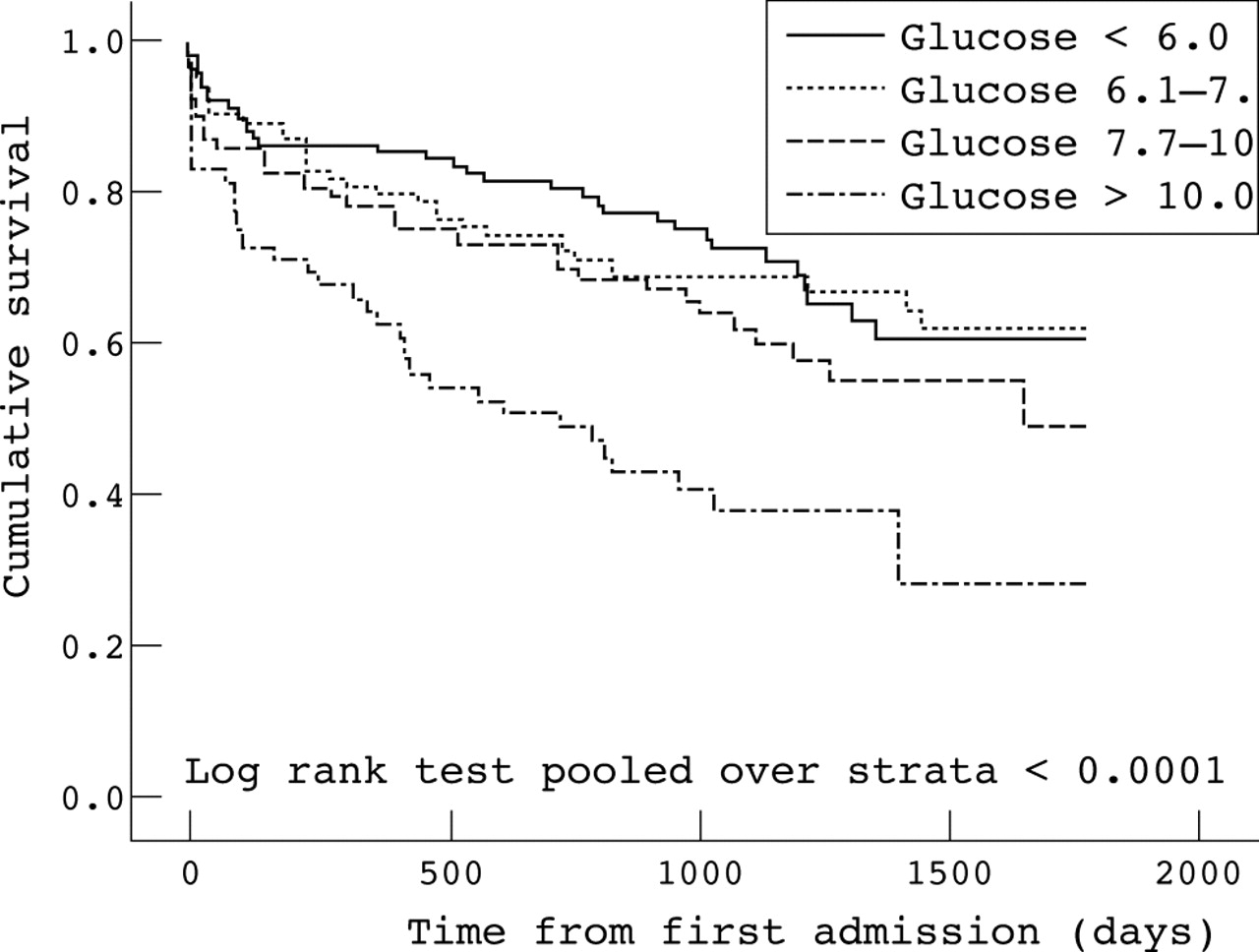
Abstract 10
Conclusion: Increased serum glucose on admission is an independent predictor of all-cause mortality in non-diabetic patients admitted with a new diagnosis of heart failure. Hyperglycaemia in non-diabetics may be a marker for increased sympathetic activity indicating more severe heart failure, and warrants further investigation.
011 PREDICTORS OF SHORT TERM MORTALITY IN HEART FAILURE: EUROHEART FAILURE SURVEY
P. Velavan, N. K. Khan, K. Goode, A. S. Rigby, L. L. Tin, M. Komajda, F. Follath, K. Swedberg, H. Madeira, J. G. F. Cleland.Academic Cardiology Unit, University of Hull, Kingston upon Hull, UK
Background: Heart failure affects 1–2% of the population. It causes about 5% of medical admissions and complicates a further 10–15%. Heart failure has a poor prognosis, as one third of patients will die within 6 months of diagnosis and the annual mortality among 6 month survivors is 10–15%.
Aim: To study the factors affecting short term mortality in heart failure.
Methods: The EuroHeart Failure survey collected data from 11 356 patients with suspected heart failure in 115 hospitals across 24 European countries during 2000–2001, over a period of 6 weeks. Investigations included a 12 lead ECG, echocardiogram, and routine blood tests. The patient characteristics and treatment profile have been published previously. We examined all the available clinical variables affecting the 12 week mortality by univariate and multivariable analysis by logistic regression.
Results: A total of 1425 (12.5%) patients died between admission and 12 weeks’ follow up. On univariate analysis, increasing age and the following variables were related to an adverse prognosis: hyponatraemia (OR 3.7; 95% CI 2.9 to 4.8), renal impairment (3.0; 2.3 to 3.8), hyperkalaemia (2.4; 1.7 to 3.2), anaemia (2.0; 1.6 to 2.6), hyperuricaemia (1.9; 1.1 to 3.5), severe mitral regurgitation (1.8; 1.4 to 2.3), severe LV systolic dysfunction (LVSD) (1.6; 1.3 to 1.8), QRS & QT prolongation (1.2; 1.1 to 1.4 and 1.3; 1.2 to 1.5), and female sex (1.3; 1.2 to 1.4). Treatment with ACE inhibitors (0.5; 0.4 to 0.5), angiotensin receptor blockers (0.5; 0.4 to 0.7), beta blockers (0.5; 0.4 to 0.6), nitrates (0.9; 0.8 to 0.9), antithrombotics (0.6; 0.6 to 0.7), and lipid lowering drugs (0.3; 0.3 to 0.4) were associated with a better prognosis. On multivariable analysis, only five factors provided independent prognostic information: age, severe LVSD, renal impairment, hyponatraemia, and treatment with beta blockers (ROC curve of predicted probability, AUC 0.73; p<0.0001).
Conclusion: Hyponatraemia, renal dysfunction, and the severity of LV systolic dysfunction appear to be the major potentially modifiable risk markers in patients with a recent admission to hospital for or complicated by heart failure. Patients treated with beta blockers have a better prognosis.
012 MORTALITY OF PATIENTS IN ENGLAND WITH LEFT VENTRICULAR SYSTOLIC DYSFUNCTION AND HEART FAILURE DUE TO OTHER CAUSES
F. D. R. Hobbs, A. K. Roalfe, R. C. Davis, R. Hare, M. K. Davies.Department of Primary Care & GP, Primary Care Clinical Sciences Building, University of Birmingham, Sandwell & Queen Elizabeth Hospitals, UK
Background: Heart failure (HF) and left ventricular systolic dysfunction (LVSD) are common conditions with essentially malignant prognoses. Data from large trials and epidemiological studies in select populations indicate three year mortality rates of 30–50%. Such studies may not represent patients in the wider community, who are often older and have more concomitant illnesses.
Methods: The ECHOES (Echocardiographic Heart of England Screening) study established the prevalence of LVSD and HF in 3960 randomly selected subjects aged 45 years and older in England. A separate cohort of 782 subjects with a prior HF label was also studied by clinical assessment and echocardiography. Mortality data are presented at least 4 years from baseline.
Results: Four year survival rate of the general population was 95% compared with 65% in those with LVSD and 66% with HF. Median survival time of HF was 6 years 4 months. Those with a prior HF diagnostic label had the lowest survival compared with the general population (log rank test, ÷2 = 9.97, p<0.002). Survival improved significantly with increasing ejection fraction (log rank test for trend, ÷2 = 486.4, 1, p<0.0001). People with multiple causes of HF had the poorest survival.
Conclusion: ECHOES mortality data confirm the poor prognosis of HF patients in the community, providing a generalisable risk estimate of 8–9% per year. This is lower than rates in select population studies. Importantly, borderline systolic dysfunction carries a poor prognosis and prognosis is worse in patients with a correct clinical label of HF. Aetiology does not exert an effect on mortality rates
013 INDICATORS OF INCREASED RISK OF MORTALITY FOLLOWING FIRST HOSPITAL ADMISSION WITH HEART FAILURE: THE VALUE OF ROUTINE CLINICAL VARIABLES
J. Newton, I. B. Squire.Department of Cardiovascular Sciences, University of Leicester, Leicester, UK
Introduction: Numerous variables predict adverse outcome in heart failure. We assessed the value for prediction of increased risk of death of routine variables available within 24 hours of first admission with heart failure.
Methods: Retrospective analysis of 528 patients with first heart failure admission. Demographics, comorbidity, drug therapy, examination findings, and routine serological parameters were abstracted from case notes. Mean follow up was 1257 days. Proportional hazard modelling identified independent predictors of all-cause mortality, for use in a simple risk scoring model.
Results: See figure. Mean age at admission was 69.5 years, 43% were female and 238 (45%) died. Compared with those aged <63 years, hazard ratio (HR) for those aged 63–70 was 1.545 (95% CI 1.101 to 2.364) and 2.206 (1.454 to 3.348) for those >77 years. HR for creatinine >133 μmol/l and glucose >10.0 mmol/l were HR 2.502 (1.668 to 3.752) and 1.916 (1.344 to 2.372). Hb as a predictor varied by sex, with Hb <11.5 g/dl in women = HR 1.816 (1.211 to 2.723), and Hb <13.4 g/dl in men = HR 3.618 (1.986 to 6.589). Diuretic use on admission = HR of 1.339 (1.035 to 1.734). A scoring system was derived (potential score 1–8). A cut-off of 1–3 = low risk and 4–8 = high risk has a sensitivity of 78% and specificity of 57%.

Abstract 13
Conclusion: Age, haemoglobin, creatinine, and plasma glucose measured soon after admission provide powerful prognostic information for patients hospitalised with a new diagnosis of heart failure, and a simple model based on these parameters performs similarly to the prospectively validated American Heart Failure Survival Score.
014 ETHNICITY AND VARIATION IN PROGNOSIS FOR PATIENTS NEWLY HOSPITALISED FOR HEART FAILURE
J. Newton, I. B. Squire, H. M. Blackledge.Department of Cardiovascular Sciences, University of Leicester, UK
Introduction: Prognosis for patients with coronary heart disease (CHD) and congestive heart failure (CHF) is said to vary with ethnicity. We compared mortality in age matched South Asian and white cohorts after first admission for heart failure.
Methods: Retrospective analysis of 528 patients admitted to hospital with a new diagnosis of heart failure; 176 South Asian patients and 352 age and sex matched white patients. Demographics, comorbidity, baseline drug therapy, clinical examination, and biochemistry were recorded, along with discharge drug therapy and results of echocardiography.
Results: See figure. Compared with whites, South Asian patients more often had prior diagnosis of hypertension (45% v 33%, p = 0.006) and diabetes (46% v 18%, p<0.0001) but similar rates of prior CHD. Atrial fibrillation (15% v 31%, p = 0.0002) and prior prescription of diuretic (39% v 48%, p = 0.037) were less common in South Asians. Left ventricular function was more often recorded as normal (38% v 23%, p = 0.002) and less often as severely impaired (18% v 28%, p = 0.025) for South Asians. During follow up (520–1880 days), 73/176 (41.2%) of South Asian and 167/352 (47.4%) of white patients died. South Asian ethnicity was associated with lower all-cause mortality (OR 0.71, 95% CI 0.53 to 0.96, p = 0.02).
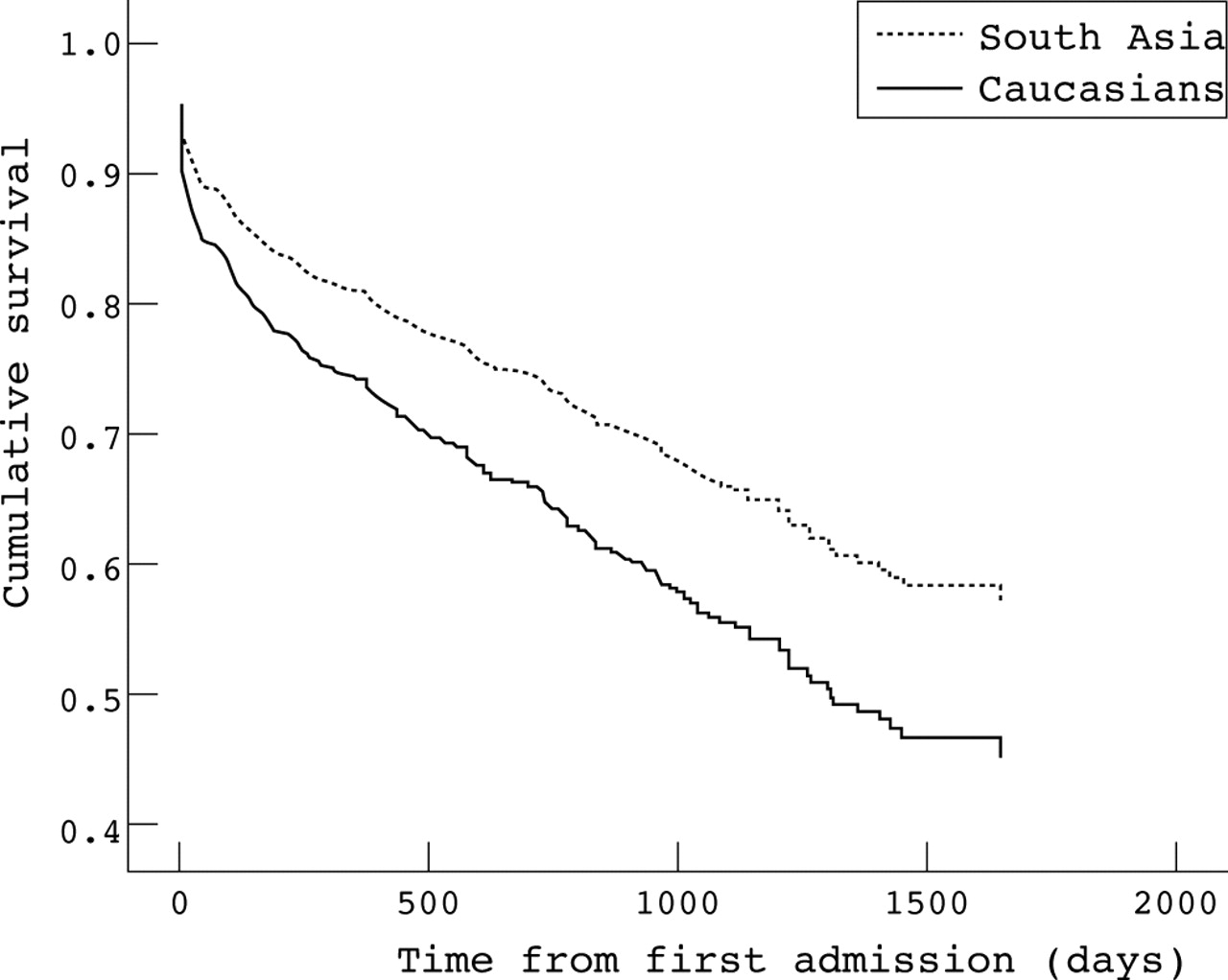
Abstract 14
Conclusion: At first hospitalisation for CHF, survival is better for South Asians compared with whites. Heart failure appears to be less advanced in South Asians, among whom diabetes and hypertension are more prevalent.
015 DETERMINANTS OF EARLY RECURRENCE OF AF IN PACEMAKER AF SUPPRESSION STUDY PATIENTS
J. Silberbauer, A. Arya, L. Boodhoo, A. Mitchell, D. Hildick-Smith1, S. O’Nunain1, K. Kamalvand3, G. W. Lloyd, N. R. Patel, V. Paul2, A. N. Sulke.Eastbourne DGH 1Royal Sussex County Hospital; 2Ashford and St Peters Hospital; 3William Harvey Hospital
Introduction: The pacemaker AF suppression (PAFS) study is a prospective multicentre investigation evaluating DDDRP AF suppression efficacy using implanted pacemakers (Vitatron Selection 9000 and T70). The extensive diagnostic features of this device record AF burden and frequency as well as detailed onset reports. These show beat-to-beat atrial and ventricular episodes preceding the onset of atrial fibrillation (AF) episodes allowing analysis of preceding triggers. Patients with at least three symptomatic episodes of PAF in the last month and refractory to at least two drugs were recruited.
Methods: 192 patients (72 (SD 9) years, 55% male) enrolled. Devices were programmed to DDD60 with all prevention algorithms off and patients monitored for one month. 47 patients suffered an AF burden of 1–50% and their data were used for subsequent analysis.
Results: In 252 AF episodes 87% had an identifiable trigger. Early re-initiation of AF (ERAF) was defined as a recurrent AF episode within one minute of termination of the prior AF episode. Late early re-initiation (LERAF) was defined as occurring within 5 minutes of the previous episode termination. ERAF caused 46% and LERAF 6% all AF episodes. Premature atrial contractions (PAC) caused 36% of all AF episodes. 4% of episodes had preceding sinus tachycardia and no episodes were due to bradycardia. This contrasts with the AFT study in which 22% of AF was bradycardia induced when paced in DDD at 40 bpm. ERAF had an identifiable trigger in 82% of cases, only 18% were “sudden onset”. 74% of ERAF episodes were triggered by one or more PACs. There was no significant diurnal variation in ERAF/LERAF onsets. Drug therapy which was stable throughout the study showed no significant effect on ERAF onsets except ß blockers which suppressed all sinus tachycardia onsets.
Conclusion: The predominance of early re-initiation of AF due to PACs as an AF trigger should provide a good substrate for successful ERAF prevention with appropriate pacing algorithm suppression therapy.
016 A NOVEL RECTANGULAR BIPHASIC WAVEFORM FROM A RADIOFREQUENCY DEFIBRILLATOR COMPARED WITH A CONVENTIONAL WAVEFORM FOR THE TRANSVENOUS CARDIOVERSION OF CHRONIC ATRIAL FIBRILLATION IN PATIENTS
B. M. Glover1, C. J. McCann1, S. J. Walsh1, M. J. Moore1, G. Manoharan1, M. J. Roberts1, C. M. Wilson1, J. D. Allen1, J. M. C. Anderson2, A. A. J. Adgey1.1Regional Medical Cardiology Centre, Royal Victoria Hospital, Belfast; 2University of Ulster, Jordanstown, UK
Purpose: The optimal waveform for the transvenous direct current cardioversion (DCC) of atrial fibrillation (AF) is unknown. A novel rectangular biphasic waveform (6/6 ms duration, phase 2 peak voltage 50% of phase 1) delivered from a radiofrequency (RF) powered defibrillator was compared with a conventional capacitor based exponential biphasic waveform of equivalent duration and voltage.
Method: Patients with chronic AF (fully anticoagulated) were randomised to receive either the RF or a conventional trapezoidal waveform (Ventritex HVS-02). Defibrillation electrodes were positioned in the right atrial appendage (cathode) and distal coronary sinus (anode). All shocks were R-wave synchronised. Phase 1 peak voltage was increased in stepwise progression from 50V–300V. Success was defined as return of sinus rhythm for ⩾30 seconds. Cardiac troponin and CKMB were checked post procedure.
Results: Patients (n = 16, 11 male) received 83 shocks (RF = 40, conventional = 43). Mean age was 63 (SD 11.6) years, mean BMI was 28 (SD 6) and mean duration of AF was 5.8 (SD 5.7) months. The groups were matched in terms of age, sex, BMI, duration of AF, aetiology, drugs, and echocardiographic features. The RF waveform performed significantly better than the conventional waveform for the cardioversion of chronic AF (7 of 8 patients (87%) v 1 of 8 patients (12%) success, p = 0.003). The mean leading edge voltage for the RF was 221V (range 100–300) and for the conventional waveform was 240V. No significant arrhythmias, sinus pauses, or episodes of hypotension occurred. There was no elevation of cardiac enzymes.
Conclusion: The novel biphasic waveform has a superior efficacy at a lower voltage compared with the conventional waveform in the transvenous cardioversion of AF. There were no arrhythmic, haemodynamic complications or elevation of markers of myocardial injury. Use of this waveform may improve the efficacy of implantable devices for the treatment of AF.
017 CAN ATRIAL FIBRILLATION WITH A COARSE ECG APPEARANCE BE TREATED BY CATHETER ABLATION OF THE TRICUSPID VALVE-INFERIOR VENA CAVA ISTHMUS? PRELIMINARY RESULTS OF A MULTICENTRE RANDOMISED CONTROLLED TRIAL
M. J. Earley, G. A. Haywood, L. Richmond, S. C. Sporton, P. Broadhurst, N. S. Peters, R. J. Schilling (coarse AF investigators).St Bartholomew’s Hospital, London; Derriford Hospital, Plymouth; St Mary’s Hospital, London; Aberdeen Royal Infirmary, UK
Background: AF may be driven by a macroreentry circuit limited by the same lines of block as found in typical atrial flutter. We hypothesised that a strategy of ablating the tricuspid valve-inferior vena cava isthmus (TV-IVC) in patients with coarse atrial fibrillation (AF) would be superior to DC cardioversion to prevent recurrences.
Methods: Patients with AF and an ECG with irregular p waves ⩾1.5 mV in ⩾1 lead were included. All antiarrhythmic drugs were stopped and warfarin started at least 6 weeks before the procedure. Patients were randomised to DC cardioversion (group 1) or TV-IVC ablation +/− DC cardioversion (group 2). Techniques for each arm of the study were dictated by the local hospital protocol. Patients were reviewed 4, 16, and 52 weeks post procedure. Quality of life (QOL, SF36) and symptom (modified Karolinska) questionnaires were performed at baseline and follow up. The primary endpoint of the study was freedom from any recurrence of sustained AF at 1 year. Secondary endpoints were time to first AF recurrence, symptoms and QOL.
Results: Forty six patients (8 female) aged 56 (SD 8) years have been randomised (24 to group 1), median follow up 7.8 (range 0.7–12) months. Baseline QOL, symptom scores (37 (SD 22) v 34 (SD 31)) and LA sizes (44 (SD 6) v 46 (SD 6) mm) were similar in each group. In group 1, two patients reverted to SR spontaneously and 13 of the remaining 22 were successfully treated, needing 1.3 (SD 0.5) shocks (163 (SD 73) J). In group 2, 16 achieved bidirectional block, two unidirectional, and four failed. Overall (intention to treat) procedural success was 15/24 (63%) group 1 v 18/22 (81%) group 2 (p = 0.15). 22 patients have reached 1 year follow up with none having complete freedom from AF. Maintenance of SR at 1, 4, and 6 weeks if the procedure was successful was group 1 v 2; 80, 67, and 35 v 67, 37, and 12% (p = 0.07). If SR was maintained at 4 weeks there was a significant reduction in symptom (n = 12, 32 (SD 29) to 14 (SD 8), p<0.01) and QOL scores but not if AF recurred (symptoms n = 44, 37 (SD 28) to 36 (SD 32), p = NS).
Conclusion: Symptoms and QOL are improved if SR is restored; however as a first line strategy TV-IVC ablation offers no advantage over DC cardioversion for the management of coarse AF.
018 ABLATION OF EPICARDIAL AUTONOMIC GANGLIONATED PLEXI DURING MINIMALLY INVASIVE SURGICAL ABLATION OF ATRIAL FIBRILLATION
D. Lockwood, H. Nakagawa, B. Scherlag, R. Wolf, M. Peyton1, W. M. Jackman.Oklahoma University Health Sciences Center, Oklahoma City, OK; 1University of Cincinnati College of Medicine, Cincinnati, OH, USA
Background: There are four autonomic ganglionated plexi (GPs) located within fat pads (FPs) on the epicardial surface of the left atrium (LA) near the pulmonary veins (PVs). Canine studies suggest that high activity in GPs (dysautonomia) may cause or facilitate atrial fibrillation (AF). In those studies, GPs were activated using high frequency stimulation (HFS) over FPs. The FPs are easily visualised in patients during a minimally invasive surgical AF ablation procedure, using a bipolar radiofrequency (RF) clamp (Isolator, AtriCure) to isolate the LA cuff of the PVs. The aims of this study were to determine (1) whether epicardial HFS can be used in patients to locate the four GPs; and (2) whether GPs are destroyed by ablation aimed only at PV isolation.
Methods: Seven patients with AF undergoing minimally invasive surgical PV isolation were studied. Before and after successful PV isolation, an electrode catheter with 1 mm tip electrode was maneuvered around the PV myocardial sleeves, adjacent LA and FPs to (1) identify the presence or absence of PV (and adjacent LA) potentials to confirm PV isolation post ablation and (2) apply bipolar HFS (cycle length 50 ms, 12V, 1 ms pulse width) to the FPs, PVs, and surrounding LA. A positive HFS (vagal) response was defined as >50% increase in mean R-R interval during AF.
Results: All PVs were isolated by RF clamp applications. Before ablation, HFS produced a vagal response at: (1) FP anterior to the right PVs (anterior right GP, ARGP) in 7/7 patients, (2) FP inferior to the right inferior PV (inferior right GP, IRGP)in 7/7 patients; (3) FP rightward of the insertion of the ligament of Marshall into the pericardium, between the left superior PV and right pulmonary artery (superior left GP, SLGP) in 5/7 patients, and (4) FP inferior to the left inferior PV (inferior left GP, ILGP) in 6/7 patients. After PV isolation, the vagal response to HFS was eliminated at 3/7 ARGP, 5/7 IRGP, 5/5 SLGP, and 5/6 ILGP sites.
Conclusion: The four GPs in FPs on the epicardial surface of the LA can be located using epicardial HFS. The vagal response to HFS is often, but not always, eliminated by ablation aimed solely at PV isolation.
019 SURFACE ATRIAL FREQUENCY ANALYSIS IN PATIENTS WITH ATRIAL FIBRILLATION: ASSESSING THE EFFECT OF TWO STANDARD LINEAR ABLATION LESIONS SITED IN THE LEFT ATRIUM
D. Raine, P. Langley1, A. Murray1, S. S. Furniss, J. P. Bourke.1Departments of Cardiology and Medical Physics, Freeman Hospital, Newcastle upon Tyne Hospitals NHS Trust, UK
Introduction: Our group has shown previously that measurements of atrial frequency can be obtained from surface 12 lead ECG recordings of patients during atrial fibrillation (AF), using a combination of principal component and Fourier transform algorithms. Such measurements are reproducible over time and change with drug manipulation of the arrhythmia. This study had two aims: (1) to determine whether linear left atrial ablation, using a combination of “roof” and “mitral isthmus” lines, results in changes in surface atrial frequency during AF and (2) to assess the contribution of each individual line when sited sequentially.
Methods: Computerised recordings from 26 patients, who had undergone linear ablation procedures for AF, were reviewed retrospectively. The atrial signal was extracted from the 12 lead ECG data by principal component analysis and the main frequency component identified using Fourier analysis. Atrial frequency before and after these two standard ablation lines was compared. Lesions were sited with the help of x ray screening and the LocaLisa intracardiac catheter guidance system (LocaLisa, Medtronic Inc, USA). Individual lesions were performed using a 7-French, 4 mm irrigated-tipped ablation quad-polar catheter using 30–50W with temperature limited to 50°C and an irrigation flow rate of 600 ml normal saline/hour. The duration of recordings varied between patients with a median of 141 (range 23–627) seconds before and 115 (range 16–587) seconds after both ablation lines were sited.
Results: Atrial frequency decreased significantly after the combination of roof and mitral isthmus lines (5.66 v 5.15 Hz; p = 0.0001) and when either roof (5.61 v 5.13 Hz; p = 0.002) or mitral isthmus (5.89 v 5.75 Hz; p = 0.032) lines were sited first. However, only the roof line led to a significant reduction in atrial frequency when sited second (5.64 v 5.49 Hz; p = 0.033).
Conclusion: Measurements of atrial frequency can be obtained from surface 12 lead ECG recordings during AF and change as predicted in response to linear left atrial ablation. This technique may be useful in assessing antiarrhythmic treatments for AF.
020 CATHETER ABLATION OF ATRIAL FIBRILLATION: PRIMARY AND LONG TERM EFFICACY FOR THREE APPROACHES IN A SINGLE CENTRE
J. M. Morgan, A. M. Yue, P. R. Roberts.Wessex Cardiac Centre, Southampton General Hospital, UK
Background: Percutaneous techniques for ablation of paroxysmal or persistent atrial fibrillation (AF) have evolved rapidly. However, the long term efficacy following primary procedural success is not yet established.
Methods and Results: We performed a retrospective analysis on 168 consecutive patients (123 male, mean age 52 years) between 1998 and 2004 who underwent AF ablation (excluding AV node ablation) in Southampton. Patients are reported in three groups. Group I: 1998–2000; 23 patients underwent targeted ablation of trigger sites (mean fluoroscopy time 56 minutes, procedure time 230 minutes) in highly selected patients demonstrating frequent atrial ectopy/atrial fibrillation) on ambulatory monitoring. Trigger sites were targeted using either non-contact mapping or multipolar contact catheters introduced into pulmonary veins. 15 (65%) patients were free of atrial fibrillation at 54 (range 47–60) months without antiarrhythmic drugs. Significant pulmonary vein (PV) stenosis was documented in two (9%). Group II: 2001–2003; 86 patients underwent PV ostial ablation for abolition of PV potentials using PV ostial mapping catheters (mean fluoroscopy time 46 minutes, procedure time 167 minutes). 55 (61%) patients were free of AF, 12 (22%) were on antiarrhythmic drugs at 15–36 (mean 21) months follow up. PV stenosis was documented in two (2%). Pericardiocentesis for tamponade was performed in five. Group III: 51 patients underwent combined PV ostial and left atrial ablation using a combination of ostial ablation and linear lesion creation – left lower PV to mitral isthmus and left atrial roof lesions (mean procedure time 112 minutes). Eight had undergone a previous ablation procedure. At follow up 48 (81%) were free of AF at 3–15 (mean 9) months. Surgical intervention was required in one as a complication of transeptal puncture. PV stenosis was documented in one.
Conclusion: New approaches to AF suggest that the clinical techniques are becoming mature. Although success rates are lower in earlier procedural approaches, long term efficacy in primarily successful cases is proven. Primary success appears to have increased with newer techniques although long term efficacy needs continuing evaluation.
021 EXPERIENCE WITH 75 CONSECUTIVE CRYOABLATION PROCEDURES IN A SINGLE UK TERTIARY CENTRE
A. E. French, K. Woodburn, T. R. Cripps.Department of Cardiology, Bristol Royal Infirmary, UK
Methods: Cryoablation (Cryocath) was performed in 75 patients between July 2003 and November 2004. Follow up data were checked in all cases, and procedural success, procedure length, fluoroscopy duration, and complications compared with 98 RF ablations carried out between August 2002 and November 2004. Subgroup analysis was performed according to arrythmia mechanism.
Results: There was a significantly shorter mean fluoroscopic screening time for Cryocath procedures compared with RF procedures (22.4 minutes v 25.6 minutes, p = 0.037), despite a longer procedure duration (141.6 minutes v 136.6 minutes, p = 0.044). Within the separate subgroups, cryoablation for AV nodal re-entrant tachycardias (AVNRT) had a higher procedural success rate than RF (100%, n = 44 v 91.5%, n = 47), with one late recurrence in the RF group; five patients (11.1%) had a recurrence in the Cryocath group. Three RF AVNRT patients required permanent pacemaker implantation (6.4%), compared with zero incidence of heart block in the Cryocath group. For typical atrial flutter circuit ablations there was a higher procedural success rate for cryoablation (81%, n = 21 v 70%, n = 10), with a shorter mean procedure duration and fluoroscopic screening time. One patient in each group required temporary pacemaker as a result of the procedure, but only the RF patient progressed to permanent pacemaker implantation. One late recurrence was reported in the Cryocath group (4.8%). Accessory pathway cryoablation was carried out in 10 patients (five with right anteroseptal location) with a 90% success rate and zero incidence of heart block. 41 patients underwent RF accessory pathway ablation with a 95.1% success rate. One patient required temporary pacing as a result of RF (2.4%). There was a shorter mean screening time with Cryoablation. Three patients (one RF (2.4%) and two (20%) Cryocath reported recurrence. Two were subsequently successfully treated with cryoablation.
Conclusion: Cryoablation is a safe and effective technique. There was a trend towards shorter fluroscopy times and a higher success rate for typical flutter. The incidence of permanent heart block was zero, including ablations for AVNRT and para-Hisian accessory pathways. Higher catheter costs were offset against the elimination of a need for permanent pacing.
022 THE GROWTH OF CARDIAC REHABILITATION IN THE UK SINCE 1998
H. J. N. Bethell, J. Evans, S. C. Turner.Basingstoke & Alton Cardiac Rehabilitation Centre, UK
Introduction: Between 1987 and 2000, the number of cardiac rehabilitation (CR) centres in the UK increased from 87 to over 300. However the proportion of eligible patients enrolled in CR programmes has remained low. This paper describes the increase in patients enrolled into CR since 1998 and relates this to the number of those eligible for CR.
Methods: Annual questionnaire to all the CR coordinators in the UK. Each year’s figures have been uprated to give estimates of the total number of patients treated, assuming that the non-respondents had similar throughputs to the responders.
Results: The table indicates the number of patients treated, as an absolute figure and as a percentage of those eligible to be treated, for patients recovering from acute myocardial infarction (AMI), from coronary artery bypass grafting (CABG) and from percutaneous coronary intervention (PCI). The proportion of AMI patients treated increased from 23% to 27% with a slight fall over the past two years. The proportion of CABG patients treated increased from 56% to 74% with a slight fall over the past two years. The proportion of PCI patients treated has increased from 10% to 18% and has shown a recent sharp increase (see table).
Abstract 22
Conclusion: After a steady increase in the proportion of AMI and CABG patients treated in CR centres, the numbers are now static or falling. Despite a rapid increase in the number of PCI procedures, the proportion of these patients included in CR has nearly doubled. However the total number of eligible patients treated in CR centres is still nowhere near the NSF expectation of 85%.
023 CHANGES IN HEART RATE VARIABILITY MEASURES DUE TO CARDIAC REHABILITATION
G. R. H. Sandercock, J. Ganachaud, T. Hughes, R. Groocott-Mason, D. A. Brodie.Buckinghamshire Chilterns University College and Hillingdon Hospital NHS Trust, UK
Aim: To evaluate the effects of cardiac rehabilitation (CR) on autonomic function by heart rate variability.
Methods: Thirty (12 F, 18 M) patients (mean age 56 (SD 8) years) underwent 5 minute, resting ECG recording at CR entry and exit assessments. ECG data were automatically filtered and a time series of normal-to-normal RR intervals created. The mean (NN) and the SD of normal-to-normal intervals (SDNN) were created. A fast Fourier transform was then applied to the time series to calculate the power spectral density of the NN intervals. Total spectral power (TP, 0.04–0.4 Hz) was divided according to recommended guidelines into the vagally mediated high (HF, 0.15–0.40 Hz) and the mixed, sympathetic, and vagal low (LF, 0.04–0.15 Hz) frequency components of the power spectrum. Values were log transformed and compared using repeated measures t tests.
Results: The table shows the results for repeated measures t tests for all measures. Global (SDNN) and spectral measures (LF and HF) were all increased following CR. There was also a trend toward increased NN interval.
Abstract 23
Conclusion: In post-MI patients, HRV measures (SDNN, LF, and HF) are known risk factors for future cardiac event. In the present study, these measures of autonomic modulation were all increased. An increase in HRV provides protection against cardiac arrhythmia. As CR increases HRV, this study provides evidence of its effectiveness as a therapeutic intervention.
024 PSYCHOLOGICAL REHABILITATION FOR CARDIAC PATIENTS: SYSTEMATIC REVIEW AND META-ANALYSIS
K. Rees, R. West, P. Bennett, G. Davey-Smith, S. Ebrahim.University of Bristol, Bristol, UK University of Wales College of Medicine, Cardiff, UK
Background: Psychological interventions are offered in rehabilitation programmes, either on their own or as part of comprehensive cardiac rehabilitation (CR). These interventions may involve stress management or less focussed counselling approaches, with the aim of reducing stress and risk of cardiac events and of improving quality of life.
Objectives: To determine the effectiveness of psychological interventions, particularly stress management, on mortality, morbidity, anxiety, depression, quality of life, and modifiable cardiac risk factors in patients with coronary artery disease (CAD).
Methods: Electronic databases were searched for randomised controlled trials, using standard trial filters. Reference lists of retrieved papers and expert advice were sought. The review included trials of psychological interventions, administered by trained staff, either alone or with other CR interventions, to adults of all ages with CAD (myocardial infarction, coronary artery bypass graft or angioplasty, angina) and with at least 6 months follow up. Two reviewers selected studies and abstracted data independently.
Results: Thirty six trials met the inclusion criteria (12 841 patients) and 18 trials (5242 patients) evaluated stress management. Quality of many was poor, with for example only six blinding outcome assessment. All trials combined showed no strong evidence of effect on total mortality (odds ratio OR = 0.93 (0.81–1.06)), cardiac mortality or revascularisation. They did show a reduction in non-fatal infarction (OR = 0.78 (0.67–0.90)) but not in the two large trials and there was evidence of publication bias. Relatively few trials reported psychological outcomes: there were small reductions in anxiety and depression (eight trials, standardised mean difference −0.32 (−0.56 to −0.08)) but not in the only large trial, indicating marked heterogeneity. Few reported effects on modifiable cardiac risk factors or quality of life.
Conclusion: Psychological interventions showed no significant effect on total or cardiac mortality but did show some evidence of small reductions in anxiety and depression. Findings for stress management trials alone were similar.
025 PHYSICAL ACTIVITY BEHAVIOUR IN USERS OF A MENU BASED CARDIAC REHABILITATION PROGRAMME: A LONGITUDINAL SURVEY
S. Catto, G. Bowman, C. Goodier1, L. Young1, P. MacIntyre.Royal Alexandra Hospital, Paisley, UK; 1University of Glasgow, UK
Background: Participation in traditional standardised cardiac rehabilitation (CR) is associated with short term improvements in physical activity levels but the majority of individuals struggle to maintain regular exercise once supervision is withdrawn.
Aims: To examine adherence to physical activity following participation in comprehensive, menu based CR and associated Phase 4 services.
Methods: Physical activity levels were assessed for seven consecutive days at three time points (week preceding phase 3 (T1), phase 3 completion (3 months later for non-completers) (T2), and 1 year following start of phase 3 (T3)) in 36 patients referred consecutively to CR at the Royal Alexandra Hospital, Paisley. Assessment was made using the seven day physical activity recall questionnaire (PAR), exercise stage of change (SOC) and the Computing Science & Applications (CSA) accelerometer. Data were analysed for within group (completers v non-completers) differences over time using Wilcoxon signed ranks test for numeric and McNemar’s test for categorical variables. Due to losses to follow up, data for non-completers were analysed from T1–T2 only.
Results: The proportion of regularly active completers (n = 28) (that is, action and maintenance SOC) increased from T1–T2 and decreased from T2–T3 (82% v 100% v 91%; p = 0.13, p = 0.25) but these changes were non-significant; change for non-completers (n = 8) from T1–T2 was also non-significant (50% v 67%, p = 1.00). Completer PAR scores increased significantly from T1–T2 and were sustained from T2–T3 (355 v 458 v 459 minutes; p = 0.02, p = 0.32). Non-completer PAR scores did not increase significantly from T1–T2 (128 v 197 minutes; p = 0.14). Completer CSA counts rose from T1-T2 and fell from T2-T3 but these changes were not significant (2.65×106 v 3.42×106 v 2.75×106; p = 0.17, p = 1.00). Non-completer CSA counts did not increase significantly from T1–T2 (1.45×106 v 2.68×106; p = 0.30).
Conclusion: The study provides some evidence that completion of menu based CR is associated with short term increases in physical activity. Although it is unclear whether this level of activity is maintained long term, the majority of completers were still regularly active at 1 year.
026 EFFECTS OF PHYSICAL TRAINING ON ANXIETY AND DEPRESSION IN CHRONIC HEART FAILURE
S. Gupta, N. Gandhi, L. Burgess, N. Brooks.Wythenshawe Hospital, Manchester, UK
Background: Heart failure patients experience psychological distress, reduced social functioning and diminished quality of life. Anxiety and depression are common in these patients and the severity may affect clinical outcomes. Physical training improves exercise time and anaerobic threshold in heart failure. However, there are few data on the effects of physical training on depression and anxiety.
Method: 267 patients with heart failure completed the Hospital Anxiety and Depression (HAD) score before beginning their physical training. Of these, 48 had anxiety or depression scores of ⩾11. HAD score was repeated in all 48 patients after completion of physical training.
Results: Out of 267 patients referred for physical training, NYHA Class I, II, III, and IV was present in 28 (10%), 132 (49%), 103 (39%), and 4 (2%) respectively. In the majority, heart failure was due to either ischemic heart disease (189; 71%) or dilated cardiomyopathy (43; 16%). Before training, HAD depression score ⩾11 was present in 12 (4%), anxiety score ⩾11 in 26 (10%), with 12 (4%) having both anxiety and depression score of ⩾11. Mean LVEF of patients with anxiety and/or depression was 32.2 compared with 30.7 in entire group. After the training programme, mean anxiety score reduced from 11.6 (SD = 3.1) to 10.0 (SD = 3.6), p = 0.001, and depression score decreased from 9.8 (SD = 3.1) to 8.6 (SD = 3.1), p = 0.02. In patients with both anxiety and depression, reduction in score was from 13.1 (SD = 1.9) to 10.6 (SD = 2.7), p = 0.007. Reduction in score for anxiety and depression was seen irrespective of NYHA class. In males, mean anxiety score reduced from 11.3 (SD = 3.0) to 10.0 (SD = 3.2), p = 0.008, and depression score reduced from 10.5 (SD = 2.7) to 8.7 (SD = 3.2), p = 0.003. In females, mean anxiety score reduced from 12.4 (SD = 3.4) to 10.2 (SD = 4.8) and depression score changed from 7.9 (SD = 3.4) to 8.6 (SD = 3.2), after physical training.
Conclusion: Anxiety and depression are common in heart failure. Physical training improves HAD score suggestive of a beneficial effect in the psychological wellbeing in these patients.
027 AUDIT: MANAGEMENT OF PATIENTS WITH HEART FAILURE IN A DISTRICT GENERAL HOSPITAL
U. K. Prasad, L. A. Wilson, A. Cooke, J. M. Rowley.Department of Cardiology, Kings Mill Hospital, Sutton-in-Ashfield, Nottinghamshire NG17 4JL, UK
Introduction: Pharmacological improvements in treatment of heart failure (HF) with BB, ACEI, and spironolactone have improved morbidity and mortality. There is a large discrepancy in diagnosis and treatment of HF in primary care and among hospital specialities.
Aim: To identify patients with a new diagnosis of HF, to discover how the diagnosis was made, to determine what drugs were prescribed and if they were optimised. To identify the proportion admitted under the care of the cardiologists and other team and their follow up.
Method: The study was carried out at Kings Mill Hospital, which is a busy district general hospital. A list of 384 patients admitted between January and December 2003 with a diagnosis of HF was compiled by using the ICD-10 coding determined on discharge: I50.0-CCF, I50.1-LVF, and I50.9-HF unspecified. 100 out of 384 patients were chosen randomly for this audit. Data were extracted from the individual case notes and entered on Microsoft Excel for statistical analysis.
Results: The mean age was 78.8 years, 49% were male. 56% were given a diagnosis of HF for the first time during admission. For 50% of patients the aetiology was thought to be due to IHD or HT, and a further 25% had mixed aetiologies. Only 35% were admitted under the cardiology team. 58% of patients received an ECHO and only 79% of these showed evidence of HF (systolic dysfunction). All patients received diuretics, but only 13% had spironolactone in addition. 67% were discharged on ACEI (51% on optimal dose) and only 27% with a BB (41% on optimal dose). In only 20% of cases, advice was given to the GP on optimisation and 35% had the dose increased on subsequent FU. In 56% of cases in which the diagnosis of HF was new, 29% were under a cardiologist. 23% were given a BB (54% optimal dose) and 70% were given an ACEI (44% optimal dose). Patients were more likely to receive BB, ACEI, spironolactone, and ECHO under care of a cardiology team.
Conclusion: BB, ACEI, and spironolactone is still underused in HF. Patients are discharged with little education and information is not being communicated well to GPs regarding optimisation of therapy. There are differences between the treatment received within the department of cardiology and elsewhere and use of the HF specialist nurse is almost exclusive to patients under a cardiologist.
028 RAPID ACCESS CHEST PAIN CLINICS IN THE POST NATIONAL SERVICE FRAMEWORK ERA: ARE PROTOCOL DRIVEN NURSE LED CLINICS SAFE? A RETROSPECTIVE AUDIT
V. C. Kuppuswamy, R. S. Patel, S. Duffy, S. Gupta.Department of Cardiology Whipps Cross University Hospital National Health Service (NHS) Trust, London, UK
Background: Chest pain (CP), that is, angina or undifferentiated CP, is one of the commonest symptoms for patient seeking medical help. There are 22 600 new cases of angina in the UK annually and the national service framework (NSF) standard for angina is investigation and treatment to relieve pain and reduce coronary risk. This led to the setting up of a rapid access chest pain clinic (RACPC) in every acute NHS hospital in the UK with a standard of assessment within 2 weeks of the referral. However there is a lack of consensus on the staffing of the RACPC leaving the options open. Although the nurse led clinic is a preferred way of delivering this service, from anecdotal evidence the safety of this model is largely untested.
Objective: To audit the safety of a nurse led RACPC in an acute inner city district general hospital.
Method: A sample of 700 subjects discharged between March (2002–03) from a cohort of 2672 subjects were followed up using a postal questionnaire after a median of 12 months following their “alleged” normal exercise tolerance test (ETT). The main outcomes were: events (myocardial infarction (MI)/death); need for revascularisation (percutaneous coronary intervention (PCI)/coronary artery bypass surgery (CABG)); visits (GP/A&E); investigations (thallium scan/angiogram), and reassurance.
Results: Of the 700 questionnaires posted 372 were returned, a response rate of 53%. Of the responders 200 subjects (54%) were men with a mean (SD) age of 55 (11) years. Of the 372 subjects: three (0.8%) have sustained MI; 12 (3%) have had angiograms; five (1%) have undergone PCI; 65 (17%) have revisited their GP of which one patient was referred to A&E and eight (2%) to cardiology OPC; 5 (1%) patients visited A&E directly. Two hundred and ninety two (75%) of the 372 subjects had not experienced any further chest pain in 12 months and felt reassured. Thirty five subjects (9%) were not reassured and 23 (6%) of them were having CP but have not sought any medical help.
Conclusion: Our audit confirms that a nurse led “zero waiting time” model can safely identify low risk patients from the undifferentiated CP/angina referral while significantly reducing the number of unnecessary hospital admissions. These findings compare favourably with data from studies evaluating physician or technician led RACPC. The audit is ongoing and there has been no mortality so far.
029 CONTEMPORARY PROGNOSIS OF ANGINA AND NON-CARDIAC CHEST PAIN AT THE INTERFACE BETWEEN PRIMARY AND SECONDARY CARE: MULTICENTRE OUTCOME ANALYSIS OF 8802 PATIENTS ATTENDING RAPID ACCESS CHEST PAIN CLINIC
N. Sekhri, G. Feder, C. Junghans, S. C. Cotter, H. Hemingway, A. D. Timmis.Newham University Hospital, and Barts and the London Queen Mary School of Medicine, London, UK
Background: Two key assumptions have underpinned the proliferation of rapid access chest pain clinics (RACPCs): (1) the prognosis of chest pain in primary care is unfavourable and (2) the prognosis can be improved by rapid assessment to identify those with angina who might benefit from treatment to protect against acute myocardial infarction (AMI) and death. This study was undertaken to test these assumptions.
Methods: Multicentre cohort study of 8802 first time attendees at RACPCs with undiagnosed chest pain. Patients known to have coronary disease (previous ACS, revascularisation or diagnostic angiography) were excluded. Median (IQR) follow up was for 2.57 (1.96–4.15) years.
Results: Angina was diagnosed in 27% of the cohort. These patients were older and more frequently male and white than patients diagnosed with non-cardiac chest pain. In patients diagnosed with angina, relative to those with non-cardiac chest pain, adjusted hazard ratios for CHD death and non-fatal MI were 1.94 (1.19–3.15), rising to 4.50 (3.34–6.06) for hospital admission with acute coronary syndromes. Standardised all-cause mortality ratios (SMRs (95% CI)) in patients with angina were not significantly different from the general population, but for coronary death were significantly increased in both men (203 (151 to 255)) and women (218 (136 to 301)). SMRs (all cause and coronary) for non-cardiac chest pain were always lower compared with angina and were comparable to the general population.
Conclusion: This study challenges the assumption that chest pain in patients referred for RACPC assessment has an unfavourable prognosis. However, it shows that in patients diagnosed with angina, fatal and non-fatal coronary event rates are high, confirming the need for vigorous preventive strategies in this group.
030 A RAPID ACCESS CARDIOLOGY SERVICE EFFECTIVELY DIAGNOSES NON-CARDIAC DISEASE AND LOW RISK AMONG PATIENTS PRESENTING WITH CHEST PAIN, BREATHLESSNESS, AND PALPITATIONS
J. N. Tenkorang, K. F. Fox, D. A. Wood.Department of Cardiology, Hammersmith Hospitals NHS Trust at Charing Cross Hospital, London, UK
Introduction: The triage of patients presenting with symptoms suggestive of cardiac disease is the key role of rapid cardiology services (for chest pain, arrhythmia, and heart failure). However there are few data on the long term mortality and morbidity of patients seen in these services. We conducted a prospective 1 year follow up study of all patients seen in the rapid cardiology service at Charing Cross Hospital.
Methods and Results: 1223 patients were seen between 1 November 2002 and 31 October 2003. 940 (77%) consented to participate. Non-participants and participants were well matched for demography and diagnosis. Information on all consenting patients was extracted from patient questionnaires, hospital information systems, GP information, and the ONS. The initial diagnosis made at the rapid access clinic visit and diagnosis by 1 year are shown in the table. The 1 year diagnosis incorporated any changes based on data from the above sources. 98% diagnosed initially with non-cardiac disease did not develop a cardiac diagnosis by 1 year. There were 26 (10 cardiac) deaths among the cohort of 940 patients. Cardiac mortality for those diagnosed initially with cardiac disease was 7/205 (3.4%) and for those with non-cardiac/possible diagnosis 3/735 (0.4%).
Abstract 30
Conclusion: A rapid cardiology service promptly and effectively excludes cardiac disease in patients presenting with symptoms suspicious of a cardiac pathology who are at very low risk of cardiac death within one year.
031 GENE TRANSFER OF A BROAD SPECTRUM CC-CHEMOKINE INHIBITOR REDUCES MACROPHAGE RECRUITMENT AND SMOOTH MUSCLE CONTENT IN VEIN GRAFT ATHEROSCLEROSIS IN APOLIPOPROTEIN E-KNOCKOUT MICE
Z. A. Ali, C. A. Bursill, Y. Hu, R. P. Choudhury, Q. Xu, D. R. Greaves, K. M. Channon.Department of Cardiovascular Medicine, University of Oxford & Department of Cardiological Sciences, St Georges Hospital Medical School, UK
Introduction: Neointimal hyperplasia and accelerated atherosclerosis are major causes of vein graft failure after bypass surgery. Several CC-chemokines (CKs) mediate macrophage recruitment and smooth muscle cell (SMC) proliferation in native atherosclerotic plaques; we hypothesised that CC-CKs may be critical in the development of SMC neointimal hyperplasia and accelerated atherosclerosis in vein grafts.
Methods: Using in vivo gene transfer, we administered a soluble CC-CK binding protein (35K) to 26 ApoE -/- mice that underwent interposition bypass grafting of the vena cava from isogenic donor mice to the carotid artery. Recombinant adenoviruses encoding either 35K (Ad35K) or green fluorescent protein (AdGFP, control) were injected via the tail vein.
Results: After 2 weeks, 35K gene transfer dramatically reduced macrophage content and SMC α-actin-positive neointimal area compared with AdGFP controls (see fig). At 4 weeks, the early reduction in macrophage content in Ad35K mice had normalised, whereas SMC α-actin-positive neointimal area remained significantly lower (see fig). Finally, 35K gene transfer significantly reduced total vessel wall thickening at both 2 weeks (74%, 13 (SD 4.2) v 52 (SD 8.3) μm; p<0.01) and 4 weeks (45%, 41 (SD 7.3) v 76 (SD 8.3) μm; p<0.01) after surgery compared with controls.
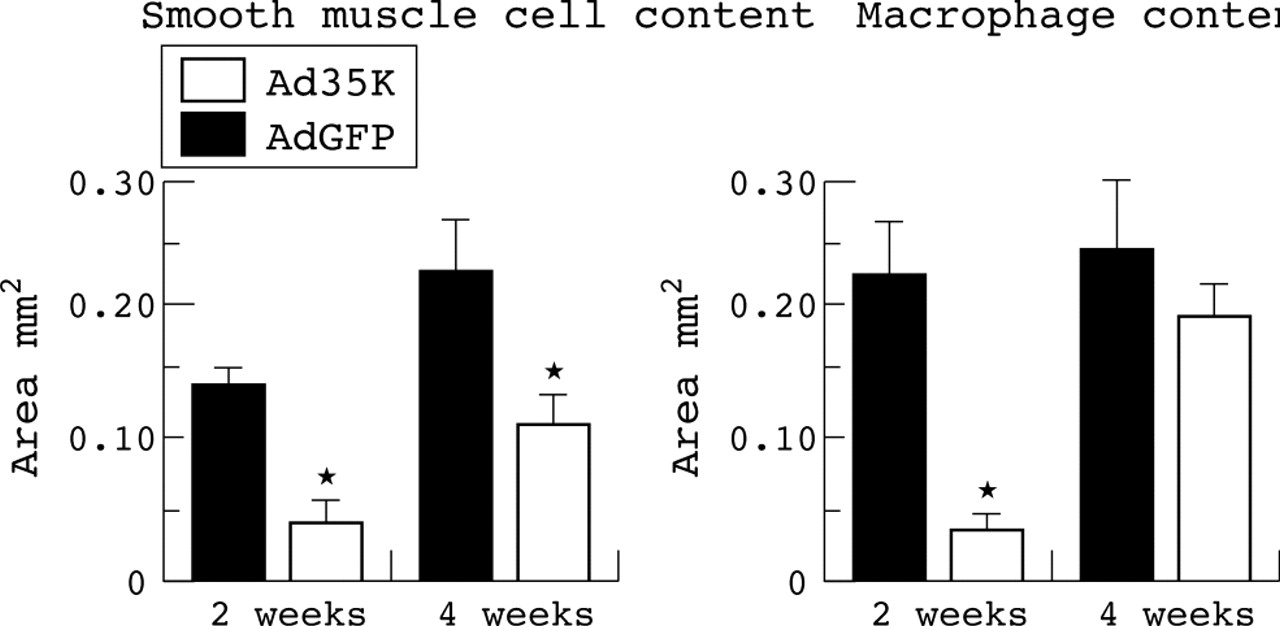
Abstract 31
Conclusion: A single intravenous injection of the CC-CK inhibitor 35K significantly reduced smooth muscle cell proliferation, early macrophage recruitment and total vessel wall thickening in carotid-caval vein grafts in ApoE -/- mice. This study highlights the importance of the CC-CK class in vein graft disease and their role as a potential target for improving vein graft potency.
032 INVESTIGATION OF P2X7 DEPENDENT MECHANISMS OF INTERLEUKIN-1 BETA (IL-1β) RELEASE FROM HUMAN ENDOTHELIAL CELLS
R. W. Varcoe, L. Stokes, S. E. Francis, S. Dower, A. Surprenant, D. C. Crossman.Institute of Molecular Physiology, University of Sheffield, UK; Cardiovascular Research Group, Northern General Hospital, Sheffield, UK
Introduction: Endothelial cell (EC) IL-1β is important in the pathogenesis of the atherosclerotic plaque and the arterial wall response to injury. Release of IL-1β from ECs has not been well characterised but in immune cells has been shown to require activation of the P2X7 ligand gated ion channel by ATP. We set out to investigate P2X receptor expression in human ECs and to demonstrate functional P2X responses, in particular, the processing and release of mature, bioactive IL-1β in response to activation of the P2X7 receptor.
Methods: Human umbilical vein ECs (HUVECs) were cultured in the presence of a variety of proinflammatory cytokines; lipopolysaccharide (LPS), interferon gamma (IFNγ), tumour necrosis factor alpha (TNFα), and IL-1β itself. P2X mRNA was measured by a qRT-PCR assay and protein by western blotting, immunoprecipitation, FACS analysis and immunocytochemistry. Functional P2X responses were measured by electrophysiology and calcium imaging techniques. IL-1β release was measured by ELISA, western blotting, immunoprecipitation, and a dual luciferase reporter bioassay.
Results: In unstimulated HUVECs P2X4 and P2X7 mRNA and protein were the predominant P2X subtypes detected, with P2X4 the most abundant. The proteins were shown to associate together by co-immunoprecipitation but very little P2X7 was detected at the cell surface. Pro IL-1β synthesis was also negligible. Stimulation with IFNγ and TNFα for 48 hours had a potent effect on mRNA levels with a 75× increase in P2X4 and a 50× increase in P2X7 compared with baseline. These changes were also reflected at the protein level and significant expression of P2X7 was seen at the cell surface for the first time. There was a similarly potent effect on Pro IL-1β synthesis and treatment of these cells with the P2X7 agonist BzATP resulted in the release of mature IL-1β. Overexpression of P2X7 in HUVECs by adenoviral transfection produced similar results.
Conclusion: These findings suggest that under proinflammatory conditions ECs synthesise and release IL-1β with potential pro-atherogenic consequences and that this release process is dependent on the activation of P2X7 ion channels by extracellular ATP. They also suggest this receptor as a possible future therapeutic target in the treatment of atherosclerotic vascular disease.
033 CALCIFIC CRYSTALS DIRECTLY INDUCE THE RELEASE OF OSTEOPONTIN FROM HUMAN MACROPHAGES VIA PI3-KINASE, ERK1/2 MAP KINASE, AND NFκB SIGNALLING PATHWAYS: IMPLICATIONS FOR ATHEROGENESIS AND CALCIFIC VASCULAR DISEASE
I. Nadra, P. Philippidis, M. Johns, G. M. McCarthy1, R. C. Landis, D. O. Haskard.BHF Cardiovascular Medicine Unit, Eric Bywaters Centre, Hammersmith Hospital, Imperial College London, UK; 1RCS, Dublin, Ireland
Introduction: Osteopontin (OPN) is a protein mediator capable of promoting macrophage and vascular smooth muscle cell (VSMC) recruitment. Within atherosclerotic lesions, local production of OPN occurs from macrophages at sites of calcification. Via hydroxyapatite (HAP) and RGD binding motifs OPN is thought to act as a bridging molecule that facilitates calcific-crystal removal by co-localising macrophages. As the precise triggers for OPN release in calcified plaques are still largely unknown, we aimed to investigate whether HAP may activate human macrophages to release OPN.
Methods and Results: Human monocytes isolated from peripheral blood were differentiated in vitro into macrophages and treated with HAP crystals for 20 hours. Using scanning electron microscopy we demonstrated that macrophages physically bound HAP. Western blotting (WB) of these cells clearly demonstrated the induction of OPN expression, first detected at 12 hours and peaking at 48 hours. OPN gene expression was also confirmed by RT-PCR, with an increase in mRNA first seen at 6 hours (p<0.01). Macrophage conditioned media (CM) was then screened for OPN by ELISA. In contrast to resting macrophages significantly lower levels of OPN were detected in CM from HAP stimulated cells (1004 (SD 227) ng/ml and 52 (SD 14) ng/ml respectively, n = 8, p<0.001). WB analysis of proteins bound to HAP crystals from the macrophage cultures revealed a high level of crystal-bound OPN, suggesting that the decreased detection in HAP treated CM was due to sequestration of OPN by HAP. Blocking crystal uptake using the cytoskeleton inhibitor cytochalasin D significantly inhibited OPN release. WB of HAP stimulated macrophages pretreated with pharmacological inhibitors for the PI3-K, ERK1/2, and NFkB signalling pathways also showed a reduced expression of OPN. Further evidence for the involvement of these pathways was obtained by demonstrating the rapid phosphorylation of AKT and ERK1/2 along with IκBα degradation in response to HAP.
Conclusion: This is the first study to report that calcific crystals are capable of directly inducing OPN release from human macrophages. This involves PI3-K, ERK1/2, and NFκB signalling pathways. Released OPN subsequently binds avidly to surrounding HAP, helping remove calcific deposits by macrophages. However the macrophage and VSMC-chemotactic properties of OPN may also promote further chronic inflammation.
034 PROSPECTIVE ANALYSIS OF THE ASSOCIATION OF MEAN LEUCOCYTE TELOMERE LENGTH WITH RISK OF CORONARY HEART DISEASE AND INTERACTION WITH STATIN TREATMENT
S. Brouilette, J. Moore, J. R. Thompson, A. McMahon, C. Packard, A. H. Goodall, N. J. Samani on behalf of the WOSCOPS InvestigatorsDepartment of Cardiovascular Sciences, University of Leicester and Department of Pathogical Biochemistry and Robertson Centre, University of Glasgow, UK
Introduction: Variation in biological as distinct from chronological age may predispose to coronary heart disease. We have previously shown in cross sectional studies that shorter mean leucocyte telomere length (TL), an indicator of more advanced cellular age, is associated with coronary atherosclerosis and premature MI. To determine whether shorter telomeres predict risk of CHD events we carried out a “prospective” analysis in subject participating in the West of Scotland Coronary Prevention Study (WOSCOPS).
Methods: Mean TL in baseline DNA was assessed in 484 male subjects (cases) who subsequently had a CHD event (death, MI, CABG, or PTCA) over a mean follow up period of 4.7 years and in 1058 age and smoking status matched subjects (controls) who did not develop an event. Mean TL was measured using a real-time quantitative PCR based technique and expressed as a ratio (CQ) of telomere repeat copy number to a single copy gene repeat number.
Results: Age had a highly significant effect on CQ with a reduction in the ratio of −0.008 (SD 0.002) per additional year of age (p = 0.002). After adjustment for age, CQ was significantly lower in cases compared with controls (difference: 0.075 (SD 0.002), equivalent to an age difference of 9.4 years, p = 0.006). Subjects in the WOSCOPS study were randomised to receive either pravastatin or placebo with 31% fewer CHD events in those receiving pravastatin. When subjects were grouped into tertiles by CQ ratio, no benefit of pravastatin was seen in subjects with the highest CQ ratio (tertile 1). Furthermore, while in the placebo group risk of CHD doubled in those in the lower two tertiles of CQ ratio (hazards ratios (HR) of 1.93 (95% CI 1.33 to 2.81) and 1.95 (1.33 to 2.84) respectively in tertiles 2 and 3 compared with tertile 1), this increase in risk with shorter telomeres was completely attenuated by statin treatment (HR 1.12 (95% CI 0.75 to 1.69) and 1.02 (0.68 to 1.52) respectively in tertiles 2 and 3 compared with tertile 1).
Conclusion: These novel findings show that mean leucocyte telomere length predicts risk of development of CHD in previously healthy subjects. There is a significant interaction between benefit from statin treatment in reducing CHD events and mean leucocyte telomere length. The mechanism underlying this interaction and its clinical importance needs further investigation.
035 ERYTHROPOIETIN DELAYS ENDOTHELIAL CELL SENESCENCE BY PRESERVING TELOMERE LENGTH
M. Vasa-Nicotera, S. Brouilette, P. Nicotera1, N. J. Samani.Department of Cardiovascular Sciences, Univesity of Leicester, UK; 1MRC Toxicology Unit, University of Leicester, UK
Background: Replicative senescence and telomere shortening of endothelial cells has been suggested to play a critical role in atherogenesis. In line with this proposal, recent findings have shown that the rate of telomere attrition is increased in patients with coronary artery disease (CAD). Accumulating evidence suggests that the kidney erythroid cytokine erythropoietin (EPO) has cardiovascular protective effects. Here we examined the effects of EPO on endothelial cell senescence.
Methods: Human umbilical vein endothelial cells (HUVECs) were kept in culture by continued passaging up to passage 18. RhEPO (100 ng/ml) was added to the cultures from passage 7 every 48 hours. Senescence was determined by staining HUVECs with senescence associated (SA)-β-galactosidase (pH 6.0). Telomere length was measured by a novel PCR based method in which a relative quantification (rq) ratio of telomere sequence to single copy gene (36b4) is determined for each sample. Telomerase activity was determined using the telomeric repeat amplification protocol (TRAP) assay.
Results: RhEPO significantly reduced the number of SA-β-galactosidase positive cells starting at passage 9 (34 (SD 7)% reduction) with a maximal effect at passage 14 (51 (SD 9)% reduction, p⩽0.05). Inhibition of endothelial cell senescence was associated with a delay in the telomere attrition rate in EPO treated cells evident at passage 8 (rq ratio of 1.11 v 1.00 in controls, p⩽0.05), maximal at passage 11 (rq ratio of 1.16 v 0.96, p⩽0.01) and still present at passage 16 (rq ratio of 0.87 v 0.72). Moreover, telomerase activity was significantly augmented following EPO stimulation (twofold increase at passage 10 and threefold increase at passage 14).
Conclusion: EPO delays endothelial cell senescence via activation of telomerase and maintenance of telomere length. EPO or EPO mimicking drugs may have a protective action against plaque formation and CAD.
036 CIRCULATING ENDOTHELIAL CELLS, VON WILLEBRAND FACTOR, AND FLOW MEDIATED DILATATION AS INDICES OF ENDOTHELIAL DAMAGE/DYSFUNCTION IN PATIENTS WITH ACUTE CORONARY SYNDROMES
A. Blann, K. Lee, G. Lip.Haemostasis Thrombosis and Vascular Biology Unit, University Department of Medicine, City Hospital, Birmingham B18 7QH, UK
Background: Separate studies have shown increased circulating endothelial cells (CECs, reflecting endothelial injury) in coronary artery disease that express functionally active tissue factor (TF) and correlate with impaired flow mediated vasodilatation (FMD) and plasma TF. We hypothesised that increased CECs are related to impaired FMD and elevated plasma TF (an index of coagulation), von Willebrand factor (vWf, also marking endothelial damage) and IL-6 (a proinflammatory cytokine) in patients with acute coronary syndromes.
Methods: We studied 120 patients with ACS (80 acute myocardial infarction (AMI) and 40 unstable angina; 86 male, age 65 (SD 12) years) and 40 age and sex matched patients with stable CAD and 40 healthy controls (HC). Plasma vWf, TF, and IL-6 levels were measured by ELISA. CECs were quantified using epifluorescence microscope after immunomagnetic separation with CD146. Brachial artery FMD and glyceryl-trinitrate mediated dilatation (NMD) used to assess endothelium dependent and independent vasodilatation, respectively, in a subset of 39 ACS patients, who were compared with the stable CAD and HC groups.
Results: As expected, ACS patients had significantly higher CECs, vWf, TF, and IL-6 levels, but lower FMD, when compared with stable CAD and HC (all p<0.001) and all intercorrelated significantly. However, only CECs and FMD were independently related. In stable CAD, significant correlations were again found between many of the indices, but on multivariate analysis, IL-6 and vWf were both independently related to FMD.
Conclusions: Increased endothelial cell damage/injury in ACS (abnormal CECs, FMD and vWf) is closely associated with abnormal coagulation (TF) and inflammation (IL-6). These findings support the concept of a central role of endothelial damage/injury and inflammation in the activation of vascular and coagulation abnormalities in ACS.
037 ASSOCIATION BETWEEN THE -174G/C POLYMORPHISM OF THE INTERLEUKIN-6 GENE AND CAROTID ATHEROSCLEROSIS: FAMILY STUDY AND META-ANALYSIS
B. Mayosi, P. Avery, M. Baker, N. Gaukrodger, H. Imrie, M. Farrall, H. Watkins, B. Keavney.Universities of Newcastle and Oxford, UK; The Cardiac Clinic, New Groote Schuur Hospital, Cape Town, South Africa
Background: Previous studies have produced conflicting results concerning the putative association between the interleukin 6 (IL-6) -174 G/C polymorphism and carotid intima-media thickness (IMT), a measure of subclinical atherosclerosis. We have used a family based genetic association design to assess the heritability of carotid IMT and investigate the hypothesised association. To place our results in context, we conducted a meta-analysis of all published studies, including a total of 3095 individuals.
Methods: 854 members of 224 white families were studied. The heritability of carotid IMT was determined using MERLIN. Genetic association analyses between carotid IMT and the IL-6 -174 G/C polymorphism were carried out using analysis of variance and family based tests of association implemented in the QTDT program.
Results: The heritability of carotid IMT was 24% (p<0.00001). Under a recessive model (GG and GC v CC), there was significant evidence of association between genotype and adjusted log maximal carotid IMT (F = 5.469, p = 0.02). The CC genotype was associated with a 4.3% greater adjusted log maximal carotid IMT. Genotype at the IL-6 -174 G/C polymorphism accounted for 0.6% of the observed variation in the phenotype. A meta-analysis including the present and four previous studies yielded significant evidence of association between the IL-6 -174 C/C genotype and higher carotid IMT (p = 0.0028), There was significant heterogeneity in genotype frequencies between the contributing studies (χ2 70.21, p<0.001) which was largely accounted for by two studies with less than 100 participants. When just the three larger studies were combined, there was stronger evidence for association between the C/C genotype and CIMT (p = 0.0014).
Conclusion: We observed a small but significant association between IL-6 (-174) C/C genotype and higher carotid IMT, which was confirmed in the meta-analysis. These findings support the notion that genetically determined differences in cytokine gene expression are causally related to the development of atherosclerosis, though the magnitude of such effects may be of marginal clinical relevance.
038 TRIBBLES-1, A MITOGEN ACTIVATED PROTEIN KINASE (MAPK) SCAFFOLD REGULATES INFLAMMATION IN VASCULAR SMOOTH MUSCLE CELLS (VSMC) AND ATHEROSCLEROSIS
H. Y. Sung, S. Francis, D. C. Crossman, E. Kiss-Toth.Cardiovascular Research Unit, Division of Clinical Sciences (North), University of Sheffield, UK
Introduction: Inflammation of the vessel induces proliferation of VSMC. A major signalling network involved in the regulation of proliferation is the MAPK cascade. We have recently identified a novel gene family that regulate MAPK activation called tribbles (trb).1 In flies, trb have been shown to regulate mitosis, during ventral furrow formation. Our data suggest that trbs act at the level of MAPKK/MAPKs, and control MAPK phosphorylation/activity. Depending on their expression level, they are able to potentiate or inhibit MAPK responses. Using co-IP experiments we found that MEK-1 interacts with both trb-1 and trb-3, MKK7 specifically with trb-3, and MKK4 specifically with trb-1. The aim of this study was to investigate a possible link between inflammation, atherosclerotic coronary disease, and trb expression.
Methods: In segments of whole artery wall taken from explanted hearts of patients with ischaemic heart disease (IHD) and dilated cardiomyopathy (DCM) at the time of cardiac transplantation, we compared mRNA levels of known pro and anti-inflammatory cytokines with tribbles using Taqman qRTPCR normalised to GAPDH levels.
Results: In atherosclerotic arteries (n = 8), IL-1β increased threefold (p = 0.0226), IL-1RA increased 4.8 fold (p = 0.0226), IL-10 increased 2.5 fold (p = 0.0138), and IL-18 increased twofold (p = 0.0008) compared with arteries from patients with DCM (n = 6). IL-1α and β TNFα levels were not different. Further, trb-1 increased 2.1 fold (p = 0.0305) while trb-2 levels were unchanged in the atherosclerotic samples. Trb-3 expression levels were below the detection limit. In human aortic smooth muscle cells (HASMC) and human umbilical vein endothelial (HUVEC) stimulated by IL-1β (1 nM) or LPS (100 ng/ml) for 0–48 hours, transient upregulation (up to threefold) of trb-1 was observed in HAMSC but not in HUVEC (n = 3).
Conclusion: These data suggest that trb-1 is a proinflammatory regulator of the smooth muscle cell response in the human atherosclerotic vessel wall. As trb-1 regulates MAPKK activity1 we suggest that this protein may be a key novel component of inflammatory signal processing networks in VSMC.1
1
039 CIRCULATING SYSTEMIC LEVELS OF INTERLEUKIN-6 AND INTERLEUKIN-10. DO THEY INDICATE THE PRESENCE OF A VULNERABLE PLAQUE?
S.-Y.M. Ooi, J. M. McLenachan, D. Thompson, S. G. Ball.Leeds General Infirmary, UK
Background: Peripheral circulating interleukin-6 (IL-6) levels are increased and interleukin-10 (IL-10) levels are decreased in patients with acute coronary syndromes (ACS) and both are independently predictive of future cardiovascular events. However, it is yet to be determined whether this cytokine imbalance identifies the presence of an “at risk” plaque, or is merely part of a generalised systemic inflammatory response.
Objective: To determine whether circulating systemic IL-6 and IL-10 originate from the acute plaque.
Methods: Fourteen stable patients and 10 ACS patients were recruited prior to percutaneous coronary intervention. All patients had single vessel disease and no history of prior myocardial infarction, coronary revascularisation, or concurrent inflammatory, infective, or neoplastic disease. The ACS patients had dynamic ECG changes and raised troponin I levels on admission, and were within 48 hours of their last episode of chest pain. None reached the “old” CK diagnostic criteria for myocardial infarction. Blood samples were taken from the proximal coronary artery (before the culprit lesion), distal coronary artery (beyond the culprit lesion) and the coronary sinus before balloon inflation. These samples were immediately centrifuged and plasma was frozen at −70°C. IL-6 and IL-10 levels were determined using high sensitivity ELISA.
Results: No significant increase in IL-6 levels over the culprit lesion (from proximal to distal coronary artery) was demonstrated in either the stable (4.67 v 4.79 pg/ml; p = 0.143) or ACS (5.20 v 5.42 pg/ml; p = 0.415) patients. IL-6 levels in the coronary sinus were significantly lower than in the distal coronary artery in stable patients (4.29 v 4.79 pg/ml; p = 0.015), but did not differ in the ACS group (5.67 v 5.42 pg/ml; p = 0.669). No significant differences in IL-10 levels were seen either over the plaque or the myocardium in both the stable and ACS patients.
Conclusion: In both stable and ACS patients, neither coronary plaque nor myocardial release of IL-6 and IL-10 contribute significantly to peripheral circulating levels. Thus, circulating levels of IL-6 and IL-10 are not reflective of the inflammatory state of the culprit coronary lesion, but are representative of a generalised systemic inflammatory response.
040 DIAGNOSTIC ACCURACY OF NON-INVASIVE CORONARY ANGIOGRAPHY WITH MULTISLICE COMPUTED TOMOGRAPHY IN PATIENTS PRESENTING WITH ACUTE CHEST PAIN
D. R. Coles, P. Wilde2, C. Rogers, M. Oberhoff, K. R. Karsch, A. Baumbach.Bristol Heart Institute, Clinical Radiology2, Bristol Royal Infirmary, UK
Background: Multislice computed tomography (MSCT) coronary angiography has shown potential to detect coronary artery stenoses in selected elective patient groups. The aim of this prospective clinical trial was to assess the accuracy and clinical relevance of MSCT coronary angiography in patients presenting with acute chest pain.
Methods: 120 consecutive patients (mean age 61.9 years, 65% male) underwent coronary MSCT angiography (Siemens Sensation 16) before a scheduled conventional coronary angiography (CCA). All patients were admitted to the hospital with acute chest pain. Patients with STEMI and patients requiring immediate cardiac catheterisation were excluded. Further major exclusion criteria were atrial fibrillation and renal impairment. Coronary MSCT was acquired with a 16 slice CT, using retrospective ECG gating, 420 msec rotation and collimation: 12×1.0 mm (n = 57) and latterly 16×1.0 mm (n = 63). Blinded visual assessment of coronary MSCT to detect coronary artery disease was performed on a 11 segment model after image quality assessment. The accuracy of coronary MSCT was compared with CCA to detect significant stenoses (>50%).
Results: 113 patients underwent both investigations (8 previous CABG, 7 previous stent). The mean heart rate was 61 (SD 9) bpm. Prevalence of significant coronary artery disease was 74%. 1243 native segments were assessed by MSCT, of which 22% were non-analysable (199 non-diagnostic, 74 not seen). The majority of non-analysable segments were in distal and side branch segments (68%). The overall ability of coronary MSCT to detect the presence of at least one significant stenosis in all native segments had a sensitivity of 92% and specificity 55%, a positive predictive value 86% and negative predictive value of 70%. Coronary calcification was a major cause of inaccuracy. In patients without coronary calcification (n = 10), MSCT angiography had a negative predictive value of 100%.
Conclusion: In this patient cohort with a high prevalence of coronary disease and high levels of coronary calcification, the accuracy of MSCT coronary angiography was less than in previously reported studies on elective patients. The clinical relevance of this technology to screen and risk stratify patients with acute chest pain is limited.
041 PROGNOSTIC VALUE OF CORONARY ARTERY CALCIUM SCREENING IN ASYMPTOMATIC PATIENTS WITH TYPE 2 DIABETES
V. A. Dhakshinamurthy, D. Hopkins, P. Sharp, E. Lim, R. Corder, A. Lahiri.Cardiac Imaging and Research Centre, Wellington Hospital, Northwest London Hospitals NHS trust and William Harvey Research Institute, UK
Background: Type 2 diabetes is associated with accelerated atherothrombosis and high rates of cardiovascular morbidity and mortality. Conventional risk factors have a limited ability to identify diabetic patients with subclinical atherosclerosis, who are at substantial risk of cardiovascular events. Coronary artery calcification is closely associated with extent of histological coronary atherosclerosis and can be detected by electron beam tomography (EBT). We prospectively evaluated the prognostic value of coronary calcium scores to predict cardiovascular events in asymptomatic patients with type 2 diabetes.
Methods: Asymptomatic type 2 diabetic patients without known CAD were recruited from four community based diabetic clinics in northwest London. Traditional risk factors including HbA1c and lipid profile and inflammatory markers (hs-CRP, IL-6) were measured at baseline. All patients underwent coronary artery calcium (CAC) imaging by EBT and were followed up for cardiovascular events (death, myocardial infarction, acute coronary syndrome, late revascularisation, and stroke). A Cox proportional hazard model was used to examine event free survival.
Results: 510 patients were enrolled (mean age 53 (SD 8) years; 61% were male). 236 patients (46.3%) had significant coronary calcification (CAC⩾10 Agatston units). The extent of CAC was mild (11–100) in 19.6%, moderate (101–400) in 15.1%, severe (401–1000) in 6.1%, and extensive (>1000) in 5.5%. 15 cardiovascular events (1 death, 8 myocardial infarctions, 2 acute coronary syndromes, 3 strokes, and 4 late revascularisations) occurred during a mean follow up of 17.9 (5.5) months. Conventional risk factors were associated with coronary calcification in a multivariate logistic regression model. However, only the extent of coronary calcification predicted event free survival in both univariate and multivariate models.
Conclusion: Coronary calcification is highly prevalent in asymptomatic type 2 diabetics and was the single most powerful predictor of event free survival, among the factors examined. This is most likely because it provides an integrated measure of vascular risk that includes both conventional and novel risk factors. Clinical management algorithms incorporating its use merit further investigation.
042 RADIATION DOSE IN CORONARY MULTISLICE CT: A COMPARISON WITH CONVENTIONAL DIAGNOSTIC ANGIOGRAPHY
D. R. Coles, M. Smail2, I. Negus2, P. Wilde3, M. Oberhoff, K. R. Karsch, A. Baumbach.Bristol Heart Institute; 2Medical Physics and Bioengineering; 3Clinical Radiology, Bristol Royal Infirmary, UK
Background: Developments in technology have made multislice CT (MSCT) a viable modality for cardiac imaging. We compared the effective dose from MSCT coronary angiography with that from conventional coronary angiography (CCA). The effective dose from calcium scoring scans is also estimated, together with the effect of ECG controlled tube current modulation for radiation dose reduction. MSCT is a potentially high dose imaging technique and the relative radiation risk should be understood before incorporating it into clinical protocols.
Methods: In a prospective study 94 patients with suspected coronary artery disease underwent both Coronary MSCT (Siemens Sensation 16) and conventional coronary angiography (Siemens Axiom Artis FC/BC). CT exposure data were collected for the complete coronary MSCT protocol including calcium scoring (12×1.5 mm collimation) without (group 1: n = 52) and with ECG controlled tube current modulation (group 2: n = 42). MSCT coronary angiography, including test bolus scans, used either 12×0.75 mm collimation (group 1) or 16×0.75 mm collimation (group 2). Effective doses were estimated using the NRPB/ImPACT CT dosimetry calculator. Exposure data were collected for CCA using a single or biplane system and effective doses were estimated using PCXMC.
Results: The mean effective dose for MSCT coronary angiography including test bolus was 14.5 (SD 2.3) mSv for 12 detectors (group 1) and 15.5 (SD 3.3) mSv for 16 detectors (group 2), while that for CCA was 5.7 (SD 3.7) mSv (group 1) and 5.3 (SD 3.3) mSv (group 2). The mean effective dose for calcium scoring was 4.0 (SD 0.3) mSv, and with ECG controlled tube current modulation prospectively applied mean effective dose was reduced by 35% to 2.6 (SD 0.3) mSv.
Conclusion: The mean effective dose for MSCT coronary angiography was significantly higher than that for CCA. Calcium scoring alone is a relatively low dose technique, particularly if ECG controlled tube current modulation is used. These results demonstrate that coronary MSCT is a high radiation dose examination. Further evaluation and optimisation of patient dose in the clinical setting is needed.
043 PROGNOSTIC POWER OF NORMAL MYOCARDIAL PERFUSION SCINTIGRAPHY WITH 99M-TC AGENTS: THE DGH EXPERIENCE
M. J. Smith, R. Muthusamy, S. Mahon.Rotherham General Hospitals NHS Trust, UK
Introduction: Studies demonstrating the favourable prognosis for patients with normal myocardial perfusion scintigraphy (MPS), originate mainly from teaching centres in the USA. We have analysed survival of patients who have undergone routine MPS in our district general hospital (DGH) to see if the same applies.
Methods: Retrospective analysis of results from all patients undergoing MPS over a 6 year period. Scans were graded “normal or “abnormal” based on the text of the reports. Survival status was ascertained from records of deaths of Rotherham residents, all of which are notified to the hospital. Causes of death were determined from death certificates.
Results: See figure. Altogether 1166 MPS studies were conducted, but 75 were excluded from analysis (48 non-Rotherham residents, 27 incomplete/non-diagnostic); 640/1091 (59%) included scans were abnormal. During follow up (mean duration 50 (SD 21) months), 105 deaths occurred; 61 had cardiac disease listed as a cause; 6/61 had normal MPS, 55/61 abnormal MPS. The increased cardiac related death rate in patients with abnormal MPS compared with normal MPS was highly significant (p<0.0001, hazard ratio 6.5, 95% CI 3.9 to 10.9). The estimated mean rate of death from cardiac disease in patients with normal MPS was 0.3% per year.
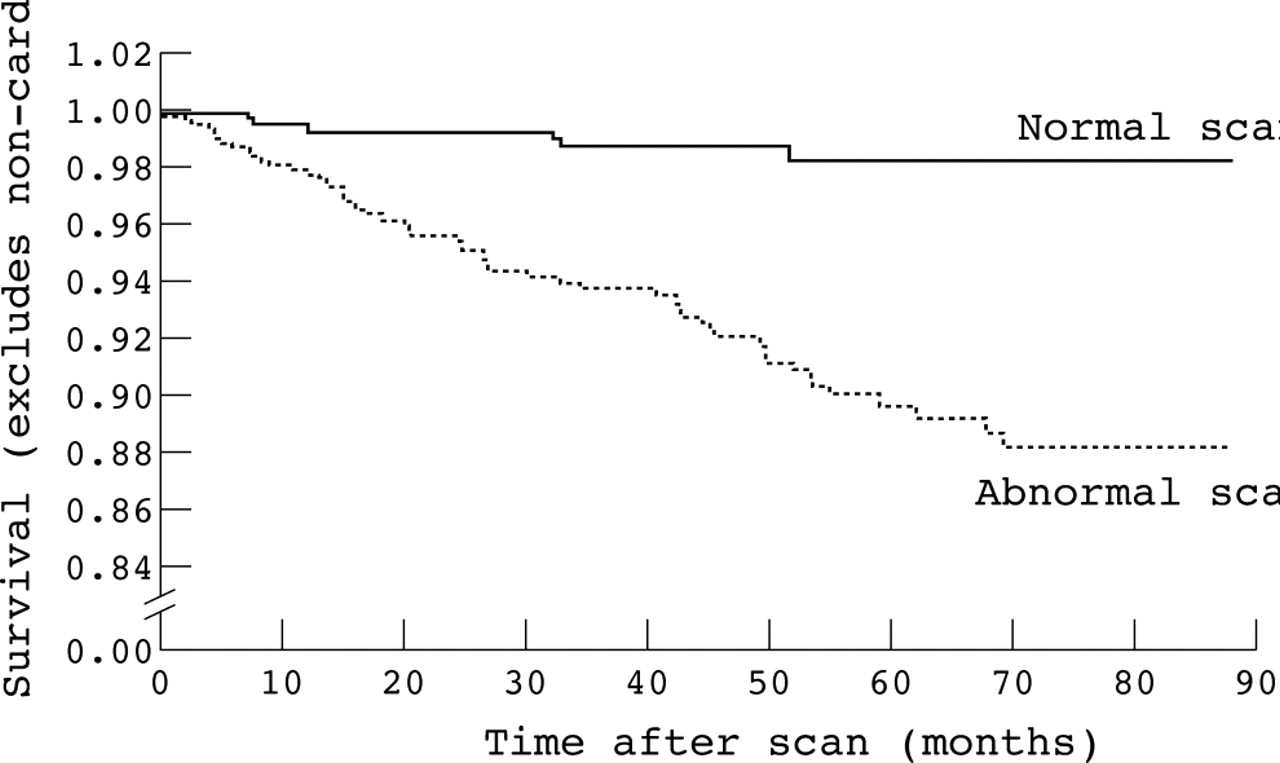
Abstract 43
Conclusion: This study appears to confirm a favourable prognosis associated with a normal MPS scan in routine clinical practice in our DGH.
044 MYOCARDIAL PERFUSION SCINTIGRAPHY PREDICTS FUNCTIONAL OUTCOME FOLLOWING PERCUTANEOUS CORONARY INTERVENTION
M. B. Al-Housni, F. Hutchings, M. Dubowitz, R. Grocott-Mason, M. Mason, C. Ilsley, A. D. Kelion.Nuclear Medicine Department, Harefield Hospital, UK
Introduction: Myocardial perfusion scintigraphy (MPS) is often used to assess the physiological significance of angiographic coronary stenoses. However, there has been no prospective blinded study demonstrating that MPS predicts functional benefit following revascularisation.
Methods: Thirty three consecutive patients (age 63 (SD 10) years, male 22) awaiting elective percutaneous coronary intervention (PCI) underwent MPS using a one day stress rest Tc-99m-tetrofosmin SPECT protocol. Studies were analysed semiquantitatively scoring 17 segments 0–4. All patients subsequently underwent the planned PCI, and the interventionalist was blinded to the result of MPS. Treadmill exercise time was compared before (at the time of MPS) and 6 months after PCI; supervising staff were blinded to the MPS and angiographic findings.
Results: Fifteen (45%) patients had angina, six (18%) non-cardiac sounding chest pain, and 12 (36%) no chest pain. Seven could not perform treadmill exercise and five suffered a cardiac event between PCI and follow up; these were excluded from further analysis. Improvement in exercise time increased with summed difference score (SDS) (see fig). The improvement was +1.7 (SD 2.3) minutes for patients with SDS >3 versus −0.8 (SD 2.8) minutes for those without significant inducible hypoperfusion.

Abstract 44
Conclusion: Only patients with significant inducible hypoperfusion on Tc-99m-tetrofosmin SPECT demonstrated objective functional improvement following PCI. MPS is a valuable method of selecting patients for revascularisation.
045 ISOLATED LEFT VENTRICULAR NONCOMPACTION: TWO YEAR EXPERIENCE WITH CARDIOVASCULAR MAGNETIC RESONANCE
Z. R. Yousef, S. Chalil, C. Gibbs, P. Jordan, R. E. A. Smith, F. Leyva.Department of Cardiology, Good Hope Hospital, Sutton Coldfield, West Midlands, UK
Introduction: Isolated left ventricular non-compaction (ILVNC), a rare dysembreogenic cardiomyopathy with hypertrabeculation (HTb) of the left ventricle (LV), can present as heart failure (HF), thromboembolism (TE), and/or arrhythmias (AR) in adults. We describe a cohort of patients with HTb of the LV identified from referrals to a tertiary cardiovascular magnetic resonance (CMR) service over two years.
Methods: CMR (1.5T GE Signa) consisted of gradient echo sequences (FIESTA) and gadolinium (Gd) DTPA-enhanced 1st pass and delayed imaging using multiphase inversion recovery fast gradient recalled echo (IR-FGRE). Non-compacted (NC) myocardium was suggested by HTb of the LV and intra-trabecular perfusion with Gd during 1st pass imaging. Compacted (C) and NC areas were quantified by planimetry of end-diastolic two chamber views. Standard electrocardiographs (ECG), and transthoracic echocardiograms (TTE) were recorded.
Results: Of 446 CMR studies, 21 cases of LV HTb were identified. Of these, 14 presented with typical symptoms of ILVNC (ILVNC-gp; prevalence 0.03%); HF (n = 9), TE (n = 2), and AR (n = 3). The remaining seven patients (non-ILVNC gp) included patients screened for Marfan’s syndrome (n = 1), sudden cardiac death (n = 2), and familial dilated cardiomyopathy (n = 1), and atypical chest pain (n = 3). The ECG was abnormal in 80% of the ILVNC-gp; bundle branch block (n = 8), LV hypertrophy (n = 2), and atrial fibrillation (n = 2). ECG abnormalities were present in 40% of the non-ILVNC gp; bundle branch block (n = 1), LV hypertrophy (n = 2). TTE failed to identify HTb of the LV in all 21 cases. Concentric LV hypertrophy by TTE was present in all non-ILVNC patients, and in 12 of the 14 ILVNC-gp. In the remaining two ILVNC patients, TTE suggested apical LV hypertrophy. CMR derived C:NC ratio for the ILVNC-gp was 2.11, and for patients presenting with HF; 2.25, TE; 2.52, and AR; 1.41. C:NC ratio for the non-ILVNC gp was 1.35 (p<0.01 for ILVNC-gp v non-ILVNC gp)
Conclusion: ILVNC is a spectrum comprising dysrrhythmias, left ventricular dysfunction, and thromboembolism. The superior spatial resolution of CMR compared to TTE allows for greater differentiation of C from NC. The prevalence of ILVNC may be considerably higher than previously reported by TTE studies.
046 PLASMA OSTEOPROTEGERIN LEVELS PREDICT THE EXTENT OF SUBCLINICAL CORONARY ATHEROSCLEROSIS AND ADVERSE CARDIAC EVENTS IN ASYMPTOMATIC TYPE 2 DIABETIC SUBJECTS
V. A. Dhakshinamurthy, A. Lahiri, E. Lim, R. Corder.Cardiac Imaging and Research Centre, Wellington Hospital and William Harvey Institute, Queen Mary University of London, UK
Background: Osteoprotegerin (OPG) is a novel member of the tumour necrosis factor receptor superfamily which exerts anti-inflammatory effects on the coronary vasculature. Arterial calcification is a prominent feature of atherosclerosis which has been strongly linked with cardiovascular events (CV) events. As type 2 diabetic patients have an increased risk of CV events, we prospectively evaluated the relation between plasma OPG levels, the extent of subclinical coronary atherosclerosis, and CV events in this patient group.
Methods: Asymptomatic type 2 diabetic patients without prior coronary disease were recruited from four community based diabetic clinics in northwest London. Traditional risk factors including HbA1c and lipids, inflammatory markers (hs-CRP, IL-6) and plasma OPG levels were measured at baseline. All patients underwent coronary artery calcium (CAC) imaging by electron beam tomography and were followed up for CV events (death, MI, acute coronary syndrome, late revascularisation, and stroke). Multivariate logistic regression analysis was performed to evaluate predictors of CAC. A Cox proportional hazard model was used to examine event free survival.
Results: 510 patients were enrolled (mean age 53 (SD 8) years; 61% male). 236 patients (46.3%) had significant CAC (⩾10 Agatston units). The extent of CAC was mild (11–100) in 19.6%, moderate (101–400) in 15.1%, severe (401–1000) in 6.1%, and extensive (>1000) in 5.5%. The median hs-CRP, IL-6, and OPG levels were 4.28 mg/l (1.72–8.01), 1.93 pg/ml (1.2–3.1), and 6.82 pmol/l (4.68–11.55) respectively. 15 CV events occurred during a mean follow up of 17.9 (5.5) months. OPG levels correlated with increasing CAC scores (r = 0.40, p<0.0001) and adverse CV events (hazard ratio in patients with OPG >9.52 pmol/l = 5.76 (1.3–26)). In the multivariate model, OPG levels also predicted increased CAC in addition to age, male sex, hypertension, and statin use.
Conclusion: A high proportion (46.3%) of asymptomatic diabetic patients has significant subclinical atherosclerosis based on CAC imaging. Of the biochemical markers studied, only increased OPG levels predicted both subclinical disease and near-term CV events. Hence, measurement of plasma OPG merits further investigation as a simple test for identifying high risk diabetic patients.
047 IMPROVED HAEMODYNAMIC PROFILE AND LEFT VENTRICULAR FUNCTION FOLLOWING AORTIC VALVE REPLACEMENT WITH A STENTLESS RATHER THAN STENTED BIOPROSTHESIS: A RANDOMISED CONTROLLED TRIAL
R. Graham, J. Thambyrajah, M. Stewart, S. Kendall, S. Hunter.The James Cook University Hospital, Middlesbrough, UK
Introduction: Stentless bioprosthetic valves are considered to have a superior haemodynamic profile compared to stented bioprostheses for aortic valve replacement (AVR), but it is not certain that this translates to improved left ventricular (LV) remodelling and function. This randomised controlled trial was designed to compare the effects of stentless versus stented bioprosthesis following AVR using echocardiography.
Methods: Fifty four patients (35 male, mean age 73 years) undergoing bioprosthetic AVR were randomised to either Sorin Freedom stentless (n = 28) or Sorin More stented (n = 26) valves. Standard echocardiography, including tissue Doppler imaging to assess peak systolic velocity of the mitral annulus (S′) as a measure of long axis function, was performed preoperatively and 6 months postoperatively. There was no significant difference in baseline characteristics between the two groups. The aortic valve area (AVA), left ventricular mass index (LVMI), LV ejection fraction (LVEF), and S′ at 6 months following AVR are depicted in the table below (values quoted as mean (SD)).
Abstract 47
Conclusion: The stentless aortic valve bioprosthesis results in a larger aortic valve area, greater regression of left ventricular hypertrophy, and improved recovery of long axis function at 6 months. These data suggest that the stentless aortic valve is associated with improved haemodynamic profile and better cardiac function.
048 A RANDOMISED COMPARISON OF STENTLESS VERSUS STENTED VALVES FOR AORTIC STENOSIS
D. Perez de Arenaza, B. Lees, M. Flather, F. Nugara, M. Khan, J. Pepper on behalf of the ASSERT InvestigatorsClinical Trials and Evaluation Unit, Royal Brompton Hospital, UK
Introduction: Aortic valve replacement (AVR) is the established treatment for severe aortic stenosis. The main objective is to achieve a reduction in left ventricular mass. Stentless porcine valves have been introduced to reduce obstruction and maximise flow area. We conducted a randomised controlled trial to compare a stentless with a stented valve in adults with severe aortic stenosis. The primary outcome measure was left ventricular (LV) mass and LV function, measured by transthoracic echocardiography, and in a subset, by magnetic resonance imaging (MRI).
Methods: Measurements were taken before valve replacement and at 6 and 12 months. Patients undergoing AVR with an aortic annulus <25 mm diameter were randomly allocated to a stentless (Freestyle) (n = 93) or a stented supra-annular (Mosaic) (n = 97) valve. Mean age was 71 years, (range 40–86 years), 55% male, mean annulus size 23 mm (range 19–25 mm).
Results: There were no significant differences in index LV mass between the stentless versus stented groups respectively at baseline (180 (SD 61) and 180 (SD 63) g/m2) or at 6 months (142 (SD 48) and 129 (SD 45) g/m2) although within-group changes from baseline to 6 months were highly significant and reached the normal range in both groups. Changes in LV mass measured by MRI in a subset of 38 patients were consistent with the echo findings. There was a greater reduction in peak aortic velocity with the stentless compared with the stented from baseline (4.3 (SD 0.7) and 4.4 (SD 0.7) m/sec) to 6 months (2.1 (SD 0.5) and 2.7 (SD 0.5) m/sec; p<0.001) and a greater increase in indexed effective orifice area (EOA) in the stentless group from baseline (0.42 (SD 0.17) and 0.40 (SD 0.19) cm2/m2) to 6 months (1.03 (SD 0.31) and 0.77 (SD 0.28) cm2/m2; p<0.001). Mean cardiopulmonary bypass time was greater for stentless valves compared to stented (133 v 99 min, p<0.001). There were no differences in clinical outcomes between the two valve groups.
Conclusion: The use of stentless or stented valves leads to similar reductions in LV mass at 6 months, which persist at 12 months, despite significant differences in EOA and peak flow velocity in favour of the stentless valve.
049 AN OPERATION FOR THE MARFANOID AORTA WHICH SPARES THE AORTIC VALVE AND THE VASCULAR INTIMA: ROBISCEK’S CONCEPT REALISED BY A RAPID PROTOTYPING ENGINEERING SOLUTION
J. Pepper, R. Mohiaddin, R. H. Anderson, T. Treasure.The Royal Brompton Hospital, Guy’s Hospital, Great Ormond Street Hospital and Imperial College, London, UK
Introduction: Replacement of the ascending aorta in Marfan’s syndrome is an exercise in brinkmanship; if the aorta dissects, one has left it too late—if it has not dissected, one may be intervening unnecessarily. Typically, young people suffer years of anxiety provoking echo measurements until some criteria are met to justify root replacement. A mechanical valve commits to lifelong anticoagulation; valve sparing surgery requires great skill and is uncertain. Our objective is to move from “the workmanship of risk” towards “the workmanship of certainty” (Pye 1968). In this new approach the individual’s MRI data are used to sculpt an exact model of the ascending aorta by “rapid prototyping”.
Methods and Results: On the model, a tight-fit macroporous external support is manufactured, 5% undersized. On 24 May 2004 the first recipient had his tailor made support placed around his ascending aorta, from proximal to the coronaries to beyond the subclavian artery. The operation does not require cardiopulmonary bypass, cooling, or any other interference to blood flow to the heart or the brain. The patient is now completely well. The before (left; see fig) and after MRIs show a barely discernable increased signal from the aortic wall. The valve and the natural blood/endothelium interface are entirely undisturbed.

Abstract 49
Conclusion: This is a low risk, prophylactic operation for patients without aortic regurgitation. It is unusual to present a surgical “first”. Harken took nine pages of the NEJM in 1948 to report his first successful mitral valvotomy. We believe that before an aorta is allowed to expand too far, and is resected along with the valve, both surgeon and patient should know of this alternative.
050 PRESENTATION AND OUTCOME OF MARFAN’S SYNDROME PATIENTS WITH TYPE B DISSECTION AND THORACOABDOMINAL AORTIC ANEURYSM
B. Davies, K. Kotidis, M. Kalkat, V. Singh, D. Pagano, R. Bonser.Department of Cardiothoracic Surgery, Queen Elizabeth Hospital, Edgbaston, Birmingham, UK
Background: Patients with Marfan’s syndrome frequently develop aneurysms or dissections involving multiple segments of the aorta. Replacement of these segments may improve life expectancy. Recognised indications for intervention and graft replacement of the thoracoabdominal aorta segment include impending rupture, visceral or limb malperfusion, or an aortic diameter ⩾5.5 cm.
Methods: We retrospectively analysed prospectively collected data on 13 patients (6 male), mean age of 40.9 years (range 30–52) with Marfan’s syndrome and TAAA. Serial pre-operative minimum aortic short-axis diameters were measured using a calliper method. Differences in measured dimensions were analysed using Mann-Whitney and Wilcoxon’s signed ranks tests.
Results: All patients had residual type A or chronic type B dissection. Five out of 13 had undergone previous proximal aortic surgery. Two patients presented with acute rupture, two with airway obstruction and one with intermittent paraplegia after noting an increasing expansion rate. Aortic dimension prior to surgery in all, elective and emergency/urgent patients were 7.65 cm (IQR 5.85, 9.08), 7.49 (IQR 5.68, 8.99) and 7.65 cm (IQR 5.85, 9.16) (all values medians). There was no significant difference between these groups. Expansion rate prior to operation was median 3.09 (IQR 1.12, 4.43). In the year immediately prior to surgical intervention, linear expansion rate increased significantly from a background of 0.145 to 2.92 cm/yr (p = 0.057). All patients underwent Crawford II TAAA repair utilising profound hypothermia, CSF drainage (10/13) and/or HCA (10/13). There was no early mortality, paraplegia, nor any requirement for renal replacement therapy. The mean CPB time (mins), ITU LOS (days) and hospital LOS (days) were 213, 8.4 and 18.9 respectively. After a median follow-up of 33 months (6–60) there remains 100% survival.
Conclusion: Patients with Marfan’s syndrome are prone to multifocal thoracic aortic pathology, which in the descending segment include Crawford extent II aneurysms and associated dissection. These may be independent or co-exist with proximal aortic pathology. Using contemporary techniques, thoracoabdominal aortic aneurysm repair can be undertaken with low mortality and morbidity.
051 PATIENT PROSTHESIS MISMATCH IN AORTIC VALVE REPLACEMENT—SIZE DOES NOT MATTER
N. Howell, E. Coby, S. George, V. Barnet, R. Bonser, B. Keogh, T. Graham, S. Rooney, I. Wilson, D. Pagano.Department of Cardiothoracic Surgery, University Foundation Hospital Birmingham, Birmingham, UK
Objectives: Prosthesis mismatch (PPM) has been reported to increase perioperative mortality and reduce postoperative survival in patients undergoing aortic valve replacement (AVR). We analysed the effect of PPM on survival following AVR in our unit.
Methods: Prospectively collected data on patients who had undergone AVR (± coronary artery revascularisation) since 1997 were analysed. Functional in vitro valve effective orifice area (EOA) and geometric prosthesis internal orifice area assuming a circular orifice shape (GOA) were evaluated. The values were indexed to body surface area (cm2/m2). PPM was defined as EOAi <0.6 (EOAM) and/or GOAi <1.1 (GOAM). Survival data from hospital discharge was obtained from the Institute of National Statistics.
Results: Twelve per cent of patients (137/1119) had severe PPM. There were 52/1119 in-hospital deaths (overall mortality 4.65%) with no difference between the groups (10/137 PPM v 42/982 Controls p = 0.13). Survival data (median 36 months; interquartile range 17–55 months) was available on 909 out of 1067 patients discharged from hospital. There were 85 deaths (8/105 PPM v 77/727 Controls). The 5 year survival estimate was similar for both groups (90.7% PPM (98 survivors); 85.7% (660 Survivors) Control; p = 0.37). Cox-hazard analysis identified advanced age as the only predictor of reduced survival (age >80 RR 2.43; 95% CI 1.28-4.586; p = 0.007)
Conclusion: In this study PPM at values previously considered severe did not affect perioperative mortality or mid-term survival.
052 ANTICOAGULATION CONTROL AND OUTCOME IN PATIENTS WITH SECOND GENERATION MECHANICAL HEART VALVES
B. C. Reeves, K. C. Santo, J. Wild, A. J. Bryan, G. D. Angelini.Bristol Heart Institute, Bristol, UK
Objectives: Longitudinal data for participants in a randomised controlled trial of second generation mechanical heart valves (St Jude and Carbomedics) were analysed, to investigate the association between quality of Anticoagulation (AC) and outcome.
Methods: Patients were categorised by the location of the implanted valve(s): (a) aortic valve replacement (AVR); (b) mitral valve replacement with or without an aortic valve replacement (MVR+/−AVR). AC was calculated as the percentage of follow-up time in range (TIR). Two target international normalised ratio (INR) ranges were considered: (i) 2.5 to 3.5 irrespective of group; (ii) 2.5 to 3.0 for the AVR group and 3.0 to 3.5 for MVR+/−AVR group. Three outcomes were investigated, valve-related death, non-fatal thromboembolic and haemorrhagic events resulting in admission to hospital. Survival free from different events were described using Kaplan Meier curves, the hazard ratios for different measures of AC were estimated using Cox regression modelling, after adjusting for key prognostic variables.
Results: Of 484 participants recruited to the trial, 24 died within 30 days and 26 died from other causes without INR follow-up; 412 (median duration of follow up 7.0 years) were included in the analysis (AVR, n = 245;MVR+/-AVR, n = 167). Cumulative 5-year valve related death (VRD) rates were 0.4% (95% CI 0.1 to 3.1) and 2.5% (95% CI 1.0 to 6.6) respectively; 5-year haemorrhagic or thromboembolic event or VRD rates were 13.3% (95% CI 9.6 to 18.3) and 21.7% (95% CI 16.1 to 28.9). AC was poor based on target ranges (i) and (ii), 31% and 5% of patient respectively had TIR> = 67%. There were no consistent associations between AC and outcome for either group or target range.
Conclusion: Outcome was not associated with AC. VRDs and other serious events were infrequent, despite generally poor AC, implying that second generation mechanical valves are safe.
053 RELATIONSHIP BETWEEN MILD RENAL DYSFUNCTION AND OUTCOMES AFTER CORONARY ARTERY BYPASS GRAFTING
R. Zakeri, N. Freemantle, V. Barnett, R. S. Bonser, T. R. Graham, S. J. Rooney, I. C. Wilson, R. Cramb, B. E. Keogh, D. Pagano.Cardiothoracic Surgical Unit, University Hospital Birmingham, Birmingham, UK
Background: Risk stratification algorithms for coronary artery bypass grafting (CABG) do not include a weighting for preoperative mild renal impairment defined as a serum creatinine 130–199 μmol/L (1.47–2.25 mg/dL), which may impact on mortality and morbidity following CABG.
Methods and results: We reviewed prospectively collected data between 1997 and 2004 on 4403 consecutive patients undergoing first-time isolated CABG, with a preoperative serum creatinine <200 μmol/L (2.26 mg/dL) in a single institution. The in-hospital mortality was 2.5% (112/4403), need for new dialysis/haemofiltration 1.3% (57/4403), and stroke rate 2.5% (108/4403). There were 458 patients with a serum creatinine 130–199 μmol/L or 1.47–2.25 mg/dL (mild renal dysfunction group) and 3945 patients with a serum creatinine <130 μmol/L (<1.47 mg/dL). Operative mortality was higher in the mild renal dysfunction group (2.1% v 6.1% p<0.001) and increased with increasing preoperative serum creatinine level. New dialysis/haemofiltration (0.8%v 5.2%; p<0.001) and postoperative stroke (2.2% v 5.0%; p<0.01) were also more common in the patients with mild renal impairment. Multivariate analysis adjusting for known risk factors confirmed preoperative mild renal impairment (creatinine 130–199 μmol/L or 1.47–2.25 mg/dL) (odd ratios 1.91–95% CI 1.18 to 3.03; p = 0.007) or glomerular filtration rate estimates <60 ml/min/1.73 m2, derived using the Cockroft-Gault formula, (odds ratio 1.98 95% CI 1.16 to 3.48; p = 0.015) as independent predictors of in-hospital mortality. Preoperative mild renal dysfunction adversely affected the 3-year survival probability following CABG (93% v 81%; p<0.001).
Conclusion: Mild renal dysfunction is an important predictor of outcome in terms of in-hospital mortality, morbidity and mid-term survival in patients undergoing CABG.
054 ATORVASTATIN IMPROVES ENDOTHELIAL FUNCTION AND DECREASES THE EXPRESSION OF PROINFLAMMATORY CYTOKINES AND ADHESION MOLECULES IN PATIENTS WITH HEART FAILURE
D. Tousoulis, C. Antoniades, M. Kotsopoulou, E. Bosinakou, K. Marinou, M. Charakida, J. Lee, C. Shirodaria, C. Pitsavos, C. Stefanadis.Athens University Medical School, A’ Cardiology Department, Athens, Greece
Background: Heart failure is characterized by endothelial dysfunction, while inflammatory molecules such as interleukin-6 (IL-6), tumor necrosis factor alpha (TNF-a), monocyte chemoattractant protein-1 (MCP-1), and soluble vascular cell adhesion molecule (sVCAM-1) are implicated in the pathogenesis of heart failure. We evaluated the effect of atorvastatin on endothelial function and inflammatory process in patients with heart failure.
Methods: Thirty-seven patients with heart failure (33 males, 4 females, aged 69 (SD 2.3) years old, NYHA II-IV with ejection fraction <35%) were enrolled. Nineteen patients received atorvastatin 10 mg/day while 18 (control group) received no statin for 4 weeks. Forearm blood flow was measured by venous occlusion strain-gauge plethysmography. Endothelium dependent dilation (EDD) and endothelium independent dilation (EID) were expressed as the % change of flow from baseline to the maximum flow during reactive hyperemia or after sublingual nitroglycerin administration respectively. Serum levels of sVCAM-1, IL-6, MCP-1 and TNF-a were determined by ELISA.
Results: Basal forearm blood flow remained unchanged in both groups after treatment. EDD was significantly increased in atorvastatin group (from 44.2% (4.5) to 89.5% (12.0) p<0.01) but not in controls (from 47.2% (4.7) to 43.1% (5.4), p = NS). Levels of sVCAM-1, IL-6 and TNF-a were significantly decreased in atorvastatin group (from 650.7 (61.7), 7.69 (0.69) and 3.8 (0.35) to 471.6 (44.5) ng/ml, 6.02 (0.81) pg/ml and 2.8 (0.22) pg/ml respectively, p<0.05 for all) but not in controls (from 656.2 (70.0), 7.30 (0.72) and 4.5 (0.62) to 643.9 (71.1) ng/ml, 6.31 (0.81) pg/ml and 4.53 (0.61) pg/ml respectively, p = NS for all). EID and levels of MCP-1 remained unchanged in both atorvastatin-treated (from 66 (8) and 305.9% (29.7) to 65% (6) and 291.4 (26.1) ng/ml respectively, p = NS for both) and control group (from 66 (8) and 311.0 (26.0) to 60(7%) and 321.5 (19.6) ng/ml respectively, p = NS for both).
Conclusion: Atorvastatin improves endothelial function and decreases the expression of IL-6, TNF-a and sVCAM-1 in patients with heart failure. These findings indicate that statins may have further antiinflammatory effects in patients with heart failure, beyond their lipid-lowering effects.
055 ACTIONS OF ALDOSTERONE BLOCKADE IN PATIENTS WITH MILD-MODERATELY SEVERE HEART FAILURE
C. Berry, N. Murphy, G. deVito, S. Galloway, A. Seed, C. Fisher, W. S. Hillis, N. Sattar, P. Vallance, J. J. V. McMurray.University of Glasgow, University of Strathclyde, University College Hospital
Background: Aldosterone receptor blockade with spironolactone (SP) improves prognosis in severe heart failure (HF), however, the effects of this drug in patients with mild-moderate HF treated with a beta-blocker are uncertain.
Methods: We conducted a randomised, double-blind, placebo (P) controlled study of SP (25 mg daily) in patients with optimally treated HF due to left ventricular systolic dysfunction. Blood was collected at baseline and after 12 weeks for measurement of arginine vasopressin (AVP), b-type natriuretic peptide (BNP), a marker of collagen turnover (procollagen type III N-terminal amino peptide (PIIINP)), and endogenous inhibitors of nitric oxide synthase (asymmetric dimethylarginine (ADMA)). Heart rate variability and cardiopulmonary function at rest or in response to exercise were also quantified. Compliance with study treatment was confirmed by pill-counts. Comparisons of mean (standard deviation (SD)) change in variables between P and SP-treated groups were performed using ANOVA with correction for baseline differences.
Results: 40 patients with NYHA class I (20%); II (70%) or III (10%) HF were randomised. SP-treated patients were older (mean (SD) age 65 (SD 7.4) years v 59 (9.5) years, but the groups were well matched otherwise. Two P-treated patients did not complete the study. No changes were observed in any of the study tests in the P-treated patients. In SP-treated patients, an increase from baseline was observed in serum potassium concentration: 4.4 (0.4) mmo/L to 4.7 (0.5) mmol/L, p = 0.05. Decreases from baseline in the SP group were found in the plasma concentrations of PIIINP: 3.5 (1.0) mmolL to 2.9 (0.6) mmolL, p = 0.04; BNP: 116 (140) pg/ml to 53 (64) pg/ml, p = 0.09 and ADMA: 0.7 (0.2) mmolL to 0.5 (0.05) mmolL; p = 0.008. Creatinine clearance decreased by −39.1 (39.8) mL/min in SP-treated patients. No other between-group differences were observed.
Conclusion: Aldosterone receptor blockade resulted in potentially beneficial changes in potassium and some biomarkers. Although renal function declined, SP was well tolerated.
056 EFFECTS OF OPTIMAL PHARMACOLOGICAL TREATMENT ON LEFT VENTRICULAR REMODELLING, SYSTOLIC AND DIASTOLIC FUNCTION IN PATIENTS WITH CHRONIC HEART FAILURE
N. P. Nikitin, K. K. A. Witte, J. Ghosh, R. de Silva, A. L. Clark, J. G. F. Cleland.University of Hull, Kingston upon Hull, UK
Background: Studies conducted prior to the widespread introduction of ACE inhibitors and beta-blocker therapy suggested that left ventricular (LV) remodelling was an important mechanism driving the progression of LV systolic dysfunction and chronic heart failure (CHF). This prospective observational study was designed to investigate whether adverse LV remodelling occurs in patients with CHF despite optimal pharmacological treatment.
Methods: 220 patients (aged 67 (SD 11) years) with symptomatic CHF and persistent LV systolic dysfunction (ejection fraction <45%) despite >6 months treatment with beta-blockers and ACE inhibitors/ARBs underwent serial echocardiography with LV end-diastolic volume (EDV), end-systolic volume (ESV), ejection fraction (EF), and Doppler indices of LV diastolic filling measured at baseline, 6, 12 and 24 months.
Results: 44 patients died and 3 patients underwent heart transplantation (non-survivors) during the 2-year follow-up. In 158 patients who completed the study (survivors) there was a decrease in heart rate (64 (12) v 72 (14) bpm, p<0.001), LV EDV and ESV (195 (72) v 219 (72) ml, p<0.001 and 121 (53) v 144 (56) ml, p<0.001, respectively) while EF improved significantly (39 (8) v 35 (6) %, p<0.001). At 2 years, 47.5% of the patients showed a reduction in LV ESV>15% from baseline, 9.5% showed an increase in ESV>15% and 43% showed no change. There were no significant differences in baseline echo-characteristics of these 3 subgroups. In non-survivors, no evidence of progressive adverse LV remodelling was observed prior to death. The non-restrictive pattern of LV diastolic filling was more common among survivors compared to non-survivors (60 v 41%, p = 0.026), and its prevalence diminished over the course of treatment in survivors from 27 to 14% (p = 0.009).
Conclusion: Most patients with CHF already receiving chronic therapy with beta-blockers and ACE inhibitors/ARBs do not demonstrate progressive LV remodelling or deteriorating LV systolic function. Death is seldom preceded by progressive LV remodelling in patients on optimal medical therapy. Optimal treatment also leads to less restrictive LV diastolic filling which may have prognostic significance.
057 TESTOSTERONE THERAPY IN MEN WITH HEART FAILURE: A DOUBLE BLIND PLACEBO CONTROLLED TRIAL
C. J. Malkin, P. J. Pugh, J. N. West, E. van Beek, T. H. Jones, K. S. Channer.Department of Cardiology, Royal Hallamshire Hospital, Sheffield. Academic Unit of Endocrinology, University of Sheffield, UK
Background: Chronic heart failure is associated with maladaptive and prolonged neurohormonal and pro-inflammatory cytokine activation causing a metabolic shift favouring catabolism, vasodilator incapacity, and loss of skeletal muscle bulk and function. In men, androgens are important determinants of anabolic function and physical strength and also possess anti-inflammatory and vasodilatory properties.
Methods: We conducted a randomised, double blind, placebo controlled parallel trial of testosterone replacement therapy (5 mg Androderm®) at physiological doses in 76 men (mean age 64 years) with heart failure (mean ± SEM ejection fraction, 32.5% (SD 1.3%)) over a maximum follow-up period of 12 months. The primary endpoint was functional capacity as assessed by the incremental shuttle walk test (ISWT).
Results: At baseline, 18(24%) had serum testosterone below the normal range (total testosterone <7.5 mmol/L and/or bioavailable testosterone <2.5 nmol/L) and testosterone level correlated with distance walked on the initial ISWT (r = 0.3, p = 0.01). Exercise capacity significantly improved on testosterone therapy compared with placebo (mean treatment effect (95% CI) at 6 months 38 m (11.6 m to 64 m, p = 0.006) corresponding to an 18% (4 to 31%, p = 0.01) improvement from baseline. The increase in exercise capacity in the treatment group (19.2 (8.3) metres) was positively correlated with the rise in serum testosterone level (2.02 (0.9) nmol/L), (rS = 0.36, p = 0.02). Symptoms improved by at least one New York Heart Association functional class on testosterone in 13(35%) v 3 (8%) on placebo (p = 0.01). No significant changes were found in handgrip strength, skeletal muscle bulk by cross sectional computed tomography nor in cytokine activation. Testosterone therapy was safe with no excess of adverse events although the patch preparation was not well tolerated by the study patients.
Conclusion: The correction of the metabolic maladaptations of heart failure by drug therapies has proven efficacy. Many patients with heart failure very low levels of serum testosterone and most have borderline androgen deficiency. Testosterone replacement therapy improves functional capacity and symptoms in men with moderate to severe heart failure.
058 THE EFFECT OF SMOKING AND OTHER LIFESTYLE FACTORS ON THE LEFT VENTRICULAR GROWTH RESPONSE TO EXERCISE IN 312 YOUNG HEALTHY MEN ASSESSED USING CARDIOVASCULAR MAGNETIC RESONANCE
J. R. Payne1, M. World2, S. E. Humphries1, D. J. Pennell3, H. E. Montgomery1.1University College London; 2Royal Centre for Defence Medicine; 3Royal Brompton Hospital, UK
Introduction: Increasing left ventricular (LV) mass is a risk factor for cardiovascular (CV) morbidity and mortality. In this study we are the first to examine the role of lifestyle and CV risk factors on exercise-induced LV growth in response to a defined stimulus.
Methods: LV mass was measured using cardiovascular magnetic resonance (CMR) in 312 British Army recruits before and after an identical 12-week physical training program. Age, height (Ht), body weight (Wt), systolic and diastolic blood pressure (SBP and DBP respectively) recorded twice, indices of physical activity (IPA), alcohol consumption (AC) and smoking status (SS) prior to training were documented. Data are presented as mean SD.
Results: Pre-training LV mass increased from 164.8 (SD 24).9 g to 168.7 (24.0) g post-training (p<0.0001). Mean change in LV mass (ΔLVM) was +3.68 (11.8) g. By univariate analysis, SS was associated with ΔLVM (1.4 (13.5) g v 4.8 (10.2) g for (never smokers) v (ex- and current smokers) respectively, p = 0.026). There was a non-significant positive association of SBP with ΔLVM. Neither age, Ht, DBP, AC, nor IPA were significantly associated with ΔLVM. Multivariate analysis showed independent predictors of ΔLVM were Wt, SS, and SBP with incremental R2 = 3.4%, 4.8% and 2.1%; p = 0.004, 0.025, and 0.020 respectively. The association of SS with ΔLVM was explored in ex- and current smokers combined: for those smoking (<20) v (> = 20) cigarettes per day, %ΔLVM was 2.8 (6.0%) v 7.5 (7.9%) respectively, p = 0.021; whilst for those who have smoked for (<4) v (4 to 7.9) v (>8) years, %ΔLVM was 2.7 (6.3%) v 2.8 (6.2%) v 7.4 (5.5%) respectively, p = 0.012. The use of raw (rather than %) ΔLVM, or exclusion of ex-smokers did not alter these findings.
Conclusion: We have shown that smoking and SBP are positively associated with ΔLVM using a prospective model, a defined stimulus, a large number of subjects and CMR (a highly reproducible measure of LV mass). In addition, our demonstration that smoking may influence LV mass in young men is important given the relatively limited exposure of these subjects to smoking.
059 EFFECT OF DOBUTAMINE STRESS ON LEFT VENTRICULAR FILLING IN ISCHAEMIC CARDIOMYOPATHY: PATHOPHYSIOLOGY AND PROGNOSTIC IMPLICATIONS
A. Duncan, E. Lim, D. Gibson, M. Henein.Department of Echocardiography, Royal Brompton Hospital and Imperial College, London, UK
Background: Restrictive left ventricular (LV) filling pattern (RFP) has poor prognosis. The prognostic value of LV filling at peak stress in ischaemic cardiomyopathy (ICM) is unknown. We aimed to assess the effect of dobutamine stress on LV filling pattern in ICM, possible mechanisms for change in filling pattern, and whether RFP persisting at peak stress affects prognosis.
Methods: 69 patients with ICM were studied. Early (E) and late (A) LV filling velocities were measured using pulsed-wave Doppler. RFP was defined as E: A ratio ⩾1.0, isovolumic relaxation time (IVRT) <80 ms, E deceleration time (EDT) <120 ms. LV inotropy (peak aortic acceleration-PAA), stroke volume (SV), peak mitral E acceleration (PMEA), and tricuspid regurgitation (TR) were measured at rest and peak stress.
Results: 27 out of 69 patients had non-RFP at rest and stress (AA), 24 out of 69 had RFP at rest and non-RFP at stress (EA) and 18 out of 69 had RFP at rest and stress (EE). There was no difference between EE and EA at rest but the stress response differed significantly. In EA, PAA, and SV increased (by 0.8 g and 6 ml respectively p<0.01), IVRT and EDT lengthened (by 43 ms and 46 ms p<0.01), and PMEA and TR decreased (by 0.3 g and 26 mmHg p<0.001) (1 g = 9.81 m/s2). The stress response in AA was similar to EA. In EE, PAA increased (by 0.2 g p<0.001), SV did not change, IVRT and EDT shortened (both by 21 ms, p<0.001), and PMEA and TR increased (by 0.4 g and 13 mmHg respectively p<0.01). Thus IVRT and EDT were shorter (by 64 ms and 62 ms), and PMEA and TR were greater (by 0.7 g and 39 mmHg) in EE than EA (all suggesting increasing left atrial pressure) while PAA was 75% lower (all p<0.001). Median follow-up (IQR) after stress was 34 (20–57) months. 3-year survival was 89% for AA, 78% for EA, and only 49% for EE (log-rank p<0.001). Compared with AA, the overall hazard ratio for EE was 9.5 (95% CI 4.3 to 14.7; p<0.001) and 1.9 for EA (95% CI −4.2 to +8.1; p = NS).
Conclusion: When restrictive filling persists during dobutamine stress in patients with ischaemic cardiomyopathy, left ventricular inotropic response is almost abolished and left atrial pressure rises strikingly. Furthermore survival is markedly reduced (hazard ratio 9.5). Stress echo thus provides major prognostic data, identifying high-risk patients who may benefit from early intervention.
060 CARDIAC DYSYNCHRONY AS MEASURED BY TOTAL ISOVOLUMIC TIME MAY PREDISPOSE TO CENTRAL SLEEP APNOEA IN CHRONIC HEART FAILURE
A. Vazir, P. C. Hastings, A. M. Duncan, H. M. McIntyre, M. J. Morrell, M. R. Cowie, P. A. Poole-Wilson, A. K. Simonds, M. Y. Henein.Cardiac Medicine and Sleep & Breathing unit. Royal Brompton Hospital, National Heart & Lung Institute, Imperial College, London, UK
Background: Central sleep apnoea/Cheyne-Stokes respiration (CSA) is common in patients with severe chronic heart failure (CHF), and is associated with significant morbidity. CSA is also associated with prolonged circulation time and enhanced chemosensitivity to carbon dioxide. A recent study has suggested that cardiac resynchronisation therapy with biventricular pacing can improve CSA. Total isovolumic time (t-IVT) is defined as the time when the left ventricle (LV) is neither ejecting nor filling, and reflects the degree of dysynchrony.
Aim: To determine the association between prolonged t-IVT and CSA in patients with CHF.
Method: 35 men, mean age of 60.1 (12.8) years, with stable CHF due to LV systolic dysfunction (EF < 45%) and not in atrial fibrillation were studied by polysomnography, cardiopulmonary exercise, and 2D Doppler-echocardiography. All were in NYHA Class II or III and on optimal medical therapy. None had evidence of valve or pulmonary disease (FEV1> 0.7). The aetiology of heart failure was coronary artery disease in 16 (46%). The t-IVT was measured as the number of seconds/min when the LV was neither ejecting or filling. CSA was defined as an apnoea-hypopnoea index (AHI) >15 events/hour of sleep with >50% of apnoeas central in origin.
Results: 18 patients (51%) had CSA. CSA patients were more symptomatic than those without CSA as assessed by the Minnesota living with heart failure score (43.1 (SD 17.6) v 29 (22.7); p = 0.05). They were also older (65.5 (9.2) years v 54.6 (13.7); p = 0.01). No differences were found for the proportion with coronary artery disease (44% v 47%; p = 0.98), LV ejection fraction (29.7 (10.9) % v 30.4 (9.2); p = 0.86), MVO2 and VE/VCO2 slope. The t-IVT was higher in CSA patients compared to those without CSA, (11.5 s/min (6.9-26.3) v 8.26 (2.4-23.7) p = 0.02). The t-IVT correlated with the percentage of sleep time spent in Cheyne-Stokes respiration (R = 0.62, p = 0.001).
Conclusion: The t-IVT is significantly prolonged in CHF patients with CSA, suggesting worse ventricular dysynchrony. The correlation between t-IVT and % of sleep time in Cheyne-Stokes respiration suggests that cardiac cycle inefficiency may predispose to destabilisation of the control of breathing, and subsequent CSA. Cardiac resynchronisation may improve CSA by improving cycle efficiency.
061 SUSPECTED HEART FAILURE IN PRIMARY CARE - THE UTILITY OF N-TERMINAL PRO B-TYPE NATRIURETIC PEPTIDE (NT PROBNP) AS A PRE-SCREENING TEST FOR SECONDARY CARE REFERRAL: A REAL LIFE STUDY
A. Fuat, J. J. Murphy, G. Brennan, A. A. Mehrzad, J. I. Johnston, W. S. A. Smellie.Darlington Pct, Darlington Memorial & Bishop Auckland Hospitals, University of Durham, Durham, UK
Introduction: Recent national guidelines recommend using BNP or NT proBNP in the diagnostic triage of patients with suspected heart failure. Patients then need referral for assessment of left ventricular function. Previous work has suggested that NT proBNP below 150 pg/ml demonstrates high negative predictive value for excluding heart failure due to left ventricular systolic dysfunction. This is the first study describing the use of NT proBNP by GPs in a real life clinical setting.
Study design: A prospective study using an observational, non-randomised clinical trial design.
Study aims: To determine the practicality and cost benefit of using NT proBNP as a pre-screening test, or filter, to secondary care referral in a pragmatic GP setting.
Subjects and setting: 600 consecutive primary care patients identified from practices in Darlington, the Dales and Sedgefield PCTs (total population 282,000) had a NT proBNP assay for suspected heart failure symptoms between August 2003 and June 2004. All 34 general practices participated. GPs were encouraged to refer all patients with a level over 150 pg/ml to one stop diagnostic clinics at Darlington or Bishop Auckland.
Results: The 600 patients had a median age of 77 years (range 35–95) and 368 (61%) were women. 396 (66%) of assays were above the limit of 150 pg/ml. In this group NT proBNP levels ranged from 157 to 33805 with a median of 711 pg/ml. 333 (84%) of these patients were referred to diagnostic clinics, of whom 84 (25%) had LVSD (14% of the total group). Of the 63 not seen in clinic, 18 had died, 2 had refused referral and 4 had not attended. Reasons for non-referral in the remainder were unclear. Of the 249 patients with raised NT proBNP but normal LV function, the majority had cardiovascular causes. Four patients were referred to clinics despite a normal NT proBNP, but none had LVSD. During the period of study, clinic waiting times increased from 2 to 8 weeks.
Conclusion: In a primary care setting, the majority of patients tested had raised NT proBNP. Of these, only 25% had LVSD although most had other cardiovascular problems. Introducing the service significantly increased waiting times. Raising the cut off to 300 pg/ml would have avoided a further 100 referrals and only missed 4 with mild and 1 moderate LVSD. The optimum cut off has yet to be resolved
062 AN ANALYSIS OF THE APPARENT FREQUENCY OF DIASTOLIC HEART FAILURE IN A SECONDARY CARE SETTING, USING DIFFERENT PUBLISHED DEFINITIONS
Martha R. Scott, Robin M. Egdell.Department of Cardiology, Macclesfield District General Hospital, Macclesfield, Cheshire, UK
A proportion of patients with symptoms and signs of heart failure have normal or preserved left ventricular systolic function on echocardiography. However, there is a lack of clarity over the degree of preservation of systolic function that should be used to distinguish the entity of diastolic heart failure from conventional heart failure. We have estimated the proportion of patients with a clinical diagnosis of heart failure who have diastolic heart failure, according to a variety of definitions used in previous published studies. All patients admitted to our institution or attending general cardiology or specialist heart failure clinics in 2002/3, with a diagnosis of heart failure made by a consultant cardiologist, were identified retrospectively and their echocardiograms reviewed. Patients with significant valvular disease or hypertrophic cardiomyopathy were excluded. Fractional shortening, ejection fraction by the modified Simpson’s method and wall motion index were recorded. Twelve different definitions of diastolic heart failure from published studies were then applied to the data to establish the proportion with this condition. 313 patients were identified with a clinical diagnosis of heart failure. Of these, 236 had recent echocardiographic studies available for review and were included in the study. The percentage with diastolic heart failure varied from 13.9% using a definition of ejection fraction >0.5 and no wall motion abnormality (Kitzman et al, 2002) to 71.2% using a definition of fractional shortening >0.17 (Kinney et al, 1989). Ejection fractions in the whole patient group were normally distributed with a mean of 0.49. Hence the percentage with diastolic heart failure was very sensitive to small differences in ejection fraction cut-off in this range: >0.4 = 67.6%, >0.45 = 59.0%, >0.5 = 46.2%, >0.55 = 35.2%.
Conclusion: The percentage of patients with heart failure identified as having diastolic heart failure varies widely according to the definition used. Considerable work needs to be done to define this group of patients more accurately. It may be premature to conduct therapeutic trials into this condition until it has been better differentiated from conventional heart failure.
063 THE REACT (RESCUE ANGIOPLASTY V CONSERVATIVE TREATMENT OR REPEAT THROMBOLYSIS) TRIAL: RESULTS ACCORDING TO ACTUAL TREATMENT RECEIVED
A. Gershlick, N. Uren, deA. Belder, J. Davis, M. Pitt, F. Alamgir, A. Banning, A. Baumbach, M. Shiu, P. Schofield, R. Henderson, S. Stevens, K. Abrahms, S. Hughes, R. Wilcox.Universtiy Hospitals of Leicester and others
Up to 40% of patients suffering acute myocardial infarction fail to achieve TIMI Grade 3 patency following thrombolysis. The UK REACT trial randomly compared rescue angioplasty (RPCI), repeat lysis (R-Lysis), or conservative therapy (C) in such patients It examined safety and clinical outcomes to one year in 427 patients recruited till March 2004 at 35 UK hospitals. Patients receiving standard treatment ((any) lysis and aspirin) within 6 hours of onset of pain, with <50% resolution ST changes at 90 minutes ECG were included. Primary endpoint is composite MACE (death/re-infarction/CVA/severe heart failure) at 6 months.
Demographics: Male 79.2%: mean age 61.1 (SD 11) years: 42.5% anterior MI at presentation, 14.1% diabetics, 37.5% hypertensive. Streptokinase was initial lytic in 60%. The median time from pain-first lytic was 140 mins (2.3 hours). Fibrin-specific R-lysis was administered median 330 mins (5.5 hours) after onset of pain, and RPCI 414 mins (6.9 hours) (time difference 84 mins (1.4 hours)).
Results: Intention to treat analysis: R-PCI improved outcome affecting all composites MACCE at 6 months; Event free survival rates: RPCI 84.6% v R-Lysis 68.7%; v Conservative 70.1% (p = 0.004). RPCI v Conservative HR = 0.47 (95% CI 0.28 to 0.79; p = 0.004) and v R-Lysis HR = 0.45 (95% CI 0.27 to 0.75; p = 0.002). However, we have now also analysed the data according to last treatment received within the 12 hours following randomisation to ensure that it was the R-PCI rather than the randomisation to that group that was advantageous. Results were further improved. Of 142 patients who actually received R-Lysis, 44 (31.0%) suffered at least one component of the composite end-point as did 46 (29.2%) of 154 who were treated actually conservatively compared to only 18 (13.7%) of 131 who actually received R-PCI within 2 hours of failed lysis. The HR for R-PCI v R-Lysis was 0.40 (CI 0.23 to 0.70) p = 0.00012: v C HR = 0.42 (CI 0.24 to 0.72) 0.0018)
Conclusion: Treatment with Rescue PCI improves outcome in patients with failed thrombolysis and should be standard treatment.
064 LOGISTICS AND ECONOMICS OF INTERHOSPITAL TRANSFER V DIRECT ADMISSION FOR PRIMARY ANGIOPLASTY
M. Dalby, M. Al-Obaidi, R. Smith, R. Grocott-Mason, S. Dubrey, L. Hutchison, M. Teoh, M. Al-Bustami, A. Mitchell, M. Mason, C. Ilsley.Harefield Hospital and Hilligdon Hospital, UK
Background: Transfer for Primary Percutaneous Intervention (PPCI) is superior to local thrombolysis in clinical trials. However, in routine ‘real world’ practice interhospital transfer introduces substantial delays, reducing the benefit of PPCI, using considerable resource and cost.
Method: We quantified the time, logistical and financial costs of interhospital transfer (IHT) versus direct admission for PPCI in a referral population of approximately 270,000 with a single district hospital (DGH) and specialist cardiac centre (SC) 6 miles apart with a ‘hub and spoke’ protocolised PPCI programme, aiming to move from IHT to direct admission.
Results: Between March and November 2004, 71 patients underwent PPCI at the SC. 11 presented directly to the DGH, underwent IHT to the SC and were excluded from the analysis. Eighteen were taken to the DGH by ambulance and underwent IHT to the SC. Forty-two were taken directly to the SC by ambulance. All data expressed as mean SD (range). The initial ambulance journey whether to the DGH or SC was similar in time: 19.8 (SD 6.5) mins (7–30) v 19.2 (4.1) (11–35) p = ns. The SC door to balloon time was 31 (11) mins (14–59) for direct admissions and 25 (7) (15–40) for IHT (p = 0.06). By time/resource/cost, the differences between the two strategies were: Time in the DGH; 52.7±20.8 mins (23–115) (Arrival to decision to transfer 25.6 mins, decision to transfer to ambulance departure 27.1 mins).
Resource in the DGH: resuscitation cubicle for one hour, specialist nurse, doctor. Cost in the DGH, £94. For the IHT, time in transit: 19.2 (4.1) mins (11–35).
Resource: Category ‘A’ ambulance with 2 crew and cardiac nurse, cost: £198). Overall, IHT delayed reperfusion by 71.9 mins (34–150) (minus the 6 minute door to balloon gain = 65.9 mins), utilised 5 extra staff, redeployed an ambulance (taking it out of service including restocking for 1–2 hours) and cost approximately £300.
Conclusion: In spite of having a local protocol for IHT for PPCI the delays were substantial. Direct admission for PPCI offers much earlier mechanical reperfusion, utilises significantly less resource and is cheaper than interhospital transfer. Systems should be put in place within cardiac networks to offer direct admission for patients with myocardial infarction to PPCI centres.
065 PRE HOSPITAL ECG DIAGNOSIS BY AMBULANCE CREWS REDUCES TIME TO REPERFUSION IN ST SEGMENT ELEVATION MYOCARDIAL INFARCTION (STEMI) PATIENTS TREATED WITH PRIMARY ANGIOPLASTY (PA)
E. J. Smith, A. K. Jain, S. K. Shukla, S. P. Ramdany, J. Cooper, P. Moss, A. Mathur, A. D. Timmis, K. Henderson, M. Whitbread, C. J. Knight, M. T. Rothman.Departments of Cardiology and Emergency Medicine, Barts and the London NHS Trust, and The London Ambulance Service, UK
Transfer of ST Segment Elevation Myocardial Infarction (STEMI) patients from district hospital emergency departments (ED) for primary angioplasty (PA) at a heart attack centre (HAC) has been proven safe and effective. However, the time to reperfusion may be prolonged. This study compared a ‘direct access’ strategy (DA) utilising pre hospital ECG diagnosis by ambulance crews, with ED transfer (EDT) for PA.
Methods: 72 consecutive suspected STEMI patients within a network of 3 hospitals were delivered to a HAC catheter lab without referral or ECG transmission (30 DA, 42 EDT). DA allowed bypass of the nearest ED if necessary. EDT included self presentations, and non DA ambulance patients. Reperfusion times were measured from symptom onset, call for specialist help, and first hospital arrival (pain, call, and door to balloon times; PTB, CTB, DTB). Peak creatine kinase (CK) was measured as a marker of infarct size.
Results: 62 out of 72 patients had confirmed STE. 94% (58/62) underwent immediate angiography; 79% (49/62) had STEMI (19 DA, 30 EDT), all undergoing successful PA. The figure shows that DA significantly reduced all reperfusion times. Peak CK was lower in the DA group, though not reaching significance (Median CK (IQR): DA 619 iu (337–1342) v EDT 758 iu (342–1758); p = 0.59).
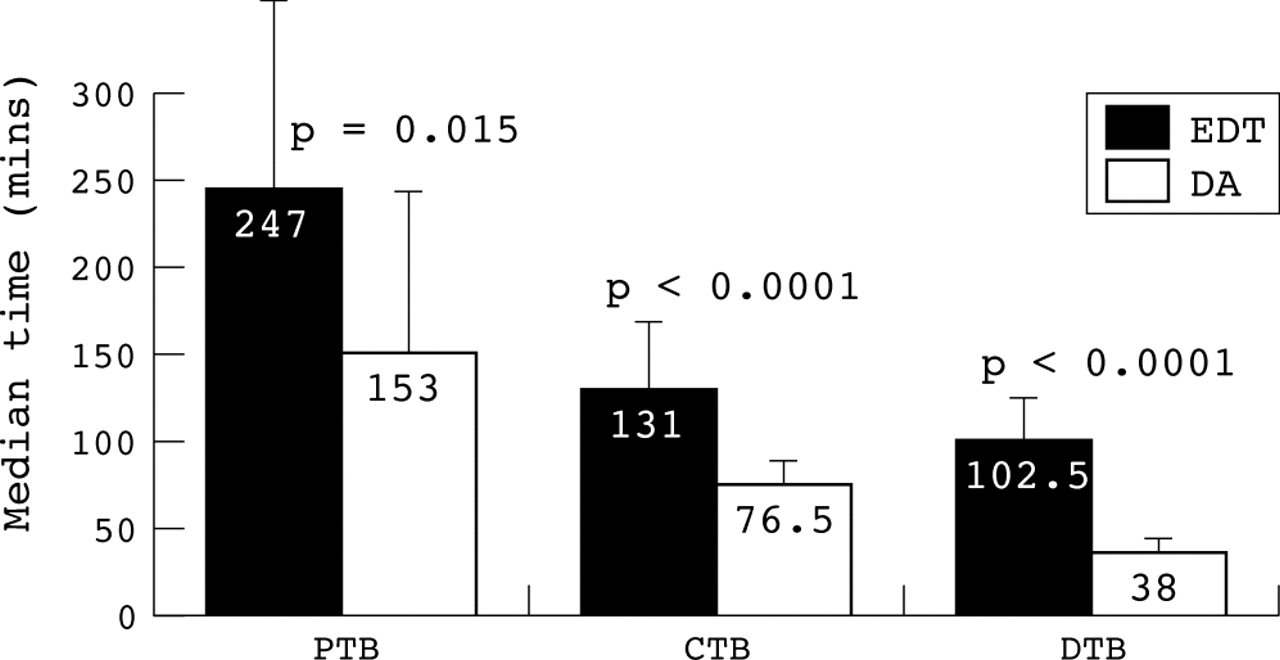
Abstract 65
Conclusion: Pre-hospital diagnosis with direct ambulance catheter lab access significantly reduces time to reperfusion. Collaboration of hospital networks with ambulance services is essential to ensure optimal reperfusion. This expertise should be utilised by centres wishing to adopt primary angioplasty as their preferred reperfusion strategy.
066 A PROSPECTIVE, RANDOMISED, CONTROLLED TRIAL TO STUDY THE EFFECT OF INTRA CORONARY INJECTION OF VERAPAMIL AND ADENOSINE ON CORONARY BLOOD FLOW DURING URGENT PERCUTANEOUS CORONARY INTERVENTION
K. Vijayalakshmi, B. Kunadian, R. Wright, J. Hall, A. Sutton, M. de Belder.Department of Cardiology, The James Cook University Hospital, Middlesbrough, UK
Background: Administration of medications such as verapamil and adenosine can increase blood flow through the coronary arteries through various mechanisms. But there are few comparative studies to determine their impact on coronary flow after angioplasty in acute coronary syndrome.
Aims: We studied the impact of the intracoronary use of these medications on coronary blood flow using the TIMI frame count method after percutaneous coronary intervention (PCI) following an acute coronary syndrome.
Methods: In total, 150 patients underwent urgent PCI of the culprit artery. The baseline characteristics were matched in all 3 groups. Following completion of the PCI procedure, patients were randomised to receive either verapamil−500 mcg (n = 49), adenosine−30 mcg (n = 51), or normal saline−10 mls (n = 50). TIMI frame count (TFC) was assessed pre PCI, post PCI and after the administration of the study medications.
Results: A total of 9 (18%) patients in the verapamil group developed transient heart block (p = <0.001). There was a significant improvement in the TFC between (a) the verapamil and the normal saline group, p = 0.02; and (b) the adenosine and the normal saline group, p = 0.002. However there was no significant improvement in the TFC between the verapamil and the adenosine group, p = 0.2 (table).
Abstract 66
Conclusion: Administration of verapamil and adenosine significantly improves coronary flow compared to the control group after PCI. However, there was no significant difference between the verapamil and the adenosine group. Verapamil was significantly associated with transient heart block compared to the adenosine and the control group.
067 OPTIMISING TARGET VESSEL REPERFUSION TIMES WITH PRIMARY PERCUTANEOUS INTERVENTION FOR ACUTE MYOCARDIAL INFARCTION
M. Al-Obaidi, M. Dalby, C. Schultz, A. Asherson, R. Smith, D. Davies, R. Grocott-Mason, A. Mitchell, M. Al-Bustami, M. Mason, C. Ilsley.Harefield Hospital and Hillingdon Hospital, UK
Backround: Mounting evidence suggests primary percutaneous intervention (PPCI) for acute myocardial infarction (AMI) is superior to thrombolysis in reperfusion success rate and in reducing morbidity and mortality. Inherent in getting this benefit, however, is the need to achieve rapid door to intervention times in routine practice.
Methods: Patients presenting with chest pain and ECG changes suggestive of AMI were received either directly via local ambulance service (LAS) or transferred from a district general hospital (DGH). We provided a 24/7 PPCI service aiming to achieve a short door to balloon time (DTB) by rapid transfer of patients directly from the ambulance to the catheter lab.
Results: PPCI was performed in 71 (48 males) patients (LAS = 42 (59%), DGH = 29 (41%)), Mean age SD was 64 (SD 14) (Range: 37–93). The average time from LAS call to arrival at our centre was 15 (8) minutes (min-max; 2–34 minutes) whilst the time taken from the patient arriving at the referring DGH to our centre was 1 hour and 11 minutes (min-max; 00:34–2:30 hh:min). The majority of patients 69/71 (97%) were directly transferred from the ambulance to the catheter laboratory whilst 2/71 (3%) required brief transfer to a designated holding bay. The average DTB time was 29 (1.0) minutes (min-max; 14–59 minutes), this was marginally longer in patients arriving via LAS compared to those arriving via the DGH (31 (1.1) v 26 (0.7) minutes, p = 0.06). DTB was however not influenced by time of arrival of patient at daytime (08:00 to 20:00) compared to night time (20:00 to 08:00), (27 (0.9) v 31 (1.0) minutes respectively, p = NS). TIMI III flow was achieved in 64 (90%) patients. There were three (4%) 30-day major adverse events recorded; two deaths (cardiogenic shock) and one Cerebrovascular event.
Conclusion: A programme for provision of rapid PPCI service is possible and safe allowing short door to target vessel reperfusion times comparable to the best published trial data.
068 FACTORS INFLUENCING LEFT VENTRICULAR FUNCTION FOLLOWING SUCCESSFUL RESCUE PERCUTANEOUS CORONARY INTERVENTION FOR FAILED THROMBOLYSIS IN ACUTE MYOCARDIAL INFARCTION
K. P. Balachandran, C. Berry, D. O’Halloran, B. D. Vallance, M. Malekianpour, T. J. Gilbert, A. C. H. Pell, K. G. Oldroyd.Bristol Royal Infirmary, Bristol, UK; Western Infirmary, Glasgow, UK; Lanarkshire NHS Trust, East Kilbride, UK
Background: 30–50% of patients do not achieve complete reperfusion following thrombolytic therapy for acute myocardial infarction and some centres in the United Kingdom offer ‘rescue’ percutaneous coronary intervention (PCI) as a salvage modality. The variables that contribute to changes in left ventricular function following rescue PCI have not been well established.
Objective: To study the influence of clinical and angiographic factors on global and regional left ventricular (LV) function following rescue PCI.
Methods: We performed repeat cardiac catheterisation in 102 patients who had undergone rescue PCI at our centre. 82 patients had suitable baseline and follow up ventriculograms, which were analysed offline by an automated edge detection technique. Pre and post PCI TIMI flow and post PCI TIMI myocardial perfusion grade (TMP) were assessed.
Results: Mean (standard deviation (SD)) follow-up period was 22 (15) months. Mean (SD) age was 59(12) years and 78% were male. The left anterior descending artery was the infarct related artery in 46 patients, left circumflex artery in 8 and the right coronary artery in 48. Improved global and regional LV systolic function (5 segment model) was observed in 55 (67%) patients—group I; and deterioration in 27 (33%)—group II. There were no differences in baseline clinical characteristics between the two groups. On univariate analysis baseline ejection fraction (p = 0.005) and coronary stenting (p = 0.05) were associated with improved LV systolic function. Pre-procedure TIMI flow, post-procedure TMP grade, pain to thrombolysis or PCI times and use of abciximab did not influence LV systolic function. On multivariate analysis, ejection fraction at the time of rescue PCI (OR (95% CI): 0.948 (0.913, 0.984); p = 0.006) and stenting (3.944 (1.182, 13.156); p = 0.026) were predictors of improved LV systolic function
Conclusion: Successful rescue PCI following failed thrombolysis in acute myocardial infarction was associated with improved left ventricular function at follow-up in the majority of patients. Stenting, but not glycoprotein IIbIIIa inhibitor therapy, was associated with improved left ventricular function in the area supplied by the infarct related artery.
069 SUCCESSFUL THROMBUS EXTRACTION WITH THE RESCUE THROMBUS MANAGEMENT SYSTEMTM DURING ACUTE PERCUTANEOUS CORONARY INTERVENTION (PCI): DOES NOT NECESSARILY RESTORE OPTIMAL MYOCARDIAL TISSUE PERFUSION
J. Hall, K. Vijayalakshmi, B. Kunadian, R. Wright, J. A, M. A. de Belder.Department of Cardiology, The James Cook University Hospital, Middlesbrough, UK
Thrombus extraction using thrombus removal devices may play a significant role during PCI and stenting.
Aim: We determined the effectiveness of the Rescue device in achieving optimal tissue perfusion during PCI.
Methods: 30 patients underwent PCI using the Rescue device following an acute coronary syndrome (18 (60%) ST elevation myocardial infarction and 12(40%) non ST elevation myocardial infarction).
Results: The mean age of study patients was 65.5 (SD 9.8) years, men 80%, diabetics 13%, hypertensive 37%. PCI using the Rescue device was performed in 5 (17%) left anterior descending arteries, 4 (13%) circumflex arteries, 12 (40%) right coronary arteries and 9 (30%) saphenous venous grafts. Glycoprotein IIb IIIa inhibitor was used in 21 (70%) patients. After PCI, slow-flow/no-flow occurred in 8 (27%) patients. TIMI Flow Grade 3 and Myocardial Blush Grade 3 occurred in 87% and 37% of patients respectively after PCI using the Rescue Device. There was a significant reduction in the thrombus score and TIMI frame count pre & post PCI (4±0 and 0.86±1.4, p = <0.0001 and 92.2±23.9 and 21.96±24, p = <0.0001 respectively). CK levels at 6 and 12 hours post PCI was 1548.9±2045 and 758±860. In-hospital death occurred in none of the patients (0%). One patient (4%) died at 30 day follow-up.
Conclusion: These data suggest that the use of the Rescue Thrombus Management systemTM may significantly improve the angiographic epicardial coronary blood flow. However, the small percentage of patients with MBG 3 post procedure indicates that this device alone may not result in maximal tissue perfusion in such patients.

Abstract 69
070 THE REACT (RESCUE ANGIOPLASTY V CONSERVATIVE TREATMENT OR REPEAT THROMBOLYSIS) TRIAL: IMPACT OF AGE UPON EFFICACY OF TREATMENT
A. Gershlick, S. Hughes, S. Stevens, N. Uren, deA. Belder, J. Davis, M. Pitt, F. Alamgir, A. Banning, A. Baumbach, K. Oldroyd, M. Shiu, E. Leatham, S. Redwood, K. Abrams, R. Wilcox.University Hospitals of Leicester and others
The REACT trial randomised 427 patients with failed thrombolysis (<50% resolution maximal ST segment elevation at 90 min ECG) to either Repeat Lysis, Conservative treatment (C), or Rescue Percutaneous Coronary Angioplasty (R-PCI). Event free survival @ 6 months was significantly better in the R-PCI group: R-PCI v Conservative HR = 0.47, 95% CI 0.28-0.79 (p = 0.004) and R-PCI v Repeat Lysis HR = 0.45, 95% CI 0.27-0.75 (p = 0.002). The survival rate of R-PCI was 84.6%, compared to 70.1% for Conservative treatment and 68.7% for Repeat Lysis (p = 0.004). Since previously there has been controversy surrounding newly introduced treatments and their efficacy-versus-risk benefit in the elderly (such as primary thrombolysis), this abstract examines the impact of age on treatment outcomes in the REACT trial. The mean age was 61.1 years (SD 11.0, range 34–85) and comparable between all treatment groups. As might be expected, for all patients increasing age had an adverse effect upon primary end point @ 6 months (HR = 1.05, 95% CI 1.03 to 1.07; p<0.0001)—the risk of a composite endpoint increases by 5% with every one year increase in age. For individual treatment groups the rates of composite end point increased with age. Thus for R-Lysis these were 11.9% (<60 years): 21.3% (60–70 years): 39.4% (70–80 years) and 66.7% (>80 years). For C the figures for the same age ranges were 18.3%; 19.2%; 40.9%, and 71.4% resp., and for R-PCI 4.8%; 12.2%;18.8%, and 25.0% resp. Treatment interactions with age were all found to be definitively non-significant, indicating that the benefit of R-PCI does not vary with age (R-PCI v Repeat Lysis p = 0.797, R-PCI v Conservative; p = 0.999) and that the impact of age is similar (statistically) for all three treatment groups.
Conclusion: These results suggest that following failed primary lysis, rescue PCI would be the preferred treatment, regardless of age.
071 TROPONIN T (TNT) AND CREATINE KINASE MB (CK-MB) RELEASE FOLLOWING PERCUTANEOUS CORONARY INTERVENTION (PCI): ARE THEY EQUIVALENT?
R. Moore, R. Lowe, J. L. Morris, W. L. Morrison, D. R. Ramsdale, R. A. Perry, R. Stables.The Cardiothoracic Center, Liverpool, UK
Background: Myocardial necrosis is a frequent occurrence after PCI and has been traditionally assessed by elevations in of CK-MB with large (>3 times the upper limit of normal) CK-MB releases established as a marker of poor prognosis. The adoption of troponin as the main clinical measure of cardiac enzyme release and standardisation of laboratory testing has predictably led to the replacement of CK-MB assays with troponin including following PCI. However, the relationship between CKMB and TnT in the PCI setting has not been established.
Methods: TnT and CK-MB levels were measured following revascularisation in a consecutive series of patients undergoing elective PCI between 1/4/2003 and 1/5/2004 at The Cardiothoracic Center, Liverpool.
Results: Data was available for analysis on 933 patients. The cohort consisted of 680 (73%) men of mean age 61.4 (SD 9.8). Procedures were covered with Clopidogrel preloading in 88% of cases and GPIIb/IIIa inhibitors in 59%. 29% of patients underwent multi-vessel angioplasty, 50% multi-lesion angioplasty and procedural complications occurred in 3.8% of interventions. In this cohort post procedural CK-MB levels were significantly correlated to TnT levels (R = 0.747, p>0.001). A CK-MB level of above three times normal was predicted with 95% sensitivity (48% specificity) at a TnT level of 0.11. High TnT levels with low corresponding CK-MB limited specificity irrespective of the TnT threshold used. The sole factor associated with >3 times TnT release without a concomitant >3 times CK-MB rise was the absence of procedural complications OR 0.26 (95% CI 0.09-0.73), p = 0.011.
Conclusion: TnT is a sensitive but not specific guide to CK-MB release following PCI. Elevated CK-MB titers are a more specific marker of procedural complications.
072 HOW LONG DO PATIENTS WAIT WITH ACUTE CORONARY SYNDROMES FOR INTER-HOSPITAL TRANSFER IN THE UK? RESULTS FROM THE CORONARY HEART DISEASE COLLABORATIVE NATIONAL AUDIT 2004
ABakhai, BClark, SMachin, SHall, MDancy, RLevy, RBoyle, R. G. Murray.For the Coronary Heart Disease Collaborative Group
Background: The majority of UK district general hospitals do not have facilities for coronary interventions. Patients admitted with acute coronary syndromes (ACS) may incur delay before they can be transferred to a centre with appropriate facilities.
Methods: 193 hospitals from 140 trusts submitted data to the CHD group on patients pending or undergoing inter-hospital transfer (IHT) during the month of March 2004 as part of a national survey. Reasons for transfer, age, gender, and various dates were collected to ascertain duration of stay prior to transfer.
Results: Hospital Transfer from DGH (n) 2514; mean age 64 (SD 12); male gender 71%, emergency surgery 1%, very urgent surgery 11%; PCI with prior angio 5%, Angio +/− PCI 83%; mean time to referral (median) 4 (3) days; mean time to transfer (median) 12 (9) days; mean time to procedure (median) 12 (9) days; mean time to CABG (median) 20 (14) days.
Conclusion: Patients requiring IHT from district general hospitals incur substantial delays prior to being referred for transfer and thereafter awaiting transfer. In particular there are prolonged delays for patients being transferred for CABG. Substantial resources are being spent incurring these delays. More detailed data with geographical variations are also available for presentation.
073 RAPID REDUCTION OF INTER HOSPITAL ACUTE CORONARY SYNDROME (ACS) TRANSFER WAITING TIMES; THE ROLE OF A REGIONAL TRANSFER UNIT (RTU)
R. Hitchcock, M. Watkins, N. G. Bellenger, C. Duffet, D. Jewell, D. Palliser, L. Shapland, P. Thirwel, S. Scrase, R. Burns, N. Curzen.Wessex Cardiothoracic Centre, Southampton General Hospital, Southampton, UK
Background: ACS patients are at high risk of death and non-fatal MI, and cardiovascular events (12% and 30% respectively from PRAISE UK). These patients benefit from early (72 hours) investigation and revascularization (FRISC-II and TACTICS-TIMI 18). International guidelines recommend referral for inpatient coronary angiography with a view to revascularisation, but median national waiting times are 15 days (21 locally). Furthermore, patients in non-revascularization DGHs experience a longer wait than those admitted to revascularization centres directly. Locally up to 60 patients were waiting for transfer equating to approx 21000 bed days or a cost of £4 m per annum.
Method: A dedicated 6 bedded RTU for the exclusive treatment of ACS patients transferred from a referral centre was established within an existing cardiac ward. Simultaneously, a referral proforma was devised and its use agreed by all referral centres. It was designed to ensure patients were fully prepared for the procedure on the day of transfer. Four dedicated catheter laboratory slots for angiography with a view to proceeding to PCI were reserved per day (representing 40% of ACS on call slots). An operational policy was developed that integrated medical, nursing, management, pathology departments and the local ambulance services. A strict 24 hour discharge policy was implemented, either home, back to the DGH, or step down to a general ward.
Results: 141 patients were admitted in the first 2 months (6/12 data will be available for the meeting). Referral to transfer time was reduced from 23 to 5.5 (SD 5) days (range 1–11). 96% of patients were treated within 24 hours of admission (average length of stay has reduced from 6–2 days). 56% had stents, 17% medical treatment, 8% referred for surgery, 6% were normal. 80% of patients were discharged home the day after procedure, 4% returned to their DGH, 16% stepped down for further management.
Conclusion: The implementation of a RTU has rapidly reduced inter hospital transfer waiting times. Access for patients from non-revascularization centres is now equitable and conforms more closely to the evidence base. The shorter length of stay also ensures maximum use of resources. This model involved no additional beds, staff or resources.
074 A RETROSPECTIVE ANALYSIS OF 1500 PATIENTS UNDERGOING PCI FOR UNSTABLE ANGINA—TROPONIN STATUS AT PRESENTATION DOES NOT PREDICT 1 YEAR OUTCOME
A. Sirker, G. Dixon, S. Holmberg, D. Hildick-Smith, A. de Belder.Dept of Cardiology, Brighton and Sussex University Hospital, Eastern Road, Brighton, UK
Background: Troponin measurements have identified a high-risk sub-group among patients presenting with unstable angina.
Objectives: To examine 30 day and 1 year outcomes in ACS patients undergoing PCI and compare Troponin positive and Troponin negative groups.
Methods: Prospective data is collected on all PCI patients at our institution (PATS database, Dendrite Systems). 1 year data was collected—mortality tracking was performed using NHS patient information systems. All remaining patients received a postal questionnaire. Troponin T positivity was defined as >0.03 ng/ml (ECLIA assay) prior to PCI. 30 day MACE was defined as death, Q wave MI or emergency CABG; 1 year MACE involved death, Q wave infarct, or revascularisation. Groups were compared by Chi-Squared test—p<0.05 was considered significant.
Results: Two groups were created based on Troponin positivity (Trop pos, n = 887; Trop neg, n = 613). They were well matched for age, gender, risk factor profile, baseline LV function, target vessel and type of stent used. The results are shown in Table 1.
Abstract 74
Conclusion: In patients undergoing PCI for unstable angina syndromes, troponin status at presentation does not predict 1 year mortality nor MACE.
075 IMPACT OF SECONDARY PREVENTION MEDICATION ON 30 DAY MORTALITY FOR PATIENTS ADMITTED TO ENGLISH AND WELSH HOSPITALS WITH ACUTE CORONARY SYNDROMES
J. Birkhead, C. Weston, A-MBunn on behalf of the MINAP Steering Group.Clinical Effectiveness and Evaluation unit. Royal College of Physicians London, London, UK
Introduction: Data from the national audit of myocardial infarction project (MINAP) from admisssions in 2002–3 were used to examine the impact on early (30 day) mortality of the use of secondary prevention treatment with aspirin (ASA), statins (ST), beta blockers (BB) and enzyme converting antagonists (ACEI), prescribed at or before discharge from hospital, on patients who survived to leave hospital after an acute ischaemic coronary syndrome (ACS). Mortality at 30 days was compared between those who received all four agents, and those who did not for any reason not receive either ASA, ST, BB, or ACEI.
Methods: Records of 92096 patients admitted with ACS were examined. Of these 41109 has a final diagnosis (provided by the admitting hospital) of ST elevation infarction, 33327 had non ST infarction, and 17660 had a diagnosis of acute coronary syndrome.
Findings: Overall, 60.5% were prescribed all four drugs, and 84.2% were prescribed ASA, BB, and ST at discharge. Use of BB (range 80.4%-84.6%), ST (95%-96.9%), and ASA (97.5%-98.4%) differed little between diagnostic groups, while ACEI were prescribed to 89.6% of STEMI, 83.4% of non STEMI, and 73.3% of those recorded as having an acute coronary syndrome. Of those who survived to leave hospital the all cause 30 day mortality was; all drugs 1.4% (95% CI 1.3 to 1.5), no β Blocker 2.5% (2.3 to 2.8), no Statin 3.2% (2.5 to 3.8), no ACEI 1.4% (1.2 to 1.7), and no ASA 2.1% (1.3 to 3.0). Using logistic regression analysis mortality was adjusted for ageband (20–54, 55–64, 65–74, >74 years), gender, previous infarction, previous angina, hypertension, diabetes, hyperlipidaemia, and troponin level by quartile. The adjusted odds ratio of death by 30 days was (all drugs = 1); no β Blocker 1.68 (95% CI 1.37 to 2.0, p<0.001), no Statin 1.90 (1.38 to 2.60, p<0.001), no ACEI 1.31 (1.02 to 1.68, p = 0.034), and no aspirin 1.57 (0.98 to 2.66, p = 0.59).
Conclusion: The majority of patients who survive to leave hospital in England and Wales receive intensive secondary prevention medication with three or four evidence based drugs. The use of secondary prevention medication, particularly beta blockers and statins, results in substantial early (30 day) mortality benefit for this broad group of patients with acute coronary syndromes.
076 IS IT SAFE TO DISCHARGE PATIENTS FROM ACCIDENT AND EMERGENCY USING A RAPID POINT OF CARE TRIPLE CARDIAC MARKER TEST TO RULE OUT ACUTE CORONARY SYNDROME IN PATIENTS PRESENTING WITH CHEST PAIN?
S. Rathore1, P. Knowles2, A. P. S. Mann1, P. A. Dodds1.1Department of cardiology; 2Accident and Emergency department Leighton Hospital, Crewe, Cheshire, UK
Purpose: To determine whether patients presenting with chest pain who are at low to intermediate risk for ACS can safely be discharged from A&E using Triple Cardiac Marker (TCM “CK-MB, Myoglobin, TroponinI”) without increasing risk and cost effective use of coronary care facilities.
Methods: Retrospective review of patients presenting to A&E from Dec 2003 to July 2004 was performed with 6 months follow up for future coronary events and hospital admissions. A total of 325 patients presented to A&E with chest pain who were at low to intermediate risk of ACS. Paired TCM and ECGs were performed 2 hours apart and the results were used to determine whether hospital admission was required. Follow up data was collected from hospital records, hospital database, GPs and patient interviews.
Results: 235 consecutive patients (225 men, 100 women; aged 18–97 years, median 68 years) were included in the study. Paired TCM was negative in 100 patients (30%) and they were discharged from A&E. The re-admission rate for this group of patients was 1% with ACS and no deaths at 6 months.36 patients (11%) had single TCM negative and were sent home with 3% readmission rate with ACS and no mortality at 6 months. Subgroup analysis of 43 patients who had paired TCM and subsequent Troponin I at 12 hours is shown in table.
Abstract 76
Conclusion: Almost one third patients who presented with chest pain and low to intermediate probability of ACS were discharged from A&E following paired negative TCM. Six month readmission with ACS in this group of patients was only 1% with no deaths. Therefore paired TCM can be used to safely discharge this group of patients. This marker has the potential to significantly reduce hospital admissions.
077 IMPACT OF CHANGE OF PROTOCOL FOR THE MANAGEMENT OF PATIENTS WITH ST ELEVATION MYOCARDIAL INFARCTION: AN 18 MONTH UK TERTIARY CARDIAC CENTRE EXPERIENCE
B. Kunadian, K. Vijayalakshmi, A. Turley, J. A. Hall, R. A. Wright, A. Sutton, M. A. de Belder.Department of Cardiology, The James Cook University Hospital, Middlesbrough, UK
Background: Primary angioplasty compared to conventional thrombolytic therapy is associated with a significant increase in TIMI 3 flow and reduction in mortality in patients with ST elevation myocardial infarction (STEMI). In many centres in the UK thrombolytic therapy remains the first line treatment for STEMI. Over the last 18 months, we have followed 3 different protocols for the management of STEMI in our institution leading to a 24-hour primary PCI service.
Aim: To evaluate the hospital outcome of STEMI patients who are eligible for reperfusion therapy over an 18 month period following 3 different protocols.
Methods: Between February 2003 and July2003 (Group 1), PCI was offered to patients with contraindications to thrombolysis, failure to reperfuse, cardiogenic shock, and reinfarction. Between August 2003 to January 2004 (Group 2, “Czech protocol”), PCI was offered to patients presenting >3 hours from symptom onset. Between April 2004 and September 2004 (Group 3), primary PCI service was standard treatment to all patients who presented with STEMI. A retrospective analysis of clinical and angiographic data was performed.
Results: The total study population consisted of 215 patients who were eligible for reperfusion therapy. Baseline demographics were similar during all 3 periods. Group 1: mean age 66 years (29–97 years), 75% male; Group 2: mean age 65 years (43–90 years), 72% male; Group 3; mean age 60 years (32–85 years), 75% male. Primary PCI activity increased from 5% (Group 1) to 31% (Group 2) to 97% (Group 3) with a corresponding decrease in thrombolysis activity from 80% (Group 1) to 60% (Group 2) to 2% (Group 3) respectively. Overall in-hospital mortality decreased from 13% to 0% to 2%, (p = <0.01) over this time period. There was a reduction in the incidence of rescue PCI from 3% to 0%, p = 0.1 and re-infarction PCI from 11% to 9% to 0%, (p = <0.01).
Conclusion: The introduction of a primary PCI programme has been associated with dramatic reduction in in-hospital mortality more than expected. For centers not able to provide a comprehensive primary PCI programme, the “Czech protocol” appears to offer a significant reduction in in-hospital mortality as compared to a “Thrombolysis for all” protocol.
078 THE RELATIONSHIP BETWEEN TROPONIN LEVELS AND 90 DAY MORTALITY FOR PATIENTS WITH ST SEGMENT INFARCTION; A PARADOX
J. Birkhead, C. Weston, and L. Walker for the national audit of myocardial infarction project (MINAP) Steering Group.Clinical Effectiveness and Evaluation unit. Royal College of Physicians London, London, UK
Background: In acute non ST elevation coronary syndromes there is a direct relationship between increasing troponin levels and subsequent ischaemic events and death. We questioned whether troponin release following ST segment elevation infarction (STEMI) carried similar prognostic information.
Methods: We examined outcome for 23706 patients with STEMI admitted to English and Welsh hospitals for whom a troponin value by any assay method was recorded, and for whom outcome to 90 days was known. Recorded troponin values were split into quartiles using a maximum value of 200 ng.ml. The quartile (Q) ranges were; 0.001–1.27, 1.271–4.9, 4.91–19.3, and 19.31–200 ng.ml.
Findings: Patients in each quartile were of similar age (range 69-71), but there were more females within the lower quartiles; Q1 38.3%, Q2 34.3, Q3 32.3, Q4 31.4%. Patients in the lowest quartile received the least reperfusion treatment; Q1 54.7%, Q2 66.3%, Q3 74.7%, Q4 79.4%. The all cause 90 day mortality was highest in the quartile with the lowest troponin release; Q1 972/5982, 16.2%, Q2 894/5872, 15.2%, Q3 835/5998, 13.9%, Q4 814/5854, 13.9%, while the mean interval to death (up to 90 days) was longest in the lowest troponin quartile; Q1 25, Q2 21, Q3 20, Q4 18 days.
Interpretation: Patients with STE MI and low troponin release may have temporary occlusion of a major epicardial artery, with transient or small cardiographic ST elevations. We speculate that the low utilisation of thrombolytic treatment results from this, and may influence outcome. The higher late mortality of those within the lowest troponin quartile reflects continuing plaque instability in an open epicardial artery.
Conclusion: Patients with STEMI have a risk of death by 90 days, which is inversely related to the level of troponin release. Those within the lower troponin quartiles receive the least reperfusion treatment, whilst having the highest mortality rate and the longest mean interval to death. These findings are relevent in determining the correct management strategy for patients with STE MI.
079 UK PRIMARY ANGIOPLASTY COST EFFECTIVENESS STUDY (UK-PACES) 30 DAY OUTCOME DATA
K. P. Morgan, M. Leahy, C. Sheehy, P. Eardley, C. Shotter, K. J. Beatt.Department of Cardiology, Hammersmith Campus, National Heart and Lung Institute, Imperial College London W12 0NN, UK
Primary angioplasty (PPCI) has been shown to be a superior treatment to thrombolysis for the treatment of ST segment elevation myocardial infarction (STEMI). However, thrombolysis remains the standard treatment for STEMI in the UK because of perceived logistic and cost issues. The aim of this study is to provide definitive cost analysis data comparing PPCI to thrombolysis for the treatment of STEMI within the framework of the NHS. The West London PPCI Service commenced in October 2003. PPCI is undertaken in an interventional centre with the participation of 2 non interventional centres resulting in an average of 1 patient being referred daily. Detailed health economic data has been gathered retrospectively on consecutive patients thrombolysed across the 3 sites prior to the inception of the primary angioplasty service and prospectively on all patients undergoing primary angioplasty. 30 day outcome data is now available on 150 patients in each arm. Baseline characteristics between the groups were similar. There was a fivefold reduction in 30 day mortality (15% v 3%) combined with significant reduction in median hospital stay (9 days v 4 days) in favour of PPCI. Of patients thrombolysed 87% required cardiac catheterisation as an in patient with 58% going on to have percutaneous coronary intervention and 16% undergoing bypass surgery. The initial results of this study confirm the mortality benefit seen in randomised controlled trials in favour of PPCI. Previous studies have demonstrated the importance of hospital stay as the prime predictor of cost. Given the substantial reduction in hospital stay seen in the PPCI group and the high rates of in patient intervention seen in the thrombolysis group, preliminary costing data indicates a significant in-hospital cost reduction in favour of PPCI.
Conclusion: This is the first and largest cost analysis study of primary angioplasty in the UK. Initial results already show significant improvements in outcome with a reduction in costs in favour of PPCI. A full costing and 6 month outcome data will follow and be available for presentation.
080 IMPACT OF A 24-HOUR PRIMARY PCI SERVICE FOR ST ELEVATION MYOCARDIAL INFARCTION (STEMI) ON CONSULTANTS’ WORK PATTERNS
B. Kunadian, K. Vijayalakshmi, A. Turley, J. A. Hall, R. A. Wright, A. Sutton, M. A. de Belder.The James Cook University Hospital, Middlesbrough, UK
Thrombolysis remains the predominant reperfusion strategy for STEMI in the UK. Direct PCI has emerged as an effective reperfusion strategy compared to thrombolysis. Many hospitals in the UK are currently setting up Primary PCI services.
Aim: To assess the impact of a 24-hour primary PCI service for STEMI on consultant’s work patterns.
Methods: Between February 2003 and July 2003 (P1), PCI was offered to patients with contraindications to thrombolysis, failure to reperfuse, cardiogenic shock, and reinfarction. Between April 2004 and September 2004 (P2), primary PCI was offered to all patients who presented with STEMI. Four interventionists carried out the procedures. We compared the consultants’ work pattern for these two periods.
Results: The study population consisted of 169 patients (P1: n = 68, P2: n = 101) undergoing PCI for STEMI. The number of PCI performed after hours (1800–0800 hours and week-end (b)) increased from 56% to 63%. There was a reduction in in-hospital mortality 9% to 4%, rescue PCI 26% to 4%, p = <0.01, and re-infarction PCI 50% to 28% (table). Number of PCIs for STEMI performed during office hours (a) decreased from 44% to 37%, with reduction in hospital mortality from 3%–0%. There was a reduction in the duration of hospital stay 6.6 days to 5.6 days.
Abstract 80
Conclusion: The increased workload with the development of primary PCI programme tends to increase out off hours work, 69% mainly done before midnight. Consultant’s job plans must be developed to refer to this change in work pattern.
081 NOX-2 (GP91PHOX) DISRUPTION PREVENTS ENDOTHELIAL ISCHAEMIA-REPERFUSION INJURY IN HUMANS
S. P. Loukogeorgakis1, 3, J. M. van den Berg2, E. de Groot3, T. W. Kuijpers2, R. J. MacAllister4, J. E. Deanfield1.1Vascular Physiology Unit, ICH, UK; 2Paediatric Immunology; 3Vascular Medicine, AMC, Netherlands; 4Clinical Pharmacology, UCL, UK
Hypoxic cell death follows interruption of the blood supply to tissues. Although successful restoration of blood flow is mandatory for salvage of ischaemic tissues, reperfusion can place tissues at risk of further injury. Generation of reactive oxygen species (ROS) has been implicated in the pathophysiology of ischaemia-reperfusion (IR) injury. Recent studies suggest that a neutrophil-type NADPH oxidase may be a source of ROS during IR in endothelial cells. This multi-component enzyme includes the membrane-bound cytochrome b558 (gp91phox/Nox-2 and p22phox), and several cytoplasmic proteins to form an active oxidase. Using an in vivo model of endothelial IR injury in the forearm, we compared the endothelial response to IR in healthy controls with patients with X-linked Chronic Granulomatous Disease (CGD). These patients have a molecular lesion in the Nox-2 (gp91phox) subunit of NADPH oxidase that renders the enzyme inactive. Vascular ultrasound was used to assess endothelial function in a group of patients with X-linked CGD by measuring dilatation of the brachial artery in response to increased blood flow during reactive hyperaemia (flow-mediated dilatation; FMD). Endothelial IR injury was induced by 20 min of upper limb ischaemia (inflation of a blood pressure cuff to 200 mm Hg) followed by reperfusion. FMD was determined before IR and after 20 min of reperfusion. Comparisons were made in a group of age- and sex-matched controls. FMD (percentage change from baseline diameter) was expressed as mean SEM and compared statistically by ANOVA. There was no significant difference in pre-IR FMD between the two groups. IR caused a significant reduction in FMD after 20 min of reperfusion in controls (8.0 (0.7)% pre- v 2.9 (0.5)% post-IR, n = 13, p<0.001). IR-induced reduction in FMD was not observed in CGD patients (9.1 (1.1)% pre- v 7.7 (0.8)% post-IR, n = 13, p = NS).
Conclusion: These data indicate, for the first time in humans in vivo, that disruption of the Nox-2 (gp91phox) subunit of NADPH oxidase prevents endothelial IR injury. This is consistent with a role for endogenous ROS as a determinant of endothelial function after IR injury in humans. These findings have implications for the design of strategies to limit clinical IR injury.
082 INCREASED NUMBERS OF CIRCULATING ENDOTHELIAL CELLS PREDICT ADVERSE CARDIOVASCULAR EVENTS FOLLOWING AN ACUTE CORONARY SYNDROME
A. D. Blann, K. Lee, G. Y. H. Lip.Haemostasis Thrombosis and Vascular Biology Unit, University Department of Medicine, City Hospital, Birmingham UK
Background: Markers of endothelial perturbation (e.g. von Willebrand factor (vWf) and circulating endothelial cells (CECs)) are altered in acute coronary syndromes (ACS). Raised vWf predicts major cardiovascular endpoints (MACE) but it is unclear whether or not raised numbers of CECs are also predictive, or are superior to vWf. We hypothesised that CECs and vWf levels during the first 48 hours of ACS would predict MACEs at 30 day and 1 year.
Methods: 156 patients with ACS were included. Blood was drawn on admission (baseline) and 48 hours later for plasma vWf (ELISA) and CECs (CD146 immunomagnetic separation).
Results: At 30 days, 48 patients had ¡Ý1 MACE, predicted by baseline and 48 hr CECs, 48 hr vWf levels, and by the ¡®admission̈C48 hr change¡¯ in CECs and vWf (all p ¡Ü0.002). On multivariate analysis, 48 hr CECs (p<0.001) were the strongest predictor of MACE, followed by change in vWf (p = 0.048); 48 hr CECs were the only predictor of death (p = 0.007). At 1 year, 65 patients had ¡Ý1 MACE, predicted by 48 hr CECs (p<0.001). Age (p = 0.046) and 48 hr CECs (p<0.001) were the only predictors of death. CECs>6 cells/mL (median of the entire group) on admission correctly identified 97.5% of 30 day MACEs, 90% of 1 year MACEs, 100% of 30 day deaths and 93.3% of 1 year deaths
Conclusion: Admission, 48 hour, and the acute rise in vWf and CECs all generally predicted adverse outcome. However, admission CECs were the best overall predictors of MACE and death at 30 d and after a year, indicating the crucial role of endothelial/vascular damage in ACS pathophysiology.
083 INSULIN RESISTANCE IS A SUBSTRATE FOR ACCELERATED ENDOTHELIAL DYSFUNCTION IN MIDDLE AGE—STUDIES IN MICE HETEROZYGOUS FOR KNOCKOUT OF THE INSULIN RECEPTOR GENE (IRKO)
E. R. Duncan, S. B. Wheatcroft, J. M. Li, A. M. Shah, M. T. Kearney.Cardiovascular Division, Kings College London, London, UK
Ageing and insulin resistance are associated with the development of coronary atherosclerosis, a hallmark of which is endothelial dysfunction. We sought to explore the effect of mild insulin resistance on endothelial function in young (2 months) and middle aged (6 months) IRKO and their wildtype littermates (WT). We studied metabolic function and blood pressure in vivo, and vascular function in aortic rings ex vivo in IRKO & WT of both ages (n = 6-8 per group). Data presented as mean SEM, p<0.05 taken as significant. Fasting glucose was similar in young & middle aged IRKO (8.4 (SE 0.4) v 7.8 (0.4) & WT (9.1 (0.6) v 8.2 (0.5)), whereas the increment in response to a glucose challenge (1 mg/g i/p) was significantly greater in IRKO aged 6 months than in WT (123 (16)% v 68 (15)%). Systolic blood pressure measured by tail cuff plethysmography was significantly greater in IRKO. With ageing IRKO showed significantly augmented contraction to phenylepherine (Pe) and impaired acetylcholine (Ach) mediated relaxation. IRKO Ach responses were partially normalised by the SOD mimetic MnTMPy (10 μm/l; Emax pre 77.6 (6); post 91 (2); p = 0.03). WT vascular responses were unchanged between 2 and 6 months. See table.
Abstract 83
Conclusion: Our data demonstrates that mild insulin resistance leads to accelerated decline in endothelial function with ageing. It also supports a role for reactive oxygen species in this process. This work was supported by the British Heart Foundation.
084 ALTERED CORONARY MICROVASCULAR FUNCTION AND PERIPHERAL ENDOTHELIAL DYSFUNCTION IN YOUNG PATIENTS WITH SYSTEMIC LUPUS ERYTHEMATOSUS
C. C. Lang, K. Hirata, K. Amudha, M. Kinjo, K. Sugioka, R. Otsuka, J. Yoshikawa, S. Homma, A. M. Choy.Ninewells Hospital and Medical School, Dundee, UK; Osaka City University Medical School, Japan and Columbia University, USA
Background: Accelerated atherosclerosis is an important cause of mortality and morbidity in patients with systemic lupus erythematosus (SLE). Altered coronary microvascular function and peripheral endothelial function may act as markers for changes predisposing to the development of significant coronary vascular disease. The purpose of this study was to compare coronary flow reserve (CFR) and peripheral brachial endothelial function, in a group of pre-menopausal women with SLE (n = 19, mean (SD) age, 29.4 (SD 5.9) years) with an age- and race-matched group of healthy controls (n = 19, 28.2 (4.3) years).
Methods: CFR was assessed by transthoracic Doppler echocardiography and calculated as the ratio of hyperaemic, which was induced by intravenous adenosine tri-phosphate administration, to baseline coronary flow velocity of the left anterior descending artery. Flow-mediated endothelium dependent dilation (FMD) and glyceryl trinitrate (GTN)-induced endothelium independent dilation of brachial artery were assessed by high-resolution vascular ultrasound and calculated as the ratio of hyperaemic to baseline diameter of brachial artery.
Results: The SLE Disease Activity Index in these patients ranged from 4 to 21. CFR and FMD were significantly lower in patients with SLE, as compared to controls (CFR; 3.4 (SD 0.8) v 4.5 (0.5), p<0.0001 and FMD; 3.3 (5.7)% v 13.1 (3.9)%, p = 0.0002, respectively). However, there was no significant difference in endothelium-independent vasodilation between the two groups.
Conclusion: These findings provide direct evidence that both coronary and peripheral endothelial function are impaired in patients with SLE and that this may represent an early atherosclerotic process in these patients.
085 NITRIC OXIDE IS NOT REQUIRED FOR VASCULOGENESIS OR ANGIOGENESIS IN ZEBRAFISH EMBRYOS
T. J. A. Chico, C. Gray, P. G. Hellewell, P. W. Ingham, D. C. Crossman.Cardiovascular Research Unit & the Centre for Developmental Genetics, University of Sheffield, Sheffield, UK
Introduction: The zebrafish embryo has emerged as a novel model of vertebrate vascular development. Its external development allows manipulation and observation from immediately after fertilisation, and its transparency allows serial in vivo vascular imaging unrivalled in other model systems, despite its small size (≈2 mm). Its rapid development (achieving circulation in 24 hours) allows efficient screening of angiogenesis inhibitors. We studied the effects of nitric oxide (NO) synthase inhibition on vasculogenesis (precirculatory migration of angioblasts) and angiogenesis (sprouting of ECs from the primitive circulation), as NO has been shown to modulate angiogenesis in non-embryonic angiogenesis.
Methods: Embryos were obtained at the 1–4 cell stage and incubated in varying doses of the NO synthase inhibitor L-NAME. The effect of L-NAME on nitrite levels in embryo medium was assessed using the Griess reaction. Heart rate was measured by direct cardiac observation. Vasculogenesis and angiogenesis were assessed using transgenic Fli1-GFP fish (expressing endothelial GFP). The developing vasculature was visualised by fluorescence microscopy. Successful vasculogenesis was defined as formation of the dorsal aorta and cardinal vein by 24 hour post fertilisation (hpf). Subsequent angiogenesis was assessed by length and number of intersomitic vessels sprouting from the dorsal aorta at 36 and 48 hpf. Data represents mean SEM. Statistical analysis was by ANOVA.
Results: L-NAME (0.0625–6.6 mM) induced a concentration dependent reduction in nitrite levels, reaching 97% reduction at 1mM, indicating significant NO synthase inhibition. At 72 hpf, concentrations of L-NAME 0.25mM and higher significantly reduced heart rate (control 139 (SE 2)bpm, 0.25mM L-NAME 120 (2)). Developing embryos incubated in L-NAME (1–9.9mM) from 0.5hpf showed no defect in vasculogenesis by 24 hpf or in angiogenesis at 36 or 48 hpf.
Conclusion: We conclude that despite the proven role of NO in angiogenesis in other settings we found no effect of NO synthase inhibition on vasculogenesis or angiogenesis in developing zebrafish. This lack of effect was seen despite a reduction in both nitrite levels and heart rate (hallmarks of adequate NO synthase inhibition). Our data suggests that not all angiogenic processes are NO dependent.
086 THE ADIPOCYTE DERIVED PEPTIDE HORMONE LEPTIN IS AN ENDOTHELIAL INDEPENDENT VASODILATOR IN HUMANS: IMPLICATIONS FOR VASCULAR HOMEOSTASIS
A. Momin, A. M. Shah, S. B. Wheatcroft, D. J. Grieve, L. John, A. E. l. Gamel, M. J. Marrinan, J. Desai, T. Nelson, C. Driver, R. Sherwood, M. T. Kearney.Cardiovascular Division, GKT School of Medicine, Kings College London. Cardiothoracic Department, Kings College Hospital, London, UK
It has been suggested that leptin, the adipocyte-derived peptide hormone has vasoactive actions in animal models. We sought to define the mechanisms and determinants of leptins vascular actions in humans. We examined the effect of leptin (0.0001–100nM) on ex-vivo vascular function in saphenous vein rings (SV) taken from 131 patients (age 65.7 (SD 0.7)) undergoing elective CABG. Mean maximal relaxation to leptin in the whole population was 24.5 (1.6)% and all rings relaxed fully to sodium nitroprusside. Relaxation to leptin was unaffected by the nitric oxide synthase inhibitor L-NMMA (0.1mM) (n = 8, 17.4 (3.4) v 17.8 (3.3)%, p = NS) and endothelial denudation (n = 8, 17.4 (4.4) v 22.5 (3.0)%, p = NS). Since the central effects of leptin are thought to be mediated through opening of potassium channels we explored the possibility that its vascular effects are mediated in a similar fashion. In the presence of KCl (30mM) to inhibit hyperpolarisation, the vasodilator effect of leptin was completely blocked (n = 10, 12.6 (5.6) v 0.08 (4.1)%, p<0.001). The only independent correlate of leptin mediated vasodilatation was TNF-α (R = 0.23, p<0.05). Markers of total fat mass (BMI) or visceral fat (waist) had no relationship with leptin-mediated vasorelaxation, supporting tissue specificity of leptin resistance.
Conclusion: Leptin is an endothelial independent vasodilator in humans, leptin mediated vasorelaxation is mediated by smooth muscle hyperpolarisation. The independent and positive correlate of leptin-mediated vasorelaxation is the cytokine TNF-a. These results may have implications for blood pressure regulation in different inflammatory conditions in humans such as sepsis and obesity.
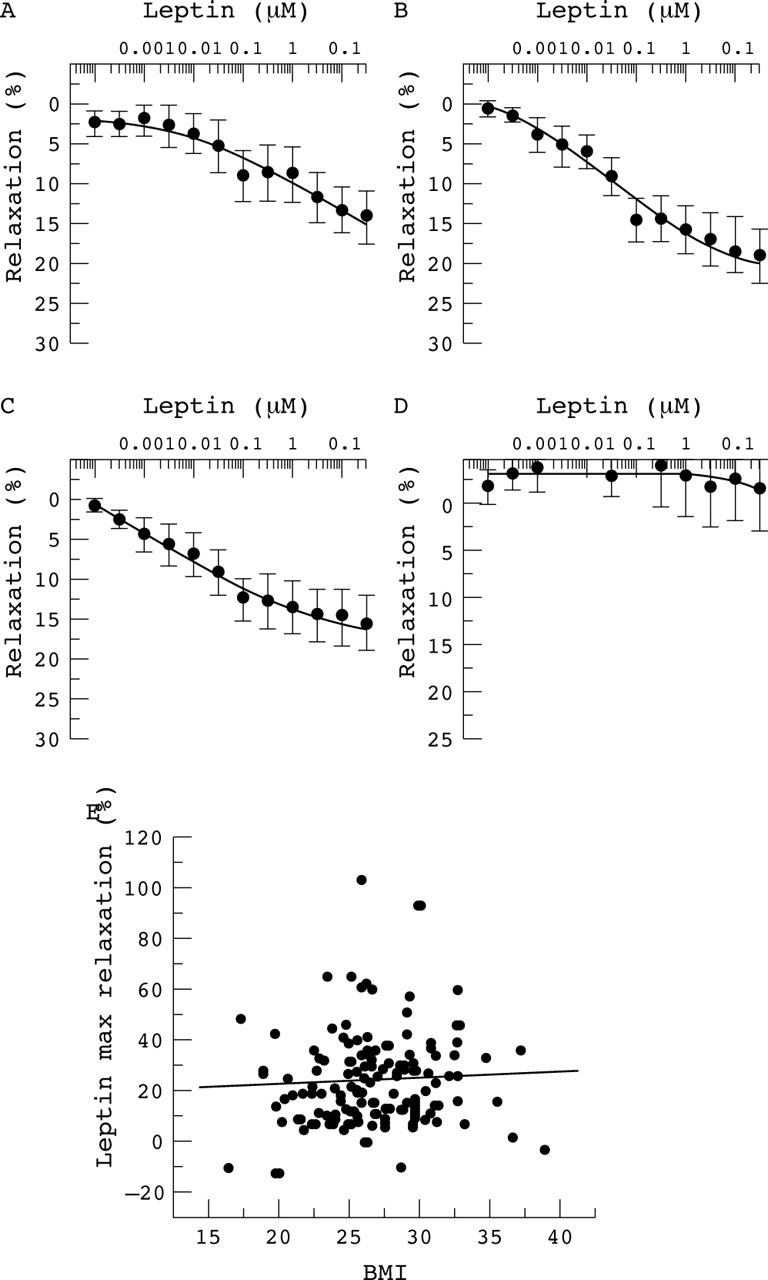
Abstract 86
087 INHIBITORY SMADS REGULATE PATHOLOGICAL CELLULAR DIFFERENTIATION IN ATHEROSCLEROSIS
A. Qasim, N. L. Figg, P. L. Weissberg, C. M. Shanahan.University of Cambridge, Cambridge, UK
In atherosclerosis vascular smooth muscle cells (VSMCs) migrate from the media to the intima where they de-differentiate from their contractile phenotype and contribute to matrix deposition, plaque calcification and lipid accumulation. We and others have previously shown that transforming growth factor-β (TGF-β) superfamily members influence VSMC phenotype, and can cause osteogenic differentiation of bone marrow stromal cells (BMSCs). BMSCs are mesenchymal stem cells that animal studies suggest contribute to vascular repair in atherosclerosis and transplant arteriopathy. TGF-β signalling is mediated by the Smad family of intracellular proteins, and inhibitory Smads (I-Smads) regulate this process, with Smad 6 blocking bone morphogenetic protein signalling and Smad 7 blocking this and the TGF-β pathway. We investigated the role of I-Smads in human VSMC and BMSC differentiation. In vitro VSMCs and BMSCs responded to osteogenic differentiation medium (ODM) with increased alkaline phosphatase (AP) activity and calcification detected by Von Kossa stain. Adenoviral overexpression of Smad 6 inhibited calcification and abolished the rise in AP activity in VSMCs and BMSCs in ODM (p<0.01). Oil red-O staining demonstrated that Smad 6 overexpression led to lipid accumulation in cytoplasmic vacuoles. This was associated with a significant rise in adipogenic markers PPAR-γ, CEBP-α and SREBP-1 as detected by Western blotting; a fall in smooth muscle markers α-smooth muscle actin and calponin, and reduced expression of the osteogenic transcription factor cbfa-1. Smad 7 overexpression partially inhibited the osteogenic effects of ODM, and this is consistent with partial inhibition of BMP signalling. Immunohistochemistry demonstrated high levels of I-Smad expression in VSMCs in normal arteries, with a significant reduction in I-Smad levels in VSMCs in atherosclerosis (p<0.01).
Conclusion: I-Smad overexpression inhibits osteogenic differentiation and leads to a reduction in smooth muscle cell markers in VSMCs and BMSCs, and causes adipogenic differentiation. These findings suggest that I-Smads may maintain the contractile smooth muscle phenotype in normal arteries, and that reduced expression may allow pathological differentiation of VSMCs and BMSCs in atherosclerosis.
088 BETA-BLOCKERS INHIBIT TRANSGENE EXPRESSION UNDER TRANSCRIPTIONAL REGULATION OF THE MAJOR IMMEDIATE-EARLY CYTOMEGALOVIRUS ENHANCER/PROMOTER IN VIVO
H. K. Salem, C. E. Appleby, P. Ranzjad, A. M. Heagerty, P. A. Kingston.Vascular Gene Therapy Unit, Department of Medicine, University of Manchester, Manchester, UK
The major immediate-early CMV enhancer/promoter (MIECMV) is the most potent and widely used promoter in vascular gene transfer studies. We previously reported that isoprenaline enhanced β-galactosidase (β-gal) expression in porcine coronary smooth muscle cells by MIECMV in vitro. This effect was prevented by β-blockade. We have investigated the effects of β-blockade on transgene expression in stented porcine coronaries.
Methods: Coverstents loaded with 2.5×109iu of RAd36 (expressing lacZ under control of the murine MIECMV) were deployed into the LAD of 15 large white pigs. 5 received oral propranolol (80 mg twice daily) for 96 hours pre-and 72 hours post-stenting, 5 received atenolol (100 mg once daily) and 5 received no β-blocker. After 72 hours arteries were harvested and OCT-embedded. β-gal expression was quantified in X-gal stained sections.
Results: Effective β-blockade was confirmed by reduced resting heart rate in treated animals (P = 0.02). The mean area of blue staining in sections from animals exposed to atenolol and propranolol was 6.67±4.6 and 2.8±1.6ìm2 respectively (see fig). The area in sections from animals not exposed to a β-blocker was 81.8 (SD 18.86) ìm2 (p<0.0001).

Abstract 88
Conclusion: β-blockade inhibits transgene expression within the vasculature from the murine MIECMV. As β-blockers are widely prescribed in cardiovascular diseases, attention must be paid to promoter selection in order to ensure that therapeutically relevant levels of transgene expression can be acheived in the presence of concomitantly administered pharmacologicals in the clinical setting.
089 A MEMBRANE-BOUND VACCINIA VIRAL PROTEIN ‘MEM35K’ BLOCKS CC-CHEMOKINE INDUCED CELL MIGRATION AND CC-CHEMOKINE ACTIVITY IN VITRO
C. Bursill, D. Greaves, K. Channon.Departments of Cardiovascular Medicine and Pathology, University of Oxford, Oxford, UK
CC-chemokines (CC-CKs) play an important role in mediating the chemotaxis of monocytes in atherosclerosis. The Vaccinia virus expresses a 35kDa soluble protein (35K) that inactivates the CC-CK class. If expressed locally in a vessel, broad-spectrum CC-chemokine blockade may be a therapeutic strategy to reduce CC-CK induced atherosclerosis. We have generated an adenovirus expressing membrane-bound 35K (Admem35K) with an N-terminal green fluorescent protein (GFP) to aid visualization. Successful gene transfer of Admem35K was confirmed by infection of 293 cells in vitro and mouse liver in vivo, as cell membranes expressed GFP and 35K protein was detected using western blotting. We then investigated whether mem35K could block CC-CK induced cell migration in vitro. In chemotaxis assays, cells co-expressing CCR5 and mem35K had significantly less migration towards CC-CKs RANTES (A) and MIP-1α compared to cells expressing CCR5 only (A). This did not occur for negative control receptor cells expressing the unrelated fractalkine receptor (CX3CR1) towards fractalkine (B). Also, addition of cells expressing only mem35K to cells only expressing CCR5, inhibited the CCR5-directed cell migration towards RANTES in a dose response fashion, indicating mem35K can sequester CC-CK activity.
Conclusion: These studies identify a CC-chemokine blockade using membrane-bound 35K expression as a promising strategy to determine the importance and therapeutic potential of CC-chemokines in monocyte migration in atherosclerosis.

Abstract 89
090 3D CONTRACTION FRONT MAPPING: NOVEL, HIGH RESOLUTION IMAGING OF MECHANICAL CONTRACTION OF THE LEFT VENTRICLE
S. Kapetanakis, E. Ho, S. P. Turner, M. J. Monaghan.King’s College Hospital, London, UK
LV Mechanical Dyssynchrony (LVMD) has emerged as a therapeutic target in resynchronisation therapy (CRT). Real-Time 3D Echo (RT3DE) offers superior spatial resolution of the LV and utilising this we developed Contraction Front Mapping (CFM), a novel modality to combine temporal and spatial visualisation of the contraction of the LV.
Methods: 20 patients were investigated on clinical grounds. 16 patients had LV dysfunction, of which nine had left bundle branch block on ECG and one had a permanent pacemaker (PPM). Of the four patients with normal function, one had a PPM. CFM was derived by representing the myocardium that reaches peak contraction every 25 milliseconds using a bulls-eye display of the LV, based on RT3DE.
Results: In six of the nine patients with LBBB, a U-shaped contraction wave was noted, with maximum delay in the postero-lateral region. In one patient, a similar pattern was noted at the septal region, while two patients had homogenous activation of the LV. In the 6 with normal conduction and LVF, three had homogenous conduction, while one had antero-apical delay (anterior MI) and two had U-shaped activation, with delay in the postero-septal region. Pacing induced early activation of the septal region. There was homogenous contraction with normal function.
Conclusion: CFM is a robust tool for non-invasive visualisation of spatial and temporal distribution of LVMD. In keeping with other studies, LBBB activation is variable. This may be valuable in patient selection for CRT.

Abstract 90
091 NEW GENERATION THREE-DIMENSIONAL ECHOCARDIOGRAPHY FOR LEFT VENTRICULAR VOLUMETRIC AND FUNCTIONAL MEASUREMENTS: COMPARISON WITH CARDIAC MAGNETIC RESONANCE
N. P. Nikitin, C. Constantin, P. H. Loh, J. Ghosh, E. I. Lukaschuk, A. Bennett, S. Hurren, A. L. Clark, J. G. F. Cleland.University of Hull, Kingston upon Hull, UK
Non-invasive assessment of left ventricular (LV) structure and function is important in the evaluation of cardiac patients. This study was designed to test the accuracy and reproducibility of new generation 3-dimensional echocardiography (3DE) in measuring volumetric and functional LV indices as compared with cardiac magnetic resonance (CMR).
Methods: 64 subjects with good acoustic windows, including 40 cardiac patients with LV ejection fraction (EF) <45%, 14 patients with EF ⩾45% and 10 normal volunteers underwent 3DE using a commercially available Philips Sonos 7500 scanner equipped with a matrix phase-array ×4 ×MATRIX transducer, and CMR on a 1.5T Signa CV/i scanner (GE Medical Systems). Volumetric assessment was performed with analytical 4D-LV-Analysis software (TomTec) for 3DE and MRI-Mass software (Medis) for CMR.
Results: The study subjects represented a broad spectrum of LV dimensions and global function. LV end-diastolic volume (EDV) varied from 66 ml to 371 ml (on 3DE) and from 61 ml to 367 ml (on CMR). LV end-systolic volume (ESV) ranged from 15 to 305 ml (on 3DE) and from 8 to 310 ml (on CMR), and LV EF varied from 12 to 82% (on 3DE) and from 12 to 88% (on CMR). We found no significant differences in LV EDV, ESV and EF with excellent correlations between the indices measured using 3DE and CMR (r = 0.97, r = 0.98, and r = 0.94, respectively). Bland-Altman analysis revealed bias of 7 ml for EDV, 3 ml for ESV and −1% for EF for 3DE with corresponding limits of agreement (2SD) of 28 ml, 22 ml and 10%. Intraobserver and interobserver variability were for EDV: 3% and 4% (3DE) v 2% and 2% (CMR), for ESV: 3% and 6% (3DE) v 2% and 3% (CMR), and for EF: 4% and 4% (3DE) v 2% and 4% (CMR), respectively.
Conclusion: New generation 3DE provides accurate and reproducible quantification of LV volumetric and functional data in subjects with good acoustic windows as compared with current golden standard of non-invasive cardiac imaging, CMR.
092 CAN REAL-TIME 3D ECHOCARDIOGRAPHY PREDICT REVERSE LEFT VENTRICULAR REMODELLING POST CARDIAC RESYNCHRONISATION THERAPY?
S. Kapetanakis, E. Ho, S. P. Turner, M. T. Kearney, M. J. Monaghan.King’s College Hospital, London, UK
Left ventricular mechanical dyssynchrony (LVMD) has been linked with reverse LV remodelling post cardiac resynchronisation therapy (CRT). We investigated the accuracy of Real-Time 3D Echo (RT3DE) in predicting the long term outcome from CRT.
Methods: 26 patients undergoing CRT were investigated prior to, 2 (SD 1) days and 10 (1) months post implantation of biventricular pacemaker. NYHA class, 2D and RT3D echo were recorded on both occasions. RT3DE datasets were analysed offline to calculate the end-diastolic volume, LVEF and to produce regional time-volume curves corresponding to the 16 standard myocardial segments. A Systolic Dyssynchrony Index (SDI) was estimated from the dispersion of times to minimum volume for all 16 regions.
Results: RT3DE was performed in all patients prior to CRT and in 16 patients at 10±1 months. Responders were identified by reduction in NYHA class 2 months post CRT, at which time 3 patients reported no symptomatic improvement (11.6%) and had significantly lower pre-implant SDI (p = 0.04). Reverse remodelling was defined as reduction in EDV ⩾20%. ROC curves for pre-implant SDI, EDV and LVEF showed that only SDI was predictive (AUC 0.841). A cut-off of 9.2% had a sensitivity and specificity of 88.9% and 85.7% respectively.
Conclusion: Real-Time 3D quantification of LVMD had high predictive value for the occurrence of reverse LV remodelling long term post CRT in this cohort. Larger studies are needed to confirm these findings.

Abstract 92
093 ROLE OF REAL-TIME TRANSTHORACIC 3D ECHOCARDIOGRAPHY IN THE ASSESSMENT OF MECHANICAL ASYNCHRONY
E. Liodakis, O. Al Shareef, D. Dawson, P. Pearson, P. Nihoyannopoulos.Echocardiography Department, Hammersmith Hospital, London, UK
Introduction: Mechanical asynchrony (MA), assessed with Real-Time 3D echocardiography (RT3DE) is a major observation in patients with left ventricular dysfunction. This asynchrony can be measured using the Dyssynchrony Index (DI), which derives by calculating the standard deviation of the time it takes each of the 16 segments, as described by the ASE, to reach its minimum volume.
Methods: We investigated 35 heart failure patients, which were paired with 35 normal subjects. RT3D scanning was performed using the SONOS7500 system. Offline analysis was performed with the Tomtec software.
Results: From the 35 patients that were investigated 38%had mild, 40% moderate and 22% severe systolic dysfunction. The DI was 9.5 (SD 1.1),12.8 (1.2) and 17.5 (1.2) respectively which was statistically significant higher than that observed in the normal subjects(5.6 (0.9) p<0.01). A strong negative correlation between the ejection fraction and DI was found with a higher systolic dysfunction associated with a higher degree of asynchrony.(r = −0.78 n = 35, p<0.01, fig 1). The length of the QRS complexes was <120 minutes in 29%, between 120—140 minutes in 26.4% and >140 minutes in 45% of the patients. The DI was 6.1 (1.1),13.2 (1.3) and 16.8 (1.09) respectively. There was a positive correlation between the length of the QRS complex and the DI (r = .44 n = 35, p<0.001).

Abstract 93
Conclusion: RT3DE is an effective tool for quantifying mechanical asynchrony which is strongly correlated with systolic dysfunction and electrical asynchrony.
094 PROGNOSTIC VALUE OF MYOCARDIAL CONTRAST ECHOCARDIOGRAPHY IN PATIENTS PRESENTING TO HOSPITAL WITH ACUTE CHEST PAIN AND NEGATIVE TROPONIN
P. Jeetley, L. Burden, K. Greaves, R. Senior.Department of Cardiology, Northwick Park Hospital, Harrow, Middlesex, UK
Background: Myocardial contrast echocardiography (MCE) is a new bedside technique that facilitates the diagnosis of coronary artery disease (CAD). We hyopthesised that MCE can be used to risk stratify patients with coronary risk factors presenting to hospital with acute chest pain, non-diagnostic ECGs and negative 12-hour troponin.
Methods: All subjects underwent standard clinical tests for risk stratification. Subsequently low power MCE was performed using SonoVue as a continuous infusion at rest and following vasodilator stress. Patients were recommended for coronary angiography by treating physicians on the basis of standard tests for risk stratification and blinded to MCE results.
Results: A total of 139 patients underwent MCE at a mean time of 17 (SD 27) days after admission. At coronary angiography, 26 (19%) patients were found to have significant CAD, 21 (81%) of which were detected by MCE. At follow-up (7.3 (4.1) months), patients with an abnormal MCE (n = 49 pts) had higher cardiac event rates (death, non-fatal myocardial infarction and urgent revascularisation) compared to those with normal MCE (36% v 7%; p<0.0001). Hard cardiac event rates (death and non-fatal myocardial infarction) were low 3(3%) in the patients with normal MCE (n = 90 pts).
Conclusion: MCE accurately classified patients presenting to the hospital with coronary risk factors but troponin negative chest pain into high and low risk groups. A normal MCE confers an excellent prognosis in such patients.
095 IMPROVED ACCURACY OF LOW POWER CONTRAST ECHOCARDIOGRAPHY FOR THE ASSESSMENT OF LEFT VENTRICULAR REMODELING COMPARED WITH UNENHANCED HARMONIC ECHOCARDIOGRAPHY FOLLOWING ACUTE MYOCARDIAL INFARCTION: COMPARISON WITH CARDIAC MAGNETIC RESONANCE IMAGING
T. K. Lim1, R. Janardhanan1, L. Burden1, P. Chai2, J. Moon2, D. Pennell2, R. Senior1.1Department of Cardiology, Northwick Park Hospital, Harrow, Middlesex; 2Royal Brompton Hospital, London, UK
Background: Assessment of left ventricular (LV) remodeling following acute myocardial infarction (AMI) has both therapeutic and prognostic implication. Low power contrast echocardiography (CE) has the advantage of simultaneously assessing myocardial perfusion and LV remodeling. We aimed to evaluate the accuracy of low power CE to assess LV remodeling following AMI compared to unenhanced harmonic echocardiography (HE).
Methods: Accordingly, 36 consecutive patients underwent HE, CE (SonoVue) and cardiac magnetic resonance (CMR) imaging 7–10 days after AMI. LV ejection fraction (LVEF), LV end-systolic volume (LVESV), and LV end-diastolic volume (LVEDV) were assessed.
Results: Absolute differences for LVESV and LVEDV between CMR and CE was significantly smaller than that between CMR and HE (table). CE estimate of LVEF more accurately classified patients into LVEF <35%, 35–45%, >45% (agreement = 83%, kappa = 0.66 with CMR) compared to HE (agreement = 69%, kappa = 0.33 with CMR).
Abstract 95
Conclusion: Low power CE is more accurate than HE for the estimation of LV remodeling after AMI.
096 CAN REPERFUSION BE PREDICTED BY ACUTE THICKENING OF THE AT RISK MYOCARDIUM IN STEMI? FULL PRESSURE V PRESSURE LIMITING REPERFUSION
E. Merli, S. Sutcliffe, T. Karu, A. Baltabaeva, A. Kiotsekoglou, A. Marciniak, S. J. Brecker, N. Bunce, G. R. Sutherland.Department of Cardiology, St George’s Hospital, London, UK
Experimental studies have shown that if an acute transmural myocardial infarction is reperfused at full pressure there is an immediate and persisting increase in end-diastolic wall thickness due to massive intramural oedema with the amount of oedema inversely related to the % residual stenosis in the infarcted related artery. To determine if these findings are paralleled in the clinical setting and whether the resultant myocardial substrate differs after PCI v thrombolysis, (the latter having a higher incidence of residual flow limiting stenosis in the culprit vessel), the following study was undertaken.
Methods: 33 consecutive pts with STEMI were enrolled. 14 underwent primary PCI (Group 1) and 19 thrombolysis (Group 2). All thrombolysed pts. routinely underwent day 2 control angiography. Of these 10/19 required secondary PCI for residual vessel stenosis. All 33 pts. underwent day 1–5 M mode and 2-D gray scale echocardiography to determine the myocardial area at risk and evolution of wall thickness. For analysis the left ventricle was sub-divided into 16 standard segments. Regional end-diastolic wall thickness (EDWT) was measured and EDWT in distal non-infarct segments was compared to EDWT in infarct segments after thrombolysis and after primary or secondary PCI.
Results: 528 myocardial segments were analysed: 158 infarct and 370 normal distal segments. Post primary PCI 13/14 pts had TIMI 3 flow. Post thrombolysis 11/19 had TIMI 3 flow, 1 TIMI 2, 3 TIMI 1, and 3 TIMI 0. Mean EDWT of infarct segments post thrombolysis compared to distal normal segments did not differ (p = ns) but was significantly thicker than the thin wall of those segments with no reflow. However, infarct zone wall thickness after PCI was significantly increased compared to distal normal segments (p<0,001). In the 10 thrombolysed pts with a flow limiting stenosis, there was a marked increase in EDWT following the secondary PCI (p<0.001).
Conclusion: In STEMI, full-pressure reperfusion is characterised by increased EDWT, consistently measureable by echo. In contrast, pressure limiting reperfusion(typical for thrombolysis) results in normal EDWT. Persistently thin segments (<80% distal wall EDWT) represent areas of no-reflow. This confirms experimental data that PCI and thrombolysis can differ in their resultant myocardial substrate.
097 PREDICTION OF TRANSMURALITY OF ACUTE MYOCARDIAL INFARCTION—COMPARISON BETWEEN MYOCARDIAL CONTRAST ECHOCARDIOGRAPHY AND RADIONUCLIDE PERFUSION IMAGING
S. A. Hayat1, R. Janardhanan1, J. C. Moon2, D. Pennell2, R. Senior1.1Northwick Park Hospital, Harrow, Middlesex; 2Royal Brompton Hospital, London, UK
Background: It is well established that contrast enhanced cardiovascular magnetic resonance imaging (CMR) can be used to assess transmural extent of infarction (TEI). We sought to determine the relative accuracy of myocardial contrast echocardiography (MCE) and Tc-99m sestamibi (SPECT) to predict TEI after acute myocardial infarction.
Methods: MCE, SPECT, and CMR were performed in 40 patients with AMI 7–10 days post thrombolysis. CMR was used to divide TEI into 5 groups: 0%, 1–25%, 26–50%, 51–75%, and 76–100%. TEI scores for dysfunctional segments were compared to qualitative MCE scores (0-absence of contrast, 1-heterogenous opacification, and 2-homogenous opacification) and SPECT (0-normal perfusion, 1-mild reduction, 2-moderate reduction, 3-severe reduction, and 4-absent uptake).
Results: There was a significant relationship (p<0.0001) between decreasing contrast intensity assessed qualitatively by MCE and increasing TEI on CMR as was the case for SPECT (fig 1). Segmental concordance between MCE and CMR was superior (kappa 0.50) than for SPECT and CMR (kappa 0.38). The sensitivity of MCE (75%) to predict >50% TEI was significantly (p<0.03) superior to SPECT (66%). Absence of uptake on MCE and SPECT virtually ruled out <50% TEI (negative predictive values: 93% and 89% respectively).
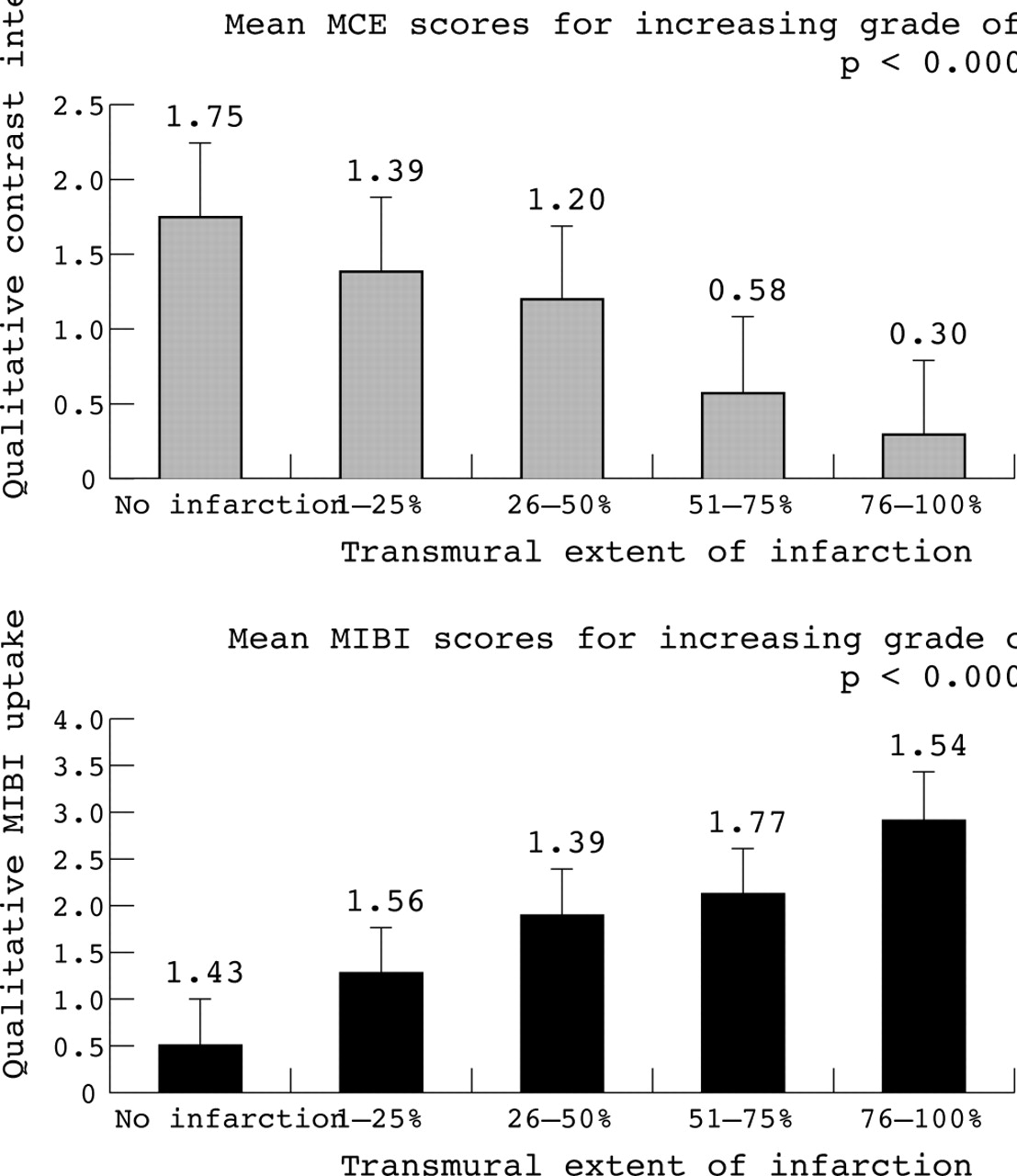
Abstract 97
Conclusion: We have demonstrated for the first time that both MCE and MIBI correlate well with the transmural extent of infarction. Furthermore, myocardial contrast echocardiography is significantly more sensitive in predicting greater than 50% transmural extent of infarction.
098 PROGNOSTIC VALUE OF NORMAL STRESS ECHOCARDIOGRAPHY IN PATIENTS WITH SUSPECTED NON-ST ELEVATION ACUTE CORONARY SYNDROME AND NEGATIVE TROPONIN
P. Jeetley, L. Burden, A. Banfield, R. Senior.Northwick Park Hospital, Harrow, Middlesex, UK
Introduction: A normal stress echocardiogram (SE) has been shown to predict excellent outcome in patients with known or suspected coronary artery disease (CAD). We investigated the prognostic value of SE in patients presenting to hospital with suspected acute coronary syndrome (ACS) and normal cardiac enzymes, but who required further risk stratification.
Methods: Patients were eligible for the study if they presented with cardiac sounding chest pain, a non-diagnostic ECG and a negative serum Troponin at 12 hours but had ⩾2 coronary risk factors. Early SE was then performed under dobutamine or exercise treadmill stress using standard protocols. Patients were considered to have a negative test if there was no new wall motion abnormality seen at peak stress. End points were death, non-fatal myocardial infarction (MI) and revascularisation.
Results: In total, 215 patients underwent SE, of which 166 (77%) had normal studies. Of the 166 patients with normal SE, 7 (4%) suffered cardiac events (1 death, 2 acute myocardial infarction, and 4 underwent revascularisation) at a mean follow-up of 7.5 (SD 4.4). The hard cardiac events were only 3 (1.8%). Presentation characteristics (TIMI score, number of risk factors, beta-blocker use or presenting ECG) or stress parameters (workload, exercise time, % of age-adjusted target heart rate) did not predict those patients suffering events compared to those who did not.
Conclusion: Normal SE confers an excellent prognosis in patients with suspected non-ST elevation ACS but normal cardiac enzymes and ⩾2 coronary risk factors. Thus, SE may be utilised to risk stratify such patients.
099 THE ROLE OF PARADOXICAL EMBOLISM AND THROMBOPHILIA IN ISCHAEMIC STROKE IN YOUNG ADULTS
S. R. Sastry, G. Riding, J. Morris, D. Taberner, N. Cherry, A. M. Heagerty, C. N. McCollum.Departments of Surgery and Cardiology, South Manchester University Hospital, Manchester, UK
Background: The role of paradoxical embolism in ischaemic stroke (IS) in young adults remains uncertain. We investigated venous-to-arterial circulation shunts (v-aCS), usually due to patent foramen ovale (PFO), and thrombophilia in a case-control study.
Methods: Young adults aged 16–39 years suffering IS (n = 101) between 1993 and 1998 were matched by age and sex to 101 controls from the same GP practices. V-aCS were detected by transcranial Doppler following intravenous microbubble ultrasound contrast. A “significant” v-aCS was defined as ⩾15 microbubbles within 12 cardiac cycles of contrast injection which correlated with a PFO on transoesophageal echocardiography. A “major” v-aCS was ⩾50 microbubbles spontaneously or ⩾10 microbubbles spontaneously with ⩾80 following provocation with cough or Valsalva manoeuvre. Venous blood was taken for a thrombophilia screen.
Findings: IS was more frequent in women and was associated with migraine and hypertension but not the other usual cardiovascular risk factors. The frequency of “significant” v-aCS in IS cases and controls was similar (45% v 40%; odds ratio (OR) = 1·22, 95% CI (0·70, 2·11); p = 0·48). This OR was increased to 1·34 (95% CI (0·74,2·42); p = 0·33) by adjustment for confounding factors. “Major” v-aCS were detected in 25% of IS cases compared with 12% of controls giving an OR of 2·20 (95% CI (1·04-4·64), p = 0·039). After adjustment for confounding factors, the OR increased to 2·80 (95% CI (1·21-6·48), p = 0·016). Thrombophilia was not significantly associated with IS.
Conclusion: Only “major” v-aCS were associated with stroke in young adults. Closure of smaller PFOs may not be justified in young adults suffering stroke.
100 IS EXERCISE TRAINING BENEFICIAL IN ADULTS WITH CONGENITAL HEART DISEASE?
J. S. Dua1, A. R. Cooper2, K. R. Fox2, A. G. Stuart1.1Congenital Heart Unit, Bristol Royal Infirmary, Bristol, UK; 2Deptartment of Exercise and Health Sciences, University of Bristol, Bristol, UK
A wide range of health benefits are associated with regular exercise training but its influence on exercise capacity & quality of life in adults with congenital heart disease (CHD) has not been fully investigated.
Methods: 61 patients were recruited and divided into three subgroups depending upon their NYHA class. Exercise capacity was determined by treadmill walking. Quality of life was ascertained using four questionnaires: Physical Activity Questionnaire (PAQ), Diener’s Satisfaction with Life Questionnaire (DSLQ), Physical Self-Perception Profile (PSPPs), and Health Survey (SF-12). Accelerometers were used to measure baseline energy expenditure. These data were used to devise an individualised incremental 10-week exercise regimen of walking for 5 days/week, with weekly increases in walking time. Assessment was repeated after 10 weeks.
Results: 44 patients (mean age 31.7 (SD 11) years; 26M) have completed the study measures so far. Treadmill walking time increased from a mean of 7.7 minutes to 9.6 minutes (p<0.0001). Mean questionnaire scores of all four questionnaires increased after training implying improvement in quality of life, physical self-perception and perceived health status (table).
Abstract 100
Conclusion: A simple physical activity intervention is effective in significantly increasing the exercise capacity of adults with CHD and improves the quality of life by improving physical self-perception, satisfaction with life and general health.
101 PREGNANT CARDIAC PATIENTS: DEVELOPMENT OF A GENERIC TEST TO EVALUATE THE FUNCTIONAL ADEQUACY OF DISEASED HEARTS TO COPE WITH PREGNANCY AND LABOUR
D. Barker, D. Schlosshan, H. McLoughlin, G. Mason, L. B. Tan.Leeds University and Leeds General Infirmary, Leeds, UK
Background: Pregnancy in women with heart disease is becoming increasingly common. From a cardiological perspective, pregnancy/labour (PL) can be viewed as a finite protracted stress on the heart. We propose that the adequacy of a diseased heart (irrespective of aetiology) to cope with PL can be evaluated by a generic exercise test.
Method: Sixteen pregnant women with heart disease (mean age 30 years (range 18–41), mean gestation 21 weeks) and 22 healthy pregnant women with no known cardiovascular disease (mean age 32 years (range 19–38), mean gestation 23 weeks) underwent maximal symptom-limited treadmill cardiopulmonary exercise testing (CPX). All participants exercised to cardiopulmonary limits (respiratory exchange ratio (RER)>1). Cardiac output (CO) was measured at rest and peak exercise using CO2-rebreathing methods. Cardiac power output (CPO) was calculated as the product of CO and mean arterial pressure (MAP).
Results: A single vasovagal reaction was the only complication. Compared to healthy pregnant women, pregnant cardiac patients had 16% lower peak CPO. This was due to 11% lower peak CO, and 5% lower MAP at peak exercise. Both groups exercised to similar levels (equivalent RER), although exercise duration was 18% lower in cardiac patients. See table (mean SD).
Abstract 101
Conclusion: Maximal CPX can be safely conducted in pregnancy. Pregnant cardiac patients were found to have a lower exercise cardiac reserve compared to controls. This generic test would enable identification of individual pregnant patients with congenital or acquired cardiac diseases who have limited cardiac reserve to cope with the cardiovascular stresses of pregnancy/labour.
102 QUADRICEPS AND RESPIRATORY MUSCLE STRENGTH IN PATIENTS WITH A FONTAN CIRCULATION
M. Dayer, B. Johansson, N. Hopkinson, E. Swallow, B. Bouzaz, A. Moore, M. Gatzoulis, M. Polkey.Respiratory Muscle Laboratory, Royal Brompton Hospital, London, UK; Adult Congenital Heart Disease, Royal Brompton Hospital, London, UK
Adults with a Fontan Circulation have similarities to patients with congestive heart failure (CHF). In patients with CHF, Quadriceps strength (QS) is reduced and tests of respiratory muscle function have suggested mild respiratory muscle weakness. However, there are no data yet as to whether there is muscle dysfunction in patients with a Fontan Circulation. We studied 20 adults (11 women), 16.1 (SD 3.8) years after their initial Fontan operation, and 20 healthy age (Fontan: 25.0 (6.6) years; controls 27.2 (3.0) years, p = 0.095) and sex-matched controls. The controls were taller (1.73 (0.11) m v 1.64 (0.08) m, p = 0.008) and heavier (66.6 (11.6) kg v 57.6 (10.3) kg, p = 0.011). 15/20 Fontan patients were in NYHA class I, 3 were in class II, and 2 were in class III. Maximal QS was assessed using a specially adapted chair. Predicted QS was calculated by the formula 0.75 x body mass. The maximal static inspiratory pressure averaged over 1s (MIP) was used as a measure of inspiratory muscle strength. Predicted MIP was calculated from published regression equations. Peak QS was reduced in the Fontan group (362 (128) N v 491 (152) N, p = 0.011), but when body mass was adjusted for this difference became less marked (85 (26)% predicted v 99 (20)% predicted, p = 0.088). Inspiratory pressures were not significantly reduced in the Fontan group (MIP: 89.4 (35.1) cmH2O v 97.2 (23.2) cmH2O, p = 0.436; percent predicted MIP 95.0 (34.6)% v 100.0 (15.9)%, p = 0.434). By ATS criteria only 2 patients in the Fontan group, both of whom had a reduced NYHA class, had clinically important inspiratory muscle weakness.
Conclusion: QS is reduced in patients with a Fontan circulation. Inspiratory muscle strength is preserved in those with a high functional class. It may, however, be impaired in patients with symptoms of heart failure, potentially compromising the respiratory drive to transpulmonary blood flow and cardiac output in the Fontan circuit.
103 LATEST RESULTS OF ENDOCARDIAL ARRHYTHMIA ABLATION FOLLOWING THE MODIFIED FONTAN
D. J. Abrams, M. J. Earley, S. C. Sporton, M. A. Gatzoulis, M. J. Mullen, J. A. Till, S. Cullen, J. E. Deanfield, R. J. Schilling.St. Bartholomew’s Hospital, The Royal Brompton Hospital, The Heart Hospital
Introduction: Radiofrequency ablation (RFA) of atrial arrhythmia after the Fontan procedure is challenging due to distorted anatomy, difficulty in creating transmural lesions and complex arrhythmia mechanisms. We examined if technological advances improve outcome in the short to medium term.
Methods: Studies were performed in 15 pts aged 25.7 (SD 9.7) years (range 15–44) 8.2 (6.8) years after atriopulmonary (12) or RA-RV (3) modifications of the Fontan. Simultaneous electroanatomic and non-contact mapping were used. Chamber anatomy derived from contrast MRI was used in 8 cases to aid geometry construction. Activation maps were created during SR, atrial pacing and arrhythmia on both systems. Entrainment and pace mapping were used to identify candidate sites for cooled RFA. Acute success was defined as termination during RFA and non-inducibility. Freedom from arrhythmia was assessed by symptoms and ECG.
Results: Arrhythmia was incessant in 4 patients and induced in 11. 31 circuits were mapped (CL 365 (120) ms), which were macroreentrant (23), focal (6), AVNRT (1), and left atrial (1). RFA of 23 circuits lead to termination in 20 (87%) and slowing in 1 (5%). 2 (9%) terminated spontaneously and were non-inducible after RFA in SR. RFA was not attempted due to non-sustained (4), left atrial (1), AVNRT (1), and para-Hisian focal activation (1). Procedure duration was 295 (75) mins and screening time 26 (15) mins, not significantly altered by the use of MRI data. There were no complications. At 8.6 (7.9) months’ follow up arrhythmia has occurred in 4 pts, successfully treated by medication (2) or repeat ablation (1). One patient has brief self-terminating episodes of palpitations not treated. All report significant clinical improvement. Nine out of 13 patients ablated (70%) patients are arrhythmia free. Anti-arrhythmic drugs have been stopped in 8 pts.
Conclusion: The results of RFA using modern mapping and ablative technology following the modified Fontan procedure are encouraging, and although arrhythmia recurrence occurs it can be successfully treated. Radiofrequency ablation is safe and should be considered first choice treatment in those without surgical indications.
104 ROLE OF THE PLANAR CELL POLARITY PATHWAY IN THE DEVELOPMENT OF THE OUTFLOW TRACT
H. Phillips, D. Henderson.Institute of Human Genetics, University of Newcastle upon Tyne, UK
The Loop-tail (Lp) mutant mouse has congenital heart defects that include double outlet right ventricle, where the aorta remains connected to the right ventricle. The proximal outlet septum, derived from the fused endocardial cushions in the proximal outflow tract, becomes muscularised during development, partitioning the aorta into the left ventricle. The muscularisation of the proximal outlet septum involves two steps. Firstly myocardial cells extend into the cushion tissue from the outflow tract wall (myocardialisation) and then this is followed by recruitment of mesenchymal cushion cells into the muscular lineage. Our data suggests that there is a defect in the muscularisation of the proximal outlet septum in Lp. The gene mutated in these mice is Vangl2, which is thought to play a role in the planar cell polarity (non-canonical Wnt) pathway. We have shown that Vangl2 is expressed in the myocardialising cells, which is consistent with a role in the muscularisation of the proximal outflow tract. We have shown that these cardiomyocytes show typical characteristics of motile cells, such as extension of lamellipodia and re-organisation of the actin cytoskeleton. Furthermore, other genes in the planar cell polarity pathway including Wnt5a, Wnt11, and Dvl2 are also expressed in the same cells. Genes downstream of Vangl2, including RhoA and Rho kinase1, which are known to play roles in regulating the cytosketelton and cell motility, are expressed in complementary patterns in the septum, but overlap in the myocardialising cells. However, in the Lp mutant mouse there is no region of common expression between these two genes and unlike the wild type littermates, the actin cytoskeleton in the myocardialising cells is not reorganised.
Conclusion: Vangl2 signalling is mediated via RhoA/Rho kinase 1 in the developing heart, and our data suggests that this pathway plays a major role in the development of the proximal outflow tract. This pathway is therefore a candidate for causing cardiac alignment defects, such as double outlet right ventricle, in humans.
105 IDENTIFICATION OF CARDIAC ABNORMALITIES IN THE SONIC HEDGEHOG MOUSE MUTANT USING OPTICAL PROJECTION TOMOGRAPHY
V. Hildreth, D. Henderson.Institute of Human Genetics, University of Newcastle upon Tyne, UK
Sonic Hedgehog (Shh) is a signalling molecule that mediates important patterning events during embryonic development. In vertebrates it is expressed in the limbs, notochord and floor plate, and can act as a short-range, contact-dependent factor, or as a long range, diffusible morphogen influencing many events including dorso-lateral patterning of the central nervous system, somite proliferation, and anterior-posterior patterning in the limb. Shh also has a critical role in the development of several organ systems. Targeted disruption of the shh gene in mice produces a range of defects including craniofacial abnormalities, laterality defects, aberrations of the central nervous system, and severe abnormalities of the heart, lungs, kidneys, and foregut. Many of the cardiac defects observed in shh-/- embryos have not been studied in detail, and the processes leading to such abnormalities are largely unknown. We have used optical projection tomography (OPT) to study a range of shh-/- whole embryos and dissected hearts at different gestational ages. OPT produces high quality three-dimensional images, which can be viewed through any plane, making them invaluable for detailed morphological studies. Our analyses have confirmed the presence of previously observed shh-/- heart abnormalities such as left atrial isomerism and atrial septal defects, and have identified novel abnormalities including double outlet right ventricle and common arterial trunk.
Conclusion: These studies highlight the uses of optical projection tomography in studying the developing heart, visualising previously undetermined defects in the sonic hedgehog mutant mouse.
106 RESYNCHRONIZATION THERAPY IN ADULTS WITH CONGENITAL HEART DISEASE
B. Skaria, C. Kiesewetter, J. Boullin, J. Morgan, A. Salmon, B. Keeton, G. Veldtman.Wessex Adult Congenital Heart Unit, Southampton, UK
Background: Cardiac resynchronization therapy (CRT) may be of particular benefit to adults with congenital heart disease (CHD) and ventricular dysfunction (VD).
Methods: Retrospective hospital records review.
Results: Between 2001 and 2004, 6 patients (pt) had 5 successful implants, 4 with defibrillators (5 males, mean age 37.2 (SD 15) years). Diagnosis included repaired Fallot (n = 2), congenitally corrected transposition of great arteries (CCTGA) (n = 1), Ebstein’s anomaly (n = 1) and Mustard with transposition (n = 2). The two Mustard pt had severe arrhythmia in addition to the severe heart failure which was common for all six pt. The left ventricle was paced first in the repaired Fallot pt and the right ventricle in the others. Implantation failed in the patient with Ebstein’s anomaly. Leads were placed epicardially in the two Mustard pt (no transvenous access to appropriate pacing site). High pacing thresholds due to scarring prevented early CRT in one pt. CRT was possible at 6 weeks. The transvenous approach was technically difficult in three pt: gigantic right atrium in two (Ebstein’s pt and CCTGA pt) and anatomic variation of coronary sinus in one (CCTGA) pt. Aortic valve Doppler time velocity integral and diastolic times were used to optimise CRT (early and at 6 weeks). At 10 months median follow up (range 4–36), all pt improved in regional and/or global ventricular function (n = 5) and arrhythmia control (n = 2: atrial fibrillation cessation in Fallot pt; ventricular tachycardia in Mustard pt). The other Mustard pt had more frequent atrial flutter, coinciding with changed antiarrhythmics. At last follow-up, two of three pts (Fallot pt, CCTGA) had developed severe pulmonary ventricle atrioventricular(AV) valve regurgitation, and recurrent heart failure (both pt had defibrillators, and the CCTGA pt had a preexisting transvenous lead). Three of the five pt currently remain off the transplantation list.
Conclusion: CRT may improve hemodynamics in adults with CHD and VD. Congenital and acquired anatomic variation dictates site and ease of lead placement. Epicardial leads may have high pacing thresholds early after procedure. Late AV valve regurgitation may precipitate heart failure/arrhythmia, and calls for improved lead placement techniques especially when CRT is combined with defibrillator therapy.
107 THE EFFECT OF BOSENTAN ON EXERCISE CAPACITY IN PATIENTS WITH EISENMENGER’S SYNDROME
R. J. Irving, J. O’Sullivan, R. Crackett, J. De Soyza, A. J. Fisher, J. L. Lordan, G. A. MacGowan, P. A. Corris.Northern Pulmonary Vascular Unit and Adult Congenital Group, Cardiothoracic Unit, Freeman Hospital, Newcastle-upon-Tyne, NE7 7DN, UK
Bosentan is an oral non-selective endothelin A and B receptor antagonist licensed for the treatment of idiopathic pulmonary arterial hypertension. We report our institution’s initial experience of the use of bosentan in the management of patients with Eisenmenger’s syndrome. 23 patients have been treated (median age 38 years, range (7–74)) for 196 days (1 to 967). 12 patients had atrial septal defects (ASDs), 3 patients had ventricular septal defects (VSDs), 2 had VSDs with pulmonary atresia, 2 had patent ductus arteriosus, 1 double outlet right ventricle, 1 transposition of great arteries palliated with Senning’s procedure, and 2 “complex” congenital heart disease. Therapy was initiated at 62.5 mg BD and increased to 125 mg BD after one month. Seven patients had discontinued therapy at 4 months because of perceived lack of clinical response, three of these (all non ASD) stopped within 7 days due to adverse effects and are not analysed. No patient required to stop therapy because of liver function abnormalities. Six-minute walk test (6MWT) was undertaken at baseline and at approximately 1 month and 3 months. Median 6MWT distance prior to treatment was 344 m (160–504), with a median Borg dyspnoea score of 3 (0–15), median oxygen saturations were 83% (72–97%) pre walk and 77% (48–97%) post-walk. At both subsequent 6MWTs, distance had increased: subsequent median walk distances were 362 m (235–502) and 363 m (235–503), (Wilcoxon matched pairs p = 0.01 and p = 0.02). There were no differences in Borg scale perception of breathlessness, nor in resting and post exercise oxygen saturation on treatment. Analysis of response according to cardiac anatomy showed that patients with an ASD had improved (median walk distances 341 m, 372 m, 388 m (difference at 1 month p = 0.01, 3 months p = 0.02)) and patients with other lesions had not (median walk distances 344 m, 340 m, 360 m, difference at one month p = 0.36, p = 0.40).
Conclusion: Exercise capacity is improved in patients with an ASD and Eisenmenger’s syndrome following treatment with bosentan measured by 6MWT distance. We found no significant change in Borg score or peripheral oxygen saturations. Endothelin antagonism is a promising treatment strategy for patients with Eisenmenger’s syndrome and an ASD, but requires further investigation in other lesions.
108 DOFETILIDE SIGNIFICANTLY REDUCES ACUTE AND CHRONIC DEFIBRILLATION THRESHOLDS IN PATIENTS WITH AN INADEQUATE DEFIBRILLATION SAFETY MARGIN
R. D. B. Simon, J. L. Sturdivant, R. B. Leman, J. M. Wharton, M. R. Gold.Medical University of South Carolina, USA
Introduction: Defibrillation thresholds (DFTs) are reduced with the use of modern lead systems, waveforms, and active cans. However, high DFTs with an inadequate defibrillation safety margin remains an infrequent but troubling problem, often requiring the addition of subcutaneous leads, connectors and possibly thoracotomy for patch placement. Dofetilide is a selective Class III antiarrhythmic drug that reduces DFTs in canine models. We hypothesied that dofetilide would reduce DFTs in humans, both acutely and chronically obviating the need for complex lead systems.
Methods and Results: 14 consecutive patients with DFTs >21 J at implant received dofetilide therapy and underwent follow-up DFT testing 3–330 days later. The patient population had a mean age of 59 (SD 11) years and were 93% were male. Mean ejection fraction was 29 (4)% with four patients receiving amiodarone. On dofetilide, acute DFTs (3–6 days) (N = 12) were decreased from 29 (4) J to 20 (7) J (p = 0.0004), resulting in a safety margin of 14 (8) J for the implanted devices. Chronic DFTs (43–330 days) (N = 8) were reduced from 27 (5) J to 12 (4) J (p = 0.0001). 4 patients subsequently had spontaneous arrhythmias terminated successfully with shocks. There was no proarrhythmia.
Conclusion: Dofetilide safely reduces DFTs both acutely and chronically helping to prevent the need for reoperation for placement of more complex lead systems. Dofetilide is safe and well tolerated in this group of patients with no proarrhythmia. This strategy should be considered when an inadequate defibrillation safety margin is present.
Abstract 108
109 ANGIOTENSIN II TYPE 1 RECEPTOR (AT1R) BLOCKADE HAS NO EFFECT ON THE SELF PERPETUATION OF AF OVER 4 WEEKS OF BURST PACING IN A GOAT MODEL OF ATRIAL FIBRILLATION (AF)
S. Kirubakaran, M. C. S. Hall, N. Peters, C. J. Garratt.Manchester Heart Centre, Manchester Royal Infirmary, Manchester, UK; Imperial College, London, UK
Previous studies have shown AT1R blockade may prevent short-term electrical remodeling and longer-term (4 weeks) structural remodeling in a rapidly paced dog model of AF. We evaluated the effects of the AT1R blocker candesartan during 4 weeks of atrial burst pacing in a goat model.
Method: Eight goats underwent atrial burst pacing according to the Allessie protocol. Four goats received oral candesartan (0.5 mg/kg/day) for 1 week before and for 4 weeks of burst pacing, whilst four received placebo. AERP, AF duration, AF cycle length (AFCL), and sinus cycle length (SCL) were recorded twice daily for 5 days, then daily. In six other goats, we assessed biological activity of oral candesartan (0.5 mg/kg/day) by the effect on the pressor response to angiotensin II (up to 40 ng/kg/min).
Results: Candesartan v burst pacing alone had no effect on SCL (595 (SD 9) ms v 581 (16) ms, p = ns), the AERP at baseline (155 (21.8) ms v 155 (19.4) ms, p = ns), the fall in AERP with atrial pacing (after 3 days 77.5 (2.5) ms v 85 (15.5) ms, p = ns) or AFCL (103 (2.9) ms v 103 (1.4) ms, p = ns). Candesartan had no demonstrable effect on increasing stability of AF with time (figure). Candesartan suppressed the pressor response to angiotensin II (at 40 ng/kg/min systolic BP rise 8.1 (3.2) mmHg v 34 (1.9) mmHg control, p = 0.002).

Abstract 109
Conclusion: Candesartan is absorbed orally in the goat and has activity at the AT1 receptor. Blockade of the AT1 receptor has no effect on atrial refractory period or induced AF duration during a 4-week protocol of atrial burst pacing in the conscious goat model.
110 THE SAFETY OF DC CARDIOVERSION UNDER SEDATION: LONG-TERM EXPERIENCE
A. Arya, J. Silberbauer, G. Bordoli, G. W. Lloyd, N. R. Patel, A. N. Sulke.Eastbourne District General Hospital, Eastbourne, UK
Introduction: External DC cardioversion (EDCV) is commonly used to terminate atrial tachyarrhythmias. This procedure is usually performed under general anaesthetic (GA) but long waiting times, improved efficiency and patient acceptability has increased interest in sedation EDCV. However, concerns remain regarding safety and efficacy of use of sedation in the absence of anaesthetists for EDCV. We provide data of our experience of nurse and physician led EDCV under sedation at Eastbourne General Hospital (EGH).
Design: Meta-analysis of 3 EDCV sedation studies.
Setting: EGH CCU.
Objective: To evaluate the safety of sedation-led EDCV.
Methods: The data from 582 patients who underwent 676 EDCV procedures of atrial tachyarrhythmias under sedation between 2000 and 2004 at EGH was subjected to a meta-analysis for outcome data on mortality, recall and sedation after-effects.
Results: The average age of this cohort was 71 (SD 10) years. Of 582 patients, 511 received in vitro sedation with diazepam and 71 patients with midazolam; the average dose ranged between 23.0–27.2 mg for diazepam and was 12.5 (5) mg for midazolam. The EDCV success rate was 86%. There were no deaths prior to hospital discharge and following 535 EDCV procedures in 441 patients (where such data were available), there were no deaths at 28 days. 92% of patients had total amnesia of the procedure at 24 hours and 96% at 48 hours. 98% of patients were satisfied with their experience: defined as a willingness to have the procedure again under sedation. 7% had minor side-effects as a result of the sedation, 2.9% required flumazenil administration but no patient required intubation and ventilation or presence of an anaesthetist. We estimate cost savings over the study period of at least £102,304 compared with EDCV under GA. The waiting list time fell from 6 months in 1999 to 4 weeks in 2004 with an increase of 50% in procedures undertaken.
Conclusion: EDCV under sedation is a safe, effective, and well tolerated method of EDCV without requiring the presence of an anaesthetist. Similar sedation techniques are used in ICD implant testing and guidelines currently suggest deep sedation should only be undertaken with an anaesthetist. Such guidelines will have a major impact on arrhythmia management and should be reviewed.
111 DOES INCREASED AREA OF PULMONARY VEIN ISOLATION DECREASE THE NUMBER OF NON PULMONARY INITIATORS OF ATRIAL FIBRILLATION?
R. D. B. Simon, S. W. Burke, J. L. Sturdivant, R. B. Leman, M. R. Gold, J. M. Wharton.MUSC
Background: Atrial fibrillation (AF) ablation should probably involve pulmonary vein (PV) isolation and ablation of non pulmonary initiators (NPIs). The optimal method for achieving this remains controversial. Three possible approaches are: method 1: An ostial segmental PV isolation; method 2: a periostial anatomical PV isolation; and method 3: a wide area circumferential ablation (WACA) including a roof and left atrial isthmus line guided by electroanatomical mapping. Theoretically, the number of NPI sites in the left atrium will be reduced by method 2 and more so by method 3, compared with method 1, making the subsequent ablation of NPIs less arduous and possibly unnecessary.
Methods: We performed AF ablation on 171 consecutive patients using Methods 1, 2, and 3 in consecutive cohorts. NPIs were then mapped and ablated. NIPs caused either repetitive premature atrial complexes, atrial tachycardia and/or AF, either spontaneously or after atrial burst pacing or induction of AF followed by DC cardioversion, on or off isoprenaline. The percentage of patients with NPIs in each ablation group seen after PV isolation was analysed.
Results: AF ablations were performed in 171 patients, with groups equivalently matched for age, gender, and presence of cardiovascular disease. The percentage of patients with NPIs with Methods 1, 2, and 3 was similar (49%, 53%, and 55% respectively). The percentage of right sided NPIs in each group was 23%, 44%, and 35%. The percentage of left sided NPIs was 38%, 35%, and 26%. The percentage of patients free of AF at 5 months was 75%, 75%, and 95%, respectively for Methods 1, 2, and 3.
Conclusion: The total number of NPIs is high and unaffected by the ablation method. WACA does not reduce the number of NPIs and additional ablation of NPIs with WACA may increase the single procedure success rate.
112 INTERACTIONS BETWEEN FOCAL TIGGERS AND LEFT ATRIAL SUBSTRATE IN THE INITIATION AND MAINTENANCE OF ATRIAL FIBRILLATION: A STUDY USING DOMINANT FREQUENCY ANALYSIS OF NON-CONTACT MAPPING DATA
T. Wong, P. Kojodjojo, D. W. Davies, V. Markides, N. S. Peters.St. Mary’s Hospital and Imperial College, UK
Although focal triggers (FT) are known to play a critical role in the initiation of atrial fibrillation (AF), the interaction between these and the left atrial (LA) substrate and their role in the perpetuation of AF remain largely unknown.
Methods: A non-contact system was used to map the LA and guide AF therapy in 21 patients (pts). Spontaneous episodes of AF lasting >10 s were recorded in 9 of these pts of whom 6 had paroxysmal and 3 had persistent AF. These episodes were divided into sequential 6.8 s segments of data, beginning with the point of initiation in paroxysmal AF pts, and analysed using fast Fourier transformation. Dominant frequencies (DF) of the reconstructed electrograms from 64 LA sites were calculated. FT were defined as discrete areas of high maximum DF, >2 Hz greater than neighbouring points. The first data segment from the point of initiation of AF was defined as the initiation phase and the remaining segments as the maintenance phase. Paroxysmal AF episodes were dichotomised into short (⩽30 s) or sustained (>30 s).
Results: A total of 25 AF episodes (97 segments) were analysed in pts with paroxysmal AF of which 14/25 (56%) were sustained. FT activity was seen in 22/25 episodes during the initiation phase (1.4 (SD 0.8) foci/episode, DF 11.2 (2.9) Hz). Those foci were located at the pulmonary veins (42%), anterior LA (18%), lateral LA (12%), LA appendage (9%), septum (6%), posterior wall (6%) and roof (6%). FT activity continuing into the maintenance phase was seen more frequently during sustained than short episodes (12/13 v 5/9, p<0.01). In 8/13 (62%) focally initiated and sustained paroxysms, the FT seen during both the initiation and maintenance phases had identical DF and locations. When comparing recordings from pts with persistent AF (30 segments) to those from paroxysmal AF pts (72 maintenance phase segments), FT activity was seen less frequently (8% v 57%, p<0.01).
Conclusion: Our data confirm the importance of LA triggers, not only during the initiation but also in the early maintenance of paroxysmal AF. FT activity was far less frequent during persistent AF, confirming the importance of other factors in maintaining persistent AF. These findings have important implications regarding choice of ablation strategies for pts with different patterns of AF.
113 CHARACTERISATION OF THE ELECTRICAL WAVEFRONTS SEEN IN HUMAN PERMANENT AF
M. J. Earley, D. J. Abrams, S. C. Sporton, R. J. Schilling.St Bartholomew’s Hospital, London, UK
The mechanism of maintenance of AF in humans is unclear due to the difficulty of sequential global mapping. We present the first analysis of non contact mapping (NCM) of left atrial (LA) permanent AF.
Methods: Patients (pts) underwent a catheter maze procedure to compartmentalise their LA, guided by NCM. AF was analysed in 19.5 s segments prior to the introduction of any ablation lesions. Wavefront (WF) number, direction, velocity, areas of scar, lines of block (electrogram delay of >50 ms), and characteristics of reentry circuits seen were analysed.
Results: 25 pts (22M/3F) aged 50 (SD 9), who had been in AF continuously for 12±8 months (5 (4) years since first episode), were studied. 11 pts had lone AF and 14 structural heart disease (10 hypertensive). Mean LA volume and diameter on echo were 98 (28) mls and 46 (7) mm. The number of WF detected simultaneously was 0, 1, 2 and >2 for 4, 51, 42, and 3% of the total time analysed. The WF were tracked and found to progress over large areas of the LA interacting with lines of functional block; a vertical line on the anterior wall extending down from the roof and a diagonal line extending from the septal roof, inferiorly and laterally toward the left inferior pulmonary vein (PV) on the posterior wall. Macroreentry circuits were found at the left PV and LA appendage (LAA) in 64%, on the anterior wall in 48% and around the right PV/septum in 12%. Cycle length (CL), pathway length and mean velocity of the reentry WF seen were 143 (27) ms, 90 (27) mm and 61 (17) cm/s. The CL of observed reentry circuits correlated well with a bipolar contact electrogram (egm) at the proximal (r2 = 0.89) and distal coronary sinus (r2 = 0.87) but not the right atrium (r2 = 0.1). The virtual egms of the posterior, septum and medial anterior LA were consistently more fractionated and of lower amplitude than other areas of the LA.
Conclusion: NCM reveals permanent AF to be characterised by smaller numbers of WF than previous studies suggest. Re-entry circuits are often found in the LAA/LPV area with cycle lengths similar to that measured by contact egms in the LA. This may explain why extensive ablation in this area has been a successful strategy. Further evidence is needed to define whether observed WF drive AF.
114 CHARACTERISTICS OF GLOBAL ELECTRICAL RESTITUTION DETERMINE VENTRICULAR ELECTRICAL STABILITY IN MAN
A. M. Yue1, M. R. Franz2, P. R. Roberts1, J. M. Morgan1.1Southampton General Hospital, UK; 2Veteran Affairs Medical Center, Washington, USA
Introduction: Ventricular fibrillation has been associated with steep action potential restitution (slope >1) and conduction velocity (CV) restitution, but clinical measurement of global electrical restitution had not been feasible. We studied global characteristics of electrical restitution in the human ventricle using noncontact mapping.
Methods: Activation-recovery interval (ARI) and CV restitution curves were simultaneously constructed from 16 regional segments of the left and right ventricle of 8 patients (6 male, age 42 (SD 17) years) following successful ablation of idiopathic ventricular tachycardia in the absence of structural disease guided by the Ensite system. ARIs were determined from reconstructed unipolar electrograms as validated with monophasic action potential recordings. ARI restitution slopes were determined using the overlapping least-squares linear segments method.
Results: Electrical restitution curves had biphasic or supranormal characteristics. The mean ARI restitution slope from 128 sites was 0.79 and was significantly greater in the left than the right ventricle (0.93 (SD 0.49) v 0.65 (0.26), p<0.001). Dispersion of ARI restitution slopes increased with decreasing diastolic intervals. CV restitution operated over a narrower range of diastolic intervals, reaching a plateau 10 (6) ms after refractoriness, compared with 38 (13) ms for ARI restitution (p<0.001). The magnitude of CV restitution was also greater (steeper) than ARI restitution (25 (10)% v 18 (9)%, p<0.001)
Conclusion: Global ARI restitution in the human ventricle without inducible arrhythmias is heterogeneous but the mean slope is <1. The narrow and steep CV restitution may underlie the mechanism for inducibility of ventricular fibrillation at very short diastolic intervals (<15 ms) and maintenance of myocardial electrical stability at longer diastolic intervals
115 CATHETER LOCATION TRIAL: A PROSPECTIVE RANDOMISED COMPARISON OF CARTO, NavX AND FLUOROSCOPY FOR CATHETER ABLATION
S. J. Harris, D. Gupta, M. Alzetani, M. J. Early, S. C. Sporton, A. W. Nathan, R. J. Schilling.Barts and the London NHS Trust, London, UK
Introduction: Non fluoroscopic mapping systems have the potential to dramatically reduce X-ray exposure generated by electrophysiological procedures, however, it is unknown whether they are as successful, safe, or cost effective as conventional mapping. The aim of this study was to compare electroanatomical (Carto) and high frequency electrical field (NavX) catheter location with conventional fluoroscopic guidance during routine ablation procedures.
Methods: All patients undergoing catheter ablation (except AV node and permanent AF cases) were randomised to a Carto, NavX or Fluoroscopy. Data was collected prospectively on our ablation database. Immediate procedure success was defined using standardised criteria (for example, bidirectional block for typical atrial futter, non inducibilty of AVNRT etc). All patients were seen 6 weeks following the procedure and success defined as both freedom from symptoms and no documented recurrence of any arrhythmia other than ectopy. Procedure costs included diagnostic and ablation catheters, Carto reference patch and the complete NavX kit. All costs are the published UK list prices.
Results: 84 patients (54% men) aged 48 (SD 17) were randomised. Results are displayed in the table. P values displayed are comparing to conventional.
Abstract 115
Conclusion: For all catheter ablation procedures, procedure duration and outcome are similar for Carto, Navx, and Conventional procedures. Both Carto and Navx are associated with reduced fluoroscopy time and radiation dose when compared to Conventional x-rays but with an increased cost.
116 REAL-TIME INTEGRATED X-RAY AND MAGNETIC RESONANCE IMAGING (XMR)-A NOVEL STRATEGY TO OPTIMISE PRECISE CATHETER PLACEMENT DURING PULMONARY VEIN ISOLATION
P. Lambiase, S. Hegde, M. Sermesant, K. S. Rhode, D. L. G. Hill, R. Razavi, J. S. Gill.Guy’s and St Thomas’ Hospital, King’s College London, London, UK
Background: We have developed a technique based on optical tracking to co-register MR & X-ray images enabling the real-time overlay of registered MRI derived cardiovascular anatomy onto live X-ray fluoroscopy images. Ten pulmonary vein (PV) isolation procedures were performed.
Method: MR and X-ray image registration is achieved by a combination of calibration and real-time optical tracking using a Northern Digital Optotrak 3020. A specially designed acrylic calibration object imaged using a T1-weighted MR sequence and then 50 tracked X-ray views were acquired for a range of c-arm orientations for calibration. Fiducial markers were automatically located in all the images and this data used to compute the perspective projection parameters of the X-ray system and the relationship between the MR scanner and the X-ray system. PV Isolation Cases: A 16-electrode Helix catheter (Cardima, USA) was deployed into the left upper, left lower and right upper PV orifices in turn and ablation was performed. Before each ablation, biplane X-ray images were acquired of the catheter and the 3D location of the catheter was reconstructed and displayed in the MR derived anatomy. During the procedure the left atrial surface overlaid onto the X-ray images of the catheter was displayed (Fig).

Abstract 116
Conclusion: XMR guidance improved: 1. Precise positioning of the helix catheter at the true PV ostium; 2. Visualisation of ostial cross-sectional shape and area; 3. Identification of PV branches and common ostia, which can impair helix catheter positioning; and 4. Localisation of small PV ostia. Our guidance system should reduce procedure times and patient X-ray doses in complex EP interventions.
117 IN-PATIENT, 30-DAY MACE AND MACE AT 1–6 MONTHS IN 73 CONSECUTIVE BIFURCATION LESIONS TREATED WITH TAXUS STENTS AND THE ‘CRUSH-T STENT’ TECHNIQUE
S. N. Doshi, J. N. Townend, N. P. Buller, S. S. Constantinides, R. Gulati, P. F. Ludman.University Hospital Birmingham, Birmingham, UK
Introduction: Bifurcation stenting remains controversial. Crush T-stenting is a recently described bifurcation stenting technique using Cypher stents. The technique has the potential to reduce the risk of restenosis at the side branch ostium by ensuring complete circumferential stent coverage. Data of CRUSH stenting using cypher stents are encouraging, however, no data are available for CRUSH-T-stenting using the taxus drug-eluting stent.
Aims: To examine the acute procedural success (no death, successful stent delivery, residual lesion <50%), in-patient MACE (death, myocardial infarction (creatinine kinase >5 fold), target lesion revascularisation (TLR)), 30-day MACE and MACE from 1–6 months in a consecutive series of bifurcation lesions treated by the CRUSH technique and using Taxus stents at the University Hospital Birmingham (UHB).
Methods: An analysis of prospectively gathered data entered on the interventional cardiology database at UHB for cases treated between July 2003 and December 2004.
Results: Over the period examined 73 patients underwent Crush stenting with Taxus stents. Mean age was 63 (SD 11) years, males 71%, diabetics 17.8%, and 59% were admitted with an acute coronary syndrome. Abciximab was used in 100%. Procedural success was 97.2% (71 cases), in one case failure was due to inability to introduce the side-branch stent and in the other to closure of the side-branch following main vessel stent deployment. A kissing balloon dilatation was attempted in 44 cases (60.3%) and was successful in 32 (72.7%). In-patient MACE was 0%. 30-day MACE was 2.7% (2 cases), due to one ischaemia driven TLR and one Q-wave-myocardial infarction following side-branch stent thrombosis. From 1–6 months MACE was 1.4% due to one case of TLR at the side-branch ostium.
Conclusion: The procedural success with bifurcation stenting using the Crush technique and Taxus stents is high and comparable to that using Cypher stents. In-patient and 30-day MACE rates are low, indicating good immediate and short-term safety. Ischaemia driven TLR to 6 months is also low suggesting a low rate of clinically relevant restenosis
118 RETROSPECTIVE STUDY TO INVESTIGATE THE USE OF DRUG ELUTING STENTS (DES) FOR THE TREATMENT OF IN-STENT RESTENOSIS – ‘ THE REAL WORLD’ EXPERIENCE
R. A. Anderson, F. Fath Ordoubadi, S. Young, B. Clarke, R. Khatter, L. Neyses, R. A. Swallow, K. D. Dawkins, N. P. Curzen.Manchester Royal Infirmary, Manchester, UK; Wessex Cardiac Centre, Southampton University Hospital, Southampton, UK
In-stent restenosis (ISR) remains the major limitation to bare metal stent (BMS) implantation during percutaneous intervention (PCI). Optimal treatment for ISR has yet to be determined, but data suggest that DES may be effective. We evaluated clinical follow-up of consecutive patients with BMS ISR treated with DES at the Manchester Royal Infirmary (MRI) from April 2002 to April 2004 reflecting ‘real world’ clinical practice, as a part of a larger two centre project.
Methods: 74 patients with significant ISR (after a BMS) in a native coronary artery or saphenous vein graft (SVG) were treated with a DES. Sirolimus (CYPHER) DES was used in 40 patients and Paclitaxel (TAXUS) DES in 34 patients. All patients were retrospectively followed up to evaluate the incidence of major adverse cardiac events (MACE), anginal class and the need for further angiography. Data was collected between 7 and 24 months after PCI (mean 15.2 months). 34.6% of patients were diabetic (17% insulin treated). 8% of lesions were ostial and 6.6% involved a bifurcation. 17% of lesions were in small vessels (reference diameter <2.5 mm), 45% were long lesions (>20 mm in length). 2.6% of cases involved ISR within a SVG. Clinical presentation at the time of diagnosis of ISR was new recurrent stable angina in 86.4% of patients, and as an acute coronary syndrome in 13.6%.
Results: Mortality at 15 months of follow up was 4% (range of time of death from the PCI was 3–7 months). 12% of patients did require further angiography during follow-up. However, only 3 patients (4%) developed ISR within the treated segment: 1.4% was treated by further DES implantation and 2.6% by CABG. There was clear symptomatic benefit, mean Canadian anginal class decreasing from 2 to 0.8. All patients achieved an improvement in angina with 21% becoming symptom free and 85.4% free of MACE. There was no difference in clinical outcomes in those who received a TAXUS(45%) and CYPHER(55%) DES.
Conclusion: This observational study shows that use of DES implantation for the treatment of ISR is safe, effective and associated with low recurrence rates in a ‘real world’ cohort of patients with complex anatomical and clinical factors.
119 CLOPIDOGREL PRELOADING AND MYOCARDIAL NECROSIS AFTER PCI
R. Moore, R. Lowe, J. L. Morris, W. L. Morrison, D. R. Ramsdale, R. A. Perry, R. H. Stables.The Cardiothoracic Center, Liverpool, UK
Background: Myocardial necrosis is a frequent occurrence after PCI with large (>3 times the upper limit of normal) cardiac enzyme releases recognized as a marker of poor prognosis. Preloading with Clopidogrel has been shown to offer clinical benefit and negate the advantage of Abciximab for elective patients undergoing PCI.
Methods: We examined the influence of Clopidogrel preloading on TnT and CK-MB release post procedure in a consecutive series of patients undergoing elective PCI between April 2003 and May 2004 at the Cardiothoracic Center Liverpool.
Results: Data was available for analysis on 933 patients. The cohort consisted of 680 (73%) men of mean age 61.4 (SD 9.8). Procedures were covered with Clopidogrel preloading in 88% of cases and GPIIb/IIIa inhibitors in 59%. 29% of patients underwent multi-vessel angioplasty, 50% multi-lesion angioplasty and procedural complications occurred in 3.8% of interventions. Multivariate predictors of >3 times normal CK-MB release were procedural complications (OR 13.64, p<0.001), multi-vessel angioplasty (OR 2.77, p<0.001, lack of angiographic success (OR 2.44, p = 0.020) and lack of Clopidogrel preloading (OR 2.56, p>0.001). The same variables were also independantly associated with a >3 times baseline TnT release: procedural complications (OR 22.30, p<0.001), multi-vessel angioplasty (OR 2.96, p<0.001, lack of angiographic success (OR 3.70, p = 0.020) and lack of Clopidogrel preloading (OR 1.32, p>0.001).
Conclusion: The lack of Clopidogrel preloading is an independent predictor of >3 times normal CK-MB and >3 times normal TnT release following elective PCI.
120 EVALUATION OF NOVEL DOSE OF C7E3FAB (ABCIXIMAB)ON PERIPROCEDURAL RELEASE OF TROPONIN I AND THROMBIN GENERATION MARKER (PF1+2) IN RADIAL ACCESS CORONARY STENTING AS ELECTIVE DAY CASE PROCEDURE ‘THE ENFORCED STUDY’
R. Anantharaman, S. Manivannan, S. Kumar, J. Ansell, P. Kelsey, M. Pirmohammed, A. Chauhan, D. H. Roberts.Blackpool Fylde & Wyre Hospitals NHS Trust, Blackpool. UK; University of Liverpool, Liverpool, UK
Background: Radial approach provides the safety and feasibility to do day case percutaneous coronary intervention (PCI). Standard dosing regimen of abciximab could not be used for day case PCI. We studied the effect of either bolus or bolus plus 6 hour infusion of abciximab, on Troponin I (TnI) and Prothrombin Fragment 1+2 (PF1+2) release in this setting.
Method: In this prospective study 180 consecutive patients were randomized to group 1 (n = 60): no abciximab, group 2 (n = 60): bolus abciximab (0.25 mg/kg) and group 3 (n = 60): bolus (0.25 mg/kg) plus 6 hour infusion (0.125 µg/kg/m) of abciximab. All patients were pre-treated with Aspirin 300 mg and Clopidogrel 300 mg 12 to 24 hour preprocedure. Blood samples were collected for TnI, PF1+2, and for inhibition of platelet aggregation (IPA) using the Ultegra RPFA assay at baseline, 15 minutes, 4 hours and 24 hours after study drug was given. Primary end point was the incidence of TnI elevation (>0.1 µg/L) at 24 hour post procedure. Major adverse cardiac events (MACE) including myocardial infarction (MI), target lesion revascularization (TLR) and death at 24 hour and 30d post procedure were recorded.
Results: There was no significant difference between the 3 groups in baseline and angiographic characteristics. Procedural success (residual stenosis <25%, without abrupt closure or symptomatic MI) was 96%, with 95% receiving stents and in >95% through successful radial access in all three groups. The results showed, elevated TnI% (38, 37 p>0.99, 35 p = 0.71) and PF1+2 (nmol/L) (22.30, 22.75 p = 0.89, 20.49 p = 0.52) in groups 1, 2, and 3 respectively. The PF1+2 results represents the mean value obtained after combining all the time points observed using area under the curve. The IPA% (15 minutes, 4 hour) were 90.9 (SD 9.8), 78.1 (10.7) and 92.8 (6.0), 84.1 (5.3) in groups 2 and 3 respectively. There was one death on day 28 in group 1 due to MI in the community (1.6% MACE at 30d) and no MACE at 24 hours.
Conclusion: Addition of either bolus or bolus plus 6 hour infusion of abciximab in patients pre-treated with Aspirin 300 mg and Clopidogrel 300 mg 12 to 24 hours pre-procedure is not associated with significant decrease in elevated TnI or thrombin generation (PF1+2 release) during uncomplicated moderately complex elective PCI.
121 CLINICAL PRESENTATION WITH IN-STENT RESTENOSIS IS NOT ALWAYS BENIGN
S. Wheatcroft, P. MacCarthy, R. Wainwright, A. Shah, M. Thomas.Department of Cardiology, King’s College Hospital, Denmark Hill, London, SE5 9RS, UK
In stent restenosis (ISR) typically results from smooth muscle proliferation and neointima formation, rather than progression of atherosclerosis, and is widely believed to present with recurrent stable anginal symptoms. We have previously shown that asymptomatic ISR detected incidentally at angiography has an excellent prognosis. Clinical experience, however, suggests that in a proportion of patients who do develop symptoms, ISR may present acutely and result in unplanned hospital admission. Our objective was to define more precisely the mode of presentation of symptomatic ISR in clinical practice.
Methods: We retrospectively analysed the database of all coronary interventional procedures carried out at our institution from February 1995 to November 2004 and selected those patients treated for ISR. Their mode of presentation was classified into three categories: 1) stable angina, 2) acute coronary syndromes (unstable angina or non ST-segment elevation myocardial infarction) resulting in unplanned hospital admission, and 3) ST segment-elevation myocardial infarction.
Results: A total of 467 patients received treatment for ISR. Median age was 63 years, 71% were male, 21% had diabetes, 48% were hypertensive, 55% were current, or ex-smokers, and 2% had renal failure. Of the 467 patients treated for ISR, 74% presented with stable angina. A substantial proportion, however, presented with either an acute coronary syndrome (24%) or ST segment elevation myocardial infarction (2%) resulting in unplanned hospital admission. Treatment of ISR comprised further stent deployment in 50% of patients (with drug eluting stents in 15%), rotational atherectomy in 11%, and intra-coronary brachytherapy in 29%. A procedural success of 96% was achieved, with an in hospital rate of major adverse cardiac events of 2.6% (4 patients died, 6 suffered a procedure-related myocardial infarction, and 2 required emergent coronary bypass surgery).
Conclusion: Over a quarter of patients treated for ISR presented with myocardial infarction or unstable angina, requiring unplanned hospital admission, prior to repeat intervention. The clinical manifestation of ISR, therefore, may be less benign than previously recognised. These data emphasise the importance of ongoing aggressive measures to prevent ISR.
122 TRANSRADIAL CORONARY INTERVENTION WITHOUT PRE-SCREENING FOR A DUAL PALMAR BLOOD SUPPLY
A. Ghuran, G. Dixon, A. de Belder, S. Holmberg, D. Hildick-Smith.Sussex Cardiac Centre, Brighton, UK
Background: Percutaneous coronary intervention via the radial artery is expanding nationally. It is usual practice to perform an Allen’s test or plethysmography to determine the presence of collateral blood supply to the hand prior to radial artery cannulation. We propose that pre-screening for a dual palmar blood supply is not necessary and the presence of a palpable radial pulse is sufficient to allow successful radial artery cannulation without subsequent vascular complications.
Method: We undertook a retrospective analysis of our interventional PTCA registry between 2002 and 2004. Only patients who had a transradial procedure without being pre-screened with an Allen’s test or plethysmography were included. Assessments were made the day after the procedure and at 30 days to determine if there were any complications.
Results: During the period under review, 479 coronary interventions were performed via the radial artery without pre-screening. There were 337 males and 142 females, mean age 65.5 (SD 10.8) years. 14% had had thrombolysis within 24 hours. There were 469 right and 9 left radial procedures. PCI success rate was 94.3%, with a 4% incidence of failure to cross the lesion. 30-day complication rates were: death n = 5; acute vessel closure n = 3; non-Q-wave MI n = 7; no reflow n = 5; pericardial effusion n = 1, cerebrovascular event n = 1. Vascular complications included two significant haematoma. There were no pseudoaneurysms, arteriovenous malformations or requirements for surgical intervention. There were no episodes of hand or forearm ischaemia.
Conclusion: Transradial coronary intervention can be safely undertaken without pre-screening for a dual palmar arch supply. This increases the numbers of patients eligible for the approach, and facilitates lab turnover, while maintaining an extremely low rate of vascular complications.
123 MEASUREMENT OF CORONARY STENT EXPANSION USING STENTBOOST™ IMAGE ENHANCEMENT SOFTWARE: A COMPARISON WITH INTRAVASCULAR ULTRASOUND
D. S. G. Conway, W. H. T. Smith, J. Moore, M. U. Sivananthan.Yorkshire Heart Centre, The General Infirmary at Leeds, Leeds, UK
Background: Under-expansion of coronary stents increases risk of restenosis. We compared assessment of stent expansion using StentBoost™ (a software package under development for enhancement of stent visibility during percutaneous intervention) versus intravascular ultrasound (IVUS).
Methods: We examined 43 coronary stents (median size 3×18 mm) in 33 patients (16 male; mean age 65 years). Immediately following stent deployment, StentBoost™ images were acquired in two view planes, followed by IVUS assessment of stent deployment using a controlled pullback device. Stent cross-sectional area (CSA, by IVUS) and diameter (D, by StentBoost™) were measured at 1 mm intervals. Minimum stent expansion was defined in 2 ways; firstly as minimum: mean CSA (%) for IVUS or minimum:mean D (%) for StentBoost™, and secondly as minimum:maximum CSA (%) or minimum:maximum D (%). The longitudinal position of minimum stent expansion was recorded.
Results: We found significant correlations (2-tailed Spearman) between IVUS and StentBoost™ measurements of stent expansion, using both definition 1 (r = 0.44, p = 0.003) and 2 (r = 0.57, p<0.001, see figure). In 36 of the 43 cases, longitudinal position of minimum expansion by IVUS and StentBoost™ were within 5 mm of each other.

Abstract 123
Conclusion: Measurement of coronary stent expansion using StentBoost™ appears feasible. Although IVUS and StentBoost™ are not equivalent, the observed relationships between StentBoost™ and IVUS suggest that StentBoost™ may be of clinical value for assessing stent expansion and locating the optimum longitudinal position for post-dilatation of under-expanded stents.
124 STENT EXPANSION: “A FAILURE TO DELIVER”. A COMBINATION OF DELIVERY BALLOON CONSTRAINT AND ACUTE STENT RECOIL REDUCES PREDICTED STENT DIMENSION BY 27% IRRESPECTIVE OF REFERENCE VESSEL SIZE
S. Aziz, J. L. Morris, R. A. Perry, R. H. Stables.The Cardiothoracic Centre, Thomas Drive, Liverpool, UK
Introduction: Despite using high-pressure stent deployment, coronary stents often fail to reach the expected diameter. Failure of the stent delivery balloon to achieve the expected diameter and stent elastic recoil after balloon deflation are two factors that contribute to stent under deployment. We investigated the incidence and magnitude of this problem.
Methods: We performed a prospective observational angiographic study recruiting consecutive patients undergoing coronary stent implantation between September 2003 and October 2004. Using quantitative coronary angiography (QCA) the minimal lumen diameters of the delivery balloon during stent deployment (MLD1) and following balloon deflation were measured (MLD2). The expected balloon diameter for the deployment pressure according to the manufacturer’s chart was also recorded. Delivery balloon deficit was measured by subtracting the MLD1 from the expected balloon size and stent recoil was calculated by subtracting MLD2 from MLD1. The relationship between delivery balloon deficit and stent recoil as a function of reference vessel diameter (RVD) and nominal stent diameter was calculated using analysis of variance.
Results: A total of 499 individual lesions with suitable images for quantitative coronary angiography were recorded. The final stent MLD was a mean (SD) 27.2 (7.2) % less than the predicted diameter. The delivery balloon deficit was 0.65 (SD 0.27) mm and stent recoil was 0.28 (0.17) mm. The mean (SD) percentage delivery balloon deficit was 18.9 (7.0) % and the mean (SD) percentage stent recoil was 10.0 (5.9) %. Percentage stent recoil and delivery balloon deficit was independent of RVD and nominal stent size.
Conclusion: Failure to achieve predicted final stent diameter is a real problem with contribution from delivery balloon under expansion and stent recoil. On average the final stent MLD is only 73% of the expected diameter irrespective of vessel size.
125 EVIDENCE FOR THE PRESENCE OF A SECOND WINDOW OF PRECONDITIONING IN HUMANS DURING SERIAL BALLOON OCCLUSION AT ANGIOPLASTY ON CONSECUTIVE DAYS
R. D. Smith, R. Edwards, M. Al-Obaidi, A. Asherson, M. Dalby, M. Al-Bustami, M. MAson.Harefield Hospital, Middlesex, UK
Background: An early window of ischaemic preconditioning (EIP) has been convincingly demonstrated in humans during serial balloon occlusions at angioplasty. Animal data also suggests the presence of a second window of preconditioning (SWOP) from around 12–72 hours. The effect of balloon coronary occlusion on SWOP has not been reported.
Methods: 14 patients (13 male, age 57.1 (SD 10.8)) for elective single vessel left anterior descending angioplasty were recruited. The lesion was crossed with a 0.014 pressure tipped guidewire. Three serial balloon coronary occlusions were performed (In1, In2, In3) separated by 5-minute periods of reperfusion. The following day, at an average of 19.6 hours after In1, 2 further balloon occlusions were performed as described within the existing stent (In4, In5). During each balloon occlusion the degree of ST segment deviation (STD), the collateral flow index (CFI, derived from simultaneous coronary sinus, coronary artery wedge and aortic pressures), and the chest pain score (on a 0–10 scale) were recorded.
Results: All patients completed the protocol on day 1. Two patients were withdrawn before day 2. We observed a significant attenuation of STD between In1 and In2 (2.77 v 2.18 mm, p = 0.01) and I1 and I3 (2.77 v 2.27, p = 0.01). In addition, a strong trend towards a significant reduction in STD between In1 and In4 (2.77 v 1.54, p = 0.08) was seen. A significant reduction in chest pain score between In1 and In4 (5.61 v 2.54, p = 0.01) and between In1 and In2 (5.61 v 4.79, p = 0.01) was also observed. There was no significant difference between CFI during each of the five inflations.
Conclusions: We have convincingly demonstrated EIP. In addition, we are, to our knowledge, the first to demonstrate evidence in humans to support the presence of SWOP in a coronary occlusion model. Larger studies are required to confirm this protective effect and possibly to allow it to be clinically harnessed.
126 ASSOCIATION BETWEEN SERUM THYROTROPHIN CONCENTRATIONS AND OCCURRENCE OF ATRIAL FIBRILLATION IN A LARGE COMMUNITY-BASED POPULATION OF ELDERLY SUBJECTS (THE BIRMINGHAM ELDERLY THYROID STUDY)
L. Roberts, J. Parle, J. A. Franklyn, S. Wilson, R. Holder, M. C. Sheppard, F. D. R. Hobbs, M. D. Gammage.Departments of General Practice & Primary Care, Cardiovascular Medicine and Medicine, University of Birmingham, Birmingham, UK
Atrial fibrillation (AF) is the commonest sustained arrhythmia, but the role of sub-clinical hyperthyroidism in the development of AF in an older population remains unclear. We conducted a prospective study of 5784 subjects aged 65 or over, without previous diagnosis of thyroid dysfunction, screened and identified in primary care. The cohort comprised 2934 women, 2850 men, mean age 73.5 years (range 63.5–98.6). All had TSH measured in a sensitive assay (normal range 0.4–5.5 mU/l), as well as free T4 (normal range 9–20 pmol/l), and resting 12-lead electrocardiograms. AF was present in 4.81% of the cohort. The prevalence of AF showed significant variation with serum TSH concentrations, being highest in the group with low but detectable TSH (AF in 1 of 43 subjects with TSH <0.1 mU/l (2.33%), AF in 12 of 109 subjects with TSH 0.1–0.3 (11.01%), AF in 258 of 5443 with normal TSH (4.74%), AF in 7 of 189 subjects with TSH >5.5 mU/l (3.70%), p<0.02). Only six of 109 subjects with low but detectable TSH had free T4 above the normal range, the highest value being 22.6 pmol/l. The association between TSH and AF was similar in men and women; as expected, AF was associated with increasing age (p<0.001) and male sex (p<0.001). Serum free T4 concentration was higher in those with AF than those without (mean serum free T4 14.89, standard error (SE) 0.13 pmol/l versus 14.41, SE 0.03 pmol/l, p<0.001). There was an association between AF occurrence and free T4 considered as a continuous variable (p = 0.001), both in the whole cohort and in men and women. This large prospective community-based study of the over 65’s has demonstrated an association between low serum TSH and occurrence of AF, as well as a positive association between serum free T4 and AF occurrence.
Conclusion: Our findings suggest that in this age group even mild thyroid hormone excess may be a risk factor for AF, a finding with potentially important epidemiological implications for cardiovascular morbidity and mortality in older subjects.
127 PREVALENCE, INCIDENCE, PRIMARY CARE BURDEN, AND MEDICAL TREATMENT OF ANGINA IN SCOTLAND: AGE, SEX, AND SOCIO-ECONOMIC DISPARITIES
N. F. Murphy, C. R. Simpson1, K. MacIntyre, F. A. McAlister2, J. Chalmers3, J. J. V. McMurray.1University of Glasgow, University of Aberdeen; 2University of Alberta, Canada; 3Information and Statistics Division, Edinburgh
Objective: To examine the epidemiology, primary care burden and treatment of angina. Design: Cross-sectional data from primary care practices participating in the Scottish Continuous Morbidity Recording scheme between April 1 2001 and March 31 2002.
Setting: 55 primary care practices (362,155 patients). Subjects: 9508 patients with angina.
Results: The prevalence of angina in Scotland was 28 per 1000 in men and 25 per 1000 in women (p<0.05). The prevalence of angina increased with increasing socioeconomic deprivation from 18 per 1,000 in the least deprived category to 31 per 1,000 in the most deprived group (p<0.001 for trend). The incidence of angina was higher in men (1.8 per 1,000) than in women (1.4 per 1000) (p = 0.004). The incidence of angina also increased with increasing socioeconomic deprivation (p<0.001 for trend). On average, patients with angina saw their general practitioner 0.5 times per annum. In contrast with prevalence and incidence, socioeconomically deprived individuals were less likely to see their general practitioner on an ongoing basis than affluent individuals (p<0.001 for trend). In men, 52% were prescribed b-blockers, 44% a calcium channel blockers, 72% aspirin, 54% statins, and 36% ACE inhibitors or angiotensin receptor blockers. The corresponding prescription rates for women were 46% (p<0.001), 41% (p = 0.02), 69% (p<0.001), 45% (p<0.001) and 30% (p<0.001). In patients under 75 years 52% were prescribed a β-Blocker and 58% a statin. The corresponding figures for patients over 75 years were 42% (p<0.001) and 31% (p<0.001)
Conclusion: Angina is a common condition and is more common in men than in women. Socioeconomically deprived individuals are more likely to have angina but are less likely to consult their general practitioner. Guideline recommended treatments for angina are underused especially in women and the elderly.
128 DECLINING CASE FATALITY RATES FOR ACUTE MYOCARDIAL INFARCTION IN SOUTH ASIANS AND WHITES IN THE LAST 15 YEARS
R. Liew, S. Sulfi, K. Ranjadayalan, J. Cooper, A. D. Timmis.Departments of Cardiology, Newham University Hospital NHS Trust, London Chest Hospital, UK
Background: Mortality rates from acute myocardial infarction (AMI) have been declining over the last two decades. It is not known if south Asians, in whom cardiovascular risk is high, have shared in the overall decline in infarct mortality.
Methods: Cross sectional, observational study involving 2640 patients (29% south Asian) with AMI admitted to CCU over a 15 year period. Outcome analysis was by time terciles: T1, 1988–1992; T2, 1993–1997; T3, 1998–2002.
Results: The proportion of south Asians increased from 24% in T1 to 42% in T3. South Asians were significantly younger than whites, more commonly male and diabetic, and less likely to smoke. Indices of infarct severity were similar in south Asians and whites, with declining frequency of ST elevation infarction (88.2% to 77.5%, p<0.0001), Q wave development (78.1% to 56.9%, p<0.0001) and mean (interquartile range) peak serum creatine kinase concentrations (1250 (567–2078) to 1007 (538–1758) IU/l, p<0.0001) over the 15 year period from T1 to T3. Rates of hospital death (13.0% to 9.4%, p<0.01), ventricular fibrillation (9.2% to 6.0%, p<0.001), and left ventricular failure (33.2% to 26.5%, p<0.0001) all declined, the changes showing no significant interaction with ethnicity. Odds ratios (95% CI) for the effect of time on risk of death increased from 0.81 (0.70–0.93), to 1.02 (0.87–1.21), after adjustment for indices of infarct severity (ST elevation, peak CK, Q wave development, and thrombolytic therapy). Additional adjustment for serum potassium concentration and diabetes, explained the effect of time on ventricular fibrillation, but not left ventricular failure.
Conclusion: There has been a significant decline in case fatality rates for AMI in south Asians over the last 15 years, comparable to that seen in whites. Rates of ventricular fibrillation and left ventricular failure have also declined. Declining case fatality rates are largely explained by reductions in indices of infarct severity.
129 ASSOCIATION BETWEEN COMMON POLYMORPHISMS OF THE PRO-OPIOMELANOCORTIN (POMC) GENE AND BODY FAT DISTRIBUTION: A FAMILY STUDY
M. Baker, N. Gaukrodger, B. Mayosi, H. Imrie, M. Farrall, H. Watkins, J. Connell, P. Avery, B. Keavney.Universities of Newcastle, Oxford and Glasgow, UK; The Cardiac Clinic, New Groote Schuur Hospital, Cape Town, SA
Background: Rare mutations in the pro-opiomelanocortin (POMC) gene cause severe early-onset childhood obesity. But, it is unknown whether common variants in POMC are responsible for variation in body weight or fat distribution within the commonly observed range in the population. We have examined the relationship between variants spanning the POMC gene which together capture the common genetic variation at that locus and measures of obesity (waist-hip ratio and body mass index) in a large family study.
Methods: Anthropometric measurements were made, and three polymorphisms of the POMC gene (RsaI in the promoter region, C1032G in the first intron, and C8246T in the 3′UTR) were typed, in 1428 members of 248 families. Evidence for association between genotypes and haplotypes and obesity phenotypes was assessed using variance components methods.
Results: There was strong linkage disequilibrium across the 10 kb of the POMC locus. Four common haplotypes of the three markers accounted for >97% of the haplotypes present in the population. There was significant association between genotypes at the C8246T (p<0.0001) and C1032G (p = 0.003) polymorphisms and waist-hip ratio (corrected for age, sex, smoking, exercise and alcohol consumption). Each T allele at C8246T (or G allele at C1032G) was associated with an 0.2 SD higher waist-hip ratio in a codominant fashion. When waist-hip ratio was additionally corrected for body mass index (thus providing a measure of body fat distribution throughout the range of body mass indices), there remained significant evidence for association with both markers, which was of similar magnitude and statistical significance. There was no association between genotype at any polymorphism and body mass index or plasma leptin level.
Conclusion: Common genetic variants at the POMC locus influence body fat distribution within the normal range. This suggests a novel role for POMC in metabolic regulation.
130 UNDERSTANDING VARIATION: APPLICATION OF STATISTICAL PROCESS CONTROL TO THE MYOCARDIAL INFARCTION NATIONAL AUDIT PROJECT DATABASE FOR 2003–2004
C. P. Gale, A. P. Roberts, J. S. Birkhead, A. S. Hall.Yorkshire Heart Centre, The General Infirmary at Leeds, Leeds, UK
Introduction: Standards of care for myocardial infarction set by the NSF for CHD are monitored by the Myocardial Infarction National Audit Project (MINAP). We compared the results of the 3rd MINAP annual public report with a statistical process control (SPC) model designed for undertaking multiple unit comparisons.
Methods: We generated scatter plots of performance, as a percentage for each target against the number of cases reported. Continuous binomial distributions were created from limit lines at 2.66 SD from the mean for all values up to the maximum number of cases reported. We studied the door to needle time (DTN), call to needle time (CTN), use of aspirin, beta-blockers and statins in all patients between 01/04/03 and 06/06/04. We used NSF goals to define achievement and to compare them with the number of hospitals above, below, or within the confidence limits (CL) as calculated by our scatter plots.
Results: There were 99,133 patients, which covered between 225 and 230 hospitals for the 5 variables. 87,427 fulfilled the inclusion criteria for analysis by secondary prevention drugs and 15,111 by DTN and CTN times. Scatter plots for thrombolysis goals demonstrated a wide dispersion of outcome data. Those for secondary prevention conformed to the CL, though there were easily visible outliers. For DTN, 165 hospitals achieved the NSF goals, but 198 were found within or above their CL. For CTN, 100 hospitals fell outside the ‘25%’ and ‘greater than 25%’ attainment limits, using SPC we only identified 40 below the lower CL. 12 hospitals failed to reach the NSF goals for aspirin usage post AMI, but when analysed by SPC 32 hospitals remained below the lower CL. For beta-blockers usage, 42 hospitals were below the lower CL and 49 outside the achievement goals. Statin use was comparable from SPC analysis and NSF goals.
Conclusion: We believe that these plots provide more useful information on unit performance, and in particular allow better comparisons between units performing different volumes of work.
131 THE GENETIC RISK OF ACUTE CORONARY EVENTS (GRACE) STUDY COHORT - DEMOGRAPHY AND DESCRIPTION OF A LARGE UK DISCORDANT-SIBLING COLLECTION
B. D. Brown, R. A. Lawrance, N. Kilcullen, A. J. Balmforth, A. S. Hall.Institute for Cardiovascular Research, University of Leeds and Leeds General Infirmary, Leeds, UK
Background: Case-control genetic studies may yield spurious associations due to unrecognised admixture of the underlying population rather than a true association between polymorphism and disease. Such misleading associations can be avoided by choosing siblings as controls.
Methods: Study participants were recruited nationwide, following a lengthy media campaign that involved extensive national and regional TV, radio, and newspaper coverage, as well as posters in GP surgeries and local hospitals. DNA was banked from sibships that were discordant for the overt development of premature coronary disease. By definition, those affected individuals had, had an MI, PCI, CABG, or angina (exercise test positive and/or angiogram showing at least one lesion >50%) before the age of 66 years.
Results: Between 2000 and 2003, 2871 valid individuals in 930 families were interviewed. An additional 610 siblings from 157 families were excluded due to non-validation, insufficient DNA yields or lack of discordance in the resulting completed sibship. 69% of the affected siblings had had MI, 30.3% PCI or CABG without MI, and 0.7% angina only. The average age of first event in those affected (A) was 51.5 years (range 25–65 years, SD 7.7 years, 76.1% male) versus average age of unaffected (U) sibs of 58.5 years (range 32–87 years, SD 9.4 years, 41% male). 79.4% of U siblings were older than average age of A siblings. The most common family structure was the AUU trio (53.4%), then AAU (18.1%) and AU (13.3%). A further 9.7% of sibships had a minimum of 2 affected and up to 6 unaffected siblings. The remaining 5.4% had one affected and up to 5 unaffected siblings. 98.8% were of Caucasian background, the median and mean family size was 3 and 3.1 respectively. There were significantly greater reported risk factors in the affected siblings (hypertension: 56.8% A v 43.2% U, dyslipidaemia: 67% v 32.7%, BMI greater than 25: 71.6% v 62.7%).
Conclusion: We have the largest UK collection of discordant sibships that should have many applications in genetic studies of CHD, including SNP-based analyses as well as family based tests of association and linkage, such as the sibling-transmission disequilibrium test.
132 RISK SCORES FOR PRIMARY PREVENTION OF CARDIOVASCULAR DISEASE: REFINEMENT AND EVALUATION REQUIRED
PBrindle, ABeswick.University of Bristol
Background: In general practice, cardiovascular risk-scoring methods are used to identify high risk, but currently asymptomatic patients so they can be offered preventive treatment and lifestyle advice. The choice of risk scoring method should be based on its accuracy in a particular population and its effectiveness in improving patient risk factors, risk behaviours, and health outcomes.
Aim: To evaluate the accuracy of cardiovascular risk scoring methods in different populations and their effectiveness in targeting primary prevention.
Method: Systematic review of cardiovascular risk scores including studies examining the accuracy of predictive functions and their effectiveness in improving risk factors, risk behaviours, health outcomes or treatment. Articles were identified from computerised databases using Cochrane Heart Group methods. Additional information was obtained from authors.
Results: Over 3300 articles were identified and 1000 acquired as potentially relevant.
Accuracy: 126 studies looked at methodological accuracy of risk scores in different populations. 36 reported on Framingham-derived methods in 50 separate populations. Framingham methods provided a reasonable discrimination between high and low risk individuals in representative populations. However, discrimination was poorer in studies of high-risk groups. In meta-analysis, the combined predicted-to-observed ratio revealed a tendency towards over-prediction but substantial heterogeneity suggested overestimation in lower risk and underestimation in high-risk populations.
Effectiveness: Only four randomised controlled trials could be identified. One study showed a reduction in blood pressure but not mean absolute risk, and another showed increased prescribing of blood pressure and lipid lowering drugs in a high-risk subgroup. Overall, there was no consistent benefit found in patients treated on the basis of a risk score compared to controls.
Conclusion: In broadly representative populations, cardiovascular risk scoring offers reasonable ranking of individual risk. Risk scoring methods overestimate in low-risk and underestimate in high-risk groups. As with any health technology, risk-scoring methods must show benefits if they are to be used in primary prevention. Randomised trials of risk scores in general practice are required.
Keywords: risk score, cardiovascular disease, primary prevention
133 HOMOCYSTEINE PREDICTS CARDIOVASCULAR RISK INDEPENDENTLY OF THE METABOLIC SYNDROME
T. Leong, A. Fitzgerald, C. McGorrian, I. Graham, the European COMAC Group.Adelaide & Meath Hospital, Dublin, Ireland; The Haughton Institute, Dublin, Ireland
Background: The metabolic syndrome (MS) increases the risk of cardiovascular disease (CVD). Our previous analyses suggest that newer risk markers such as homocysteine (Hcy) and apolipoprotein B (ApoB) are raised in the MS, and a graded association may exist between them and the components of the MS.
Aims & Methods: The European Concerted Action Project ‘Homocysteinaemia and Vascular Disease’ (COMAC) case control study was examined to determine possible independent or interactive effects between the MS, newer risk markers, and CVD. The NCEP definition of the MS was used with BMI⩾30 in place of waist circumference. Patients with any missing components of the MS were excluded from the analyses. The top quintile of controls (without CVD) define raised Hcy (>12.1 μmol/L) and ApoB (>1.4 mmol/L). All logistic regression analyses were corrected for age, gender, conventional risk factors (blood pressure, LDL cholesterol, smoking), creatinine, folate, vitamins B6 and B12. Results of the total 1,550 patients, 400 were excluded due to missing components of the MS. Of the 565 cases (with CVD), 162 (29%) had the MS. Of the 585 controls (without CVD), 67 (12%) had the MS. Raised Hcy (adjusted OR 2.2 95% CI 1.6–3.0) and the MS (adjusted OR 2.1 95% CI 1.4–2.9), but not ApoB, were significant univariate predictors of CVD in this analysis. In a logistic regression model that also includes the MS, raised Hcy, but not ApoB, was an independent predictor of CVD. Adjusted OR for CVD (p = 0.04) showing combined effects of raised Hcy and the MS were: raised Hcy alone 2.5, the MS alone 2.5, and raised Hcy in combination with the MS 2.8 (OR relative to those with neither).
Conclusion: Despite raised Hcy in the MS, the effects on CVD risk are independent. Hcy and the MS individually double CVD risk. Their combination is associated with an almost three-fold increase in CVD risk.
134 PATIENTS WITH NON-ST ELEVATION ACUTE CORONARY SYNDROMES ASSOCIATED WITH MYONECROSIS HAVE A SIMILAR RATE OF DEATH OR MI AS ST ELEVATION MI AT 6 MONTHS: AN AUDIT OF ALL ACS ADMISSIONS IN A UK DISTRICT GENERAL HOSPITAL OVER 1 YEAR
K. K. Ray, J. Bolton, A. Veitch, T. Clayton, P. Sheridan, R. Manivarmane, G. Payne, W. Baig.Doncaster Royal Infirmary, London School of Hygeine
Background & Aims: Non-ST elevation ACS represent a broad spectrum of cases from unstable angina (UA) to non-ST elevation MI (NSTEMI) with possibly variable clinical risk. We sought to evaluate the clinical risk across the spectrum of non-ST elevation ACS and compare that with ST elevation MI (STEMI) in a UK DGH and assess the patterns of care delivered.
Methods: All patients admitted with cardiac chest pain to Doncaster Royal Infirmary were recorded onto a central database. Patients were divided into UA (Troponin T <0.01 μg/l), TnT detectable but <0.1 μg/l non ST elevation ACS, TnT ⩾0.1 μg/l non ST elevation ACS and STEMI.
Results: Between 1/5/01 and 30/4/02 1467 patients with ACS were admitted. At 6 months patients with UA had the lowest rate of CV death or MI (2%), which increased across the spectrum of ACS to 23% among STEMI (See figure, p for trend <0.001). No difference in risk was observed between non ST elevation ACS (regardless of TnT threshold) & STEMI. In a multivariable model, the independent significant predictors of death or MI were age (OR 1.81), admission under a non-cardiologist (OR 1.82), previous MI (OR 1.49), diabetes (OR 1.97), and Log TnT (OR 1.36). Among the 3 high risk groups combined, the use of angiography <6 months was 10% and exercise testing was 26%.

Abstract 134
Conclusion: One fifth of ACS patients with myonecrosis suffer a major adverse event at 6 months in an average UK DGH setting. Possible strategies to improve clinical outcome may include increased invasive and non invasive cardiac tests and increased specialist care. This may have implications on service provision and medical resources.
135 DOES PRE-OPERATIVE ATRIAL CELL ELECTROPHYSIOLOGY PREDICT POST-OPERATIVE ATRIAL FIBRILLATION?
A. J. Workman1, D. Pau1, C. J. Redpath1, J. A. Russell1, K. A. Kane2, A. C. Rankin1.1Cardiovascular and Medical Sciences, University of Glasgow; 2Dept of Physiology and Pharmacology, University of Strathclyde
Background: Atrial fibrillation (AF) is common after cardiac surgery (CS). Post-CS AF is independently predicted by old age and by post-CS beta-blocker withdrawal. However, electrophysiological mechanisms and potential predictors of post-CS AF are poorly understood.
Aim: To test the hypothesis that pre-CS atrial cell action potential, effective refractory period (ERP) and ion current characteristics differ between patients who do and who do not develop post-CS AF.
Methods: Myocytes were isolated from right atrial appendages obtained from consenting patients just prior to CS, all in sinus rhythm. Action potentials and/or ion currents were recorded by whole cell patch clamp.
Results: Post-CS AF occurred within 7 days in 44 of 170 patients (26%). Patients with post-CS AF were significantly older than those without (67 (SD 1) v 61 (1) years; p<0.05, t-test). In cells from patients with post-CS AF, the action potential duration at 50 and 90% repolarisation and the ERP were 16 (3), 216 (12) and 217 (10) ms (n = 46 cells, 20 patients), respectively. The amplitude of the L-type Ca2+ current, and of inward rectifier, transient outward and sustained outward K+ currents, was −5.1 (0.4), −3.6 (0.5), 11.8 (1.8) and 6.2 (1.2) pA/pF (n = 5–88 cells, 4–28 patients), respectively. None of these values were significantly different in cells from patients without post-CS AF (p>0.05 for each, n = 14–248 cells, 8–77 patients). Neither age-matching of patients with and without post-CS AF, exclusion of patients from whom post-CS beta-blocker therapy was withdrawn, nor sub-analysis by pre-CS beta-blockade, revealed any significant differences in atrial cell electrophysiology between patients with and without post-CS AF. Pre-CS beta-blockade (⩾7 days) significantly prolonged the ERP in cells from patients either with or without post-CS AF, and to a similar extent in each patient group: by 25 and 20%, respectively (p<0.05 for each; n = 12–113 cells, 6–40 patients).
Conclusion: Pre-operative human atrial cell ion current and action potential characteristics are not predictive of post-operative AF, whether or not adjusted for the influence of patient age, post-operative beta-blocker withdrawal or pre-operative beta-blocker use. Beta-blockade prolongs pre-operative atrial action potentials similarly in patients who do and who do not develop post-operative AF.
136 ATRIAL FIBRILLATION-INDUCED CONNEXIN 43 REDISTRIBUTION IN ATRIA OF THE GOAT
P. Dhillon1, R. Kaba1, R. Chowdhury1, M. C. Hall2, S. Kirubakaran2, C. J. Garratt2, N. S. Peters1.1Imperial College London, UK; 2Manchester Heart Centre, Manchester, UK
Introduction: Atrial fibrillation (AF) has a tendency to become more persistent with time. Altered atrial gap junction distribution and connexin (Cx) expression may be involved in the pathogenesis of sustained AF. Changes in the heterogeneity and quantity of Cx40 have been shown to occur soon after the induction of AF in the goat. Changes in Cx43 are less well described. This study examined the pattern of Cx43 distribution in a pacing induced goat AF model.
Methods and Results: Five adult female goats were maintained in AF for repetitive one month periods by programmed right atrial burst pacing, for 2 seconds at 64 Hz, on detection of sinus rhythm (SR). Between periods of AF goats were DC cardioverted to SR and their AERP, at a drive cycle length of 400 ms, was allowed to gradually return to baseline before the induction of a further month of AF. The mean duration of SR between all periods of AF for all paced goats was 4.2+ (SD 1.1) days. Sections from 5 atrial regions (right and left atrial free walls and appendages, and the posterior intravenous region of the left atrium) for each AF goat and two SR controls were immunolabelled for Cx43. A semi-quantitative scoring system, from 1 (least) to 5 (greatest), was used to assess the extent of Cx43 lateralisation. Scoring was performed under blinded conditions. There was a significant difference in scores between SR and all AF goats: 1.8 (1.23) v 3.1 (1.4), p = 0.018. Furthermore, there was a difference in scores for one month of AF and greater than one month: 1.6 (1.3) v 3.5 (1.22), p = 0.025.
Conclusion: AF is associated with atrial Cx43 redistribution in a burst pacing model in the goat, and the degree of redistribution appears to correlate with the duration of induced AF.
137 TESTOSTERONE INHIBITS EXTRACELLULAR CALCIUM ENTRY VIA VOLTAGE-GATED CALCIUM CHANNELS IN A7R5 VASCULAR SMOOTH MUSCLE CELLS AT PHYSIOLOGICAL CONCENTRATIONS
J. Hall, R. D. Jones, P. Kang, T. H. Jones, C. Peers, K. S. Channer.Division of Genomic Medicine, University of Sheffield, UK, Department of Cardiology, NHS Trust, Sheffield, UK
Testosterone (T) is a coronary vasodilator and increases ischaemic threshold in men with angina. We have demonstrated that T inhibits the pore forming α1c subunit of the cardiovascular L-type calcium channel transfected into HEK293 cells. In this study we investigated the effect of T on potassium (K+)-stimulated extracellular calcium entry in A7r5 vascular smooth muscle cells (VSMCs). A7r5 VSMCs were grown on coverslips (n = 78) in 12-well plates in DMEM containing 10% foetal bovine serum. Cells (n = 430) were then incubated in DMEM containing the calcium fluorescence probe Fura2-AM (4 μM) for 40 min, at 37degC. Fragments of coverslip were then placed in a perfusion chamber and changes in calcium were indicated from the fluorescence emitted at 510 nm due to alternative excitation at 340 and 380 nm, after a 2 min incubation in the presence of T, the L-type calcium channel blocker nifedipine (N), the T-type calcium channel blocker pimozide (P) or ethanol vehicle (0.1%), or in calcium free buffer. 50 mM High K+ induced a change in cellular fluorescence of 0.12(0.02) ratio units. Subsequent recordings are expressed as a percentage of this high K+ response. Results expressed as percentages (S.E). Compared to ethanol (0.1%), 2-min incubation with T (0.1, 1, 3, 10, 30, 100 nM) caused a concentration-dependent inhibition of this response; 94.2 (7.4), 98.3 (4.9), 98.4 (5.1), 67.6 (4.0 (p<0.01), 51.5 (5.8), 36.7 (4.0), 40.9 (2.6) (all p<0.001 respectively). IC50 = 3.1 nM. Incubation with N (5 μM) also caused similar inhibition of this response; 46.7 (4.1) (p<0.001), as did P (1 μM) 31.3 (4.4) (p<0.001) and calcium free buffer almost abolished the response 6.5 (1.3) (p<0.001), as did co-incubation with N (5 μM) and P (1 μM) 12.3 (1.2) (p<0.001). Co-incubation with T (10 nM) and N (5 μM) showed no extra inhibition; 44.1 (6.8) (p<0.001) compared to T or N alone.
Conclusion: This study demonstrates that physiological concentrations of T inhibit extracellular calcium entry via L-type voltage-gated calcium channels in VSMC’s. This effect was similar to that of N. This provides further evidence that T is an endogenous calcium channel blocker, a mechanism likely to underlie its vasodilatory action.
138 TGFBETA TYPEII RECEPTOR INTERACTS WITH TGFBETA ACTIVATED KINASE (TAK1): IMPLICATIONS FOR CONTROLLING CARDIAC HYPERTROPHY
S. J. Watkins, L. Jonker, H. M. Arthur.Institute of Human Genetics, University of Newcastle Upon Tyne, UK
TGFbeta-activated Kinase 1 (TAK1) is a MAP kinase involved in numerous signalling pathways and is strongly implicated in cardiac hypertrophy and heart failure. Transforming growth factor beta (TGFbeta) is also associated with hypertension and heart disease and evidence suggests that TGFbeta1 and TAK1 act together in a cardiac stress signalling pathway. Canonical TGFbeta signalling is mediated through Smad transcription factors but TGFbeta can also rapidly activate TAK1 in addition to the Smad signalling cascade. The activation of the Smad cascade is relatively well characterised, but little is known about how TAK1 is activated in response to TGF binding by the TGFbeta receptors. We hypothesised there might be a direct link between TAK1 and the TGFbeta receptors. We used a combination of in-vitro binding assays and co-immunoprecipitation (IP) experiments to investigate whether TAK1 interacted with the type II or type I TGFbeta receptors and interactions between endogenous proteins were tested in C2C12 cells. We found that TAK1 bound directly to the type II TGFbeta receptor (TBRII) in an in vitro binding assay and co-immunoprecipitated specifically with TBRII in both exogenous and endogenous cell systems. Immunofluorescence confirmed that TAK1 and TBRII proteins co-localized when expressed in Cos7 cells. Kinases assays confirmed the importance of this interaction for regulating TAK1 activity. This novel and specific interaction between TAK1 and TBRII directly links TAK1 to the TGFbeta signalling cascade and may be critical in the early signalling events leading to cardiac hypertrophy and heart failure.
Conclusion: We describe a novel and specific interaction between TAK1 and TBRII, which demonstrates how TGFbeta-induced activation of TAK1 occurs and directly links TAK1 to the TGFbeta signalling cascade. This work has identified a potentially critical molecular mechanism in the initiation of cardiac hypertrophy.
139 A MYOCARDIAL Nox2 CONTAINING NAD(P)H OXIDASE CONTRIBUTES TO OXIDATIVE STRESS IN HUMAN ATRIAL FIBRILLATION
Y. M. Kim, Y. H. Zhang, T. J. Guzik, M. H. Zhang, H. Kattach, C. Ratnatunga, R. Pillai, K. M. Channon, B. Casadei.University Department of Cardiovascular Medicine, John Radcliffe Hospital, Oxford, UK
Human atrial fibrillation (AF) has been associated with increased atrial oxidative stress. In animal models, scavenging of reactive oxygen species prevents atrial remodelling induced by rapid pacing, suggesting that oxidative stress may play an important role in the pathophysiology of AF. Increasing evidence indicates that NAD(P)H oxidase may play an important role in the myocardial response to stress or injury; however, whether this enzyme contributes to atrial oxidative stress in AF remains to be elucidated.
Methods and Results: Sources of superoxide production were investigated (using inhibitors and substrates of a range of oxidases, RT-PCR, immunocytochemistry, immunoblotting and oxidative fluorescent microtopography) in tissue homogenates and in isolated atrial myocytes from the right atrial appendage (RAA) of patients undergoing myocardial revascularization and/or valve surgery (n = 15 in AF and n = 39 in sinus rhythm, SR). A membrane-bound gp91phox containing NAD(P)H oxidase in atrial myocytes was the main source of atrial superoxide production (lucigenin 5 μM, cytochrome C and L-012) both in SR and in AF. NADPH-stimulated superoxide release from RAA homogenates was significantly increased in patients with AF in the absence of changes in mRNA expression of the p22phox and gp91phox subunits of the NAD(P)H oxidase. In contrast with findings in SR patients, we observed that nitric oxide synthases (NOS) contributed significantly to atrial superoxide production in fibrillating atria, suggesting that increased oxidative stress in AF may lead to NOS “uncoupling” with potentially important implications on myocardial function and thrombogenesis
Conclusion: These findings indicate that a myocardial NAD(P)H oxidase and to a lesser extent dysfunctional NOS contribute significantly to superoxide production in the fibrillating human atrial myocardium and may play an important role in the atrial oxidative injury and electrophysiological remodelling observed in patients with AF
140 FoxO TRANSCRIPTION FACTOR EXPRESSIONS AND ACTIVITY ARE REGULATED DURING THE DEVELOPMENT OF CARDIOMYOCYTE HYPERTROPHY
K. A. Bicknell, G. Brooks.School of Pharmacy, The University of Reading, Reading, Berkshire, UK
The induction of hypertrophy in cardiomyocytes involves a partial reactivation of the cell cycle machinery, coupled with a transient decrease in the expressions of negative regulators of cell cycle progression e.g. p21 and p27 such that cardiomyocytes progress through the G1-S phase transition. We hypothesised that molecules that regulate G1 or S phase progression might represent molecular targets for the abrogation of detrimental hypertrophic growth. The FoxO subclass of forkhead transcription factors, FoxO1, 3 and 4, control cell cycle entry, maintaining a G1 phase cell cycle arrest that is mediated, at least in part, by increased mRNA and protein expression of p27. Inactivation of FoxO transcription factors, via phosphorylation events mediated by PI3K/Akt, leads to nuclear exclusion of FoxO proteins and alleviation of G1 phase arrest. We hypothesized that inactivation of FoxO transcription factors might be central to the molecular events that control the induction of cardiomyocyte hypertrophy. We induced rat neonatal ventricular cardiomyocytes to undergo hypertrophy with 20% serum or 100 μM phenylephrine (PE) for 1–24 hours. We investigated FoxO DNA binding by electromobility shift assay and FoxO1, 3 and 4 mRNA expressions using real time quantitative PCR. Consistent with a reactivation of cell cycle in hypertrophic myocytes, FoxO DNA binding decreased rapidly upon the induction of hypertrophy with serum or PE although levels of FoxO binding recovered to those of serum-free controls within 4 hours of hypertrophic stimulation. Interestingly, expressions of FoxO1, FoxO3 and FoxO4 were regulated differentially during the induction of cardiomyocyte hypertrophy. Following induction of hypertrophy, FoxO1 and FoxO4 mRNA expressions peaked between 6–10 hours and 1–3 hours, respectively, whereas, FoxO3 mRNA expression was significantly decreased 1–3 hours post-stimulation.
Conclusion: A greater understanding of the mechanisms that control cardiac hypertrophy will aid the design of therapies aimed at preventing detrimental hypertrophic growth. This study demonstrates that FoxO inactivation is an early event in cardiomyocyte hypertrophy and identifies FoxO family members as potential molecular targets for the prevention of detrimental hypertrophic growth.
141 THE TUMOUR SUPPRESSOR RASSF1A ATTENUATES CARDIOMYOCYTE HYPERTROPHY IN RESPONSE TO PHENYLEPHRINE
A. Pickard, M. H. Buch, S. Gillies, A. L. Armesilla, L. Neyes.Division of Cardiology, University of Manchester, Manchester, UK
Left ventricle hypertrophy is a major risk factor for heart failure. Pharmaceutical interventions of heart failure reduce left ventricle hypertrophy and thus halt the progression to heart failure. Several studies have shown that the small GTP-binding protein Ras plays a major role in the development of cardiac hypertrophy in animal models and patients with hypertrophic cardiomyopathy. Activated Ras exerts its function through various effector proteins. Ras-mediated activation of the Raf-MEK-ERK pathway has been extensively reported to induce proliferation and cell survival in several cell types including cardiomyocytes. Recently a novel Ras-effector protein, RASSF1A (Ras-Association Factor 1 isoform A) has been linked to Ras-mediated apoptosis in tissue culture cell lines, RASSF1A is expressed strongly in the heart, however, its function is totally unknown. To investigate the physiological function of RASSF1A in cardiac cells we have generated an adenovirus encoding human RASSF1A. Infection of rat neonatal cardiomyocytes with RASSF1A attenuated hypertrophic growth (measured by cell size and total protein content) in response to phenylephrine. Ras-mediated activation of the ERK pathway has been shown in cardiac hypertrophy, ectopic expression of RASSF1A significantly reduced the activation of ERK1/2 by phenylephrine by 25% and 50% respectively (p = <0.05). Further ectopic expression of RASSF1A did not affect cell viability or induce apoptosis.
Conclusion: These results demonstrate a role for RASSF1A as a negative regulator of agonist mediated cardiac hypertrophy, without altering the viability of cardiomyocytes.
142 OVER-EXPRESSION OF MYOCYTE STRESS 1 PROTEIN IN VITRO SWITCHES ON THE FETAL GENE PROGRAMME AND ANTI-APOPTOTIC PATHWAYS
N. W. Chong, A. L. Koekemoer, N. J. Samani.Cardiology Group, Department of Cardiovascular Sciences, Glenfield General Hospital, University of Leicester, UK
Left ventricular hypertrophy (LVH) is an adaptive response that compensates for increased workload, stress or injury, by normalising wall stress and preserving cardiac contractile function. While initially a compensatory response, sustained cardiac hypertrophy is associated with decompensation, dilated cardiomyopathy and overt heart failure. LVH is an important predisposing risk factor for cardiac morbidity and death. Multiple intracellular signalling pathways have been shown to regulate the hypertrophy of cardiomyocytes, although the molecular controllers that sense pressure overload and initiate cardiac hypertrophy are still unclear. We have identified and characterised a novel gene, designated myocyte stress 1 (ms1), which is upregulated within 1 hour in the left ventricle following aortic banding in the rat, suggesting an important role in the early signalling leading to pressure-induced LVH. ms1 also plays a role in embryogenesis and is transiently upregulated during ischemia-reperfusion (I/R) in vitro. To identify putative target genes and downstream pathways to ms1, we have transiently over-expressed a cMyc-MS1 fusion protein into a heart-derived rat cell line, H9c2, and examined altered gene expression. Western blot analysis (using ms1 and c-myc antibodies) confirmed MS1 protein over-expression (about 10-fold) in H9c2 and NIH3T3 cells, compared to the empty expression vector control (n = 3). RT-PCR analysis indicated an alteration of contractile and fetal encoded genes, with up-regulation of cardiac α-actin (2.5-fold) and brain natriuretic peptide (3.5-fold). Genes that are associated with hypertrophy were also increased such as calcineurin (2-fold). Interestingly, the expression of the apoptosis repressor arc was also increased (2.5-fold): arc is highly expressed in heart and skeletal muscle, and has been demonstrated to protect the heart against I/R injury.
Conclusion: The present findings suggest that MS1 is a novel upstream initiator/regulator of the fetal gene programme and apoptotic pathways in adult cardiomyocytes. Elucidation of the precise functions of this signalling molecule may provide important insights into the mechanisms underlying several cardiac disorders and their inter-relationship.
143 ROLE OF THE PMCA-SYNTROPHIN-NNOS COMPLEX IN CARDIOMYOPATHY
F. McIntyre, C. L. Hagarty, J. C. Williams, L. Neyses.Division of Cardiology, University of Manchester, Manchester, UK
Cardiomyopathies are strongly associated with muscular dystrophies, a group of disorders caused by mutations in the gene encoding the membrane protein dystrophin. Syntrophin, another member of the dystrophin glycoprotein complex, is known to interact with nNOS (neuronal nitric oxide synthase), which has been shown to interact with and to be downregulated by the sarcolemmal calcium pump (PMCA). We have shown, via a bacterial-2-hybrid screen, that syntrophin also interacts with PMCA. A ternary complex of interaction between PMCA, syntrophin and nNOS is therefore proposed in the heart. Co-localisation of syntrophin and PMCA was shown by immunoflourescent imaging in HEK293 cells, a mammalian cell line, which were overexpressed with syntrophin and PMCA. Staining of endogenous PMCA and syntrophin in rat neonatal and adult cardiomyocytes demonstrated this co-localisation in cardiomyocytes. An interaction between these three proteins was shown by immunoprecipitation of syntrophin, PMCA, and nNOS. When each protein was pulled down, western blots were then used to measure the protein levels of the other members of the complex. Syntrophin, PMCA, and nNOS could all be detected when another member of the complex was immunoprecipitated. The functionality of the proposed complex was examined by transfection in HEK293 cells. nNOS is becoming increasingly apparent in the control of cardiac function. Therefore, the activity of nNOS was measured by cGMP expression. In the presence of nNOS alone maximal cGMP expression was observed, which was reduced 54% in the presence of syntrophin and 63% in the presence of PMCA4b. When both syntrophin and PMCA4b were expressed in the presence of nNOS the inhibition observed was further increased by 85%. This demonstrates that both syntrophin and PMCA downregulate nNOS, and that this downregulation is augmented when both PMCA and syntrophin are present.
Conclusion: In conclusion these data link PMCA and nNOS to the dystrophin complex via direct interaction with syntrophin. nNOS has been shown to be mislocated in mdx mice, the mouse model of dystrophin deficiency. Therefore, the disruption of this complex, or the regulation of this complex, may have a possible role in the increased susceptibility to cardiomyopathy in muscular dystrophy patients.
144 MULTIMARKER APPROACH TO RISK STRATIFICATION IN ‘NEW’ DEFINITION MYOCARDIAL INFARCTION
N. Kilcullen, R. Das, C. Morrell, M. B. Robinson, J. H. Barth, A. S. Hall.Institute for Cardiovascular Research, G Floor, Jubilee Building, Leeds General Infirmary, UK
Background: Matrix metalloproteinase-2 (MMP-2) is co-localised with troponin I (TnI) within the thin filaments of cardiac myocytes and it has been shown, in vitro, to degrade TnI. Also it has been implicated in the causation of plaque rupture.
Objective: To determine if MMP-2 is a useful prognostic marker, in addition to TnI, in patients presenting with ‘new definition’ myocardial infarction(MI).
Methods: Over a 6 month period, 1,635 patients with ‘new definition’ myocardial infarction were recruited from 11 adjacent hospitals. MMP-2 and TnI were measured on first day samples using the R&D Systems ‘Quantikine’ Immunoassay and the automated ACCESS 2 analyser (Beckman Coulter Ltd) respectively.
Results: MMP-2 and TnI both had a non-Gaussian distribution with median values of 266 ng/mL (93–1766) and 1.43 ng/mL (0.01–101.0) respectively. Cut-off values for normality were set at 302 ng/mL for MMP-2 and 0.06 ng/mL for TnI. Concentrations of both markers were deemed positive if above the cut-off and negative if below. Figure 1 shows mortality 6 months post MI according to MMP-2 and TnI analysed from day one samples. Patients with elevated TnI and MMP-2 were 5 times more likely to have a poor outcome compared with those who had low concentrations of both markers.

Abstract 144
Conclusion: Our results indicate that simultaneous assessment of TnI and MMP-2 provides additional prognostic information in patients presenting with ‘new’ definition myocardial infarction.
145 CHOLESTEROL CONTENT OF ERYTHROCYTE MEMBRANES MAY CONTRIBUTE TO THE DEVELOPMENT OF ACUTE CORONARY SYNDROME. A NEW PARADIGM REGARDING CORONARY ARTERY DISEASE INSTABILITY?
D. Tziakas, G. Chalikias, C. Romero, A. Theodosis-Georgilas, P. Masci, D. Holt, D. Hatseras, J. C. Kaski.Cardiology Dpt, Democritus Univ Thrace, Greece Cardiological Sciences Dpt and Analytical Unit, St George’s Hospital, London, UK
Introduction: Plaque rupture with superimposed thrombosis is the main cause of acute coronary syndromes (ACS). Vulnerability to rupture depends partly on the volume of the necrotic lipid core. Studies have shown that erythrocytes are present within necrotic cores of ruptured coronary atherosclerotic plaques. It has been suggested that the cholesterol contained in erythrocyte membranes contributes to lipid core growth. We sought to investigate whether cholesterol content differs in erythrocyte membranes of patients presenting with an ACS compared to patients with stable angina (SA). Material and methods We assessed 34 SA patients (27 men, 62 (SD 13) years) and 27 ACS patients (19 men, 65 (13) years). Total cholesterol content in erythrocyte membranes (TCEM) was measured on erythrocyte membrane ghosts using an enzymatic assay, while protein content was measured by the Bradford method. TCEM differences between the two study groups were assessed using the ANCOVA method, after adjusting for all the variables that could affect TCEM levels.
Results: TCEM content was higher (p = 0.016) in patients presenting with ACS (210.85 ìg/mg, 95%CI 176,18–245.51) compared to patients with stable angina (131.82 ìg/mg, 95%CI 116.49–147.15). Plasma total cholesterol levels were not associated with TCEM levels (p = 0.598)
Conclusion: This study shows for the first time in patients that TCEM differs significantly between patients with ACS and patients with stable angina. Thus endorsing results of previous histopathological studies that suggested a role of TCEM in plaque growth and vulnerability. Larger studies are required to establish the clinical and pathogenic significance of our preliminary results.
146 BNP DETECTS SILENT ISCHAEMIA ON EXERCISE TESTING IN TYPE II DIABETIC PATIENTS
J. I. Davies, B. S. Rana, M. M. Band, S. Pringle, A. D. Morris, A. D. Struthers.Division of Medicine and Therapeutics University of Dundee Ninewells Hospital, Dundee, UK
B-Type Natriuretic Peptide (BNP) predicts future cardiovascular events in patients with normal systolic function. This may be because BNP reflects coronary artery disease. This is known to be the case in symptomatic angina patients, but it is not known whether BNP detects ischaemia in asymptomatic patients. Type II diabetic patients are at high risk of unexpected cardiac events; hence we aimed to see if BNP detects silent ischaemia in these subjects. 145 type II diabetic patients with EF⩾40% and no history or ECG findings of heart disease underwent BNP sampling followed by a full Bruce protocol ETT. ETT was graded either as positive or negative on standard criteria: i.e.: the presence of ⩾1 mm horizontal or downsloping ST segment depression measured at 0.08 seconds after the J point, and by use of the Duke score dichotomised into positive or negative values using 0 as a cut off. BNP was greater in those with an abnormal compared to normal ETT (79.9 (118) pg/ml v 28.5 (23.2) pg/ml, p = 0.008) and was an independent predictor of a positive ETT in univariate analysis (p = 0.006). Of the other cardiovascular risk factors only BNP and age remained independent predictors of an abnormal ETT result in a multivariate analysis, p = 0.002 and 0.03 respectively. The area under the ROC for BNP detecting a positive ETT was 0.76, p = 0.001. In univariate analysis BNP was also significantly predictive of a positive duke score (p = 0.04). When the other cardiovascular risk factors were put into a multivariate model BNP was the only predictor of a positive duke score (p = 0.02).
Conclusion: BNP detects silent ischaemia in type II diabetic patients as assessed by either standard ETT criteria or by dichotomising the Duke score. As diabetic patients are at high risk of unexpected cardiac events and death BNP may become a useful screening test to decide who goes on for more detailed investigations and treatment.
147 H-FABP: A STRONG PREDICTOR OF MORTALITY AFTER ‘NEW’ DEFINITION MYOCARDIAL INFARCTION
N. Kilcullen, R. Das, C. Morrell, M. B. Robinson, J. H. Barth, A. S. Hall.Institute for Cardiovascular Research, G floor, Jubilee Building, Leeds General Infirmary, UK
Background: Heart-type fatty acid binding protein (H-FABP) is a low molecular weight protein that is rapidly released from the cytosol following myocardial ischaemia.
Objective: To determine if H-FABP is a useful prognostic marker in patients presenting with ‘new definition’ myocardial infarction.
Methods: Over a 6 month period, 450 patients with ‘new definition’ myocardial infarction were recruited from 2 adjacent hospitals. Patients were identified from coronary care registers and biochemistry records of cardiac enzyme assay requests. H-FABP was analysed in first day samples using a two-step direct sandwich ELISA using two distinct mouse anti-human H-FABP monoclonal antibodies available from Dainippon Pharmaceutical Ltd.
Results: H-FABP had a non-Gaussian distribution with a median value of 9.0 ng/mL (range 1.9–944.4). At 450 days, 83 patients had died. The median H-FABP in this group was 21.9 ng/mL (3.1–447.0) as compared to a median value of 7.9 ng/mL (1.9–944.4) for the remaining 367 patients who survived (HR 4.0; 95% CI 1.9 to 8.5; p<0.001). Figure 1 depicts Cox regression survival curves adjusted for the age of the patients for two groups based on a cutoff value for normality of 6.2 ng/mL as recommended by the manufacturer.

Abstract 147
Conclusion: Our results indicate that high levels of H-FABP are associated with a poorer outcome following ‘new’ definition myocardial infarction.
148 CLINICAL BENEFITS OF LOW LDL TARGETS IN ELDERLY PATIENTS WITH CORONARY DISEASE: AN ANALYSIS FROM PROVE IT-TIMI-22
K. K. Ray, C. P. Cannon, A. Kirtane, R. Cairns, S. Murphy, E. Braunwald, C. M. Gibson.Brigham and Women’s Hospital/Harvard Medical School, Boston, USA
Background: Elderly patients are at high risk of cardiovascular events and show benefit from statin therapy (PROSPER study). It is however unclear whether elderly patients will benefit from specific LDL guidelines.
Methods: In PROVE IT-TIMI 22, 3784 patients free from death, myocardial infarction (MI) or unstable angina (UA) at 30 days were evaluated. LDL was measured at 30 days as per the study protocol. The benefits of on treatment LDL<70 mg/dl (<1.8 mMol/L) (NCEP III) at 30 days were compared in patients <70 years (n = 3154) and ⩾70 years (n = 634) on the subsequent combined clinical endpoints of death, (MI), UA.
Results: Overall analyses from PROVE IT-TIMI 22 suggest that patients ⩾70 years randomized to intensive statin therapy may derive clinical benefit for the combined endpoint HR 0.8 (CI 0.58,1.11), similar to those seen in patients <70 years, HR 0.79 (CI 0.65,0.97). In patients ⩾70 years, an on treatment LDL of <1.8 mMol/L at 30 days after an ACS was associated with an 8% absolute risk reduction (13.5% v 21.5%), compared with patients who failed to achieve this target (HR 0.60, CI 0.41, 0.87, p = 0.008). In patients <70 y age the comparable absolute risk reduction was 2.3% (8.1% v 10.4%) in those who achieved an LDL <1.8 mMol/L(HR 0.74, CI 0.59, 0.94, p = 0.01).
Conclusion: The new NCEP targets are applicable to older patients with ACS ⩾70 years of age who may show increased benefit from these LDL targets. It remains to be seen whether such targets are adopted in our increasily elderly population.

Abstract 148
149 STRESS INDUCED QT PROLONGATION DOES NOT PREDICT ISCHAEMIA IN PATIENTS WITH STABLE CORONARY ARTERY DISEASE
P. Velavan1, K. Y. K. Wong2, D. Steeples3, J. B. Ball3.1Academy of Cardiology, University of Hull, UK; 2 Royal Liverpool University Hospital, UK; 3Whiston Hospital, Liverpool, UK
Background: Ischaemia is a recognized cause of prolongation of corrected QT (QTc) interval in patients with acute coronary syndrome. Small studies have suggested that stress induced QTc prolongation may be a marker of ischaemia. QT peak (QTp) prolongation has been shown to predict left ventricular hypertrophy but it is not known whether it predicts ischaemia.
Hypothesis: QTc and QTp are prolonged with dobutamine stress and predict inducible ischaemia on stress echocardiography, in patients with stable angina.
Methods: 102 outpatients referred to a district general hospital for stress echocardiography were recruited. Their mean (+SD) age was 57 (10) years. 55% were women. 14% had a previous history of myocardial infarction and 50% had a history of hypertension. The mean (+SD) blood pressure was 152/91 (+ 23/13) mmHg. Dobutamine stress echocardiography was performed and ECGs were recorded at rest, during peak stress and recovery. The ECGs were analyzed and QT intervals measured by a single observer, blinded to the patients’ clinical characteristics and echocardiographic results. QT peak was measured from the onset of QRS to the peak of the T wave in lead I. The intervals were corrected for heart rate using Bazett’s formula.
Results: 28% had inducible ischaemia on stress echocardiography. QTc was significantly prolonged by stress (431+31 v 459+43 ms; p<0.0001). There was no difference in QTc between patients who had inducible ischaemia and those who did not, either at rest (439+30 v 428+31 ms; p = NS) or during stress (460+56 v 459+38 ms; p = NS). QTp at rest was also similar in both groups (297+34 v 294+30 ms; p = NS). QTp was shortened by stress but there was no difference when corrected for heart rate. However, QTp at peak stress was prolonged in those with ischaemia (227+29 v 216+18 ms; p = 0.02), but when corrected for heart rate, there was no significant difference (346+48 v 334+29 ms; p = NS).
Conclusion: Stress induced QTc prolongation does not predict ischaemia in patients with stable angina. There is no clear relationship between QT peak interval and ischaemia.
150 NON-INVASIVE IMAGING OF THE CORONARY ARTERIES BY COMPUTED TOMOGRAPHY (CT) FOR EXCLUDING SIGNIFICANT CORONARY STENOSES IN PATIENTS REQUIRING AORTIC VALVE REPLACEMENT
J. G. Crilley, M. A. Kenny, L. Mitchell.Departments of Cardiology and Radiology, Freeman Hospital, Newcastle-upon-Tyne, UK
Background: It is standard practice to evaluate the coronary arteries by invasive coronary angiography (ICA) in patients with aortic valve disease who are being referred for aortic valve replacement. Image quality is often suboptimal and complications are higher. Non-invasive imaging with computerised tomography coronary angiography (CTA) now provides good image quality of the proximal/mid course of the epicardial vessels with greater safety and lower cost. We studied the value of CTA as compared with ICA in assessing the coronary arteries in this group of patients.
Methods: Twenty-three patients (61 ± 14 years) underwent both techniques. Patients had CTA performed within 4 months of ICA using multislice CT (Siemens SOMATOM VZ). Invasive coronary angiography and CTA were analysed by different observers in a blinded fashion. Coronary artery segments were defined according to the AHA classification and graded according to the presence/absence of a stenosis of ⩾70%.
Results: Computerised tomography coronary angiography could not visualise 8% of distal segments. Data are summarised in the table and presented for six pre-specified vessel segments (LMCA, prox/mid LAD, prox circumflex artery and prox/mid RCA) and grouped into individual coronary arteries. No patient with a coronary stenosis of ⩾70% that subsequently received a bypass graft was missed by CTA.
Abstract 150
Conclusion: Computerised tomography coronary angiography is sufficiently sensitive to exclude a stenosis of ⩾70% in the proximal/mid course of the three epicardial coronary arteries in patients with aortic valve disease and would therefore be an effective screening tool in this group of patients.
151 QT PEAK PROLONGATION MAY REFLECT INDUCIBLE MYOCARDIAL ISCHAEMIA
K. Y. K. Wong, S. McSwiggan, N. S. J. Kennedy, S. Y. S. Wong, R. S. MacWalter, A. D. Struthers.1Division of Medicine and Therapeutics, University of Dundee, Dundee, UK; 2Department of Nuclear Medicine, Ninewells Hospital, Dundee, UK
Introduction: Cardiac death is the most common cause of mortality in stroke survivors, yet few stroke survivors are considered for cardiac investigations even after full recovery from their stroke. Recently, it has been shown that QT peak prolongation predicts cardiac death after stroke. We have therefore tested the hypothesis that QT peak is more prolonged in stroke survivors with myocardial ischaemia.
Methods: 202 patients (122 male) who made a good recovery and were at least 1 month after a cerebrovascular event were recruited into the study. Their mean age was 66 years (SD 9.4), and mean blood pressure (BP) was 145/80 (SD 21/11) mm Hg. Technetium tetrofosmin myocardial perfusion scanning was undertaken in 134 patients who consented to the procedure and did not have contraindications such as severe asthma. Dipyridamole was used as the chemical stressor. QT peak measurements were made in lead I and were heart rate corrected using Bazett’s formula. A single observer who was blinded to the myocardial perfusion study results digitized all of the ECGs.
Results: In the 113 patients who never had a history of ischaemic heart disease or angina, 36% had abnormal dipyridamole myocardial perfusion scan. Perhaps more importantly, 27% of these patients who did not have angina had significant inducible ischaemia (Rest-Stress score >3). QTpc of lead I correlated with inducible ischaemia on dipyridamole myocardial perfusion scan (Spearman r = 0.2, two tailed p = 0.041).
Conclusion: Silent myocardial ischaemia is common in stroke survivors. QT peak prolongation predicts reversible myocardial ischaemia in stroke survivors. Future studies should assess if such a strategy of identifying reversible myocardial ischaemia in stroke survivors could result in improved cardiac outcome in this group of patients who are at high risk of cardiac death.
152 FASTING PLASMA GLUCOSE FAILS TO DETECT NEW DIABETES OR ABNORMAL GLUCOSE TOLERANCE (GT) IN PATIENTS ADMITTED WITH ACUTE MYOCARDIAL INFARCTION (MI)
K. Gangopadhyay1, J. Gane2, R. Ryder1, P. D. A. Burden1, T. Millane2.1Department of Endocrinology and Diabetes, City Hospital, Sandwell and West Birmingham NHS Trust, Birmingham, UK; 2Department of Cardiology, City Hospital, Sandwell and West Birmingham NHS Trust, Birmingham, UK
Background: A single Scandinavian study has demonstrated a high prevalence of abnormal GT in non-diabetics following acute MI, using oral glucose tolerance testing (OGTT) in preference to isolated fasting plasma glucose estimation.
Objective: A feasibility study to evaluate the prevalence of unknown abnormal GT using OGTT assessed during an in-patient admission for acute MI in an inner-city cardiac centre.
Methods: All patients entering our Cardiac Care Ward with MI (history/ECG/troponin >0.15 ng/ml and/or CKMB >30 IU/l) were eligible for this pilot study. Patients with previously diagnosed diabetes were excluded, as were patients judged “diabetic” on admission by virtue of a random plasma glucose >11.1 mmol/l. An OGTT was performed on days 3–4 using a 75 g glucose load and interpreted using World Health Organization (WHO) criteria.
Results: A total of 39 patients were screened over a 2 month period (Oct/Nov 2004). As per protocol, 17 patients were excluded (16 (41%) with known diabetes; one with high admission glucose). Of the 22 patients fitting the study entry criteria 70% were male; mean age 59 years (range 47 to 72); South Asian origin 30%. Mean admission capillary glucose was 6.2 mmol/l (range 4.6 to 8.7). Oral glucose tolerance testing was normal in only 6/20 (30%) study patients. Impaired GT was demonstrated in nine (45%) patients and in five (25%) diabetes was diagnosed. In two patients an OGTT was not completed. Overall, of the 39 patients screened, 31 (79%) were either diabetic or had impaired GT. Fasting plasma glucose was normal (<6.1 mmol/l) in all but one patient (6.6 mmol/l). Had current UK practice of using only fasting plasma glucose to assess GT been used, virtually all the abnormal glucose metabolism in these patients would have been missed.
Conclusion: Oral glucose tolerance testing identified a high prevalence (70%) of unrecognised abnormal glucose metabolism in patients with recent MI. Fasting blood sugar alone appears to be completely inadequate as an assessment tool in this high risk population.
153 ULTRASONIC STRAIN AND STRAIN RATE IMAGING: A NEW NON-INVASIVE TECHNIQUE TO IDENTIFY ACUTE REJECTION AFTER HEART TRANSPLANTATION
A. Marciniak, E. Eroglu, M. Marciniak, C. Sirbu, L. Herbots, W. Streb, W. Droogne, P. Claus, J. D. Hooge, B. Bijnens, J. Vanhaecke, G. R. Sutherland.Department of Cardiology, University Hospital Gasthuisberg, Leuven, Belgium
Background: There has been a continual search for a sensitive non-invasive technique to diagnose acute rejection in transplanted hearts. Ultrasonic strain/strain rate (S/SR) imaging could provide such a tool as it has been shown to be sensitive in detecting preclinical abnormalities in regional systolic deformation over a wide range of pathologies.
Aim: To assess S/SR prospectively in diagnosing acute rejection in heart transplant recipients (HTR).
Methods: Thirty-one HTR (10 de novo) underwent a total of 106 routine endomyocardial biopsies; standard echo data together with S/SR data was acquired within 3 hours of biopsy. To assess long axis deformation, S/SR data were acquired from the septum, left ventricular (LV) lateral wall and right ventricular free wall (RVFW). For radial deformation, LV posterior wall (LVPW) data was acquired and analysed (SPEQLE).
Results: Rejection was characterised by a regional reduction in peak S/SR and was non-uniform. Eighty-eight biopsies (group 1) had grade 0-IA rejection, and 18 biopsies (group 2) had ⩾ grade IB according to standard ISHLT criteria. For S/SR results see above table (*p < 0.05, **p < 0.001). For detecting rejection ⩾IB (based on LVPW radial deformation) strain ⩾30% had 85% sensitivity and 90% specificity; LVPW SR ⩾3.0 s−1 had 80% sensitivity and 86% specificity.
Abstract 153
Conclusion: S/SR imaging is a sensitive and specific technique in detecting ⩾IB grade of acute rejection. It can detect subtle changes in systolic function not detected by either standard echo or myocardial velocity data. It shows rejection may be non-uniform in distribution (and may not always involve the RV). It offers a new and reliable non-invasive method to detect subclinical rejection.
154 THE TRUE INCIDENCE OF PRIMARY GRAFT DYSFUNCTION LEADING TO DEATH IN HEART TRANSPLANTATION: A VALIDATED AUDIT IN 1820 PATIENTS
J. S. Ganesh, C. A. Rogers, J. van der Meulen, N. R. Banner, R. S. Bonser on behalf of the Steering groupThe UK Cardiothoracic Transplant Audit, CEU, The Royal College of Surgeons of England, London, UK
Non-validated registry data suggest that primary graft failure (PGF) is the cause of 40% of early deaths following heart transplantation. This may be an underestimate as mortality reporting may code cause of death as due to secondary organ failure phenomena. We undertook a validation audit of all deaths during the transplant admission episode to ascertain the true incidence of death due to PGF or dysfunction. From a national database between April 1995 and December 2002 we identified and reviewed the case notes of all early deaths. Primary graft failure was identified as the cause of death if patients succumbed directly or from secondary complications of graft dysfunction. Graft dysfunction was defined as cardiogenic failure necessitating inotropic support for >72 hours or use of mechanical support (IABP or VAD). Primary graft failure was excluded if there was evidence of hyperacute or acute rejection, technical failure, or another identifiable cause. If uncertainty existed, the data were reviewed by an independent committee. Of 1820 HTx, there were 248 (13.6%) early deaths. Case notes were available in 227 cases in nine transplant centres. The median age of the cohort was 51 years (IQR, 39 to 56 years), 21 recipients were < 16 years of age, and 56 (23%) were female. Primary graft failure was reported as the cause of death in 95 (38%) recipients but following validation was the cause in 156 (63%) p < 0.001. There was no difference in ischaemic time between PGF deaths (median 196, IQR 150–237 minutes) and deaths due to other causes (median 192, IQR 165–249 minutes, p = 0.9). Primary graft failure deaths occurred earlier 2.5 IQR 1–9.5 days than death from other causes (30 IQR 11–56 days) p < 0.001. Renal failure ensued in 54% (84) of PGF deaths v 35 (38%), p = 0.02).
Primary graft failure is the true cause of 63% of early deaths post-HTx and is significantly under-reported. Further studies are needed to identify risk factors and reduce the incidence of graft dysfunction.
155 HAEMOGLOBIN IS RELATED TO PROGNOSTIC FACTORS BUT IS NOT AN INDEPENDENT SURVIVAL PREDICTOR IN PATIENTS REFERRED FOR CARDIAC TRANSPLANTATION
A. B. Taegtmeyer1, A. M. Crook2, N. R. Banner1.1Transplant Unit, Harefield Hospital, Harefield, Middlesex, UK; 2Westminster Primary Care Trust, London, UK
Anaemia has been shown to be associated with functional impairment and worse prognosis in chronic heart failure (CHF). We investigated the relationship between haemoglobin (Hb) and prognosis in patients referred for possible transplantation. 235 patients (182 men) referred between 2001 and 2003 were studied. Seventy-eight (33%) had ischaemic cardiomyopathy and 18 (8%) were inotrope dependent. Anaemia was defined as Hb <13 g/dL for men and <12 g/dL for women. Outcome was death, inotrope-dependent transplant or left ventricular assist device as bridge to transplant. Correlation was assessed by Spearman’s coefficient. As peak oxygen uptake (MVO2) is a predictor of survival in CHF, data from a subgroup of 184 patients able to exercise were also analysed. The Cox proportional hazards method was used for survival analyses. Eighty-four patients were anaemic (36%). Haemoglobin was positively correlated with serum albumin (ρ = 0.44), MVO2 (ρ = 0.3), cholesterol (ρ = 0.25, n = 125), creatinine clearance (CC) (ρ = 0.2), and serum sodium (ρ = 0.18), all p < 0.01. It was negatively correlated with New York Heart Association (NYHA) class: ρ = −0.26, p = 0.0001. Renal impairment (CC < 40 mL/min) was more prevalent among anaemic (21%) than non-anaemic patients (6%), p = 0.001. In all 235 patients, 1 year event-free survival for anaemic v non-anaemic patients was 55% v 73%, p < 0.01. In the exercise subgroup, anaemia was associated with worse survival: hazard ratio (HR) 1.8, p = 0.05. Other univariate survival predictors in those who were able to exercise were MVO2, mean arterial pressure, CC, serum sodium, serum albumin, and beta blocker use (all p < 0.01), but not ejection fraction or cardiac output. Multivariate Cox analysis showed beta blocker use (HR 0.4, p = 0.001), serum albumin (HR 0.94, p = 0.002), and mean arterial pressure (0.96, p = 0.02) but not anaemia to be independent survival predictors.
Anaemia was common in this cohort. Lower Hb was associated with worse event-free survival and correlated with MVO2, NYHA class, serum albumin, and cholesterol and renal function but was not an independent survival predictor.
156 USAGE OF IMPLANTABLE DEFIBRILLATORS AND BIVENTRICULAR PACEMAKERS IN CARDIAC TRANSPLANT CANDIDATES: A SURVEY OF UK TRANSPLANT CENTRES
V. K. S. Chong, M. C. Petrie, D. T. Connelly.Scottish Cardiopulmonary Transplant Unit, Glasgow Royal Infirmary, Glasgow, UK
Introduction: Several clinical trials in recent years have highlighted the survival benefit of implantable cardioverter defibrillator (ICD) therapy in patients with heart failure and poor left ventricle (LV) systolic dysfunction. In addition, cardiac resynchronisation (CRT) with biventricular pacing can improve symptoms and quality of life in many patients with ECG and/or echo evidence of LV dyssynchrony. However, national guidelines in the UK have not yet been updated to include these new trials.
Methods: Survey by email of cardiologists/cardiac surgeons in charge of transplant programmes and electrophysiologists in charge of device implantation in all UK cardiac transplant centres.
Results: 100% response rate. The centres received a total of 446 referrals annually for consideration for cardiac transplant, and performed 140 transplants annually. Annual mortality on waiting list was estimated at between 10% and 30%. None of the centres had an agreed local protocol for ICD or CRT implantation. Thirty-three percent of centres used ICDs “often” as a bridge to transplant, 50% used them “occasionally”, and 17% “never”. Sixty-seven percent of respondents were more likely to implant ICDs in patients with ischaemic heart disease than those with idiopathic dilated cardiomyopathy. All centres would consider ICD therapy in patients who were turned down for transplantation. When considering CRT, most centres used ECG criteria alone rather than echo; the QRS width criterion used varied from 120 to 160 ms. Fifty percent of centres used exclusively CRT-ICDs in patients with drug refractory heart failure and wide QRS; the others used CRT pacemakers in 20–75% of such cases.
Conclusion: Even in candidates considered for heart transplantation, there is considerable variability in the use of ICDs and CRT devices, and no centre had an agreed protocol for either of these therapies. National and international guidelines need to be continually updated to keep pace with the evolving evidence for these technologies.
157 DONOR HEARTS WITH CORONARY ARTERY DISEASE – AN UNDER UTILISED RESOURCE IN CARDIAC TRANSPLANTATION?
P. Botha, G. Parry, L. Mitchell, J. Forty, K. White, J. H. Dark.Department of Cardio-pulmonary Transplantation, Freeman Hospital, Newcastle upon Tyne, UK
We adopted a strategy of accepting otherwise suitable donor hearts with palpable single vessel coronary artery disease (SVCAD) in January 1991. We performed concurrent coronary artery bypass grafting (CABG) at the time of transplant in these patients as donor angiography was not readily available. Long term angiographic follow up is now available and suggests that donor hearts with palpable coronary plaque may represent an under utilised resource. During the period January 1991 to November 2004, of 432 adult cardiac transplants performed at our centre, five donor hearts were found to have palpable SVCAD at procurement. In all five hearts, the disease was limited to the left anterior descending coronary artery (LAD), and left internal mammary artery (LIMA) to LAD bypass was performed at the time of transplant. Early angiography revealed no flow limiting lesions. Three of five patients developed significant LAD disease at a mean of 4.45 years (range 3.25 to 5.1). All three progressed to diffuse disease but enjoyed good long term graft survival of 5, 9, and 10 years to date with patent LIMA grafts. The remaining two patients remained free of significant disease at 4 and 8 years. Palpable coronary plaque is a poor indicator of intra-luminal disease. Although no significant stenoses were demonstrated on early angiography, three of five patients eventually developed diffuse disease. LIMA potency was poor in the remaining patients, most likely as a result of competitive flow. In the current era, otherwise acceptable hearts with palpable disease should be used, but undergo early angiography with stenting as appropriate. To date, we only have experience with hearts with single vessel palpable disease. In a 12 month period, we rejected seven otherwise acceptable hearts on the basis of palpable plaques in multiple vessels. We would now suggest that these hearts could be used with confidence if they are free of other abnormality. This could add up to 50 more organs to the national pool, an increase in activity of 30% across the UK.
We conclude that the presence of palpable coronary plaque in otherwise suitable donor hearts should not be regarded as a contra-indication to the use of the organ for transplantation. In the absence of any other abnormality, these hearts should be used, and the recipients undergo early coronary angiography with stenting of flow limiting lesions as appropriate.
158 PLASMA N-TERMINAL PRO-BRAIN NATRIURETIC PEPTIDE PREDICTS EXERCISE CAPACITY IN DEGENERATIVE MITRAL VALVE DISEASE
M. R. Yusoff, B. Keevil, N. Clayton, S. G. Ray.Wythenshawe Hospital, Southmoor Road, Manchester, UK
Functional capacity in degenerative mitral valve disease is not closely related to the severity of regurgitation. N-terminal pro-brain natriuretic peptide (NTBNP) is raised in severe mitral regurgitation but its relationship to functional capacity is unknown. To investigate whether NTBNP might be related to functional capacity, we examined the relationship between NTBNP, echocardiographic parameters, symptoms, and metabolic exercise testing in 38 patients with severe degenerative mitral regurgitation (MR). All patients had a regurgitant fraction of >50% and a mean ejection fraction of 64% (SD ± 3.4%). Seventeen patients were in New York Heart Association (NYHA) classification I, nine in NYHA II, and 12 in NYHA III. Levels of circulating NTBNP rose progressively with NYHA class; NYHA I (GM 97.1 pg/ml), NYHA II (GM169.8 pg/ml), and NYHA III (GM 451.6 pg/ml). End-systolic dimension (r = 0.46, p = 0.004) and end-diastolic sphericity index (r = 0.56, p < 0.001) correlated significantly with NTBNP levels. N-terminal pro-brain natriuretic peptide levels correlated with VO2max (r = −0.6, p < 0.001), exercise time (r = −0.52, p < 0.001), and O2 pulse (r = −0.57, p < 0.001). End-diastolic sphericity index correlated weakly with VO2max measurements (r = −0.34, p = 0.03). Of all the variables studied NTBNP and resting ejection fraction were independent predictors of VO2max (p < 0.001, p = 0.045 respectively), and NTBNP was the only predictor of exercise time (p = 0.02).
N-terminal pro-brain natriuretic peptide is associated with both symptoms and functional capacity in patients with severe degenerative MR, outperforming all echocardiographic variables. Serial measurements of NTBNP might be useful in monitoring these patients and aid in the timing of surgery.
159 EDGE-TO-EDGE REPAIR FOR BARLOW’S DISEASE: EARLY AND LATE CLINICAL AND ECHOCARDIOGRAPHIC RESULTS
G. Doukas, M. Oc, C. Alexiou, L. Hadjinikolaou, A. W. Sosnowski, T. J. Spyt.Department of Cardiac Surgery, Glenfield Hospital, University of Leicester, Leicester, UK
Objective: To define the early and late clinical and echocardiographic results obtained following the use of the edge-to-edge (E_E) repair in the setting of Barlow’s disease.
Patients and Methods: Between 1998 and 2004, 41 patients having Barlow’s disease with bileaflet prolapse had an E_E repair creating a double lumen mitral valve orifice in our unit. The patient hospital records were reviewed. Clinical and echocardiographic follow up was complete.
Results: Pre-operatively, all patients had severe mitral regurgitation (MR), 12 were in New York Heart Association (NYHA) classification class I, 15 in class II, and 14 in class III. One patient died in hospital (2.4%) and five experienced post-operative complications (12.5%). There were no late deaths. At follow up, two patients developed severe MR and underwent valve replacement, one exhibited moderate and five mild MR. Kaplan-Meier 5-year survival, freedom from re-operation and from recurrent moderate-severe MR was 97.6 ± 2.4, 94 ± 4.4, and 90.6 ± 5.1%, respectively. At latest echocardiograms (mean 35 ± 12 months) the mean left ventricular end-systolic diameter and end-diastolic diameters, and the mitral valve area decreased significantly (p = 0.0001) compared to baseline. The mean mitral valve gradient increased significantly (p = 0.001) whereas ejection fraction and fractional shortening did not change. Currently, 35 patients are in NYHA class I and five are in class II.
Conclusion: This study shows that the E_E repair is a safe technique that provides lasting restoration of mitral valve competence with measurable haemodynamic and clinical benefits. The post-repair trans-valvular gradient increases but with no clinically evident mitral stenosis. In our unit, the E_E repair is the procedure of choice for correction of MR in patients with Barlow’s disease.
160 CALCINEURIN INHIBITOR (CI) WITHDRAWAL AND REPLACEMENT WITH SIROLIMUS (SIR) IN CTR WITH RENAL DYSFUNCTION
S. Kushwaha, J. Wilson, R. Frantz, R. Rodeheffer, A. Clavell, R. Daly, C. McGregor, B. Edwards.Cardiovascular Diseases, Mayo Clinic, Rochester, MN, USA
Objectives: (1) To assess the safety and feasibility of CI withdrawal, and replacement with SIR in CTR with CI induced renal impairment. (2) To assess the effect of primary immunosuppression with sirolimus on renal function in the same population.
Methods: Stable CTR (2–7 years post transplant, n = 12) with decreased renal clearance (30–50 ml/min, iothalamate glomerular filtration rate) were selected. Following a baseline clearance, SIR was started at 1 mg per day and titrated over 2 weeks to achieve levels of 10–15 ng/ml and the dose of CI reduced to achieve half the original levels. At day 28, an echocardiogram (ECHO) and right ventricular biopsy (Bx) was performed. By day 56 the dose of CI was reduced further with an ECHO and Bx at day 70. Calcineurin inhibitor was discontinued by day 84 with repeat Bx and ECHO at days 98 and 140. Secondary immunosuppressives were unchanged, with 10 patients on azathioprine (AZA) and two on mycophenolate (MMF). Five patients received no steroids.
Results: All patients have had CI successfully discontinued. Ten patients have had ISHLT grade 0 biopsies, with one patient with a grade II (self resolving) and one patient with grade 1A, with no episodes of rejection requiring treatment. Cardiac function has remained normal. There is a significant improvement in renal clearance (ml/min): 37.2 ± 7.9, baseline; 51.5 ± 16.3, day 140, p < 0.05, with no significant change in serum creatinine. Based on the above study, an additional 47 patients with abnormal renal function or transplant coronary disease have been switched to SIR as primary immunosuppression with an improvement in renal clearance (ml/min) from 39.3 ± 13 to 48 ± 16.4, p < 0.001, and a decline in creatinine (mg/dl) from 2.1 ± 0.5 to 1.9 ± 0.5, p < 0.001.
Conclusion: This study for the first time demonstrates withdrawal of CI and replacement with SIR as primary immunosuppression in combination with AZA or MMF is safe, well tolerated, and improves renal dysfunction in CTR.
161 IS A PERICARDIAL WINDOW MORE EFFECTIVE THAN CONSERVATIVE TREATMENT IN REDUCING THE INCIDENCE OF POST-OPERATIVE ATRIAL FIBRILLATION (AF) FOLLOWING CORONARY ARTERY BYPASS GRAFTING (CABG)?
A. Momin, S. Kapetanakis, R. Deshpande, D. McCormack, J. Potts, M. Kearney, J. Desai.Cardiothoracic Department, Kings College Hospital, London, UK
Post-operative AF is common following CABG. We investigated the effectiveness of a pericardial window in reducing the incidence of AF following CABG. 108 consecutive patients undergoing CABG were prospectively studied. Study group of 50 (mean age 65.5 years, 43 male) patients had a posterior pericardial window with pleural chest drains and no mediastinal drains. The pericardial window was a 4 cm cruciate incision made parallel and posterior to the left phrenic nerve. Control group of 58 (mean age 68.4 years, 43 male) patients without a pericardial window had one anterior mediastinal chest drain and pleural drains as appropriate. All subjects underwent echocardiography by the same operator (blinded to treatment) 4 days post operatively. There was no statistical difference in the incidence of significant left ventricular dysfunction or left atrial dilatation between the two groups. In the pericardial window group, three patients (6%) had AF, compared to 12 patients in the control group (20.1%) post CABG (p = 0.03). There was no (0%) significant pericardial effusion (>1 cm) in the pericardial window group, whereas nine patients (15.5%) in the control group developed significant pericardial effusion (p = 0.004).
A posterior cruciate pericardial window allows drainage of the mediastinum without a mediastinal drain. With this approach we observed a significant reduction in early and late pericardial effusions and incidence of post operative AF following CABG.
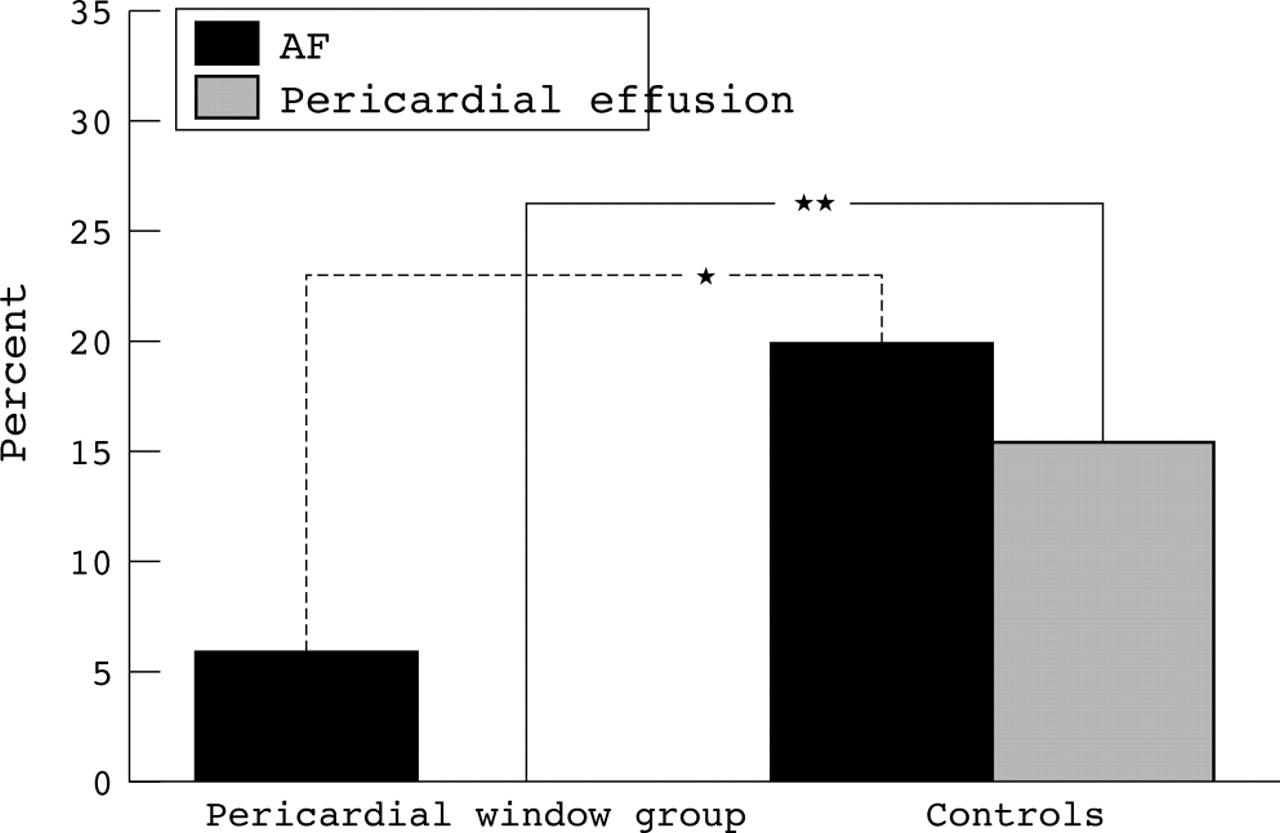
Abstract 161
162 ENDOTHELIAL TETRAHYDROBIOPTERIN (BH4) REGULATES ENOS COUPLING IN VIVO: FUNCTIONAL EFFECTS OF BH4-ENOS STOICHIOMETRY IN ENDOTHELIAL TARGETED TRANSGENIC MICE
J. K. Bendall1, N. J. Alp1, T. K. Nicoli1, K. A. Rockett1, M. Yokoyama2, S. Kawashima2, K. M. Channon1.1Department of Cardiovascular Medicine, University of Oxford, Oxford, UK; 2Kobe University School of Medicine, Japan
Endothelial dysfunction is associated with eNOS uncoupling so that superoxide is produced instead of nitric oxide (NO). This may be due to mismatch between eNOS protein levels and its cofactor BH4 although the mechanistic relationships between BH4 availability and eNOS activity remains undefined. We investigated the functional effects of BH4-eNOS stoichiometry in vivo by crossing endothelial targeted transgenic mice overexpressing either eNOS (eNOS-Tg) or GTP cyclohydrolase (GCH-Tg, in which endothelial BH4 levels are increased three fold), or overexpressing both transgenes (eNOS/GCH-Tg). eNOS protein was increased eight fold in both eNOS-Tg and eNOS/GCH-Tg mice compared with WT. However, eNOS activity, measured using arginine to citrulline conversion, was elevated only two fold in eNOS-Tg mice (p < 0.05), but by four fold in eNOS/GCH-Tg mice compared with WT (p < 0.05 v eNOS-Tg). Superoxide production, measured by both lucigenin chemiluminescence and dihydroethidine fluorescence, was increased two fold in eNOS-Tg mice compared with WT but was normalised following NOS inhibition with L-NAME, suggesting superoxide production by uncoupled eNOS. In contrast, superoxide production in eNOS/GCH-Tg mice was similar to WT and L-NAME had no effect, indicating preserved eNOS coupling. NO-mediated aortic vasorelaxations, measured in an organ bath, were paradoxically attenuated in both eNOS-Tg and eNOS/GCH-Tg mice compared with WT (p < 0.01). ACh-stimulated cGMP formation was also reduced in eNOS-Tg and eNOS/GCH-Tg mice (p < 0.05), suggesting a desensitised NO-cGMP pathway. Peroxynitrite levels, measured using luminol chemiluminescence, were elevated two fold in eNOS-Tg and eNOS/GCH-Tg mice compared with WT (p < 0.05), suggesting that redox signalling rather than NO production may mediate NO-cGMP desensitisation.
These data indicate that: (1) eNOS uncoupling is an independent consequence of a stoichiometric discordance between enzyme and BH4; and (2) chronic increases in eNOS activity may paradoxically worsen aortic relaxations due to desensitisation of the NO-cGMP pathway. Increased eNOS protein without concomitant increases in BH4 may lead to eNOS uncoupling thereby exacerbating oxidant stress.
163 INTRACORONARY DELIVERY OF A SECRETED TRANSFORMING GROWTH FACTOR-β TYPE II RECEPTOR FROM A NOVEL COLLAGEN-MEMBRANE BOUND STENT INHIBITS IN-STENT NEOINTIMAL HYPERPLASIA
C. E. Appleby, P. A. Kingston, M. Verhoeven, A. M. Heagarty.Vascular Gene Therapy Unit, Medtronic Bakken Research Center, Maastricht, Netherlands; Department of Medicine, University of Manchester, Manchester, UK
In-stent neointimal hyperplasia (NIH) is the result of excessive expression of extracellular matrix (ECM) by cells within the stented vessel segment. We hypothesised that localised inhibition of TGF-β1 (a regulator of ECM synthesis by vascular cells) in the periluminal media by stent based gene transfer would inhibit in-stent NIH and thereby reduce luminal loss after coronary stenting. Porcine coronary arteries were randomised to receive a Coverstent (a novel stent based delivery device) loaded with 1×109 iu of adenovirus expressing a secreted type II TGF-β receptor (Ad5-PREP-RIIs), β-galactosidase (Ad5-PREP-lacZ), or saline only. Angiograms were acquired pre- and post-stenting, and before vessel harvesting 28 days later. Periluminal transgene expression confined to the site of stenting was demonstrated by X-gal staining and immunohistochemistry at 72 hrs. Angiographic luminal loss at 28 days was halved in RIIs vessels (p = 0.002). Morphometric minimum luminal area in RIIs-treated arteries was 200% greater than that in control vessels (p = 0.0024). Injury score, stent area, internal elastic lamina (IEL) area, external elastic lamina (EEL) area, and total vessel area did not differ between groups. Neointimal area in the RIIs group was significantly less than that in either control group (p = 0.016).
Antagonism of TGF-β1 by stent-based Ad5-PREP-RIIs delivery reduces luminal loss post-stenting by inhibition of neointimal hyperplasia. The Coverstent provides an efficient gene delivery device to the luminal surface of coronary arteries. These findings confirm the potential of gene therapeutic antagonism of TGF-β as prophylaxis of restenosis in stented coronary arteries.

Abstract 163
164 PROTECTION AGAINST THE DEVELOPMENT OF OBESITY, INSULIN RESISTANCE, AND HYPERTENSION IN MICE BY OVEREXPRESSION OF INSULIN-LIKE GROWTH FACTOR BINDING PROTEIN-2 (IGFBP-2)
S. Wheatcroft, P. Crossey, V. Ezzat, J. Miell, A. Shah, M. Kearney.Departments of Cardiology & Medicine, Guy’s, King’s, & St. Thomas’ School of Medicine, King’s College, London, UK
Obesity and insulin resistance promote the development of type 2 diabetes, atherosclerosis, and hypertension. The cardiovascular actions of insulin and insulin-like growth factor I (IGF-I) are well described. As the activity of IGF-I is regulated by binding proteins (IGFBP) we generated transgenic mice, overexpressing IGFBP-1 and IGFBP-2, respectively, to investigate the roles of these binding proteins in metabolic and cardiovascular physiology. We previously reported that overexpression of IGFBP-1 lowers blood pressure and increases nitric oxide (NO) production. IGFBP-2 is secreted by adipocytes and inhibits the stimulatory effect of IGF-I on adipocyte hyperplasia, suggesting that it may reduce susceptibility to obesity/insulin resistance and related cardiovascular disorders. This hypothesis was studied in IGFBP-2 (TG) mice in response to aging and high fat feeding. Female TG mice were compared with wild type (WT controls (n = 6–8 per group). At 8 weeks of age, fasting glucose and insulin levels, the response to an intraperitoneal glucose tolerance test (GTT), and systolic blood pressure (SBP) were similar in TG and WT mice. At 40 weeks, a GTT provoked a lower 30 minute glucose level in TG mice than WT (10.5 ± 0.5 v 12.8 ± 0.4 mM; p < 0.05). TG mice were more insulin sensitive than WT in an insulin tolerance test. Systolic blood pressure was lower in TG mice than WT at 40 weeks (123 ± 2 v 134±2 mm Hg; p = 0.001). TG mice gained significantly less weight when fed a high fat diet for 32 weeks than WT (10 ± 2 v 17 ± 2 g; p < 0.05). Peri-gonadal and mesenteric fat depots were smaller in TG than WT animals (3.7 ± 0.8 v 13.5 ± 1.5% body mass;1.0 ± 0.04 v 2.5 ± 0.5% body mass respectively; both p = 0.01). Cross sectional fat area, measured by MRI at the level of the kidneys, was lower in TG mice than WT (40 ± 3 v 54 ± 3%; p = 0.04). Mean fat cell area was lower in TG mice than WT (2850 ± 33 μm2v 5970 ± 18 μm2; p = 0.003). Systolic blood pressure was lower in TG mice fed high fat diet than WT controls 111 ± 2 v 134 ± 3 mm Hg; p < 0.05).
These data support an important role for IGFBP-2 in protecting against the development of obesity/insulin resistance and cardiovascular sequelae in the setting of caloric excess and increasing age. The findings of this study highlight IGFBP-2 as a novel and favourable modulator of metabolic and cardiovascular homeostasis.
165 CIRCADIAN CLOCK GENES CAUSE ACTIVATION OF THE HUMAN PAI-1 GENE PROMOTER WITH 4G/5G ALLELIC PREFERENCE
N. W. Chong, D. Chan, V. Codd, N. J. Samani.Cardiology Group, Department of Cardiovascular Sciences, Glenfield General Hospital, University of Leicester, Leicester, UK
Plasminogen activator inhibitor-1 (PAI-1) is a major regulator of endogenous fibrinolysis. Reduced fibrinolytic activity due to increased PAI-1 activity is associated with risk of acute coronary events. Expression of PAI-I is regulated by the 4G/5G polymorphism in the PAI-1 promoter, with the 4G allele associated with higher PAI-levels, and in some studies with increased risk of myocardial infarction (MI). Plasma level of PAI-I also show circadian variation and this may contribute to the higher risk of coronary events in the early morning. Circadian rhythms are regulated by clock genes. In this study we investigated whether clock genes differentially interact with the two PAI-I alleles. Using a human PAI-1 (hPAI-1) promoter-reporter that included the whole of exon 1 (bp −796 to +140) we found that in transient expression assays in COS cells, co-overexpression of clock genes BMAL2 and CLOCK significantly enhanced expression from the PAI-I promoter. Furthermore, activation of the 4G hPAI-1 promoter was consistently greater than the 5G promoter (9.5 ± 0.9 fold v 5.9 ± 0.8 fold, n = 6; p = 0.008). An equal mix of 4G/5G allele reporters reduced hPAI-1 promoter activity to the level of the 5G-promoter. Addition of the negative clock factor CRY2 completely abolished the effect of BMAL2: CLOCK. Sequential site directed mutagenesis of hypoxia response elements (HREs) demonstrated that BMAL2: CLOCK activates the E-box (CACGTG) that overlaps the 4G/5G polymorphism (bp −685 to −680) but not the HRE at position −195 to −190.
These results suggest a potential novel mechanism whereby circadian clock genes can modulate the abundance of PAI-1 during the vulnerable morning period, which is dependent, at least in part, on the 4G/5G polymorphism. These findings may explain the association of the PAI 4G variant with increased risk of MI.
166 A NEW MURINE MODEL OF ARTERIAL STENTING
M. Wheatcroft1, H. Lupton2, N. Arnold1, S. Francis1, J. Gunn1.1Cardiovascular Research Unit, University of Sheffield, Sheffield, UK; 2Brivant Ltd, Galway, Ireland
Background: Animal models of arterial stenting have been limited to large and medium sized animals, such as pigs and rabbits. In contrast to these models, the mouse offers the possibility for genetic manipulation and therefore new mechanistic insights into the process of in-stent restenosis. No murine model of stenting has yet been described.
Aim: To develop a murine model of arterial stenting.
Methods: A self-expanding coil stent (2 mm× 0.7 mm) was made from nitinol wire and contained within a tubular steel introducer. Mice were anaesthetised and the carotid artery exposed. The stent was introduced via arteriotomy in the external carotid artery and deployed in the common carotid artery (diameter 0.35 mm) under direct vision. The animals were allowed to recover. Stented segments were excised, embedded in methylmethacrylate, and 10 μm sections made for histological analysis.
Results: Forty stents were tested in 39 mice, representing six versions of stent design, providing incremental improvements in deployment, vessel integrity, and animal survival to 28 days. Of the last 21 mice, stenting was successful in six, and four survived to 28 days. A mean of six sections was obtained from each stent. Staining with haematoxylin and eosin demonstrated a mature neointima (see fig).

Abstract 166
Conclusion: This is the first description of a murine model of arterial stenting. It uses what we believe to be the world’s smallest stent. A time course of vascular changes after stenting in this model is currently underway. This model may have great utility in the study of vascular injury with mechanistic insights offered from gene “knockout” and transgenic technologies.
167 SELECTIVE GENE DELETION OF THE NEURONAL NITRIC OXIDE SYNTHASE (NNOS) ACCELERATES PATHOLOGICAL LEFT VENTRICULAR REMODELLING AND FUNCTIONAL DETERIORATION AFTER MYOCARDIAL INFARCTION (MI)
D. Dawson, C. Lygate, M. H. Zhang, S. Neubauer, B. Casadei.University Department of Cardiovascular Medicine, John Radcliffe Hospital, Oxford, Oxford, UK
Over the last 10 years experimental evidence has indicated that constitutive nitric oxide (NO) production may play an important part in fine-tuning the myocardial response to stress and beta-adrenergic stimulation. It is now accepted that a myocardial nNOS regulates cardiac function. Unlike epithelial nitric oxide synthase (eNOS), nNOS expression and activity are significantly increased in the infarcted myocardium, suggesting that nNOS may play an active role in the myocardial stress response. To test this hypothesis, we compared left ventricular (LV) remodelling post-MI in nNOS knockout mice (KO) and wild type (WT) littermates by using a new and highly accurate three dimensional echocardiographic technique (1, 4, and 8 weeks post-MI) and evaluated LV pressure-volume loops at baseline and in response to dobutamine infusion (4 and 16 ng/g/minute) 8 weeks after MI or sham surgery. Sham-operated KO mice showed greater basal LV contractility (p < 0.03 for LV preload recruitable stroke work (PRSW), and ejection fraction) but an attenuated inotropic response to dobutamine (p < 0.01 for PRSW). Both basal and beta-adrenergic LV relaxation were significantly impaired in KO mice. After MI, KO mice showed a faster and more severe progression of LV dilatation when compared with WT mice with the same infarct size (p < 0.05 for both end-systolic volume (ESV) and end-diastolic volume (EDV); infarct size 39%, range 23 to 69% in both groups). Wild type mice showed a modest inotropic response to beta-adrenergic stimulation after MI. Conversely, infarcted KO mice showed a dramatic deterioration in LV contractility in response to dobutamine (p < 0.01 for PRSW v infarcted WT), which was accompanied by ESV dilatation (p < 0.05 v WT). Indices of LV pre-load or after-load and heart rate did not differ between KO and WT mice under any experimental conditions.
Neuronal nitric oxide synthase plays a significant role in preventing adverse LV remodelling and maintaining myocardial beta-adrenergic reserve after MI. Taken together, our findings suggest that upregulation of myocardial nNOS in infarcted hearts may be an important adaptive mechanism.
168 CLINICAL BENEFIT FROM CARDIAC RESYNCHRONISATION THERAPY (CRT) DEPENDS ON MYOCARDIAL VIABILITY RATHER THAN ON QRS DURATION
S. Chalil, S. Muhyaldeen, K. Khadjooi, S. Srivastava, S. Ellery, Z. R. Yousef, K. Patel, R. E. A. Smith, P. Jordan, C. Gibbs, F. Leyva.Department of Cardiology, Good Hope Hospital, Sutton Coldfield, West Midlands, UK
Background: Although the benefits of CRT are well established, they are difficult to predict from clinical, ECG, or echocardiographic parameters. Gadolinium DTPA-enhanced magnetic resonance (Gd-MR) imaging is the gold standard for the in vivo identification of myocardial scarring. This study hypothesised that the clinical benefit of CRT can be predicted from the assessment of left ventricular (LV) myocardial viability using Gd-MR.
Methods: Twenty-nine patients with heart failure due to coronary heart disease or dilated cardiomyopathy, aged 71.3 (1.8) years (mean (SEM)), in New York Heart Association (NYHA) class II (n = 1), III (n = 21), and IV (n = 7), and with a QRS of 154 (12) ms underwent a clinical assessment, including a 6 minute walk test, before and after CRT. A Gd-MR scan (1.5 T GE Signa scanner) was obtained at baseline, 10 minutes following 0.1 mmol/Kg Gd-DTPA iv, using a multiphase inversion recovery fast gradient recalled-echo (IR-FGRE) sequence. Scar volume was calculated by planimetry from short axis sections and expressed as a percent of total LV myocardial volume. Non-responders (NR) were defined as patients who died or in whom, at the most recent follow up, NYHA class and/or 6 minute walking distance had either not changed or decreased.
Results: After a follow up period of 418.0 (44.9) days, six NR were identified. Percent scar volume was 30.7 (8.9) cm3 in NR and 12.5 (2.0) cm3 in responders (R) (ANOVA, p = 0.0041). In logistic regression analyses, percent scar volume emerged as a predictor of NR (p = 0.0194), whilst LV ejection fraction, baseline QRS duration, and aetiology did not. In survivors, percent scar volume emerged as a predictor of change in walking distance from baseline to follow up (p = 0.0337).
Conclusion: Myocardial viability assessed by Gd-MR is a predictor of outcome in patients undergoing CRT. Further studies are needed to determine the role of Gd-MR in selecting patients for CRT.
169 OPTIMISATION OF ATRIOVENTRICULAR (AV) AND INTERVENTRICULAR (VV) DELAY IN BIVENTRICULAR PACING USING CONTINUOUS NON-INVASIVE MEASUREMENT OF BLOOD PRESSURE (BP)
Z. Whinnett, J. Davies, K. Willson, A. Chow, R. Foale, W. Davies, A. Hughes, D. Francis, J. Mayet.Imperial College and St. Mary’s Hospital, London, UK
Background: In principle, AV and VV delay of a biventricular pacemaker should be optimised, but current echocardiographic methods have limited reproducibility and depend on skilled personnel. We studied a new approach using continuous non-invasive BP.
Methods: Atrioventricular delay optimisation was performed on 12 patients and VV on 10 (four in common, 18 total) using non-invasive beat-to-beat BP by finger photoplethysmography (Finapres). At each delay (AV from 40 to 240 ms, VV from 40 ms to −40 ms) systolic BP was measured relative to a reference AV delay (120 ms) and VV delay (0 ms). Multiple alternations were performed and averaged to allow precise measurement of relative BP (ΔBP) for each delay: the optimum delay was defined as that yielding the maximum ΔBP.
Results: Each patient was found to have an individual optimum AV and VV delay where the ΔBP curve peaked. Bland-Altman reproducibility of optimal AV delay on separate visits (six patients) was 3 ± 8 ms. Programming AV delay 40 ms below the individual’s optimum reduced BP on average by 4.9 ± 1 mm Hg (p < 0.003); having it 40 ms above optimal decreased BP by 4.4 ± 0.7 mm Hg (p < 0.0005). A VV delay 20 ms longer or shorter than optimal caused a mean drop in ΔBP of 3 ± 0.5 mm Hg (p < 0.007).
Conclusion: Even small changes in AV or VV delay produce significant haemodynamic effects detectable by non-invasive BP measurement. The simplicity, reproducibility, and ease of this approach (and lack of patient discomfort or risk) makes it potentially useful as a clinical tool for optimisation of biventricular pacing devices.

Abstract 169
170 HOME-BASED VERSUS SUPERVISED CENTRE-BASED CARDIAC REHABILITATION IN A MULTI-ETHNIC POPULATION: 6 MONTH RESULTS OF THE BIRMINGHAM REHABILITATION UPTAKE MAXIMISATION STUDY (BRUM)
K. Jolly1, R. S. Taylor1, K. Lee2, G. Y. H. Lip2, J. W. Mant3, D. Lane2, S. M. Greenfield3, J. Raftery4, R. Lancashire1, A. Stevens1.1Public Health & Epidemiology, University of Birmingham, Birmingham, UK; 2University Department Medicine City Hospital, University of Birmingham; 3Primary Care, University of Birmingham; 4Health Services Management Centre, University of Birmingham
Background: Although meta-analyses have shown benefits of rehabilitation in heart disease populations, this evidence is predominantly based on trials of the traditional model of the supervised hospital (or centre)-based programme. The National Service Framework’s goal to expand coverage of rehabilitation to all patients with heart disease demands consideration of alternative models of service delivery, in particular home-based programmes. We report here the 6-month follow up results from the largest trial of hospital versus supervised centre-based rehabilitation to date.
Methods: 525 low/moderate risk post-myocardial infarction and revascularisation patients (mean age 61 years; 77% male, 20% ethnic minorities) referred in the 2-year period from February 2002 to four inner city hospitals serving a multi-ethnic population in the West Midlands, UK were randomly allocated to either 12 weeks of home (heart manual and nurse follow up) (n = 263) or usual hospital/community based rehabilitation. Primary outcomes were collected at 6 months in both groups and compared using intention to treat analysis, adjusting for baseline score, age, sex, and diagnosis.
Results: Primary analysis revealed no significant differences in primary outcomes between home and centre-based groups at 6 months—that is, smoking cessation 39% v 40% respectively, p = 0.9; and mean difference (MD) in exercise capacity of 14.1 m (favours hospital) (95% CI (confidence interval) 15.4 to 43.6), MD in systolic blood pressure of 0.8 mm Hg (95% CI 2.7 to 4.2), MD in diastolic blood pressure of 1.0 mm Hg (95% CI 1.1 to 3.1), MD in Hospital Anxiety and Depression Scale (HADS) anxiety of −0.2 (95% CI 0.9 to 0.5), MD in HADS depression of 0.1 (95% CI −0.5 to 0.7), and MD in total cholesterol 0.00 mmol/l (95% CI 0.2 to 0.2). In a secondary analysis, statistically significant improvements in both home and centre-based groups were seen for smoking cessation, HADS anxiety, and total cholesterol levels at 6 months compared to baseline.
Conclusion: We have shown that home-based and supervised centre-based cardiac rehabilitation programmes equally improve outcomes at 6 months in a low risk cardiac population. These findings support the policy of increased provision of home-based programmes for selected post myocardial infarction and revascularisation patients.
171 IMPACT OF PRIMARY ANGIOPLASTY (PPCI) PROGRAMME ON THE MANAGEMENT OF PATIENTS PRESENTING WITH ST-ELEVATION MYOCARDIAL INFARCTION (STEMI) IN A NORTH WEST LONDON BOROUGH
H. Recica, R. Grocott-Mason, M. Teoh, S. W. Dubrey, M. Al-Obaidi, M. Dalby, M. Al-Bustami, A. Mitchell, M. Mason, C. Ilsley.Hillingdon Hospital, Uxbridge, Middlesex, UK; Harefield Hospital, Harefield, Middlesex, UK
Primary angioplasty is recommended by the European Society of Cardiology (ESC) as the treatment of choice for acute STEMI. Since March 2004 all patients with suspected STEMI are either taken directly to the local tertiary cardiac centre catheter laboratory by the initial ambulance or transferred from the district general hospital (DGH) accident and emergency (A&E) department. The service is available 24 hours, every day for all patients with suspected STEMI, unless too unstable or medically inappropriate. We compared the impact of this strategy on the management of all patients presenting with suspected STEMI, within the DGH catchment area (population ∼270 000) between March and November 2003 and the same months in 2004. The number of suspected STEMI were similar (113 v 127). All presented to the DGH A&E in 2003, whereas 56 were taken directly by ambulance to the cardiac centre in 2004. In 2003 only one patient had PPCI and 99 had thrombolysis, whereas in 2004 only 19 were thrombolysed and 98 were referred directly to the catheter laboratory: 93/98 had angiography, 71 had percutaneous coronary intervention (PCI), two were referred for coronary artery bypass surgery (CABG), and two had surgery for aortic dissection. Mean time from door-to-PCI was 31 ± 11 minutes in patients brought directly to the cardiac centre. Mean time from arrival at DGH A&E to PCI for transferred patients has improved from 113 ± 36 minutes in the first 3 months to 90.3 ± 17 minutes in the last 3 months. In 2003, 73/113 (65%) patients with STEMI underwent coronary angiography, 28 during initial hospitalisation, and 45 after discharge (mean delay 171 days post-STEMI), of whom 17 had elective PCI (mean delay 276 days post-STEMI) and 11 CABG. Overall, in-hospital mortality for STEMI was 13/113 (11.5%) in 2003 compared to 11/125 (8.8%) in 2004. Four patients referred for PPCI died prior to angiography; in-hospital mortality for patients who had PPCI was 2.8% (2/71).
A 24 hour PPCI service is achievable in the UK. Among the benefits are proven better short term outcomes, reduced initial hospitalisation, and eradication of long waits for out-patient angiography and revascularisation. In-hospital mortality after PPCI is very low. Direct admission to a specialist centre offers the best outcome, with a significantly shorter time to revascularisation.
172 RISK FACTORS FOR SUDDEN DEATH IN INFANTS HAVING UNDERGONE THE NORWOOD OPERATION FOR HYPOPLASTIC LEFT HEART SYNDROME (HLHS)
C. Thompson, E. Kazobah, D. Anderson, C. Austin, R. Tulloh.Department of Congenital Heart Disease, Guy’s and St. Thomas’ Hospitals Foundation NHS Trust, London, UK
Background: Although operative mortality for neonates undergoing the Norwood 1 procedure (N1) for HLHS continues to improve, late mortality is still high. Suggested causes might be pulmonary vascular or myocardial perfusion abnormalities.
Aim: The aim of this study is to identify late risk factors after initially successful N1.
Methods: Patients dying suddenly >30 days after N1 between July 1995 and September 2004 were included in the study. Demographic, anatomic, ECG, echo, physiologic, and surgical parameters were compared in a 1:2 ratio with that from a matched population of controls who survived. Matching criteria were size of aorta within 1 mm, era of operation within 5 years, and birth weight within 0.5 Kg.
Results: 143 neonates underwent N1 and 103 survived more than 30 days. There were 11 late sudden deaths at median age 91 days (36–622) and at median 56 days after discharge. There was no evidence of arrhythmia but death was often after a non-specific illness. Twenty-two surviving controls were matched and compared. There was no difference in demography (weight mean (sd) in cases v controls 3.2 (0.4) v 3.1 (0.4) Kg, aortic size 3.3 (1.8) v 3.2 (1.5) mm, or anatomical subtype: 9/11 with aortic and mitral atresia v 17/22). However, preoperative mean blood pressure 50 (7) v 43 (5) mm Hg (p = 0.02), systolic blood pressure 71 (12) v 61 (9) mm Hg (p = 0.006), and oxygen saturation 87 (4) v 93 (1)% (p = 0.001) were significantly different in cases as compared with controls. There was no difference in surgical details (bypass times 86 (28) v 74 (25) minutes) or in preoperative lactate, pH, or time ventilated. The lactate was not different 24 hrs postoperatively (3.0 (1.9) v 2.2 (0.6) mmol/l), nor were other physiological parameters, nor were they at discharge. ECG (ST depression in V6 of 0.2 (1.3) v 0.02 (0.5) mm) and echo findings (RV function and degree of tricuspid regurgitation) were not different between the two groups.
Conclusion: A highly significant difference in pre-operative pulmonary blood flow between cases and controls is observed. This suggests that mortality may be due to inherent abnormalities in pulmonary perfusion or the pulmonary vascular bed, rather than in the myocardium or surgical technical complications. Perhaps a rise in pulmonary vascular resistance may be a factor in late mortality after N1.
173 REVERSAL OF VASCULAR DYSFUNCTION IN SUBJECTS AT RISK OF TYPE 2 DIABETES MELLITUS (DM)
C. C. Lang, K. Amudha, M. R. Mustaffa, A. M. Choy.Ninewells Hospital and Medical School, Dundee and University of Malaya, Malaysia
Background: Endothelial dysfunction (ED) plays a pivotal role in the genesis of vascular complications in DM. The aim of our study was to assess if ED is present in the first degree relatives (FDRs) of patients with type 2 DM and if so, whether it is reversible with statin therapy.
Methods: Sixty normotensive and normoglycaemic subjects (mean age 27 ± 4 years; BMI<25) with >1 parent with type 2 DM were compared with 20 age, sex, and BMI-matched controls (negative family history of diabetes). At baseline, we evaluated the endothelial function (by brachial artery reactivity), insulin resistance (using the homeostasis model of insulin resistance, HOMAIR), sICAM-1, and IL-6 levels in both groups. First degree relatives were then randomised to receive either atorvastatin (80 mg) or placebo for 4 weeks.
Results: At baseline, endothelium-dependent dilatation was significantly reduced in FDRs when compared to controls (3.8 ± 0.8% v 12.6 ± 0.9%; p < 0.0001). First degree relatives were significantly more insulin resistant (p < 0.002), and had significantly higher levels of sICAM-1 and IL-6 (p < 0.05 and p = 0.001 respectively) with no differences in endothelium-independent dilatation and lipid profile between groups. After 4 weeks of atorvastatin therapy in FDRs, endothelial function was significantly improved (8.9 ± 3.5% v 4.9 ± 4.6%; p = 0.002) and serum IL-6 level was significantly reduced (p = 0.004). Total serum cholesterol and LDL levels were also significantly reduced (p < 0.0001 and p < 0.01 respectively) by the acute atorvastatin therapy.
Conclusion: We have shown that significant impairment of vascular reactivity can be detected early in the FDRs of subjects with type 2 DM. This was associated with altered insulin sensitivity and elevated levels of sICAM-1 and IL-6. This ED was significantly reversed by acute atorvastatin therapy, an effect which may be related to its hypolipidaemic and anti-inflammatory actions.
174 PERCUTANEOUS TRANSTHORACIC EPICARDIAL ABLATION (PTEA) FOR FAILED ENDOCARDIAL ABLATIONS: PROMISING RESULTS OF A NEW TECHNIQUE
D. Gupta, M. J. Earley, D. J. Abrams, S. Harris, S. Sporton, A. W. Nathan, R. J. Schilling.St. Bartholomews Hospital, West Smithfield, London, UK
Background: Percutaneous transthoracic epicardial ablation has recently been described as a promising technique to treat ventricular tachycardia (VT) with epicardial circuits. However, its success rates using radiofrequency (RF) ablation are only modest, and there is no report of successful PTEA for epicardial accessory pathways (AP) as yet. This is at least partly due to inadequate power generation possible in the closed pericardial space. We hypothesised that PTEA cryoablation (Cryo) could overcome this limitation, and used Cryo in all cases where RF was unsuccessful.
Methods and Results: We attempted PTEA in six patients (four male), of which three had manifest posteroseptal APs (Group A, mean age 31 years) and three had ischaemic VTs (Group B, mean age 56 years). Percutaneous access to the epicardial space was successfully achieved in all patients without complications. Group A: all three patients had multiple previous unsuccessful endocardial ablation attempts. Excellent epicardial signals were seen in two patients who were both successfully treated with PTEA. Radiofrequency was successful in one while another (who had a large coronary sinus diverticulum) needed simultaneous endocardial RF ablation with PTEA Cryo. Percutaneous transthoracic epicardial ablation was not successful in the third patient in whom adequate power could not be delivered with RF epicardially and in whom free manipulation of the Cryo catheter along the posterior AV groove was impossible. Group B: in all three patients, no diastolic potentials (DPs) were detectable endocardially, but excellent early DPs were seen on epicardial mapping. Percutaneous transthoracic epicardial ablation with RF caused sustained VT termination in one patient but only transient cessation of VT in another (low power) in whom Cryo resulted in sustained success. The third patient had multiple morphology VTs and a combination of RF and Cryo PTEA was needed to successfully ablate all the VTs. Overall, PTEA was successful in 5/6 (83%) cases. Mean procedure time 260 ± 21 minutes, Mean Fluoro Time 39 ± 18 minutes.
Conclusion: The results of PTEA for VT and epicardial APs can be significantly improved if Cryo is used in cases where inadequate powers are achieved with RF ablation. However the currently available Cryo catheters have poor manoeuvrability in the epicardial space, which may especially limit access to the posterior atrioventricular groove.
175 THE INFLUENCE OF ATRIAL CONDUCTION, REFRACTORINESS, AND VOLUME ON OUTCOMES FOLLOWING PULMONARY VEIN ISOLATION (PVI)
P. Kojodjojo, P. Kanagaratnam, D. W. Davies, V. Markides, N. S. Peters.St. Mary’s Hospital, Imperial College of Medicine, London, UK
Background: The pathogenesis of atrial fibrillation (AF) consists of an interaction between focal triggers and substrate abnormalities. The arrhythmogenic substrate is characterised by increased chamber size, reduced conduction velocity, and decreased refractoriness (AERP). Pulmonary vein isolation is associated with a significant failure rate and we hypothesise that patients with greater degrees of substrate remodelling are less likely to benefit from such ablation strategies targeting focal triggers.
Methods: Patients with drug-refractory AF were recruited. Pre-ablation isochronal maps of both atria were created during pacing at 600 ms cycle length (CL) using CARTO™ system. Multiple triads of points were analysed using customised software incorporating Cartesian and trigonometric equations, to calculate the wavefront propagation velocity (WPV) specifically in the direction of wavefront propagation. AERP was measured at three atrial sites, at two CLs. Cardiac dimensions were measured with echocardiography. Arrhythmogenic index (AI), defined as the left atrial volume divided by the product of WPV and AERP (wavelength), was calculated. Freedom from AF off anti-arrhythmics was assessed after a mean of 13 months.
Results: Nineteen patients completed the protocol with eight having successful outcomes (42.1%). Patient’s age (56.5 ± 10.5 v 56.0 ± 9.4 years, p = NS), atrial sizes (30.3 ± 8.8 v 51.8 ± 29.0 ml, p = NS), left ventricular dimensions, indices of left atrial systolic function, AERP (221 ± 34 v 226 ± 44 ms, p = NS), biatrial WPV (RA WPV 71.0 ± 8.2 v 75.2 ± 2.4 cm/s, p = NS; LA WPV 67.9 ± 16.4 v 74.3 ± 4.3 cm/s, p = NS) or number of PV isolated (2.75 ± 0.5 v 2.40 ± 0.5, p = NS) did not differ between the two groups. However, patients with successful outcomes had significantly lower AI than failures (1.78 ± 0.28 v 5.70 ± 3.5, p = 0.04).
Conclusion: Patients with recurrent AF after PVI demonstrate a more arrhythmogenic left atrial substrate. Arrhythmogenic index may allow the identification of patients who are more likely to benefit from left atrial ablation in addition to PVI to modify the AF substrate.
176 INCREASED QT DISPERSION AS A PREDICTOR OF MORTALITY FOLLOWING BIVENTRICULAR PACING
S. Muhyaldeen, S. Chalil, S. Ellery, Z. R. Yousef, R. E. A. Smith, P. Jordan, C. Gibbs, F. Leyva.Department of Cardiology, Good Hope Hospital, Sutton Coldfield, West Midlands, UK
Background: Recent studies suggest that biventricular pacing with defibrillator back-up (BiVP-D) improves mortality in patients with heart failure. In animal studies and in acute human studies, epicardial left ventricular pacing and BiVP has been shown to prolong the QT interval and the transmural dispersion of repolarisation, both of which predispose to ventricular tachyarrhythmias. We investigated whether BiVP leads to changes in QT interval and QT dispersion (QTd) and whether such changes relate to sudden cardiac death in patients undergoing BiVP.
Methods: Seventy-six patients with heart failure in New York Heart Association (NYHA) class II (n = 1), III (n = 45), or IV (n = 30) on optimum drug treatment and with a wide QRS complex (160.7 (3.3) (mean (SEM)) underwent novo BiVP (n = 62) or upgrading from right ventricular to BiVP (n = 14). QTd, evaluated from the six standard chest leads and corrected for rate (QTcd), was measured before and 1 month following implantation.
Results: Over a follow up period of 829 (range 342 to 1492) days, seven patients died suddenly and one was resuscitated from ventricular fibrillation (VF). Whereas QTcd increased by 58.7 (23.7) ms from baseline in non-responders, it decreased by 3.5 (5.2) ms in responders (p = 0.0005, ANOVA). Baseline QRS and QT interval duration and changes from baseline in these variables did not emerge as predictors of outcome.
Conclusion: Sudden cardiac death in patients treated with BiVP is related to increased QTcd following implantation. Further studies are needed to determine whether evaluation of QTcd at the time of BiVP implantation can be used to risk-stratify patients for the use of BiVP-D.
177 SAFETY AND ACCEPTABILITY OF CONSCIOUS SEDATION FOR SUB-PECTORAL IMPLANTATION OF IMPLANTABLE CARDIOVERTER DEFIBRILLATORS (ICDs)
M. J. Royle, D. J. Fox, S. Petkar, C. J. Garratt, B. Clarke, A. P. Fitzpatrick.Manchester Heart Centre, Manchester Royal Infirmary, Oxford Road, Manchester, UK
Background: Current National Institute for Clinical Excellence (NICE) guidelines recommend implantation of ICDs using local anaesthetic (LA) and conscious sedation (CS), but this practice remains contentious. In a retrospective study we assessed safety and patient acceptability.
Methods: Medical records determined that 137 of 161 implants/revisions were sub-pectoral, and gave left ventricular ejection fraction (LVEF), procedure time (T), sedatives used (midazolam and diamorphine), and need for intervention to support respiration. Patient acceptability for ventricular fibrillation (VF) induction and defibrillation, willingness to undergo a repeat procedure, and acceptability of the total experience was assessed by questionnaire.
Results: Of 174 consecutive ICD procedures between August 1994 to February 2003, 137 were carried out sub-pectorally under LA and CS. 14/137 were ICD generator changes. The mean age (± SD) was 57.1 ± 16.2 years, 132 were male. Left ventricular ejection fraction was 37.5 ± 16.7%. Average T was 94.4 ± 35.4 minutes. All patients received midazolam 8.1 ± 3.4 mg, and 115 also received diamorphine, 4.0 ± 1.6 mg. Patient acceptability was available for 123 patients. Eight patients had died and six were unobtainable. One respiratory intervention was recorded (apnoea post VF induction requiring flumazenil reversal). There were no deaths, airway crises, or urgent intubations. Twenty-three (17%) recalled VF defibrillation, seven (5%) said it was “painful”. Ten (7%) had reservations about a second procedure but none would refuse it.
Conclusion: Implantation of ICDs under LA and CS is safe and efficacious for the sub-pectoral technique. A combination of titrated midazolam and diamorphine is safe and rarely requires pharmacological reversal. The technique was comfortable and acceptable. Only a minority recollect the procedure.
178 RAPID PULMONARY VEIN (PV) ELECTRICAL ISOLATION USING A NOVEL FOCUSED ULTRASOUND BALLOON CATHETER IN PATIENTS WITH ATRIAL FIBRILLATION (AF)
T. Wong, V. Markides, A. Alinsod, N. S. Peters, D. W. Davies.St. Mary’s Hospital, London, UK and Imperial College, London, UK
Background: Although circumferential PV ablation using conventional radiofrequency catheters is effective at treating AF, procedures can be time consuming and technically challenging. We report use of a novel focused ultrasound balloon catheter (HIFU, ProRhythm Inc, Setauket, NY, USA) to efficiently isolate PV electrically outside the venous ostium with minimal mapping.
Methods: We studied 11 patients (50 ± 10 years, 10 males) with drug refractory highly symptomatic paroxysmal AF. Anatomical circumferential ablation was performed at the antrum of 33 electrically connected PV using HIFU balloon catheters with a diameter significantly larger than that of the venous ostia (25 ± 4 v 13 ± 4 mm, p < 0.0001).
Results: Electrical isolation was achieved in 85% (28/33) of the PV after a short period of sonication (4 ± 4 min/PV). Right phrenic nerve paralysis occurred after right upper PV ablation in the fourth patient and was the only complication. All subsequent patients had high output pacing from all Lasso catheter electrodes at each PV ostium to confirm the absence of phrenic nerve stimulation prior to sonication and no further complications occurred. At 100 ± 66 days follow up, all but one patient were either free from (four patients), or had >50% reduction of (seven patients) arrhythmic symptoms.
Conclusion: A novel focused ultrasound balloon catheter can rapidly and effectively isolate PV by antral sonication. Absence of phrenic nerve capture during high output pacing near intended areas of sonication may be important to avoid phrenic nerve damage.

Abstract 178
179 ABLATION OF DIFFICULT RIGHT SIDED ACCESSORY PATHWAYS (AP) AIDED BY SIMPLE MAPPING OF THE TRICUSPID VALVE ANNULUS (TVA) USING A HALO CATHETER
T. Wong, V. Markides, N. S. Peters, D. W. Davies.St. Mary’s Hospital, London, UK and Imperial College, London, UK
Background: Ablation of right free wall AP is associated with higher rates of both initial failure and late recurrence. We describe a simple approach of using a 20-bipolar catheter (Halo™) placed at the tricuspid annulus to identify the precise location of right sided AP and to guide successful ablation.
Methods: Five patients (two males, age 33 ± 11 years) with right sided APs who had a failed previous ablative procedure (three patients) and/or initial unsuccessful ablation during the same procedure (two patients) underwent mapping of the TVA using a Halo catheter. Placement of the Halo catheter around the TVA was guided by fluoroscopy in orthogonal projections and confirmed by the coexistence of atrial (A) and ventricular (V) electrograms in bipolar recordings from each electrode pair. Sites of earliest atrial activation during V pacing (two patients) or orthodromic tachycardia (two patients), or sites of earliest ventricular activation during A pacing (one patient) during maximal pre-excitation were identified by the Halo catheter and used to guide ablation.
Results: The successful ablation sites showed contact artefact between the RF catheter and the earliest Halo bipolar signals in 3/5 patients and identical local VA/AV times between the RF catheter and earliest Halo bipole in 4/5 patients (the local VA time at the RF catheter was not measurable in one patient because of the close proximity between the two components but contact artefact was present). Loss of AP function was observed 19 ± 6 s into RF application and 60 s applications were completed. Additional consolidation RF applications were applied to the same sites guided by fluoroscopy with reference to the stationary Halo catheter (5/5 patients) and the contact artefact (3/5 patients). The locations of APs were at 8½, 9, 9, 10, and 12 o’clock of the TVA as viewed in the left anterior oblique projection. In all patients APs were ablated successfully without clinical recurrence at 12 ± 4 months follow up.
Conclusion: A Halo catheter positioned at the TVA can accurately locate the right free wall AP and facilitate successful ablation of such potentially difficult pathways. As a result, a Halo catheter is now routinely for all such cases.
180 NITRIC OXIDE MEDIATES THE EFFECTS OF VAGUS NERVE STIMULATION ON VENTRICULAR FIBRILLATION AND ELECTRICAL RESTITUTION IN THE ISOLATED INNERVATED HEART
V. H. Patel1, K. E. Brack2, J. H. Coote2, G. A. Ng1.1Department of Cardiovascular Sciences, University of Leicester, Leicester, UK; 2Division of Medical Sciences, University of Birmingham, Birmingham, UK
Background: Nitric oxide (NO) mediates aspects of vagal activity at the atrial level but its role in mediating the effects of V in the ventricle has not been characterised. The slope of the electrical restitution curve is a key determinant in ventricular fibrillation (VF) initiation. This study examines whether NO mediates the effects of V on restitution and VF in the isolated innervated rabbit heart.
Methods: Adult rabbits (2.2–3.0 kg, n = 7) were sacrificed and vagus nerves isolated at the cervical region. Restitution was studied using single ventricular extrastimuli (S2) protocol with left ventricular monophasic action potential duration (MAPD) measured. S2-MAPD were plotted against preceding diastolic intervals and maximum slope of the fitted exponential curve measured. Ventricular fibrillation threshold (VFT, mA) was determined as the minimum current required to induce VF with rapid (33 Hz) pacing. Measurements were made with and without V: at baseline (BL); with NO-synthase inhibitor LNA (200 μM); with LNA and L-arginine (L-Arg, 1 mM); with L-Arg alone; and after washout.
Results:V increased VFT and decreased maximum slope of restitution. These effects were blocked by LNA and reversed by L-Arg (without effect on its own). There was significant correlation between restitution slope and VFT (r = −0.55, p < 0.0001).
Conclusion:V flattened the restitution curve and increased VF threshold. Inhibition of NO production with LNA blocks the effects of V on the slope of the restitution curve and on VF threshold whilst replenishing substrate for NO production with L-Arg restores these effects. These results suggest that NO released during V may mediate its antifibrillatory action by altering electrical restitution.
Abstract 180
181 FOUR YEARS EXPERIENCE OF A NURSE-LED ELECTIVE EXTERNAL CARDIOVERSION SERVICE WITHIN A DISTRICT GENERAL HOSPITAL SETTING
R. J. Shelton, A. Allinson, T. Johnson, G. C. Kaye.Department of Cardiology, Castle Hill Hospital, Kingston-upon-Hull, UK
Background: External direct current cardioversion is an effective method of restoring sinus rhythm (SR) in patients with persistent atrial arrhythmias. Increasing demand for hospital beds, together with a reduction in junior doctor’s hours, has adversely affected elective cardioversion provision. A regular nurse-led cardioversion service conducted in a dedicated hospital day unit was introduced to resolve these constraints. There is little data on the safety or efficacy of such a service.
Methods: All cardioversions between December 2000 and October 2004 were performed by an appropriately trained specialist nurse, under general anaesthesia (given by an anaesthetist). Patients attended a pre-assessment clinic. Energy requirements for initial and subsequent defibrillations were guided by a local protocol in accordance with AHA/ACC/ESC guidelines. Rectilinear biphasic defibrillation was introduced in January 2004 with an appropriate protocol amendment. The aim, in the absence of complications, was to discharge patients the same day.
Results: 573 cardioversions (470 monophasic; 103 biphasic) were performed on 464 patients (72.1% male, mean (± SD) age 67.8 ± 9.4 years) with atrial fibrillation (AF) (89.7%) and atrial flutter (10.3%). Sinus rhythm was restored in 84.0% and 100% of patients with AF and atrial flutter respectively, which increased to 90.2% and 100% following the introduction of biphasic defibrillation. Biphasic shocks cardioverted AF with less energy (163 ± 22 v 289 ± 81 Joules), and less cumulative energy (230 ± 139 v 455 ± 255 Joules) than monophasic (p < 0.001 for both), despite no difference in the duration of AF (p = 0.26), or patient age (p = 0.78). Two patients required hospital admission due to transient bradycardia; both discharged within 72 hours, without the need for permanent pacing. 99.6% of patients were discharged home the same day; there were no deaths.
Conclusion: The provision of a nurse-led elective cardioversion service is feasible and effective, without compromising safety.
182 CARDIAC PHYSIOLOGIST LED ARRHYTHMIA CLINIC SUBSTANTIALLY REDUCES CONSULTANT CLINIC WORKLOAD
A. E. French, L. Grounds, K. Woodburn, T. Rashid-Fadel, T. R. Cripps.Cardiology Department, Bristol Royal Infirmary, Bristol, UK
Cardiac physiologists (“technicians”) possess skills invaluable in managing palpitation patients. They are experienced at assessing such symptoms in pacing and other non-invasive clinics, and have expertise in ambulatory monitoring analysis. During a 15 month period, 100 such patients were seen in a physiologist led clinic. Patients were selected for the clinic by Consultants from General Practitioner (GP) referrals judged to involve benign symptoms unlikely to require specialist treatment. Physiologist assessment was by structured questionnaire including character, duration and frequency of symptoms, medication, and past history. Electrocardiogram (ECG), chest x ray (CXR), and appropriate ambulatory monitoring were performed. Results were overviewed by an electrophysiologist and recommendations made to the GP by letter. Ambulatory monitoring was selected according to frequency and character of symptoms. This was a continuous ambulatory ECG (mostly 24 hour) in 24 patients, patient activated loop recorder in 46 patients, and 1 week continuous loop recorded in 15 patients. No monitoring was considered necessary in the remaining 15 patients. In 17 patients an arrhythmia (other than occasional ectopic beats) was detected on monitoring, usually short runs of atrial fibrillation (AF) (commonly aged >40 years) or brief supraventricular tachycardia (SVT) (commonly aged <40 years). There was a trend towards better arrhythmia detection using patient activated monitoring (17% with patient activated recorder v 13% for both continuous recording and continuous loop recorder). Only one patient required review in the Consultant clinic (to discuss ablation because of frequent prolonged SVT episodes) and one was listed for cardioversion because of chronic AF. Assuming 20 minutes for a new patient appointment, the clinic saved 33 hours (over 10 weeks at one 3 hour clinic per week) of out-patient waiting list time, or twice this if initial and follow up visits were required.
Delegation of patients with simple arrhythmia symptoms to a cardiac physiologist led clinic can significantly reduce waiting lists for Consultant clinics. This study provides support for the promotion of non-Consultant led arrhythmia clinics in line with the now well established chest pain clinics.
183 SCREENING FOR SUSPECTED HEART FAILURE WITH N TERMINAL PRO-B TYPE NATRIURETIC PEPTIDE (NT PROBNP) IN PRIMARY CARE: MONEY WELL SPENT?
A. Fuat, J. J. Murphy, G. Brennan, A. A. Mehrzad, J. I. Johnston, W. S. A. Smellie.Darlington PCT, Darlington Memorial & Bishop Auckland Hospitals & University of Durham, Durham, UK
Introduction: Despite inclusion in recent national guidelines, the uptake of natriuretic peptides by the NHS has been slow. Clinicians and Primary Care Trusts (PCTs) harbour concerns about appropriate cut-offs and the lack of cost benefit/effectiveness data. We have previously shown that NT proBNP below 150 pg/ml demonstrated a high negative predictive value for excluding heart failure due to left ventricular systolic dysfunction (LVD). We report the results of a cost benefit analysis in the first “real life” trial of NT proBNP in primary care.
Methods: 600 consecutive patients from 34 general practices were studied. The role and place of NT pro-BNP within the heart failure pathway was communicated to practices. General Practitioners (GPs) were encouraged to request NT proBNP if heart failure was suspected clinically and if above 150 pg/ml, the report recommended referral to a one-stop diagnostic clinic. The GPs were also asked to select an alternative management strategy from a list of options, had NT proBNP not been available.
Results: The 600 patients had a median age of 77 years (range 35 to 95) and 368 (61%) were women. 204 had an NT proBNP below the action limit. Of the 396 with raised levels, 333 (84%) were referred to diagnostic clinics within the next 3 months and 84 (25%) of those referred had heart failure due to LVD. Allowing for quality controls, we estimated the cost of each NT proBNP assay as £21. So the crude cost of detecting LVD was £150 per case. However, 204 specimens were below the action limit and of these, the reported alternative to NT proBNP testing was referral to hospital clinics in 152. Four were referred despite a normal result so potentially 148 referrals were avoided. With the introduction of “Payment by Results” from April 2005, the national tariff for a cardiology outpatient referral will be £136, so avoiding these referrals could have saved £20 128, making it attractive to PCTs.
Conclusion: In this first “real life” study of NT proBNP in primary care, 84 cases of LVD were detected from 600 specimens (14%) at a cost of £12 600 (£150 per case of LVD). However, 148 referrals to hospital diagnostic clinics were potentially avoided, at a cost saving of £20 128. This cost benefit balance will make the use of NT proBNP attractive to PCTs.
184 THE IMPACT OF THE INTRODUCTION OF NT-PROBNP INTO PRIMARY CARE ON SECONDARY CARE REFERRAL RATES
A. Turley, A. P. Roberts, B. Kunadian, A. Davies, M. A. de Belder, J. Drury, M. J. Stewart.Department of Cardiology, The James Cook University Hospital, Marton Road, Middlesbrough, UK
Background: The neurohormone N-Terminal pro B-type natiuretic peptide (NT-proBNP) is predominantly released form the left ventricle in response to increasing wall tension, and is recommended for use in the investigation of patients with suspected left ventricular systolic dysfunction (LVD).
Aim: To evaluate the impact of the introduction of NT-proBNP testing in primary care on secondary care echocardiography and out-patient (O/P) referral rates.
Methods: N-Terminal pro B-type natiuretic peptide was measured in 1054 patients with clinical symptoms and signs suggestive of LVD over a 1-year period from two neighbouring primary care trusts. We retrospectively reviewed our digital archive echocardiographic database and hospital O/P appointment system for all of these patients.
Results: N-Terminal pro B-type natiuretic peptide was elevated (NT-proBNP >150 ng/L) in 744/1054 patients (71%), 42% male, median age 76 years (33–100 years), median NT-proBNP value 611 ng/L (151–48743 ng/L). Of those patients with an elevated NT-proBNP 492/744 (66%) had a previous echocardiogram of which 386/492 (78%) were performed after the NT-proBNP result. 174/744 patients (23%) were referred to a designated heart failure clinic, 92/744 (12%) to a general cardiology clinic, 60/744 (8%) to a care of the elderly clinic, and 100 (13%) to another medical clinic. 181/744 patients (24%) with an elevated NT-proBNP were not referred for either an echocardiogram or an OP appointment. A cut off of 150 ng/L was used, sensitivity 0.97 (CI (confidence interval) 0.94 to 0.98), specificity 0.45 (CI 0.41 to 0.48), positive predictive value 0.44 (CI 0.41 to 0.48), negative predictive value 0.97 (CI 0.94 to 0.98).
Conclusion: If NT-proBNP is to be used within primary care for the investigation of patients with suspected LVD then strict guideline adherence must ensure. As over 70% of patients tested required referral for further investigation, use of NT-proBNP for triage is poor and cost-effectiveness as compared to increased access to imaging must be considered.
185 TETRAHYDROBIOPTERIN REGULATES VAGAL CONTROL OF HEART RATE
D. Adlam, E. Danson, J. Khoo, N. J. Alp, D. J. Paterson, K. M. Channon.Department of Cardiovascular Medicine and Department of Physiology, University of Oxford, Oxford, UK
Loss of cardiac vagal function is a clinically important feature of chronic heart failure. Nitric oxide (NO), generated by neuronal NO synthase (nNOS) mediates cardiac vagal function, but the mechanisms linking nNOS regulation with vagal function remain unclear. We investigated the role of the NOS cofactor, tetrahydrobiopterin (BH4), in cardiac vagal regulation in vivo. We studied the hph-1 mouse, a model of BH4 deficiency due to a mutation in the gene encoding GTPCH1, the rate limiting enzyme in BH4 biosynthesis. Blood pressure, determined by tail-cuff, was not different between hph-1 mutants (hph), heterozygous (+/−), and wild-type (WT) littermates. However, both hph and +/− mice had a significant resting tachycardia (mean (SEM): hph 656 (13) v WT 616 (11), p < 0.01). This difference was abolished by administration of the NOS inhibitor, L-NAME. In vitro vagal function, quantified by the response to vagal stimulation in isolated atria, was significantly impaired in both hph and +/− animals v WT littermates (see fig; *p < 0.05, **p < 0.005). Inhibition of nNOS by L-VNIO had no effect on the residual vagal responses in hph or +/− mice. However, L-VNIO reduced vagal responses in WT mice to the level of hph and +/− mice, an effect that was reversed by the addition of excess L-arginine.
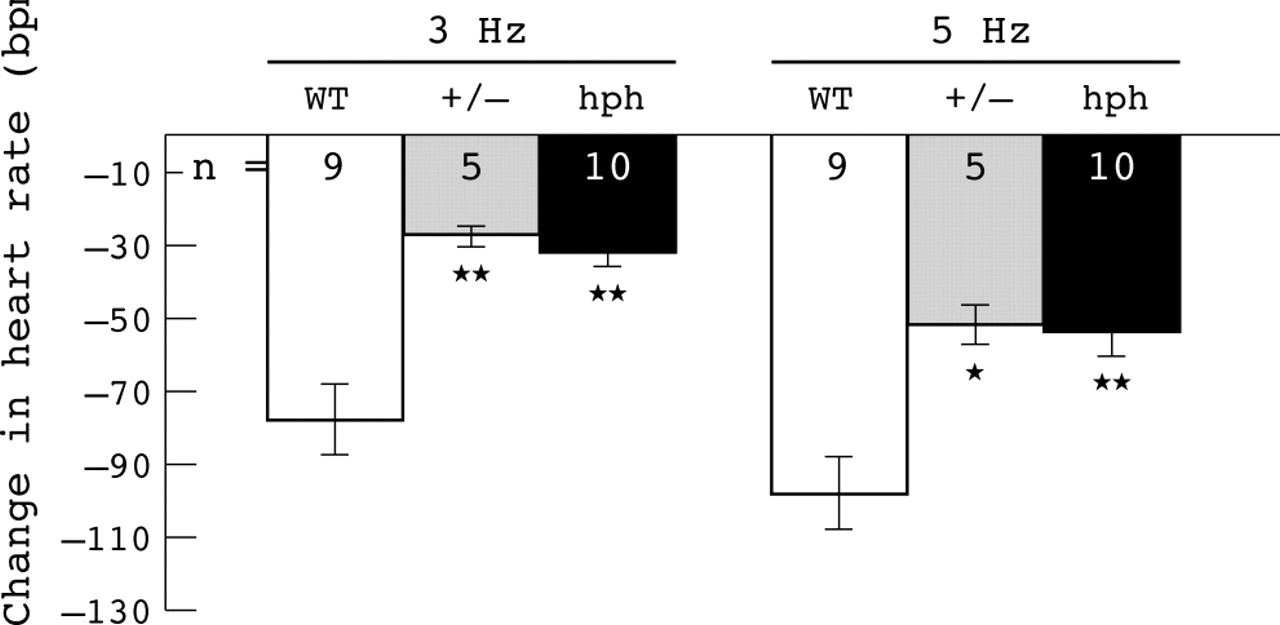
Abstract 185
Tetrahydrobiopterin regulates heart rate in vivo mediated through nNOS-dependent vagal function. This novel mechanism may provide potential therapeutic targets in heart failure and other cardiovascular disease states.
186 P38-MAPK MEDIATES THE EARLY NEGATIVE INOTROPIC EFFECT OF TUMOUR NECROSIS FACTOR-α (TNF). EVIDENCE OF SYNERGY BETWEEN A DIRECT NEGATIVE INOTROPIC EFFECT AND CORONARY CONSTRICTION
M. Bellahcene, X. B. Cao, J. Layland, M. Tanno, A. M. Kabir, R. S. Haworth, A. M. Shah, M. Avkiran, M. S. Marber.Cardiovascular Division, KCL, The Rayne Institute, St. Thomas’ Hospital, London, UK
Background: Tumour necrosis factor-α exerts a negative inotropic effect on myocardium from various species. Tumour necrosis factor-α activates p38-MAPK and this kinase is thought to depress contractility in a calcium-independent manner. We therefore examined TNF effects on contractility in mice lacking the p38-MAPK activator—MKK3.
Methods: The left ventricular developed pressure (LVDP; isovolumic contraction), coronary flow, p38-MAPK, and HSP27 phosphorylation, as well as the end-diastolic v LVDP relationship were analysed in C57BL/6 outbred, mkk3 wild-type (WT), and mkk3 knock-out (KO) isolated mouse hearts exposed to 10 ng/ml TNF i.c. for 15 minutes after 40 minutes of stabilisation. Some hearts received SB203580 (p38-MAPK catalytic site inhibitor; 1 μM) for 20 minutes starting 5 minutes before TNF infusion. All protocols were run under constant pressure and constant flow conditions. Tumour necrosis factor-α effects were also investigated in isolated murine cardiomyocytes.
Results: Tumour necrosis factor-α significantly reduced LVDP and coronary flow in outbred and mkk3-WT mice. This early negative inotropic effect was associated with a significant phosphorylation of both p38-MAPK and HSP27. However, TNF did not reduce LVDP or phosphorylate p38-MAPK and HSP27 in mkk3-KO mice. Furthermore, SB203580 attenuated TNF-induced negative inotropy, as well as HSP27 phosphorylation. The effects on the end-diastolic v LVDP relationship followed a similar pattern. Comparison of constant pressure v constant flow models of heart perfusion, demonstrated that TNF-induced coronary constriction contributes to p38-MAPK activation, and consequent negative inotropy. Finally, studies on murine cardiomyocytes confirmed a direct negative inotropic effect of TNF mediated, at least in part, by p38-MAPK.
Conclusion: Our results implicate p38-MAPK in the early negative inotropic effect of TNF and suggest this result forms a combination of a direct effect on cardiac myocytes and an indirect effect resulting from reductions in coronary flow.
187 THE PREVALENCE/INCIDENCE PARADOX OF ATRIAL FIBRILLATION IN HEART FAILURE
R. J. Shelton, A. L. Clark, J. G. F. Cleland.Department of Academic Cardiology, Castle Hill Hospital, University of Hull, Kingston-upon-Hull, UK
Background: Atrial fibrillation (AF) and congestive heart failure (CHF) are common and frequently coexist. Epidemiological surveys and large clinical trials in CHF provide strong evidence that AF is a marker of increased morbidity and mortality. Despite this, little data exists on the incidence of persistent AF in patients with CHF outside of clinical trials.
Methods: Consecutive patients who attended a community heart failure clinic were enrolled. Data was collected at initial visit and 1 year later. Systolic heart failure was defined as a left ventricular ejection fraction (LVEF) of <45% in the presence of appropriate symptoms. Persistent AF was defined as the continued presence of AF for at least 1 month. Patients with paroxysmal AF, secondary AF, a permanent pacemaker, or atrial flutter were excluded from the main analysis (you would have to report these in poster/paper). All patients underwent optimisation of heart failure medication during follow up.
Results: 778 (mean ± SD) aged 70 ± 10 years (70% male, LVEF 32 ± 9%) were diagnosed with systolic heart failure. The overall prevalence of persistent AF at initial visit was 24%. Patients with AF were older (p < 0.001), with increased serum creatinine (p = 0.02) and NT-BNP (p = 0.01). There was no difference in sex, LVEF, QRS duration, haemoglobin, or C-reactive protein between groups. On multivariate analysis by logistic regression, only age (p < 0.01) and New York Heart Association (NYHA) class III/IV (p = 0.02) were independently associated with AF at baseline. There were 132 deaths; 34 AF (18.8%), 98 SR (17.2%), within 1 year of initial assessment. Of the 473 patients in SR at initial assessment, only 12 (2.5%) had developed persistent AF at 1 year. The incidence rate of persistent AF was calculated at 25.4 per 1000 person-years.
Conclusion: Despite a high prevalence of persistent AF in patients with heart failure, the incidence appears low. For many patients the onset of AF coincides with or precedes the development of heart failure.
188 IS CLINICALLY OVERT DIABETES MELLITUS A CAUSE OR A CONSEQUENCE OF HEART FAILURE?
J. John, P. Reddy, J. Dhawan, S. F. Beer, J. G. F. Cleland.Castle Hill Hospital, Cottingham Road, East Yorkshire, UK; Scunthorpe General Hospital, Cliff Gardens, Scunthorpe, UK
Background: The prevalence of diabetes in patients with heart failure selected for clinical trials is high but the diagnostic criteria for diabetes mellitus have not been rigorous and there is a relative paucity of information from non-trial populations. Diabetes is usually considered a risk factor for, rather than a consequence of, the development of heart failure. However, it is unknown how often diabetes mellitus precedes or post-dates the development of heart failure.
Methods: We studied 618 consecutive patients attending heart failure clinic with a diagnosis of heart failure due to left ventricular systolic dysfunction (LVD) (ejection fraction (EF) <40%) and receiving treatment with a diuretic and symptoms consistent with heart failure. The baseline characteristics were recorded including the presence of diabetes. In those who had no clinically overt diabetes, a random/fasting plasma glucose (RPG/FPG) and HbA1c was performed to identify latent diabetes. Criteria for diabetes was RPG of >11.1 mmol or FPG of >7 mmol.
Results: The mean age of the population was 68.9 years and 32% were women, consistent with the epidemiology of heart failure due to LVD. 372 patients (60.2%) had a history of ischaemic heart disease. The majority of patients 513 (83%) were in New York Heart Association (NYHA) class II/III. Overall, 166 patients (32%) had diabetes. A clinical diagnosis of diabetes preceded that of heart failure in 73 patients (11.8%). Sixty-one patients (9.8%) developed clinically overt diabetes only after the development of heart failure. Thirty-two patients (5.18%) were found to be diabetic on routine blood examination at the time of diagnosis of heart failure. Heart failure patients with diabetes had a higher mean body mass index (BMI) (29.2) than those without diabetes (26.7) (p < 0.001). Mean duration from the diagnosis of heart failure to onset of diabetes was 3.2 years. No obvious differences between patients developing diabetes before or after the development of heart failure were noted.
Conclusion: Heart failure predicts the development of type 2 diabetes, irrespective of age and sex, with more prevalence higher NYHA class. About half of patients with diabetes and heart failure will develop diabetes only after the development of heart failure. The clinical course of diabetes developing before or after the onset of heart failure may be different. This requires further investigation.
189 ETHNIC DIFFERENCES IN THE PREVALENCE AND AETIOLOGY OF LEFT VENTRICULAR SYSTOLIC DYSFUNCTION (LVD) IN HIGH-RISK COMMUNITY SUBJECTS
G. I. W. Galasko, A. Lahiri, R. Senior.Cardiac Research Department, Northwick Park Hospital, Harrow, Middlesex, UK
Introduction: Heart failure is a common chronic disorder, with LVD underlying most treatable cases. Many subjects with LVD have underlying risk factors. No prior study has evaluated ethnic differences in the prevalence and aetiology of LVD, with South Asians (people from the Indian subcontinent) potentially having a higher prevalence of LVD and more underlying coronary artery disease (CAD) than whites. This study was undertaken to assess this further in high-risk subjects in a multi-ethnic community.
Methods: 1392 general population subjects and 928 high-risk subjects (ischaemic heart disease, heavy alcohol intake, diabetes mellitus, cerebrovascular disease, peripheral vascular disease, hypertension) ⩾45 years old were randomly selected from seven representative general practices in Harrow and invited to attend. Attendees underwent a questionnaire, venesection, ECG, and echocardiography examination. Subjects found to have LVD (left ventricular ejection fraction <50%) underwent stress-rest gated 99 mTc Sestamibi myocardial perfusion imaging ± coronary angiography to rule out underlying CAD.
Results: 734 general population invitees (53%) attended of whom 290 were classified as high-risk. 471 high-risk invitees (51%) attended. Thus 761 high-risk subjects attended and were analysed further—549 whites and 181 South Asians. South Asians had a higher prevalence of prior myocardial infarction (23% v 14%, p = 0.007) and diabetes mellitus (45% v 17%, p < 0.0001) and a lower mean high density lipoprotein (HDL)-cholesterol concentration (1.2 mM v 1.4 mM, p < 0.0001) than whites. Left ventricular ejection fraction (LVEF) was calculable in 738 cases (97%). Ninety-eight subjects (13.3%, 10.9–15.9%) had LVD, with prevalence increasing with male gender and increasing age. The age- and gender-adjusted prevalence of LVD was 16.9% in South Asians v 10.9% in whites (p = 0.05). The prevalence of underlying CAD was 90% in South Asians v 62% in whites (p = 0.01).
Conclusion: Left ventricular dysfunction occurs commonly in high-risk community subjects. South Asians have a significantly higher prevalence of LVD and a higher proportion of underlying CAD than whites. Potential explanations may be the higher prevalence of diabetes mellitus and prior myocardial infarction, and lower mean HDL-cholesterol levels in South Asians than whites.
190 PROGNOSTIC VALUE OF BRAIN NATRIURETIC PEPTIDE (BNP) IN PATIENTS WITH PULMONARY ARTERIAL HYPERTENSION (PAH)
M. H. Williams, C. E. Handler, M. R. Akram, C. Das, J. Smee, C. P. Denton, D. Nair, E. Neville, C. J. Smith, C. M. Black, J. G. Coghlan.Departments of Cardiology, Rheumatology, and Biochemistry, Royal Free Hospital, London, UK; UCL Medical School, London, UK
N-terminal BNP is used to diagnose left heart failure but its role in PAH and right heart failure is unclear. Patients with severe PAH are considered for expensive advanced disease-modifying treatments because they have a poor prognosis. In a previous pilot study we proposed a level of 395 pg/ml as a cut-off for excluding scleroderma associated PAH (SSc-PAH). This was a further study to test the accuracy of this proposal. We measured BNP, pulmonary vascular resistance (PVR), 6 minute walk distance (SMWD), and survival (follow up: 1 month–18 months, mean 10 months) in 82 patients with systemic sclerosis (SSc), both with and without PAH, and without significant left heart failure (pulmonary capillary wedge pressure <15 mm Hg), diagnosed by right heart catheterisation (mean PAP >25 mm Hg). Twenty-one (26%) control patients with SSc and normal mPAP had mean BNP levels of 177 pg/ml (SD 196 pg/ml). Sixty-one (74%) patients with PAH had significantly higher mean BNP levels 1602 pg/ml (SD 2760 pg/ml) p = 0.0002. Brain natriuretic peptide positively and significantly correlated with mean PAP (r = 0.62; p < 0.0001), PVR (r = 0.81; p < 0.0001), and inversely and significantly with SMWD (r = −0.46; p < 0.0001). Twenty-six (32%) patients were in WHO functional I and II and had mean BNP levels of 475 pg/ml (SD 1307 pg/ml). Fifty-six (68%) patients in classes III and IV had significantly higher mean BNP levels of 1615 pg/ml (SD 2800 pg/ml) p = 0.01. Our study revealed a sensitivity of 0.59 and a specificity of 0.86 for predicting presence of PAH.
Raised BNP levels are directly related to the severity of PAH. Levels below 395 pg/ml accurately identify patients without PAH. However, elevated levels are still found in some patients without PAH. Further studies are required before BNP can be used as a screening tool to exclude patients without PAH, in all settings including primary care.
191 CLINICAL PREDICTORS OF 6-MINUTE WALK TEST (6-MWT) PERFORMANCE IN PATIENTS WITH CHRONIC HEART FAILURE (CHF)
L. Ingle, A. S. Rigby, P. K. Jones, A. L. Clark, J. G. F. Cleland.Department of Academic Cardiology, Castle Hill Hospital, Cottingham, Hull, UK
Background: The 6-MWT is used to estimate functional capacity in patients with CHF. However, it is unclear which clinical correlates most strongly predict 6-MWT performance.
Methods and Results: 1290 patients with CHF enrolled in a chronic disease management programme (63% male; mean age 71 ± 10 years; body mass index (BMI) 28 ± 5) and completed a 6-MWT (mean distance 367 ± 108 m). Clinical measures including echocardiography, ECG, blood pressure, spirometry, quality of life assessment, and routine blood samples were undertaken. Relationships with walking distance were determined by calculating odds ratios (ORs) (odds of walking ⩽300 m v >300 m) with 95% confidence intervals (CIs). Predictors of poor walking distance (⩽300 m) included: age ⩾75 years (OR 4.8; 95% CI 3.4 to 6.9); anaemia (OR 3.0; 95% CI 2.2 to 4.1); low BMI (<20) (OR 2.6; 95% CI 1.5 to 4.4); elevated resting heart rate >80 beats/min−1 (OR 2.3; 95% CI 1.6 to 3.3); and being female (OR 1.3; 95% CI 1.0 to 1.7). Serum creatinine and NTpro-BNP showed dose-response effects, as did qualitative indicators such as self-perceived depression and anxiety scores. In a multiple regression model, the depression and anxiety scores remained independent predictors of walking distance after adjusting for demographic and biochemical variables.
Conclusion: The determinants of 6-MWT are complex and depend on physical—both cardiovascular and non-cardiovascular—and psychological factors. The 6-MWT, when adjusted for age, is a simple but useful objective marker with which to assess patients’ symptoms and overall well being.
192 DELIVERY OF PRE-HOSPITAL THROMBOLYSIS BY PARAMEDICS
M. Cooke, D. Chamberlain, H. Swanton.Ambulance Service Association, Royal Sussex County Hospital, The Heart Hospital, London, UK
It is well established that the benefit of thrombolysis in myocardial infarction is time dependant. Up to 65 lives can be saved per 1000 treated if the thrombolytic agent is given within 1 hour of symptom onset. The need to shorten the door to needle time has driven this pre-hospital thrombolysis initiative. Following acceptance by the Medicines and Healthcare Regulatory Authority in 2003, the Prescriptions Only Medicines (human use) legislation was amended in May 2004 to include tenecteplase and reteplase for use by paramedics in the pre-hospital setting. Twenty-four of the 31 ambulance trusts in England are now able to administer pre-hospital thrombolysis for ST elevation myocardial infarcts. Four others are planning to introduce the service by the end of 2004. Adjuvant unfractionated heparin is included in the protocol. There are rigid inclusion criteria for thrombolysis and the upper age limit for therapy is 75 years. Paramedic training is supported by the use of checklists, ECG telemetry, and mobile phones, but as confidence and experience grows, ambulance services are becoming more autonomous. By November 2004, 1349 patients had received pre-hospital thrombolysis (1070 in the last 12 months). There is a rapid rise in the number of patients being treated per month. The median call to needle time was <40 minutes. There has been no evidence of any major events either in terms of inappropriate administration or major haemorrhage. From December 2004 patient outcome data will become available to the ambulance service from the Myocardial Infarction National Audit Project (MINAP).
Pre-hospital thrombolysis is a rapidly expanding service in England. At present approximately 2% of patients receiving thrombolysis do so in the pre-hospital setting, but this figure will continue to rise as this initiative progresses.
193 LEFT BUNDLE BRANCH BLOCK (LBBB) MYOCARDIAL INFARCTION (MI)—A STUDY OF THROMBOLYSIS IN A DISTRICT GENERAL HOSPITAL
C. A. Blakemore, P. J. Keeling.Torbay Hospital, Torquay, Devon, UK
Background: Identification of acute MI in patients who present with a LBBB ECG is problematic. Evidence suggests that reperfusion is underused in this group and that mortality is excessive. We reviewed the use of thrombolysis and mortality rates in all patients presenting with an acute MI and a LBBB ECG over the course of 1 year in Torbay Hospital, a District General serving a population of 275 000.
Method: We used the Myocardial Infarction Audit Project (MINAP) database to identify all patients presenting between April 2002 and March 2003 with a LBBB ECG and a Troponin I >1.5 ng/ml. We recorded whether they received thrombolysis and, if not, the documented reasons for withholding treatment. We examined mortality figures and looked at strategies to improve rates of thrombolysis.
Results: 712 patients presented with acute MI over this period, of which 47 were LBBB MI. Of these 47, 35 had no contraindications to thrombolysis but only eight (23%) of these received a lytic. The reasons given for not thrombolysing the remaining 27 were “poor history” (33%), “old LBBB” (30%), “not sure if LBBB new or old” (7%). No reason was documented in the remaining 30%. Overall mortality in those not thrombolysed (including those with contraindications) was 46% (18 of 39) compared to 12.5% (1 of 8) of those lysed. Thrombolysing those with only proven new LBBB would have resulted in nine (25%) of those eligible receiving treatment. Use of ECG criteria in those with pre-existing LBBB as proposed by Sgarbossa et al (NEJM, 1996) would have identified an additional six patients, resulting in 43% of eligible patients receiving thrombolysis.
Conclusion: Patients presenting with LBBB MI were undertreated and had a high excess mortality. There was reluctance to thrombolyse patients without evidence of new LBBB. Using specific criteria would have increased the number treated; however, since the benefits of thrombolysis seem to outweigh the risks we argue that it should be considered in any patient with a good history for MI and a LBBB ECG.
194 TWO YEARS OF PRIMARY CORONARY INTERVENTION FOR ST ELEVATION MYOCARDIAL INFARCTION IN A DISTRICT GENERAL HOSPITAL
S. Qaisar, M. Fellows, H. Whitlam, R. Jaumdally, J. M. Beattie, P. J. Lowry, N. El-Gaylani, R. G. Murray, J. Ment, S. Eccleshall, M. Pitt.Department of Cardiology, Birmingham Heartlands and Solihull Hospital NHS Trust, Bordesley Green East, Birmingham, UK
Introduction: The two established models for delivering primary percutaneous coronary intervention (PCI) for acute ST elevation myocardial infarction (STEMI) involve patient transfer to tertiary “infarct centres” or PCI at the point of presentation in a district hospital. Comparable outcomes can be achieved with either model if door to intervention times are under 2 hours and clinical activity is sufficient to maintain expertise. We present our 2-year experience of primary PCI in a large district hospital (950 beds) with a single cardiac catheter laboratory and a throughput of 720 interventional procedures per year covered by off-site cardiac surgery.
Methods: From November 2002, primary PCI was offered to all thrombolysis eligible STEMI patients admitted on weekdays from 09:00 to 17:00. After April 2004, this service was rolled out to around the clock, 7 days a week. Non-thrombolysis eligible STEMI patients admitted in this period were also managed by PCI but data for these patients is not included here.
Results: 137 patients were treated in the 2-year period (89 males, mean age 67 years). Procedural success (stent delivered to target lesion) was 95%. Abciximab was used in 93% of cases. In hospital mortality was nine patients (6.6%) of whom five presented in cardiogenic shock. Median “door to coronary device” time was 86 minutes (range 25 to 286). Seventy one percent and 52% of patients had door to device times of less than 120 and 90 minutes, respectively. Median length of hospital stay was 5 days. In our centre patients receiving thrombolysis for STEMI in the years 2000–2004 had a median hospital length of stay of 8 days and in hospital mortality of 7.2%. After initiation of the round the clock service, 14 of 75 patients (19%) presented during the most unsocial hours of midnight to 08:00. Median “door to coronary device” time for these 14 patients was 95 minutes (range 47 to 201).
Conclusion: In the contemporary era of interventional cardiology it is possible to introduce and sustain a primary PCI service for STEMI in a district general hospital setting. This was delivered with no additional staffing requirement and with acceptable 24 hour “door to coronary device” times and mortality.
195 DIRECT 24-HOUR AMBULANCE TRIAGE AND TRANSFER OF PATIENTS WITH ACUTE MYOCARDIAL INFARCTION (AMI) TO A CARDIAC INTERVENTION CENTRE WITH NO ACCIDENT AND EMERGENCY DEPARTMENT
M. Al-Obaidi, M. Dalby, A. Asherson, R. Smith, N. Margerison, R. Grocott-Mason, M. Al-Bustami, A. Mitchell, M. Mason, C. Ilsley.Hillingdon Hospital, Uxbridge, Middlesex, UK; Harefield Hospital, Harefield, Middlesex, UK
Background: Ambulance crew are increasingly involved in assessment and ECG interpretation of patients with AMI. This process has allowed rapid triage and early mobilisation of staff at receiving hospitals to facilitate prompt administration of thrombolysis. Application of this system in a programme of primary percutaneous intervention (PPCI) may similarly allow shorter reperfusion times
Methods: We collaborated with our local ambulance service provider (LAS) to design a protocol for 24-hour direct hospital transfer of patients with AMI. In brief, all patients with chest pain and ECG changes suggestive of AMI were eligible; unresponsive or unconscious patients were excluded and diverted to the local district hospital.
Results: A total of 56 patients were transferred (mean age 66 years (range 34–93), 38 males (range 68%)). Of those patients, 42 underwent PPCI. Of the remaining 14 patients, 12 underwent diagnostic angiography, of whom four had normal coronaries and eight had minor coronary disease not requiring intervention. Of the two patients who did not undergo angiography, one had coronary anatomy previously defined and the other had advanced multi-organ failure and an elective decision not to proceed was made. The mean time from LAS call to arrival at our centre was 15 ± 8 minutes (min–max; 2–25 minutes) with 16/56 (29%) of calls made between 20:00 and 08:00. In the patients who underwent PPCI, the average time from arrival to target vessel reperfusion was 31 ± 11 minutes, with TIMI III flow achieved in 91% of patients. Twelve patients underwent multi vessel revascularisation either at admission (6/42, 14%) or as an electively staged procedure during the same admission (6/42, 14%). There were no complications encountered during transfer of patients and no major peri-procedural complications recorded.
Conclusion: Direct ambulance triage and transfer for PPCI is safe and time efficient. Significant reduction of time to reperfusion by PPCI by widespread implementation of this system is likely to improve the morbidity and mortality of AMI.
196 THE HOSPITAL BURDEN OF SUSPECTED ACUTE CORONARY SYNDROMES (ACS): RECENT TRENDS
N. F. Murphy1, K. MacIntyre1, J. Chalmers2, S. Frame2, A. Redpath2, A. Finlayson2, J. Pell, S. Stewart1, S. Capewell3, J. J. V. McMurray1.1University of Glasgow, Glasgow, UK; 2Information and Statistics Division, Edinburgh University, Edinburgh, UK; 3University of Liverpool, Liverpool, UK
Objective: To describe the changing burden of suspected ACS on the hospital sector of the National Health Service in Scotland between 1990 and 2000.
Methods: This was a retrospective cohort study in Scotland (population 5.1 million) using the Scottish Morbidity Record Database. Patients were all 409 755 emergency hospitalisations with suspected ACS in the Scottish population aged ⩾ 18 years between 1990 and 2000. Main outcome measures were: the number of emergency hospitalisations; individuals and readmissions with acute myocardial infarction (MI), angina, and chest pain; and length of stay, total bed days, and revascularisation rates.
Results: Between 1990 and 2000, there were 117 479 hospitalisations for acute MI, 71 927 for angina, and 123 123 for chest pain. The number of hospitalisations increased by 45% from 26 369 in 1990 to 38 285 in 2000. Length of stay declined by an average of 3 days and overall number of bed days occupied by suspected ACS fell from 300 304 in 1990 to 225 033 in 2000. There was a marked increase in coronary revascularisation rates in individuals over the study period from 1.6% to 9.3% for acute MI and 6.4% to 12.4% for angina in men.
Conclusion: Hospitalisations for suspected ACS have risen despite a fall in admission rates for acute MI. Rates of revascularisations have also increased dramatically. The burden of suspected ACS as measured by bed occupancy has not increased because of a reduction in length of stay. The burden of suspected ACS could be reduced by strategies targeting non-cardiac chest pain.
197 MOLECULAR BASIS FOR PLATELET HYPER-REACTIVITY TO ADENOSINE DIPHOSPHATE (ADP) ASSOCIATED WITH THE PLATELET P2Y1 RECEPTOR 1622 G ALLELE
S. L. Hetherington, D. Lodwick, A. H. Goodall, N. J. Samani.Department of Cardiovascular Sciences, University of Leicester, Leicester, UK; Glenfield Hospital, Leicester, UK
Background: The ADP receptors, P2Y1 and P2Y12, play a pivotal role in platelet aggregation. We have recently shown that a silent A>G substitution at position 1622 of the P2Y1 ADP receptor gene is associated with increased platelet response to ADP, as measured by fibrinogen binding to the activated GPIIb-IIIa receptor. Here we have analysed the effect of this single nucleotide polymorphism (SNP) on platelet function in more detail and explored the molecular mechanism, by measuring platelet aggregation, calcium flux, and expression of P2Y1 receptor mRNA.
Methods: Subjects were genotyped for the P2Y1 1622 SNP using a TaqMan assay. Twenty-two healthy adult subjects were recruited (eight GG and 14 AA homozygotes, age and sex matched). Maximal platelet aggregation was assessed by light transmittance, to 160 nM 2-methylthio-ADP (2MeSADP). Calcium flux was determined by fluorometry in 4×107 washed, Fluo3-AM loaded platelets following stimulation with 1.0 μM 2MeSADP. mRNA was extracted from 109 platelets using Oligo-dT Dynabeads in five of the subjects. RT-PCR was performed using primers specific to the P2Y1 and GAPDH (control) genes. Relative levels of P2Y1 cDNA were measured by spot densitometry, after gel electrophoresis of PCR products and normalised against GAPDH. Sequencing of the promoter of the P2Y1 gene was undertaken to identify sequence variation linked to the P2Y1 1622 SNP.
Results: GG homozygotes had significantly greater maximal aggregation response to 160 nM 2MeSADP compared to AA homozygotes (75.1% v 58.3%, p = 0.038). Calcium flux was also significantly greater in GG homozygotes (2.18 v 1.77 RFU, p = 0.041). Relative quantification of P2Y1 mRNA showed a two fold higher level in GG (n = 2) compared to AA homozygotes (n = 3). Several SNPs in the promoter region upstream of the P2Y1 gene were found to be in complete linkage disequilibrium with the 1622 A>G SNP.
Conclusion: Homozygosity for the P2Y1 1622 G allele is significantly associated with increased receptor signalling and platelet aggregation. An increase in P2Y1 transcript expression (or stability) is the likely mechanism for this effect. Candidate SNPs that could affect expression have been identified in the gene promoter. These findings may be important with regard to atherothrombotic risk.
198 VALUE OF HEART FATTY ACID BINDING PROTEIN (HFABP) FOR VERY EARLY DETECTION OF ACUTE MYOCARDIAL INFARCTION (AMI)
C. J. McCann, I. B. A. Menown, C. G. Owens, B. M. Glover, M. J. Moore, B. Smith, A. Tomlin, I. S. Young, A. A. J. Adgey.Royal Victoria Hospital, Belfast, UK; Craigavon Area Hospital, Craigavon, UK; Queens University, Belfast, UK
Background: Early detection of AMI remains suboptimal. ST elevation on the ECG has only 50–60% sensitivity. Cardiac troponin T (cTnT) does not reliably exclude AMI until 12 hours after symptom onset. We assessed if early detection of AMI would be improved by measuring hFABP (which like myoglobin rises rapidly but has higher cardiac specificity), and inflammatory and haemostatic markers.
Methods: We recruited prospectively 137 patients from August 2003 to February 2004 presenting to a coronary care unit with ischaemic type chest pain >20 minutes duration. Admission and 12-hour cTnT samples were obtained. Acute myocardial infarction was defined by elevated cTnT (>0.09 µg/l) on the 12-hour sample or both samples. Patients were assessed on admission for clinical characteristics (cardiac history, risk factors, tachycardia, killip class, shock), ECG features, haemostatic markers (d-dimer, fibrinogen), inflammatory markers (myeloperoxidase, white cell count, neutrophil count), and hFABP. The predictive value of abnormal clinical/ECG features and elevated biomarkers for evolving AMI were determined by univariate and stepwise multivariate regression analyses.
Results: Admission and 12-hour cTnT samples were obtained in 122 of 137 patients. Median time from pain onset to admission blood sampling was 3 hours. Acute myocardial infarction was confirmed in 63/122 (52%). Where initial cTnT was normal (24/63 (38%)), univariate predictors of AMI were elevated hFABP >5 μg/l (p = 0.002), shock (p = 0.04), and ST elevation >2 mm (p < 0.001). Other clinical/ECG characteristics and inflammatory/haemostatic biomarkers were not of predictive value. Using multivariate analysis, the predictive value of hFABP was independent of ST elevation (p = 0.04) or shock (p = 0.005). In the 24 patients with AMI where initial cTnT was normal, 14 had no ST elevation on initial ECG (58%). In these patients hFABP correctly detected evolving AMI in 11/14 (79% (p = 0.012)).
Conclusion: For patients presenting early after onset of chest pain, hFABP is of significant predictive value for detection of evolving AMI, which is independent of clinical and ECG findings as well as inflammatory and haemostatic biomarkers.
199 INFLAMMATION AND ACUTE HYPERGLYCAEMIA IN DIABETICS WITH NON-ST ELEVATION ACUTE CORONARY SYNDROMES (ACS). ANALYSES FROM OPUS TIMI 16 AND TACTICS TIMI 18
K. K. Ray, C. P. Cannon, J. Buros, A. Kirtane, E. Braunwald, C. M. Gibson.Brigham and Women’s Hospital, Boston, MA, USA; Harvard Medical School, Boston, MA, USA
Background: Inflammation and diabetes mellitus (DM) are independently associated with cardiovascular (CV) risk in ACS. In vitro glucose augments the adverse effects of C-reactive protein (CRP).
Methods: We hypothesised that DM would be associated with increased markers of inflammation and that inflammation would enhance the CV risk in DM. We analysed non-ST elevation ACS patients in the OPUS TIMI-16 trial and validated our results in the TACTICS-TIMI 18 trial (invasive arm). CRP was measured at 41 hours (mean) after ACS in OPUS and on admission in TACTICS.
Results: Median CRP was higher among diabetics (n = 541) v non-diabetics (n = 1659) in OPUS (9 v 7.8 mg/l, p = 0.002) and in TACTICS: diabetics (n = 267) v non-diabetics (n = 662) CRP 6.6 v 5.2 mg/l (p = 0.0005). Stratifying by population median CRP, diabetics with CRP < median were at similar risk of death or myocardial infarction (MI) to non-diabetics with CRP > median in OPUS (see fig). However, diabetics with CRP > median were at greatest risk of death or MI compared with all other groups (see fig). Identical observations were made in TACTICS. Among diabetics high glucose levels (tertile 3) increased the CV risk of a high CRP (see fig). In a Cox-regression model of death or MI, that included DM, glucose, and CRP, the interaction between glucose and CRP was an independent predictor of death or MI (p = 0.045).

Abstract 199
Conclusion: Diabetics have greater inflammation and hyperglycaemia may increase the CV risk associated with this. In diabetics with ACS future strategies that target better glycaemic control and that reduce inflammation, may reduce the CV risk in this high risk population
200 THROMBOGENICITY OF FLOWING BLOOD IS INCREASED IN PATIENTS WITH TYPE 2 DIABETES MELLITUS (T2DM) DESPITE TREATMENT WITH ASPIRIN
A. Natarajan1, S. Marshall2, J. Hanley3, J. J. Badimon4, A. Zaman1.1Department of Cardiology, Newcastle-upon-Tyne Hospital, UK; 2Department of Diabetes, Newcastle-upon-Tyne Hospital; 3Department of Haematology, Newcastle-upon-Tyne Hospital; 4Mount Sinai Medical Center, New York, USA
Introduction: Patients with atherothrombotic disease have worse immediate and late outcomes in the presence of T2DM. The CAPRIE study revealed elevated event rates in T2DM patients. Increased thrombogenicity has been reported to be contributory, mostly on the evidence of in vitro tests. We used the previously validated, ex-vivo, Badimon perfusion chamber (porcine aortic media as substrate) to compare thrombus burden in the presence of aspirin (ASA) in patients with T2DM and coronary heart disease (CHD) against normal controls.
Methods: Thrombus formation in 16 T2DM patients with overt CHD and risk factors (BMI>30, dyslipidaemia, hypertension) were studied. A further seven subjects without T2DM and no cardiovascular risk factors formed the control group. High shear rates were used (1690/s Reynolds number (re) = 60, flow rate 10 ml/min, average blood velocity 21.2 cm/s). Thrombus formed was fixed in formalin and stained with Masson’s trichrome stain. Thrombus burden was assessed by computerised planimetry using commercially available software (Image Pro-Plus, USA).
Conclusion: Our results show increased thrombus burden at high shear rates in patients with T2DM (on ASA) compared to controls (on ASA). In spite of effective secondary prevention the efficacy of aspirin in high risk T2DM patients is limited and could be a factor leading to increased recurrent ischaemic events. This suggests further exploration of the role of anti-thrombotics in patients with T2DM.
Abstract 200
201 USING A CORONARY HEART DISEASE (CHD) REGISTER TO SUPPORT EVIDENCE-BASED CARDIAC CARE IN GENERAL PRACTICE: LESSONS FROM THE SCOTTISH NATIONAL CHD DEMONSTRATION PROJECT
I. N. Findlay, A. M. Clark, M. Flood for the HaHP IT GroupRoyal Alexandra Hospital, Paisley, UK; University of Alberta, Edmonton, Alberta, Canada
Introduction: A significant proportion of the medical care of cardiac patients in general practice is not based on clinical evidence. Practices often lack the information management structures to rapidly evaluate provision of care or analyse its impact. A nationally innovative centralised regional computerised CHD register of those with or at risk of CHD has been developed in Scotland. This register can store, receive, and send information from a variety of national and local databases related to people with or at high risk of CHD. This information is accessed to support patient care in hospital, family practice, and patients’ homes, or for clinical audit.
Methods: To demonstrate the potential uses of the CHD register, we present an analysis of data recorded prospectively on the CHD register as part of routine clinical practice.
Results: Based on data for the Paisley region (n = 85 000), over the initial 14 months operation (September 2003–November 2004), the number of patients recorded in family practices as having CHD has increased by 839% (559 to 4694) of the local population). The percentage of these patients with smoking status recorded has risen during this period from 33% to 74% (p = 0.000), while current smokers with smoking status recorded has risen from 38% to 75%. The number of suitable patients prescribed beta blockers increased 700% (335 to 2347), though the recorded rate of patients prescribed these drugs fell significantly (60% to 50%) (p = 0.002). Similarly patients prescribed antiplatelets increased 826% (352 to 2910) but reported prescription rates remained similar (63% to 62%) (p = 0.317). The number of patients with cholesterol measurements recorded increased 857% (274 to 2347) but reported prescription rates demonstrated no significant change (49% to 50%) (p = 0.317). The number of patients on lipid lowering treatment increased 906% (347 to 3145) but did not increase significantly (62% to 67%) (p = 0.063).
Conclusion: A CHD register can allow rapid, efficient, and near real-time analysis of CHD populations and assessment of the provision of evidence-based care. In Paisley, while the number of CHD patients with key risk factors and medications recorded has increased dramatically, the register has identified that rates of evidence-based cardiac care have not increased.
202 USE OF REGIONAL GUIDELINES AND RAPID ACCESS TO CARDIAC CATHETER LABORATORIES FACILITATE EARLY INVASIVE MANAGEMENT IN PATIENTS WITH NON-ST SEGMENT ELEVATION ACUTE CORONARY SYNDROMES (NSTEACS)
P. Wong, A. Robinson, E. Rodrigues.Aintree Cardiac Centre, University Hospital Aintree, Liverpool, UK
Introduction: The Cheshire and Merseyside Cardiac Network has developed guidelines to stratify patients with NSTEACS into different risk categories by determining an acute coronary syndrome (ACS) score. Patients with ACS score ⩾9 (very high risk), and 6.5–8.5 (high risk) should be considered for coronary angiography (CA) during the index event, and those with ACS score 3–6 (intermediate risk) should be offered CA as soon as possible. We investigated the application of these regional guidelines in a secondary hospital, equipped with an on-site diagnostic cardiac catheter laboratory, and collaborated with the local tertiary hospital.
Methods: Patients admitted with NSTEACS and managed by a cardiologist during an 8-week period (5 January to 29 February 2004) were included. Acute coronary syndrome score of all patients were calculated by the presence of pre-specified event-related and pre-existing risk factors.
Results: A total of 76 patients were identified, of whom 56 (74%) were suitable for invasive management. Of these 56 patients, 12, 15, and 18 had ACS score ⩾9, 6.5–8.5, and 3–6, respectively. Coronary angiography was performed during the index event in all 12 (100%) very high risk patients. Fourteen of the 15 (93%) high risk patients had CA during the index event, and one patient had CA after discharge. Fourteen of the 18 (78%) intermediate risk patients had CA, 10 during the index event and a further four after discharge. Among the four remaining patients, one had recent percutaneous coronary intervention, one already had a recent CA, and one had a negative exercise test. In patients who underwent CA, cardiac interventions were performed in 10 (83%) very high risk, 13 (87%) high risk, and 10 (71%) intermediate risk patients, respectively. Twenty patients were not suitable for invasive management, and they had a higher mean ACS score than those suitable (8.4 + 3.0 v 5.8 + 3.5; p < 0.001).
Conclusion: The application of these regional guidelines successfully stratified NSTEACS patients into very high, high, and intermediate risk. Rapid access to either on-site diagnostic cardiac catheter laboratory or transfer to local tertiary hospital enabled CA to be performed early in suitable patients and resulted in high rates of cardiac interventions.
203 COMPLICATIONS OF DIAGNOSTIC CARDIAC CATHETERISATION (CC): RESULTS FROM A CONFIDENTIAL ENQUIRY INTO CC COMPLICATIONS
R. West, G. Ellis, N. Brooks on behalf of the Joint Audit Committee of BCS and RCP (London)University of Wales College of Medicine, Heath Park, Cardiff, UK
Objectives: To estimate the frequency and nature of complications in patients undergoing CC and to assess time trends in complications since the introduction of a voluntary system of co-operative audit.
Methods: Cardiac centres undertaking diagnostic CC in England and Wales from 1990 to 1999 participated in the study. Each centre reported numbers of patients catheterised each month and details of complications, as they occurred. Reports were scrutinised and complications classified into groups according to the most likely primary cause based on the original report (led by the late Professor David de Bono and published 1993).
Results: Forty-one centres contributed. 213 289 diagnostic procedures were registered in adults or adolescents and 5938 in patients <12 years. Eighty-nine percent of diagnostic catheter studies in adults were left heart studies with coronary arterioraphy. The second most common procedures were left and right heart studies, including coronary arteriography (10%). The overall complication rate for adult studies was 7.4 per 1000 with mortality at 0.7 per 1000. Arrhythmias represented the commonest reported group of complications (36%) with a relatively low case fatality of 4%. Vascular complications were the second commonest reported group of complications (22%) with a case fatality of 2%. Ischaemic complications were less common (11%) but accounted for a far larger proportion of deaths (case fatality rate 42%). Complication rates were lower in the last 2 years of the study and death rates declined across the whole 10 years.
Conclusion: Complication rates for diagnostic CC are low but neither negligible nor irreducible. Whilst voluntary audit of cardiac catheter complications is useful and inexpensive, there is a clear need to establish a formal reporting system in all cardiac catheter laboratories with clear definitions of reportable complications.
204 WHAT IS THE APPROPRIATE RATIO BETWEEN CORONARY ARTERY BYPASS GRAFT (CABG) AND PERCUTANEOUS INTERVENTION (PCI) IN THE DRUG ELUTING STENT ERA?
V. Ashar, A. P. Banning.Department of Cardiology, John Radcliffe Hospital, Headington, Oxford, UK
Introduction: The National Service Framework for Coronary Artery Disease gives target intervention rates of 750 procedures per million population for both PCI and CABG—that is, a ratio of 1:1 between these two methods of revascularisation. The advent of drug eluting stent (DES) has provided PCI as treatment option in previously excluded patient groups. We studied the impact of the introduction of DES on trends in coronary revascularisation in a single regional cardiac centre.
Methods and Results: Drug eluting stent were introduced in our hospital in January 2002. We analysed data from January 2001 to June 2004 from our database. All diagnostic procedures were identified and their management plans reviewed. The results are as shown in the figure. Following the introduction of DES, we observed that there was no significant increase in the total number of diagnostic angiograms performed. However, the proportion of patients referred for PCI has increased from 48% to 65%, and that referred for CABG has declined from 24% to 12%.

Abstract 204
Conclusion: Even before the introduction of primary PCI, DES technology has broadened the indications of PCI considerably. Reassessment of the optimum ratio between PCI and CABG is necessary, to ensure availability of appropriate facilities for patient management.
205 INTRODUCTION OF A RISK SCORING SYSTEM FOR PERCUTANEOUS CORONARY INTERVENTION (PCI) PROCEDURES
N. Silversides, S. Kennon, M. Rothman.Department of Cardiology, Barts and the London NHS Trust, London, UK
Background: Effective clinical governance requires interventional cardiologists monitor the number and outcome of procedures performed. Outcome data, however, should be viewed in the context of the risk and complexity of procedures.
Aims: To use an established risk scoring system to provide operators with data regarding the risk and complexity of PCI performed at our institution.
Methods: A number of risk scoring systems have been published. The Mayo Clinic Risk Scoring System (
) was selected because it is a simple integer system based on readily available data that predicts important end points and has been validated internally and externally on large cohorts of patients. Our PCI procedure database—based on the BCIS dataset—was modified to accommodate the required data points.
Outcome: Each month all operators are now provided with personal and institutional read outs documenting the number and risk profile of procedures performed over the last month, over the previous 12-month period, and all procedures since the inception of the database in October 2003. The read outs include the mean and maximum risk scores, the number of patients and complication rates in each risk group, and a break down of complications and of missing data fields. 3025 procedures have been entered into the database. The risk profile of our patients is lower than that described by the Mayo Clinic possibly due to delays between admission (with acute coronary syndromes) and PCI. Complication rates are lower than predicted for all risk groups. In-hospital outcome data is missing in 40% of cases partly due to the large (eight patients per day) day case transfer scheme where patients return to referring hospitals on the day of the procedure. Currently there is no way of ensuring that all procedures are entered into the database.
Conclusion: The Mayo Clinic Risk Scoring System provides useful information to interventional cardiologists regarding the complexity and pre-procedural risk of patients undergoing PCI. Systems are being put in place to ensure 100% data entry. When data entry is complete this risk scoring system should be validated on our cohort of patients.
206 DEMOGRAPHIC AND TEMPORAL TRENDS IN OUT-OF-HOSPITAL SUDDEN CARDIAC DEATH IN BELFAST
M. J. Moore1, B. M. Glover1, C. J. McCann1, N. A. Cromie1, P. Ferguson2, D. C. Catney2, F. Kee2, A. A. J. Adgey1.1Royal Victoria Hospital, Belfast, UK; 2Department of Epidemiology and Public Health, Queen’s University, Belfast, UK
Background: Although there has been a reduction in coronary artery disease (CAD) mortality over the last 30 years, any change in the incidence of sudden cardiac death outside hospital (SCDOH) is uncertain. In 1966 there were 297 CAD deaths outside hospital within 1 hour of symptom onset in Belfast city.
Methods: The population of Belfast in 1966 and 2001 was obtained from the census office. Prospective data were collected (1st August 2003 to 31st July 2004) for SCDOH in Belfast from four sources: mobile coronary care units, paramedic led ambulances, death certificates, and autopsy forms. We examined all SCDOHs using the Utstein style including call to response interval (CRI) for the emergency medical services (EMS). Resuscitation was defined as admission alive, and survival defined as discharged alive.
Results: There were 300 SCDOHs, 197 (66%) male: mean age 68 years (± SD14), (range 27 to 96), mean age of females 72 years (± SD13), and males 65 years (± SD14). Of SCDOH, 234 (78%) occurred at home, 47 (15.7%) in public places, and 19 (6.3%) in nursing homes. Two hundred and seventy-nine (93%) were attended by the EMS. Rhythm on EMS arrival was a systole 190 (68%), ventricular fibrillation (VF) 75 (27%), and pulseless electrical activity 14 (5%). Mean CRI was 8 minutes (± SD3). In those attended by the EMS, resuscitation was 9.7% and survival 7.2%. Presenting rhythm for all survivors was VF. Mean CRI for survivors was 5 minutes (± SD2) and non-survivors 8 minutes (± SD3), (p < 0.001). Ninety-one (30%) SCDOHs were witnessed; of these 48 (53%) had VF on EMS arrival. The survival rate for witnessed VF arrests was 20/48 (41.7%). All 20 survivors were witnessed, had VF as presenting rhythm, and CRI ⩽7 minutes. The European age-standardised incidence rate for SCDOH was 122/100 000 (95% CI 111 to 133) for males and 41/100 000 (95% CI 36 to 46) for females.
Conclusion: Despite a 37% reduction in CAD mortality in Ireland over the last 20 years, the incidence of SCDOH in Belfast has not fallen over the last 38 years. In this study, 78% of SCDOHs occurred at home. The percentage of cases with VF (27%) was low, possibly due to prolonged CRI, confirmed by the higher percentage of VF (53%) among witnessed arrests.
207 INITIAL RESULTS FROM THE NATIONAL DEFIBRILLATOR PROGRAMME (NDP)
M. Colquhoun, D. Chamberlain, S. Davies, R. Boyle.Wales Medical School, University of Cardiff, UK; Department of Health, London, UK
Public access defibrillation (PAD) with automated external defibrillators (AEDs) used by lay persons is one strategy to reduce the time to defibrillation in cases of sudden cardiac occurring in their vicinity. The NDP was established by the Department of Health (DH) to provide rapid defibrillation to victims of cardiac arrest occurring in busy public places. We report the initial results from the national programme covering 20 592 defibrillator months’ use between April 2000 and March 2004.
Methods: 681 AEDs were deployed at 110 sites identified as high risk from ambulance service data. Lay staff working at the sites were trained in basic life support and the use of AEDs. Utstein compatible data are reported for each resuscitation attempt made. After every resuscitation attempt a download of data stored electronically in the AED is analysed to determine cardiac rhythms and the response to shocks and other interventions.
Results: 172 resuscitation attempts were made during this period. A shockable rhythm was identified in 135 (78%) cases (ventricular fibrillation (VF) in 171, ventricular tachycardia (VT) in one) with shocks delivered an estimated 3–5 minutes after collapse. In this group, 38 patients (28%) survived to hospital discharge. Non-shockable rhythms were recorded in 37 cases; one survived. Irrespective of presenting rhythm, 39 of 172 (23%) survived. For witnessed cardiac arrests of presumed cardiac aetiology with a shockable rhythm (an Utstein international comparator), 37 of 124 (29.8%) survived.
Conclusion: The initial phase of the NDP has been implemented successfully with AEDs used successfully and appropriately by lay persons. The resuscitation rates are comparable with other reported PAD schemes. The provision of AEDs used by lay persons at high risk sites appears a successful strategy for saving victims of sudden cardiac death.
208 FALSE CARDIAC ARREST (FCA) CALLS–THE RIGHT TIME TO TURN AWAY?
S. Bradburn, A. Robinson, G. Kenwood, R. Steeds.Department of Resuscitation and Department of Cardiology, University Hospital (Queen Elizabeth), Birmingham, UK
Background: The Utstein template for in-hospital cardiac arrest defines a FCA as one for which no basic life support or advanced life support is needed. No further information is sought and there is little published information regarding outcome. This prospective audit was established to identify outcome for patients subject to FCA.
Methods: All cardiac arrest calls made to switchboard were logged on a daily basis over 6 months. An audit form was completed for each call by the senior medical practitioner attending and followed up by the RTO. Form retrieval over the period was complete. Data relating to Utstein survival (6 weeks or discharge from hospital) were obtained from the Patient Administration System (PAS).
Results: There were 72 FCA out of 251 arrests (29%), occurring at 9.7 ± 16 days following admission (mean age 64 ± 17 years, 38 (53%) were male). The most common reasons for FCA were: vasovagal syncope 19 (25%); deteriorated without arrest 13 (17%); and epileptic seizure 11 (14%). None died at the event (0%) but only 52 (72%) survived to discharge/6 weeks. This compares with the outcome for other cardiac arrests: VT/VF-32 (13%) arrests: 11 (34%) died at the event, 15 (47%) survived to discharge/6 weeks; PEA-56 (22%) arrests: 37 (66%) died at the event, one (2%) survived; a systole – 49 (20%): 39 (80%) died at the event, three (6%) survived; respiratory arrest – 42 (16%) arrests: none died at the event, 20 (48%) survived. The overall mortality rate for all hospital in-patients over the same period was 1.7%. Despite this adverse outcome, no action was taken following FCA in 49 (20% died); 17 were transferred to critical care (41% died); do not attempt resuscitation (DNAR) status was established in only three (all died); and immediate action was not known in three (all survived). Ten (7.2%) patients with an initial FCA suffered a further cardiac arrest with five (50%) then dying.
Conclusion: False cardiac arrest calls are common, occur relatively late in a hospital admission, and causality is often minimised. False cardiac arrests are followed by inaction, with low transfer rates and absence of DNAR classification despite having a high mortality and re-arrest rate. False cardiac arrests should be considered a “near miss” with patients then subject to close medical review.
209 DURATION OF CLOPIDOGREL THERAPY FOLLOWING PERCUTANEOUS CORONARY INTERVENTION (PCI) WITH BARE METAL (BMS) AND DRUG ELUTING STENTS (DES). A QUESTIONNAIRE SURVEY IN THE UK; DO WE NEED TO BE NICE?
M. Srinivasan, R. Anantharaman, A. Chauhan, D. H. Roberts.Blackpool Victoria Hospital, Blackpool, UK
Methods: A postal questionnaire was sent to 248 UK interventional cardiologists to evaluate the current prescribing practice for clopidogrel in relation to PCI using BMS and DES. 140 responses (56%) were received of which 123 (49.5%) were suitable for analysis.
Results: Our survey showed that 54% of UK interventionalists are using 300 mg loading dose for elective PCI with both stent types, whereas for acute coronary syndrome (ACS) intervention 52% of them are giving higher loading dose of 600 mg. The maintenance dose is universal at 75 mg. The maintenance treatment duration is longer with DES and in patients with ACS, but there is no clear consensus regarding the optimal duration of clopidogrel therapy for these patient groups. The duration of therapy was not influenced by the length or the diameter of the stented segments (see table).
Abstract 209
Conclusions: (1) Prescribing practice of clopidogrel for PCI by interventional cardiologists in the UK is variable at present and should be standardised and incorporated in the revised National Institute for Clinical Excellence (NICE) guidelines; (2) because of the problem of late thrombosis due to delayed endothelialisation with DES, we recommend at least 12 months duration especially for patients with ACS.
210 A RARE VARIANT OF THE LEPTIN (LEP) GENE HAS LARGE EFFECTS ON BLOOD PRESSURE (BP) AND CAROTID INTIMA-MEDIAL THICKNESS (CIMT): STUDY OF 1428 INDIVIDUALS IN 248 FAMILIES
H. Imrie, B. Mayosi, N. Gaukrodger, P. Avery, M. Baker, J. Connell, H. Watkins, M. Farrall, B. Keavney.University of Newcastle, Newcastle, UK; University of Oxford, Oxford, UK; University of Glasgow, Glasgow, UK; The Cardiac Clinic, New Groote Schuur Hospital, Cape Town, SA
Background: Rare mutations in the LEP gene cause severe obesity. Common polymorphisms of LEP have been inconsistently associated with obesity in previous studies, but their association with cardiovascular disease has been little studied. We have examined the impact of both common and rare polymorphisms of the LEP gene on BP, subclinical atherosclerosis as measured by CIMT, and body mass index (BMI) in a large family study.
Methods: Five polymorphisms spanning LEP were typed in 1428 individuals from 248 nuclear families. Blood pressure (using 24-hour ambulatory monitoring), CIMT, BMI, and plasma leptin were measured.
Results: The polymorphisms typed captured all common haplotypes present at LEP. There was strong association between a rare polymorphism in the 3′ untranslated region of LEP (C538T) and both pulse pressure (p = 0.0001) and CIMT (p = 0.008). C/T heterozygotes had a 22% lower pulse pressure and a 17% lower CIMT than C/C homozygotes. The polymorphism accounted for 3–5% of the population variation in pulse pressure and CIMT. There was no association between any LEP polymorphism and either BMI or plasma leptin level.
Conclusion: The rare LEP 538T allele substantially influences pulse pressure and CIMT, but does not exert this effect through plasma leptin level or BMI. Thus autocrine or paracrine effects in vascular tissue may be important physiological functions of leptin. More generally, rare polymorphisms of particular genes may have substantial effects within the “normal range” of quantitative risk factors.
211 IMPROVED SURVIVAL OF SYSTEMIC SCLEROSIS-ASSOCIATED PULMONARY ARTERIAL HYPERTENSION (SSC-PAH) IN THE ENDOTHELIN ANTAGONIST ERA
M. H. Williams, C. Das, C. E. Handler, M. R. Akram, J. Davar, C. P. Denton, C. J. Smith, C. M. Black, J. G. Coghlan.Departments of Cardiology, Academic Department of Rheumatology, and Population Sciences, Royal Free Hospital and UCL Medical School, London, UK
Background: Patients with SSc-PAH and severe symptoms have a very poor prognosis. Studies prior to the introduction of the endothelin-1 antagonists have failed to demonstrate an improvement in survival in this condition. The goal of this study was to compare survival in a cohort of patients with SSc-PAH receiving modern therapies with a matched historical control group (hcg).
Methods: This is a 6-year, observational, longitudinal study of 92 patients with SSc-PAH diagnosed by cardiac catheterisation. The patients were derived from a total population of 185 with SSc-PAH follow up between 1998 to 2004. The historical control group were those patients with SSc-PAH treated between 1998 and 2002 who met the criteria for treatment used in the bosentan group. They were matched with the bosentan group by previously defined haemodynamic predictors of mortality. Where clinically indicated, a prostanoid was used as advanced treatment. Bosentan was used as advanced treatment when it became available (bosentan-treated group). Survival was measured from the date of diagnosis of pulmonary hypertension using cardiac catheterisation. Six-minute walking distance and haemodynamics were measured at the time of diagnosis and at least 1 month after starting treatment.
Results: The historical control group comprised 47 patients, all of whom received basic therapy; 27 (57%) of these were treated with prostanoids. The bosentan-treated group comprised 45 patients who received bosentan as first-line disease modifying therapy. Kaplan-Meier survival in the historical control group was 68% at 1 year and 47% at 2 years. Survival in the bosentan-treated group was 81% and 71% (p = 0.016), respectively. The pulmonary vascular resistance increased in the historical control group whereas in the bosentan-treated group, it remained stable over an average of 9 months (p < 0.006).
Conclusion: Since the introduction of the non-selective endothelin antagonist—bosentan—survival of selected patients with SSc-PAH has improved. This improved survival is associated with stabilisation of cardiac haemodynamics.
212 EFFECTS OF BRADYKININ (BK) ON VENOUS CAPACITANCE IN HEALTH AND TREATED CHRONIC HEART FAILURE (CHF)
P. Gunaruwan, L. Williams, J. Sharman, M. Schmitt, L. Lee, R. Field, M. Frenneaux.Department of Cardiovascular Medicine, Medical School, University of Birmingham, Birmingham, UK
Background: The role of BK and of its receptor subtypes in determining basal venous tone in health and in CHF is unknown. We investigated the effects of basal and of infused BK on unstressed forearm vascular volume (FVV; a measure of venous tone) and blood flow (FBF) in healthy subjects (G1) and in CHF patients treated with angiotensin converting enzyme inhibitors (ACEI) (G2) and angiotensin II receptor antagonists (ATIIRA) (G3).
Methods and Results: We studied 20 healthy controls (G1), 16 CHF patients treated with ACEI (G2), and seven CHF patients treated with ATIIRA (G3). We used standard strain gauge plethysmography and radionuclide plethysmography (combined blood pool scintigraphy and venous occlusion plethysmography) to examine the effects of BK and of the BK antagonists B9340 (Type B1 and B2 antagonist) and HOE140 (specific Type B2 antagonist) on FVV and FBF. Following intra-brachial incremental BK infusions at 30 and 300 pmol/min either B9340 or HOE140 at 13.5 nmol/min was then co-infused with BK at 300 pmol/min. After a 0.9% saline wash out either B9340 or HOE140 at 13.5 nmol/min was then infused alone. Bradykinin increased FVV in a similar dose dependent manner in G1 and G3 (G1 maximum 12.3 ± 2.1%; p < 0.001 v baseline, G3 maximum 7.4 ± 3.9%; p < 0.05 v baseline, p = NS for difference) but the increase in FVV in G2 was significantly higher (maximum 28.8 ± 7.8%; p < 0.001 v baseline; p < 0.05 for the difference between groups). In contrast, while the increase in FBF in G1 (maximum 362 ± 9%; p < 0.001) and in G2 (maximum 376 ± 12%; p < 0.001) was similar (p > 0.05 for the difference between groups), the increase in G3 was significantly less (maximum 278 ± 10%; p < 0.001; p < 0.05 for the difference between groups). Bradykinin effects were antagonised to a similar extent by both B9340 and HOE140 in all three groups. Infusion of each receptor antagonist alone reduced basal venous volume and blood flow in G2 but not in G1 or G3.
Conclusion: Bradykinin does not contribute significantly to basal venous tone in healthy subjects, but in ACEI treated CHF patients it does. This effect is mediated via the Type B2 receptor. In ATIIRA treated heart failure venous responses to BK are preserved but arterial responses are reduced compared with healthy controls.
213 AUTONOMIC REMODELLING IN HYPERTENSION FOLLOWING CARDIAC NEURAL NITRIC OXIDE SYNTHASE (nNOS) GENE TRANSFER
D. A. Heaton, M. Lei, P. Noble, S. Golding, D. J. Paterson.Burdon Sanderson Cardiac Science Centre, University Laboratory of Physiology, Oxford, UK
Background: Hypertension is associated with decreased nitric oxide (NO) bioavailability, cardiac â-adrenergic hyper-responsiveness, and tachycardia; hyper-responsiveness may occur at the level of the L-type calcium current (ICaL), since ventricular myocytes from the spontaneously hypertensive rat (SHR) exhibit elevated ICaL. We tested the hypothesis that nNOS gene transfer to the sino-atrial node (SAN) would normalise â-adrenergic chronotropic responsiveness in the SHR, since ventricular myocytes from the nNOS knockout mouse show increased calcium current density and enhanced responsiveness to â-stimulation.
Methods: Gene transfer to the right atrium was performed in 20–24-week old SHRs and normotensive (WKY) rats, using 5e10 particles of adenoviral vector encoding nNOS (Ad.nNOS) or enhanced green fluorescent protein (Ad.eGFP). Heart rate (HR) responses to noradrenaline (NA; 0.1–5.0 µM) were measured after 5 days in isolated atria, and ICaL was recorded in SAN cells.
Results: Immunoblotting showed increased nNOS expression in Ad. nNOS-transfected atria. Furthermore, fluorescence microscopy indicated expression of eGFP in both SAN sections and myocytes. A comparison of HR responses to NA in eGFP-transfected SHR (n = 20) and WKY (n = 6) atria confirmed â-adrenergic hyper-responsiveness in the SHR (e.g. 0.1µM: 66 ±7 beats per minute (bpm) v 25 ± 5 bpm (WKY), p < 0.01). Furthermore, SAN cells of the SHR (n = 4) showed increased peak amplitude of both basal (26.6 ± 5 v 7.9 ± 1.1 pA/pF, p < 0.001) and NA-stimulated ICaL (54 ± 9.6 v 17.2 ± 3.5 pA/pF, p < 0.05) relative to the WKY (n = 4). Ad. nNOS (n = 8) blunted responses of SHR atria to NA relative to the Ad. eGFP group (0.1µM: 22 ± 8 v 66 ± 7 bpm, n = 20, p < 0.01), and normalised responsiveness of the SHR relative to the WKY. This was partially reversed by NOS inhibition. Basal ICaL was unaffected by nNOS gene transfer. However, the NA-induced increase in ICaL was significantly attenuated (+41.4 ± 8% v +103.5 ± 8.4%, p < 0.01, n = 4).
Conclusion: Increased nNOS expression normalises â-adrenergic hyper-responsiveness by attenuating ICaL in the SHR. Cardiac nNOS gene transfer may therefore provide a novel intervention for correcting peripheral autonomic imbalance in hypertension.
214 GENETIC VARIATION AT THE LOCUS ENCOMPASSING 11-BETA HYDROXYLASE AND ALDOSTERONE SYNTHASE ACCOUNTS FOR HERITABILITY IN CORTISOL PRECURSOR (11-DEOXYCORTISOL) URINARY METABOLITE EXCRETION
H. Imrie, B. M. Mayosi, M. Baker, R. Fraser, E. Davies, M. Ingram, H. Watkins, M. Farrall, J. Connell, B. Keavney.University of Newcastle, Newcastle, UK; University of Oxford, Oxford, UK; University of Glasgow, Glasgow, UK; The Cardiac Clinic, New Groote Schuur Hospital, Cape Town, SA
Background: Genetic variation in the gene encoding aldosterone synthase (CYP11B2) has previously been shown to be associated with hypertension and left ventricular hypertrophy, though not in all studies. The intermediate phenotype most consistently associated with variation in this gene is that of elevated plasma 11-deoxycortisol. However, aldosterone synthase does not metabolise 11-deoxycortisol, which is converted to cortisol by the enzyme 11-beta hydroxylase, encoded by the gene CYP11B1, which lies adjacent to CYP11B2 on chromosome 8. We hypothesised that the QTL for the phenotype lies within CYP11B1, and that linkage disequilibrium across the extended locus accounted for these previous observations.
Methods: We genotyped six polymorphisms in the CYP11B2 gene and three polymorphisms in the CYP11B1 gene in 248 Caucasian nuclear families comprising 1428 individuals, and measured plasma levels of deoxycortisol (S) and cortisol (F), and urinary excretion rates of tetrahydrodeoxycortisol (THS) and tetrahydrodeoxycorticosterone (THDOC). We examined heritability of the phenotypes, and their association with genotypes and haplotypes at this locus.
Results: All steroid phenotypes with the exception of urinary THDOC were highly heritable (p < 0.00001). There was strong linkage disequilibrium across the CYP11B1/B2 locus. There was strong evidence for association between polymorphisms of both CYP11B1 and CYP11B2 and urinary THS, which is a measure of 11-hydroxylation. The association was strongest for the CYP11B1 exon 1 polymorphism (p = 0.00002). Addition of other marker data to CYP11B1 exon 1 did not improve the model’s fit. Genotype at CYP11B1 exon 1 explained ∼5% of the variance in urinary THS excretion in the population.
Conclusion: Genotype at an exonic polymorphism of CYP11B1 accounts for a small but definite difference in 11-beta hydroxylation. Further fine mapping and functional studies of the CYP11B1 locus are required to confirm the causative variant(s) for the biochemical phenotype; this may also identify susceptibility alleles for hypertension and left ventricular hypertrophy at this locus.
215 EFFECTS OF AMILORIDE AND SPIRONOLACTONE ON QT IN STROKE SURVIVORS–A RANDOMISED PLACEBO CONTROLLED DOUBLE-BLIND CROSS OVER STUDY
K. Y. K. Wong, S. Y. S. Wong, S. McSwiggan, S. A. Ogston, R. S. MacWalter, A. D. Struthers.The Tayside Institute of Cardiovascular Research, University of Dundee Medical School, Ninewells Hospital, Dundee, UK
Introduction: QT prolongation is associated with cardiovascular death. Potassium deficiency could contribute to QT prolongation, cardiac dysrhythmias, and sudden death. Therefore, increasing plasma potassium might be a useful way of reducing prolonged QT interval. Therefore, we tested the hypothesis that QTc and brain natriuretic peptide (BNP) might be reduced by oral spironolactone or amiloride.
Methods: Twelve stroke survivors already on an angiotensin-converting enzyme (ACE) inhibitor or an angiotensin II receptor blocker were recruited into a randomised, double-blinded, placebo-controlled, two-way cross over trial, with 1 month each of spironolactone, amiloride, and placebo. QTc was measured in lead III and was heart rate corrected using Bazett’s formula by a single observer blinded to BNP results and medication the patient was on. Main outcome measures were QTc and BNP.
Results: Both active treatments significantly shortened QTc (mean QTc change for spironolactone −18.2 ms, 95% CI −35.8 to −0.55, p = 0.043 v amiloride −24.7, 95% CI −41.9 to −7.5, p = 0.006); and increased potassium (mean for spironolactone +0.42 mmol/L v amiloride +0.66 mmol/l, p < 0.001). Amiloride significantly lowered BNP (−3.9 pg/ml, p = 0.042).
Conclusion: Both amiloride and spironolactone reduced QTc by increasing plasma potassium. In addition, amiloride significantly improved BNP in stroke survivors.
216 THE CARDIOVASCULAR EFFECTS OF INTRAVENOUS CORTICOTROPHIN RELEASING HORMONE (CRH) IN HEALTHY VOLUNTEERS
M. Lencioni, H. Randeva, M. Been.University Hospitals Coventry and Warwickshire, Coventry, UK; University of Warwick, Coventry, UK
Introduction: Corticotrophin releasing hormone type 2 receptor has been isolated in animals and humans in myocardium and vasculature. Stimulation of this receptor in animals increased myocardial contractility and produced vasodilatation. At present it is not known how CRH alters haemodynamic parameters in man. Therefore we investigated the early effects of an acute intravenous bolus injection of CRH on myocardial contractility and vasodilatation in man.
Methods: Ten healthy volunteers (age 23–45 years; six males, four females) were randomly assigned in a single blinded cross over study to a CRH- (100 μg) and placebo-arm. Haemodynamic and ECG parameters were continuously recorded 15 minutes prior and up to 30 minutes after bolus injection of CRH. Sympathetic activity was measured by heart rate variability (HRV).
Results: Cardiac index (CI) increased significantly after 60 seconds (4.4 = ± 0.27 v 3.4 ± 0.22 l/min/m2; p < 0.05) with a maximum after 5 minutes (4.6 ± 0.4 v 3.3 ± 0.2; p < 0.05) compared to placebo caused by an increase in myocardial contractility by a significant shortening of left ventricular ejection time (LVET) within 30 seconds and vasodilatation with a significant decrease of total peripheral resistance (TPR) within 60 seconds. SI and heart rate significantly increased with a maximum after 5 minutes. The time course of increased SA did not correlate with the change in LVET.
Conclusion: Corticotrophin releasing hormone results in a significant increase in CI mediated at least in part by a direct activation of myocardial contractility as well as vasodilatation. Additionally CRH resulted in an increase in sympathetic activity.
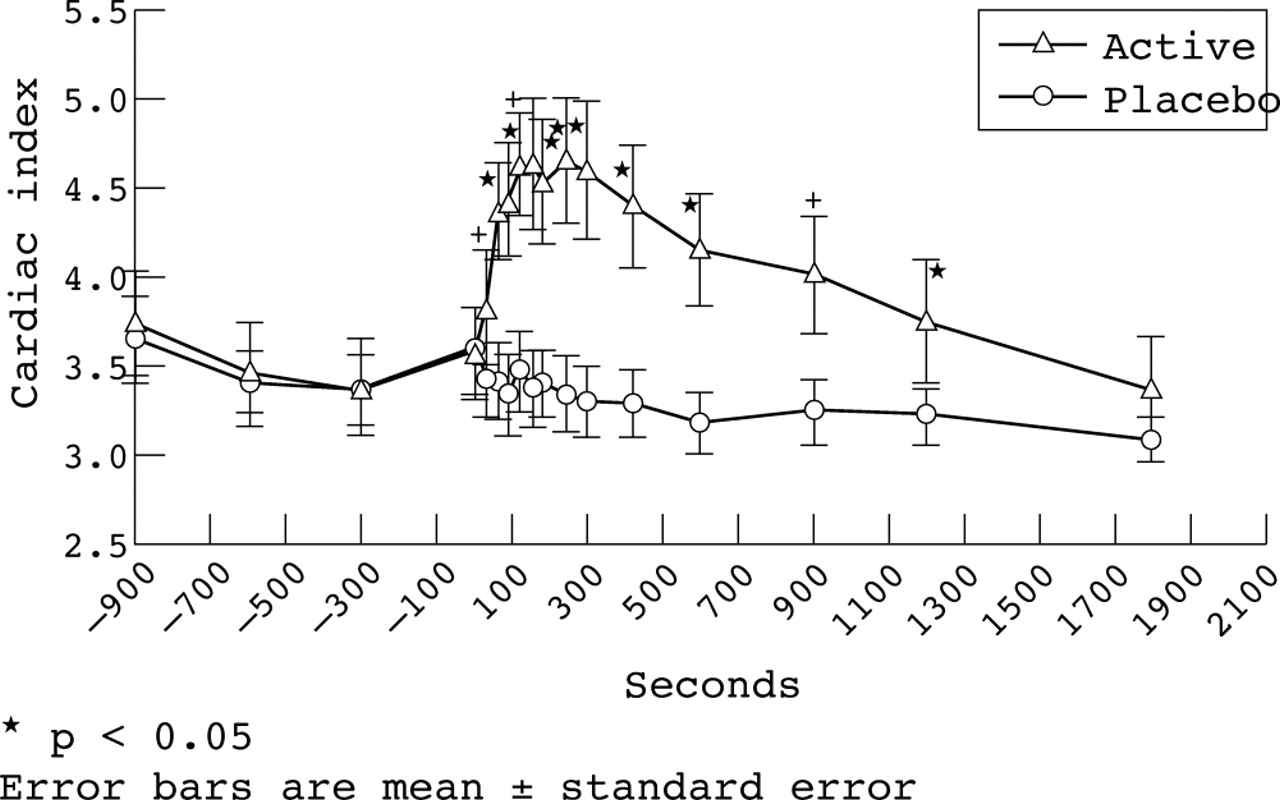
Abstract 216
217 INCREASED ARTERIAL STIFFNESS IN HEALTHY YOUNG SOUTH ASIAN MEN
J. N. Din, O. A. Ashman, S. M. Aftab, A. W. Jubb, D. E. Newby, A. D. Flapan.Centre for Cardiovascular Sciences, University of Edinburgh, Royal Infirmary of Edinburgh, Edinburgh, UK
Background: Coronary heart disease (CHD) mortality is higher in South Asians compared with European Caucasians. This is not fully explained by differences in traditional cardiovascular risk factors. The augmentation index (AIx) is a non-invasive measure of arterial stiffness and is associated with increased cardiovascular risk. This study assessed whether healthy South Asian males have greater arterial stiffness than Caucasians.
Methods: We recruited 20 healthy South Asian males (both parents from Indian subcontinent) and 20 healthy indigenous European Caucasian males. Arterial stiffness was assessed using applanation tonometry of the radial artery. The augmented pressure (AP) was the difference between the first and second systolic peaks. The AIx was the AP expressed as a percentage of the pulse pressure. Continuous variables are mean ± SEM.
Results: The South Asians and Caucasians were young (23.3 ± 0.7 v 23.1 ± 0.6 years, p = 0.8) and well matched for basal metabolic rate (BMR), smoking, glucose, lipids, and heart rate. Both groups were normotensive. South Asians had a higher AIx (2.68 ± 2.0 v −5.70 ± 1.8%, p = 0.0032) and AP (1.35 ± 0.8 v −1.93 ± 0.6 mm Hg, p = 0.0017) compared with Caucasians. As AIx varies with heart rate this was corrected for, and the derived AIx remained higher in the South Asians (−2.65 ± 2.0 v −12.35 ± 1.7%, p = 0.0007).
Conclusion: We have demonstrated for the first time that healthy young South Asian men have an increased AIx and AP in relation to matched Caucasians. This suggests greater arterial stiffness and may represent an important and previously unreported mechanism contributing to their increased cardiovascular risk.

Abstract 217
218 EFFECT OF NITRATE ADMINISTRATION ON WAVE SPEED PROPAGATION IN THE HUMAN CORONARY ARTERY
J. Davies, Z. Whinnett, D. Francis, K. Willson, R. Foale, I. Malik, S. Thom, A. Hughes, K. Parker, J. Mayet.Imperial College, International Centre for Circulatory Health, St Mary’s Hospital, London, UK
Background: Arterial wave speed, an established predictor of coronary artery disease, can be assessed in the aorta using the timing of the blood pressure waveform at two points. It is difficult to apply such techniques to the coronary arteries, as they are short and inaccessible. We present a method to measure human coronary artery wave speed for the first time and apply it to assess the effect of intracoronary nitrates.
Method: In nine subjects with normal coronary angiograms, we measured simultaneous pressure and Doppler flow with intracoronary wires, at the left mainstem and at intervals along the aorta before and after administration of 1 mg of intracoronary isosorbide dinitrate. Aortic wave speed was derived in two ways: first, by the transit time/distance method based on foot to foot delay of pressure waveforms at two sites; second, by a new method that analyses pressure-flow interactions.
Results: In the aorta estimates of wave speed by the two methods correlated well (r = 0.75, p = 0.01) and there was also close agreement between aortic and coronary wave speed (r = 0.79, p = 0.001). Following nitrates, coronary wave speed estimated by the pressure-velocity method fell by 43% from 15.38 ± 5.4 m/s to 8.7 ± 4.3 m/s, p < 0.001 (see fig).

Abstract 218
Conclusion: We have validated a new method of measuring arterial wave speed using simultaneous pressure and velocity that enables human coronary arteries to be studied. We have demonstrated the long-assumed relationship between coronary and aortic wave speed, and found that coronary wave speed is reduced by nitrates.
219 INFLAMMATORY GENOTYPES PREDISPOSING TO PREMATURE CORONARY ARTERY DISEASE (CAD) IN A LARGE DISCORDANT SIBSHIP COLLECTION AND UTILITY AS RISK PREDICTORS
B. D. Brown, R. A. Lawrance, L. Steiner, A. J. Balmforth, A. S. Hall.Institute for Cardiovascular Research, Leeds General Infirmary, Leeds, UK
Background: An increasing body of evidence supports the role of inflammation in the development and complications of atherosclerosis. To date, it remains less clear whether this observation represents cause or effect. We believe one possible solution is to investigate the genetic substrate in affected individuals.
Aims: Evaluate the role of 50 variants in candidate genes of cellular adhesion, chemotaxis, and cellular signalling in a large discordant sibship population.
Methods: Using a multilocus assay we evaluated the genotype frequency of 2875 individuals in 930 discordant sibships affected by premature CAD (myocardial infarction (MI)/percutaneous coronary intervention (PCI)/coronary artery bypass graft surgery (CABG)/angina prior to 66th birthday). After checking for genotype errors using the Graphical Representation of Relationships software data was analysed using the family based association test (FBAT).
Results: Examination for genotyping errors identified several monozygotic twin pairs and one half sibling. These families were excluded from further analysis. Allele frequencies in cases and controls were in Hardy-Weinberg Equilibrium (if rare allele frequency >1%). We observed the following significant associations: IL4R Ser478Pro (p = 0.023); IL9 Thr113Met (p = 0.033); IL1 alpha Thr549Cys (p = 0.018); C5 Ile802Val (p = 0.021). 34.2% of unaffecteds compared to 40.2% affecteds had ⩾3 of the four alleles associating with disease (p = 0.003). In a binary logistic regression model, with affected status as the dependent variable, possessing ⩾3 of the disease alleles increased the risk of developing disease by 32.0% (95% CI 1.046 to 1.666; p = 0.019).
Conclusion: We have identified four polymorphisms of inflammatory gene variants that are significantly associated with CAD. Our large family based cohort provides the power to detect an effect if present but also avoid false positive results attributable to population admixture. Furthermore, we have demonstrated how this knowledge can be combined to form the basis of a clinically useful tool.
220 CARDIOVASCULAR EFFECTS OF EXPOSURE TO AIR POLLUTANTS–HUMAN EXPOSURE STUDIES DEMONSTRATING AN ADVERSE INFLUENCE ON HEART RATE VARIABILITY (HRV)
H. C. Routledge1, J. G. Ayres2, J. N. Townend1.1University of Birmingham, Birmingham, UK; 2University of Aberdeen, Aberdeen, UK
Background: Epidemiology clearly demonstrates an association between cardiovascular mortality and daily changes in levels of particulate and gaseous air pollutants. One mechanistic hypothesis is that air pollutants cause a disturbance in cardiac autonomic control increasing the susceptibility to lethal arrhythmia. This is the first human challenge study designed to measure the cardiac autonomic response of individuals to controlled concentrations of two common air pollutants under laboratory conditions.
Methods: In a random order, double blind, four-way cross over study, 20 healthy volunteers and 20 patients with coronary disease were exposed for 1 hour to clean air, carbon particles and/or sulphur dioxide (SO2), at concentrations found during pollution episodes. Heart rate variability was measured before, immediately after, and 4 hours after exposure under controlled conditions including fixed respiration.
Results: No significant adverse changes were seen in HRV following exposure to carbon particles alone. Four hours following SO2 exposure in healthy volunteers, there were significant reductions in HRV indices of cardiac vagal control (repeated measures analysis, p < 0.05).
Conclusion: The increase in cardiac death observed during pollution episodes may be in part due to an adverse effect of SO2 on cardiac autonomic control.
Abstract 220
221 TRANSMURAL EXTENT OF INFARCTION ON CONTRAST ENHANCED MAGNETIC RESONANCE IMAGING (CE-MRI) PREDICTS RECOVERY OF CONTRACTILE FUNCTION IN PATIENTS WITH FIRST MYOCARDIAL INFARCTION TREATED WITH THROMBOLYSIS
J. L. Barclay, M. Egred, K. Kruszewski, R. Nandakumar, M. Y. Norton, T. Redpath, S. Walton, G. S. Hillis.Cardiology Department, Aberdeen Royal Infirmary and MRI Research Department, University of Aberdeen, Aberdeen, UK
Background: Delayed enhancement on CE-MRI has been shown to be of value in predicting functional recovery of left ventricular contraction after myocardial infarction in successfully revascularised patients. The aim of this study was to assess the utility of CE-MRI in a cohort of patients with acute myocardial infarction treated with thrombolysis.
Methods: Nineteen patients presenting with their first ST elevation myocardial infarction underwent cine and CE-MRI with evaluation of first pass perfusion and delayed enhancement within 7 days of admission. Cine magnetic resonance imaging (MRI) was repeated 8 weeks later. The transmural extent of infarction was determined from the first scan using a 60 segment model. Myocardial perfusion was assessed using a quantitative Patlak method. Wall thickening score was assessed on a segmental basis from both cine scans.
Results: A total of 396 of 1140 segments were dysfunctional on scan 1. Improvement in segmental wall motion was inversely related to the transmural extent of delayed enhancement both for all dysfunctional segments and those with severe dysfunction. There was no significant correlation between improvement in global contractile function and infarct size on MRI (p = 0.332) or 12-hour serum Troponin I (p = 0.610). Wall motion abnormalities were accompanied by perfusion defects in 15 of the 19 patients. Complete recovery in contractile function was observed in three of the four patients who did not have a corresponding perfusion defect.
Conclusion: The transmural extent of infarction determined from CE-MRI is predictive of recovery of contractile function in patients thrombolysed for first ST-segment elevation MI (STEMI). First pass perfusion data appear to add incremental predictive value to late enhancement. The results of this study indicate that CE-MRI may have utility in thrombolysed patients who have not necessarily had angiography.
222 DOBUTAMINE STRESS ECHOCARDIOGRAPHY (DSE) AND THE RESTING BUT NOT EXERCISE ELECTROCARDIOGRAPH (ECG) PREDICT SEVERE CORONARY ARTERY DISEASE (CAD) IN END STAGE RENAL FAILURE
R. Sharma1, D. Pellerin2, D. C. Gaze1, J. S. Shah2, C. P. Streather1, P. O. Collinson1, S. J. Brecker1.1St. George’s hospital, London, UK; 2The Heart Hospital, London, UK
Introduction: The detection and treatment of severe CAD is advocated in all renal transplant candidates. The aim of this study was to identify non-invasive predictors of severe CAD in a group of end stage renal disease (ESRD) patients.
Methods: 125 renal transplant candidates (mean age 52 ± 12 years; 80 male; mean creatinine 608 ± 272 μmol/l) were studied. All had coronary angiography, DSE, and ECG testing. Severe CAD was defined as luminal stenosis >70% by visual estimation in at least one epicardial artery. The resting ECG was recorded as abnormal if there was evidence of pathological Q waves, left ventricular hypertrophy, ST depression or elevation >1 mm, T wave inversion, or bundle branch block. Total exercise time, maximal ST segment change, maximal heart rate and systolic blood pressure, limiting symptoms, and Duke score were calculated during the exercise ECG test. Standard cardiovascular risk factors were documented. Haematological and biochemical parameters recorded.
Results: Thirty-six patients (29%) had severe CAD. Fifty-four percent were on dialysis and 39% diabetic. Patients with severe CAD were significantly older (58 ± 9 v 49 ± 13 years, p < 0.001), had higher total cholesterol (p 0.05), higher CRP level (p = 0.05), larger left ventricular (LV) end systolic and end diastolic diameter (p 0.007 for each), and lower LV ejection fraction (p 0.01). A significantly higher percentage were diabetic (p 0.05), had previous graft failure (p 0.05), mitral annular calcification (p 0.04), an abnormal resting ECG (p 0.001), and positive DSE result (p < 0.001). Cardiac symptoms and exercise ECG parameters were not significantly different in the two groups. Stepwise logistic regression identified an abnormal resting ECG (OR 7; 95% CI 2 to 34; p 0.013) and positive DSE result (OR 23; 95% CI 6 to 88 ; p < 0.001) as independent predictors of severe CAD.
Conclusion: In selecting which potential renal transplant candidates should undergo coronary angiography, the resting but not exercise ECG and DSE are the best predictors of severe CAD.
223 THE IMMEDIATE AND 2-YEAR OUTCOMES OF ENHANCED EXTERNAL COUNTERPULSATION (EECP) IN THE TREATMENT OF CHRONIC REFRACTORY ANGINA–A UK PERSPECTIVE
P. H. Loh, J. Windram, A. Louis, E. Kennard, A. Rigby, J. Cook, S. Kelsey, N. Nikitin, J. Cleland.International EECP Patient Registry (IEPR), Hull Royal Infirmary, University of Hull, Hull, UK
Introduction: The role of EECP in treatment of chronic refractory angina is currently under review by the UK National Refractory Angina Group. It has been widely available in America and China but the experience in the UK and Europe remains limited.
Method: We compared the immediate and 2-year outcomes of 53 consecutive patients treated with EECP in our centre [H] to those of 1490 patients registered in the International Patient Registry 1 (IEPR1) [I].
Results: [H] and [I] were comparable in age (66 years), left ventricular ejection fraction (LVEF) (48% v 46%), and history of prior myocardial infarction (MI, 72% v 71%), percutaneous or surgical revascularisation (percutaneous coronary intervention (PCI) or coronary artery bypass graft (CABG), 81% v 89%) and heart failure (25% v 35%). More [H] were males (89% v 73%, p = 0.012), had multivessel coronary disease (96% v 71%, p < 0.001) with longer duration of disease (14 years v 11 years, p < 0.005). Hypertension, hyperlipidaemia, and diabetes were more prevalent in [I]. Fewer [H] had Canadian Cardiovascular Society (CCS) III/IV angina (57% v 90%, p < 0.001) but on-demand glyceryl trinitrate (GTN) usage and mean weekly angina were similar to [I] (83% v 75% and 12 episodes/week respectively). Though more [H] completed a mean treatment course of 34 hours (94% v 82%, p < 0.05), both groups had a comparable and significant reduction in angina severity (CCS reduced by one grade or more in 83% [H] v 74% [I]), angina frequency (mean reduction by nine episodes/week) and GTN usage (49% [H] v 39% [I]). Major adverse cardiovascular event (MACE: death/CABG/PCI/MI) were <3% in both groups during treatment period. Eighty-seven percent of both groups completed 2-year follow up. Angina remained at least one CCS grade better in 79% of the patients in both groups with comparable and significantly lower angina frequency (four episodes/week) and GTN usage (54% [H] v 48% [I]). The cumulative MACE rate was 29.1% in [I], which was comparable to that of [H]. Major adverse cardiovascular event-free survival was 80% in [H] and 74% in [I], p = NS.
Conclusion: Data from the International EECP Patient Registry appears applicable to patients in the UK. The benefits of a course of EECP appears to be sustained for at least 2 years for the majority of patients.
224 ENHANCED EXTERNAL COUNTERPULSATION (EECP) IMPROVES ANGINA CONTROL AND EXERCISE TOLERANCE IN PATIENTS WITH CHRONIC STABLE REFRACTORY ANGINA
P. H. Loh, A. Louis, J. Windram, J. Cook, A. Rigby, J. Bryce, L. Ingle, N. Nikitin, J. Cleland.Hull Royal Infirmary, Hull, UK; University of Hull, Hull, UK
Introduction: The ESC Joint Study Group on the treatment of refractory angina has highlighted the growing number of patients suffering from this condition. There is little consensus in which treatment should be offered. Enhanced external counterpulsation is a potential, relatively inexpensive and non-invasive treatment for these patients.
Method: We report the immediate and medium-term outcome of 68 patients who had EECP for the treatment of refractory angina. They received 35 ± 5 hours of treatment over 43 ± 12 days.
Results: Ninety percent were males. The mean age was 66 ± 6 years and left ventricular ejection fraction (LVEF) was 48 ± 15%. Ninety-seven percent had multivessel coronary disease for a mean of 14 ± 6 years. Eighty-two percent had a prior percutaneous or surgical revascularisation (percutaneous intervention (PCI) or coronary artery bypass graft (CABG)). Forty-seven percent had Canadian Cardiovascular Society (CCS) III or IV angina and 82% were considered unsuitable for further PCI or CABG. Immediately post-EECP, angina frequency was reduced from 12.6 ± 13.5 to 2.7 ± 5.6 episodes/week, p < 0.001, and glyceryl trinitrate (GTN) usage from 13.5 ± 17.0 to 2.8 ± 6.7 times/week, p < 0.001. Angina severity was improved by at least one CCS grade in 79% of the patients. Thirty-four percent of them were free of angina and only 9% had CCS III/IV angina, p < 0.001. After a mean follow up of 207 ± 90 days, the angina frequency and GTN use remained significantly improved at 3.4 ± 5.2 episodes/week and 3.3 ± 5.5 times/week, respectively, p < 0.001. Twenty-one percent of the patients were free of angina and 8% had CCS III/IV angina, p < 0.001. Seventy-four percent had exercise treadmill tests and their mean exercise time improved significantly from 302 ± 129 to 378 ± 150 seconds immediately post-EECP, p < 0.001. This was sustained in the 72% who had a repeat test within 6 months (418 ± 149 seconds, p < 0.001). Only four patients failed to complete the treatment due to myocardial infarction (MI) in one, non-cardiac chest pain in one, and pacemaker interference in two. The cumulative rates for unstable angina, PCI, CABG, worsening heart failure, arrhythmia, and death were 7%, 2%, 2%, 3%, and 2%, respectively.
Conclusion: Enhanced external counterpulsation is safe and effective in reducing angina and GTN requirement in patients suffering from chronic refractory angina with an objective improvement in exercise tolerance. The effect is achieved immediately after the treatment and sustained during medium-term follow up.
225 ELECTIVE CORONARY ANGIOGRAPHY BY NON-MEDICAL ANGIOGRAPHERS. A COMPARISON WITH CARDIOLOGY SPECIALIST REGISTRARS
J. L. Caplin, M. Whitehead, J. Lavender.Hull and East Yorkshire NHS Trust, Hull, UK
The introduction of the European Working Time Directive has significantly reduced the availability of cardiology specialist registrars to perform diagnostic coronary angiography, impacting adversely on waiting times. We piloted a new role of non-medical coronary angiography practitioners. An experienced cardiac catheterisation laboratory nurse and radiographer took part. We report the results from their first 116 patients, and compare the results with 128 patients performed by specialist registrars over the same period of time. All patients admitted for elective day-case coronary angiography for possible ischaemic heart disease, without previous coronary artery surgery or known peripheral vascular disease, were eligible for the study. We collected data on success rates, screening times, complications, and diagnostic quality. None of the 116 procedures performed by the non-medical angiographers were unsucessful, and only one of the 128 procedures performed by specialist registrars was unsuccessful. The mean ± SD screening times was 4.1 ± 2.5 minutes for non-medical angiographers and was 3.8 ± 3.5 minutes for specialist registrars (p not significant). There were no major complications in the non-medical angiographers group, although one patient required in-patient coronary artery bypass graft (CABG). There were two major complications in the specialist registrar group—one patient had a ventricular fibrillation (VF) arrest that was cardioverted successfully, and one had a peri-procedural myocardial infarction. Two patients required in-patient CABG. The visible haematoma rate was 4.3% in the non-medical group and 7.8% in the specialist registrar group (p not significant). The angiograms in both groups were of adequate diagnostic quality.
Conclusion: Appropriately trained and supervised non-medical staff can safely perform diagnostic coronary angiography on selected patients. Overall success rates, screening times, complication rates, and diagnostic quality are similar to cardiology specialist registrars.
226 PERI-OPERATIVE BETA-BLOCKADE FOR PATIENTS UNDERGOING INFRA-RENAL VASCULAR SURGERY (POBBLE): RESULTS OF A RANDOMISED DOUBLE BLIND CONTROLLED TRIAL
J. Powell.on behalf of the pobble trial investigators. Imperial College, London, UK; University Hospitals Coventry & Warwickshire, UK
Objective: To assess whether a pragmatic policy of peri-operative beta-blockade, with metoprolol, reduced 30-day cardiovascular morbidity and mortality and reduced length of hospital stay in average patients undergoing infra-renal vascular surgery.
Methods: This was a randomised placebo-controlled trial in vascular surgical units in four UK hospitals. 103 patients, without previous myocardial infarction, who had infra-renal vascular surgery between July 2001 and March 2004 took part in the study. Oral metoprolol (50 mg daily, supplemented by intravenous doses when necessary) or placebo was administered from admission until 7 days after surgery. Holter monitors were in place for 72 hours after surgery.
Results: Eighty men and 23 women (median age 73 years) were randomised, 55 to metoprolol and 48 to placebo: 97 (94%) underwent surgery during the trial. Commonest operations planned were aortic aneurysm repair (37%) and distal bypass (32%). Intra-operatively inotropic support was required in 64% and 92% of placebo and metoprolol groups, respectively. Within 30 days, cardiovascular events occurred in 32 patients including myocardial infarction (8%), unstable angina (9%), ventricular tachycardia (19%), and stroke (1%): four (4%) deaths were reported. Cardiovascular events occurred in 15 (34%) and 17 (32%) patients in placebo and metoprolol groups, respectively; relative risk 0.94 (95% CI 0.53 to 1.66). Time from operation to discharge was reduced from a median of 12 (95% CI 9 to 19) days in the placebo group to 10 (8–12) days in the metoprolol group, after planned adjustment for age, sex, statin use, and aortic cross-clamping; hazard ratio = 1.71 (95% CI 1.09 to 2.66), p = 0.019.
Conclusion: Myocardial ischaemia was evident in one third of the patients following surgery. A pragmatic regime of peri-operative beta-blockade with metoprolol did not appear to reduce 30 day cardiovascular events, but it did decrease the time from surgery to discharge.
227 ANTI-ANGINAL AND ANTI-ISCHAEMIC EFFICACY OF IVABRADINE—A SELECTIVE AND SPECIFIC SINUS NODE IF CURRENT INHIBITOR—COMPARED TO ATENOLOL IN ELDERLY PATIENTS WITH CHRONIC STABLE ANGINA
K. M. Fox, J. C. Tardif, I. Ford, M. Tendera on behalf of the INITIATIVE study investigators1Royal Brompton Hospital, London, UK; 2Montreal Heart Institute, Montreal, Canada; 3University of Glasgow, UK; 4Katowice, Poland
Background: Ivabradine—a pure heart rate reducing agent acting selectively and specifically on the depolarising If current in the sinoatrial node—has shown similar anti-anginal and anti-ischaemic effects compared to atenolol in a randomised, double-blind, 4-month study (INITIATIVE study; n = 939).
Objective: Since the prevalence of stable angina is increasing with age with three quarters of patients >65 years, we further analysed the study results with the objective of confirming whether the observed benefits with ivabradine were preserved in this age category.
Method: The anti-anginal and anti-ischaemic effect of ivabradine was analysed in the INITIATIVE sub-population of 232 patients aged ⩾65 years, and randomised to ivabradine 7.5 mg bid (n = 113) or atenolol 100 mg od (n = 119), based on changes on total exercise duration (TED/primary endpoint) and time to 1 mm ST-segment depression (TST) at trough of drug activity at M4.
Results: In patients >65 years, TED was increased by 88.7 ± 119 s (from 567.2 ± 157.9 s) with ivabradine 7.5 and by 65.6 ± 136.6 s (from 555.5 ± 154.8 s) with atenolol 100 mg. ST-segment depression increased by 101.9 ± 145.9 s (from 485.2 ± 175.3 s) with ivabradine and by 81.7 ± 150.5 s (from 473.3 ± 156.3 s) with atenolol. Improvements in TED and TST with ivabradine were maintained as compared to the overall study population, while they tended to deteriorate with atenolol, even though the statistical non-inferiority of ivabradine v atenolol remained within equivalence limits, thus confirming the overall study results. Side effects of beta-blockers such as atrioventricular block, sexual dysfunction, and bronchospasm were not observed with ivabradine. A higher incidence of mild and most often transient visual symptoms was observed with ivabradine 7.5 mg bid, causing, however, no withdrawals in patients aged ⩾65 years.
Conclusion: This analysis shows that the good clinical efficacy and tolerability of ivabradine, previously demonstrated versus atenolol in 939 patients with stable angina, is maintained in the elderly. Since many patients with stable angina are >65 years, these results may have important clinical implications.
228 NOVEL MUTATIONS IN CARDIAC MYPBC3 CAUSE EARLY ONSET MALIGNANT HYPERTROPHIC CARDIOMYOPATHY (HCM)
S. Carballo, E. Blair, H. Watkins.Department of Cardiovascular Medicine, University of Oxford, Oxford, UK
A molecular diagnosis is made in 50–60% of individuals affected by HCM, and variants in genes encoding sarcomeric proteins account for the majority of these. Mutations in cardiac myosin-binding protein-C (MYBPC3) are found in 20–25% of cases. Initial genotype-phenotype studies, as well as recent and large surveys, have associated this gene with late onset disease, although a similar clinical course and mortality rate is observed once hypertrophy is manifest. As part of a systematic study, DNA was obtained from 34 consecutive families with HCM and all coding exons of MYBPC3 were screened by temperature-modulated heteroduplex analysis. Exons with aberrant profiles were sequenced and variants confirmed by restriction digestion, segregation analysis, and study of normal controls. Three novel mutations were found that appear to produce an early malignant phenotype in five unrelated families. A missense mutation, Arg502Trp, was found in three probands; in all three respective families there was symptomatic disease and/or sudden death under 16 years of age. Severe heart failure required heart transplant in one individual. A novel Tyr749X mutation was identified in a family with disease onset as young as 12 years and sudden death in one individual aged 23 years. A novel delC2096 mutation was identified in an individual with a family history of young onset disease and two instances of sudden death amongst five affected (20 and 27 years). These new data indicate that mutations in MYBPC3 can sometimes produce symptomatic HCM in the young, associated with a severe phenotype. We suggest that even where genotype-phenotype correlations in HCM are robust, and have generally been replicated, exceptions are not rare. The frequent occurrence of “private” mutations further confounds derivation of reliable genotype-phenotype correlations.
Conclusion: These new data indicate that mutations in MYBPC3 can sometimes produce symptomatic HCM in the young, associated with a severe phenotype. We suggest that even where genotype-phenotype correlations in HCM are robust, exceptions are not rare. Although clinical findings may guide molecular investigations, targeted screening of only a subset of genes cannot be justified on clinical grounds.
229 DELINEATING THE ROLE OF ADENOSINE MONOPHOSPHATE (AMP)-ACTIVATED PROTEIN KINASE (AMPK) γ2 SUBUNIT IN HYPERTROPHIC CARDIOMYOPATHY (HCM)
R. Grignani, K. Pinter, H. Farza, S. Carballo, M. Oliveira, C. Redwood, E. Blair, H. Watkins.Department of Cardiovascular Medicine, University of Oxford, Oxford, UK
Hypertrophic cardiomyopathy has traditionally been thought of as a “disease of the sarcomere”, with recent evidence suggesting that inefficient energy utilisation may be a unifying mechanism. Mutations in the γ2 subunit of AMPK—a heterotrimeric sensor of the energy status within the cell—have been found to cause conduction abnormalities with features of HCM. The molecular pathway leading from genotype to phenotype is unclear and the primary pathological role of the AMPK γ2-subunit is yet to be determined. In particular, the γ2-subunit is ubiquitously expressed, and only accounts for a minority of total AMPK activity. Our aim, therefore, is to define a specific role for the AMPK γ2-subunit in the heart. To achieve this, mRNA encoding the different AMPK γ-subunits was quantified by semi-quantitative real time polymerase chain reaction (PCR) on selected mouse and human tissues. To localise the message during mouse embryogenesis, in situ hybridisation was carried out on whole mount and tissue sections. Subcellular localisation of the protein was analysed by immunohistochemistry and confocal microscopy. In both adult mouse and human tissues, AMPK γ2 message was up to two fold higher in the heart compared to other organs. In the mouse heart, message was highest during development, peaking at birth. The AMPK γ2 protein was strongly expressed in both atria and pericardium at embryonic time point E13.5, suggesting a specific and important role during cardiac development. In adult mouse ventricular cardiomyocytes, AMPK γ2 protein is localised in the sarcomere, presenting with a striated pattern.
Conclusion: Our data for the first time, suggest an important role for the AMPK γ2 subunit in the heart, in particular during embryogenesis. The sarcomeric organisation requires further validation but implies a specific role in cardiomyocytes, which could direct further investigations to explain the cardiac specific phenotype.
230 A UK CENTRE EXPERIENCE OF THE EFFICACY OF IMPLANTABLE CARDIAC DEFIBRILLATORS (ICDS) FOR THE PREVENTION OF SUDDEN CARDIAC DEATH IN PATIENTS WITH HYPERTROPHIC CARDIOMYOPATHY (HCM)
R. Assomull, M. T. Esteban, J. Relf, S. Jones, W. McKenna, P. Elliott.The Heart Hospital, London, UK; St. Georges Hospital, London, UK
Background: Previous multicentre studies have shown that ICDs are effective in terminating life-threatening arrhythmias in HCM, particularly in the setting of secondary prevention. It has been estimated that 7% of the HCM population who are implanted with ICDs will have an appropriate discharge per year.
Aims: To assess ICD discharge rates in patients with hypertrophic cardiomyopathy who have had an ICD implanted.
Results: We followed up a cohort of patients with HCM who had ICD implantation at our centre. Ninety-two patients were followed up with a mean duration of follow up of 3.2 ± 2.4 years. Fifty-three patients were male and 68 patients had ICD implantation as a prophylactic primary prevention measure. Mean age at implant was 36 ± 14 years. Eight of the 92 patients (all men) died during the follow up period. Five died from congestive cardiac failure (CCF), one from pulmonary embolism, and two died from non-cardiac causes. Fourteen patients received appropriate shocks during the follow up period and of these eight received more than one shock. Fourteen patients also received inappropriate shocks. Four patients received both appropriate and inappropriate shocks. Overall the rate of appropriate shocks in our cohort was 5% per year. The rates were significantly higher (p = 0.04) in the secondary prevention group (9%) than in the primary prevention group (3%). Thirty-three percent of the group were treated with amiodarone following ICD implantation. This figure is higher than in previous studies where only 17% of the group continued with amiodarone treatment following ICD implantation.
Conclusion: Appropriate shock rates in our single centre study appear to be lower than in previously published figures. This may be due to a lower threshold for proceeding to ICD implantation in our cohort than in the studies published several years earlier. In addition the use of amiodarone in our cohort appears to be higher than in previously published studies.
231 DISEASE SEVERITY AND ABNORMAL COLLAGEN TURN OVER IN ANDERSON FABRY DISEASE (AFD)
J. S. Shah, M. H. Tayabjee, D. Hughes, A. Mehta, R. McFadyen, P. M. Elliott.The Heart Hospital, University College London, London, UK; The Royal Free Hospital, London, UK; City Hospital, University of Birmingham Medical School, Birmingham, UK
Background: Anderson-Fabry Disease is an inherited metabolic disease associated with death from cardiovascular and renal disease. Patients with AFD develop progressive left ventricular (LV) hypertrophy, cardiac fibrosis, and heart failure. We hypothesised that patients with AFD have altered collagen turn over compared to normal controls.
Methods and Results: Twenty-nine (15 male, aged 44.1 ± 11.7 years) consecutive patients with AFD and 21 normal controls (10 male, aged 39.7 ± 11.3 years) had serum analysed for MMP-9, TIMP-1, and TIMP-2 levels. Mean LV wall thickness in patients was 13.4 ± 4.3 mm (mean LV mass index 121.3 ± 48.4 g/cm × 2). MMP-9 levels were significantly higher in patients than controls (1003.8 ± 337.8 ng/ml v 576.7 ± 276.3 ng/ml, respectively; p < 0.001; see fig). There were no differences in TIMP levels between patients and controls. There was no correlation between LV mass or maximal LV wall thickness and MMP-9 levels. There was a negative correlation between MMP-9 and fractional shortening (FS; r = −0.5; p = 0.01). There was a positive correlation between MMP-9 levels and Mainz Severity Score Index (MSSI, a validated score for disease severity; r = 0.5; p = 0.01). These relationships were independent of gender using stepwise linear regression analysis.

Abstract 231
Conclusion: Patients with AFD have higher levels of MMP-9 compared to controls. The correlation between MMP-9 levels and disease severity suggests that altered collagen turn over may be involved in the pathogenesis of this disease. The relation between MMP-9 and FS suggests that progressive cardiac fibrosis may be the underlying mechanism for systolic dysfunction in AFD.
232 ELECTROCARDIOGRAPHY AND CARDIAC MAGNETIC RESONANCE IMAGING (MRI) BEFORE AND AFTER ALCOHOL SEPTAL MYOCARDIAL ABLATION (ASA) IN HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
G. P. McCann2, W. G. Van Dockum, A. M. Beek, F. J. Ten Cate1, J. M. Ten Berg, H. J. J. Wellens, A. C. Van Rossum.1VU Medical Center, Amsterdam, The Netherlands; Thorax Center, Rotterdam, The Netherlands; 2University Hospitals Leicester, Leicester, UK
Background: Percutaneous ASA is an established technique in patients with hypertrophic obstructive cardiomyopathy.
Methods: Twenty-six patients were studied with ECG and MRI at baseline, 1, and 6 months after ASA. Electrocardiogram voltages and voltage duration products were assessed as predictors of left ventricular mass (LVM) at baseline and 6 months after ASA (I, aVL for all subjects and Sokolow-Lyon, Cornell, I, aVL, V6, for those without right bundle branch block (RBBB)). Myocardial infarction (MI) size and location was determined at 1 month by delayed contrast enhancement.
Results: Fifteen subjects developed new RBBB and were more likely to have sustained both anterior and inferior transmural septal infarction (9/15 v 1/9, p = 0.02) (see fig) but attained similar mass reductions to those without RBBB (45 ± 14 v 29 ± 13 g, p = 0.06). At baseline aVL product was the best predictor of LVM index R2 = 42.9%, p < 0.001, and septal mass index (SMI), R2 = 39.6%, p = 0.001. Following ASA the best predictor of left ventricular mass index (LVMI) and SMI in those not developing RBBB was V6 product (R2 = 79.0, p < 0.001 and R2 = 69.3%, p < 0.001) and aVL voltage (R2 = 51.4%, p < 0.001 and R2 = 55.6%, p < 0.001) in all patients. However no ECG voltage or product significantly predicted reductions in myocardial mass.
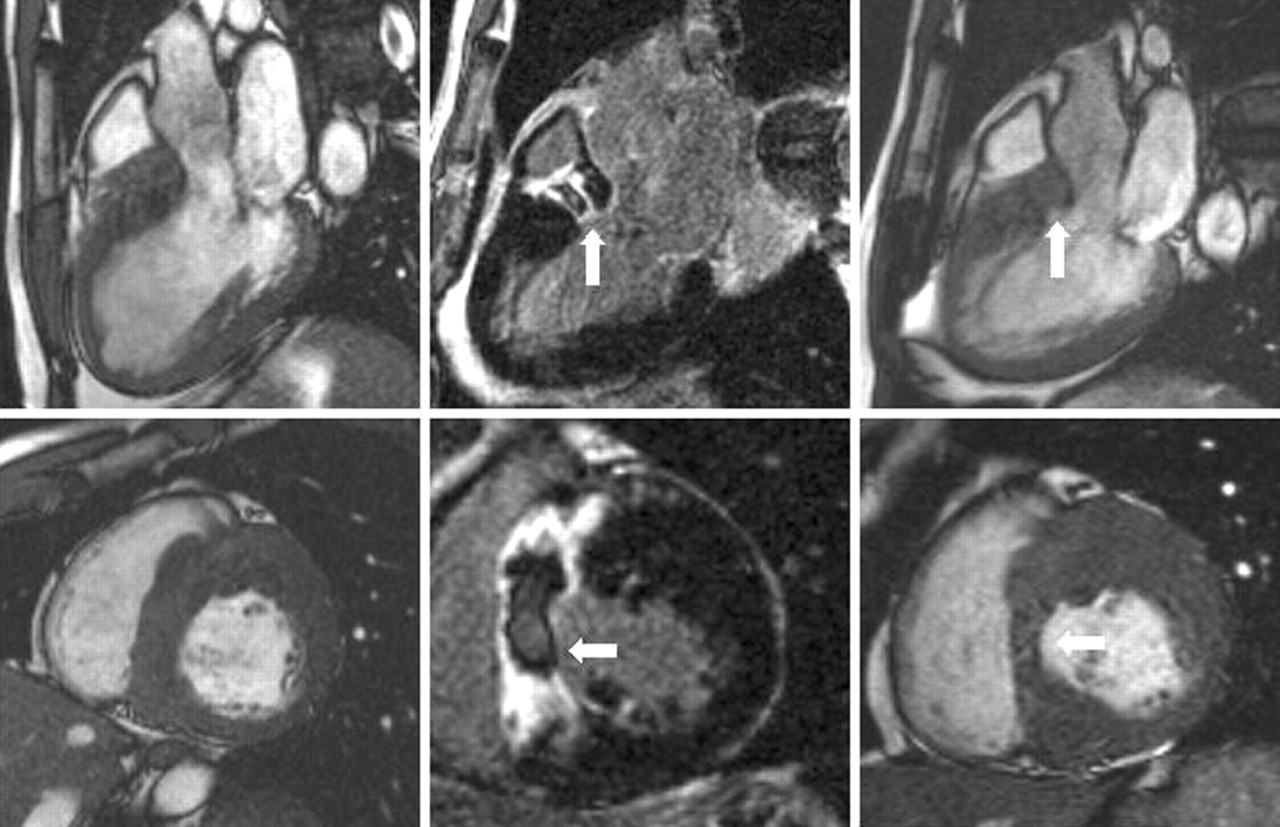
Abstract 232
Conclusion: Patients developing RBBB after ASA are more likely to have sustained both anterior and inferior septal transmural infarction compared to those without RBBB. Estimation of mass reductions following ASA is not feasible by ECG voltages and should be performed by a reliable imaging technique.
233 LEFT VENTRICULAR REMODELLING IN DILATED CARDIOMYOPATHY (DCM) WITH AND WITHOUT EVIDENCE OF LATE GADOLINIUM ENHANCEMENT-CARDIOVASCULAR MAGNETIC RESONANCE (LGE-CMR)
R. G. Assomull, J. C. Lyne, M. Khan, D. J. Pennell, S. K. Prasad.Centre for Advanced MR in Cardiology (CAMRIC), Royal Brompton Hospital, London, UK
Late gadolinium enhancement-cardiovascular magnetic resonance shows a patchy, midwall pattern in approximately 30% of patients with a clinical diagnosis of DCM. The scans of 33 consecutive patients with DCM were analysed. Overall, 22 patients (66%, 15 male, mean age 51 ± 19 years) showed no late enhancement whilst 11 (33%, nine male, mean age 40 ± 11 years) displayed midwall late enhancement. Left and right ventricular (LV, RV) dimensions and mass were compared between the two groups using a two sample independent t-test. Dilated cardiomyopathy patients with late enhancement had a significantly higher LV end diastolic volume index (LVEDVI) when compared to patients without late enhancement (166 + 50 ml/m2v 124 + 36 ml/m2 respectively, p = 0.009). The LV end systolic volume index (LVESVI) was also significantly higher in the late enhancement group (118 + 56 ml/m2v 81 + 39 ml/m2, respectively, p = 0.04). Mean LV mass index in the late enhancement group was significantly higher than in the non-enhancement group (123 + 25.4 g/m2v 103 + 26 g/m2, p = 0.04). There was no difference in LVEF, RV volumes, and RVEF between the two groups. Patients with DCM and midwall late enhancement had significantly larger LV volumes and mass than patients with no enhancement, reflecting adverse remodelling. This did not result, however, in poorer function.
Conclusion: Potential explanations are that mid-wall fibrosis is a feature of more severe LV disease or conversely that this reflects a differing underlying aetiology and pathologic process that results in greater LV volumes. Further work is required to understand the temporal onset of late enhancement and its correlation with clinical outcome.
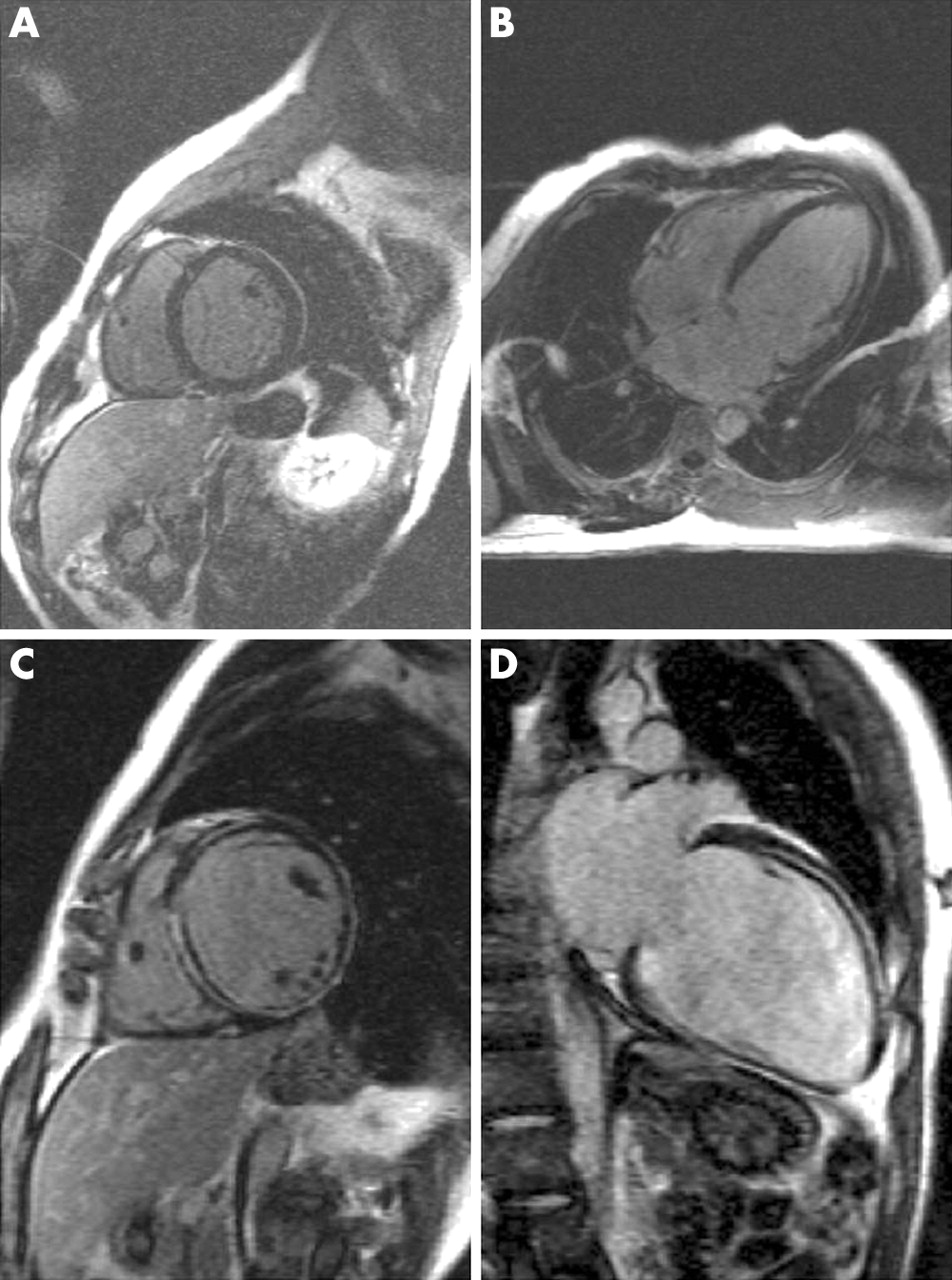
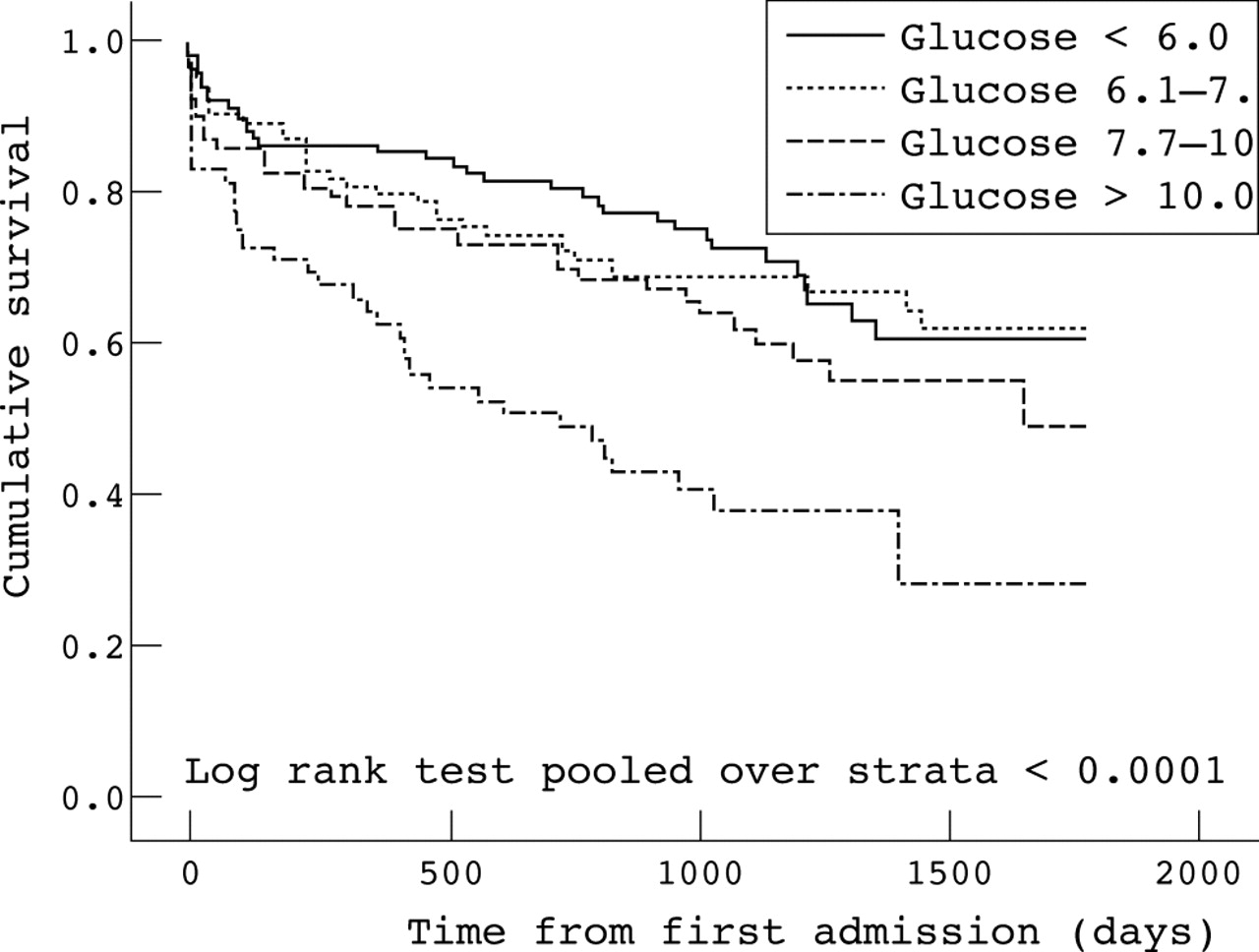{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
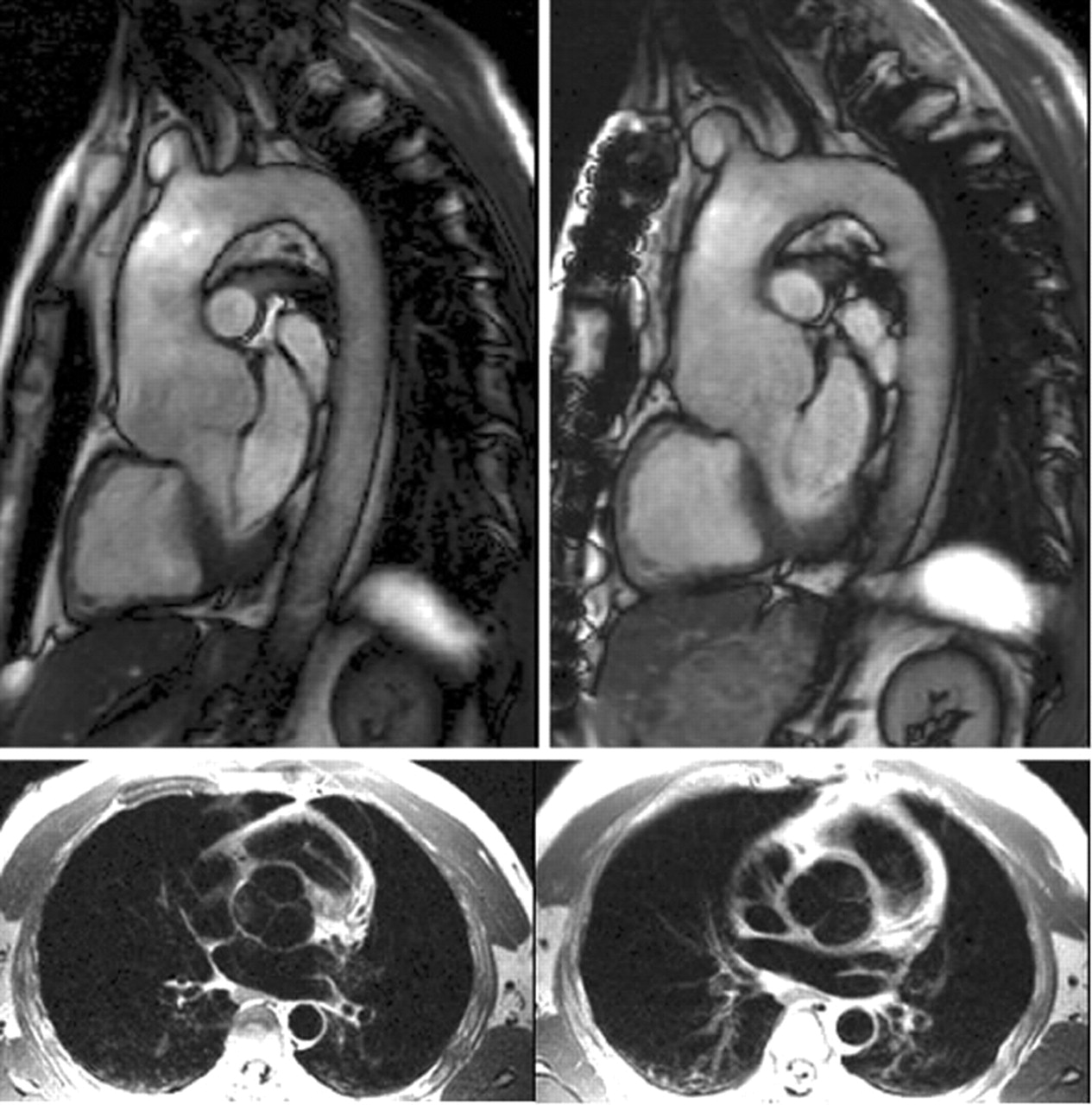{kind=link}
{kind=link}
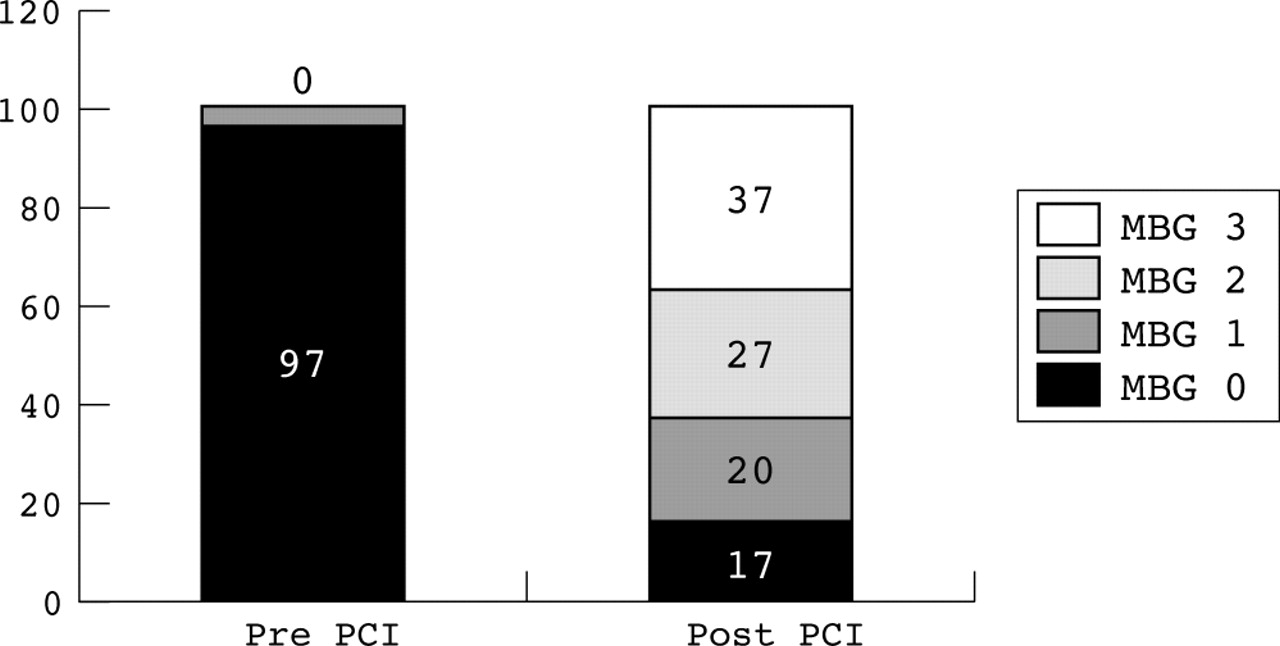{kind=link}
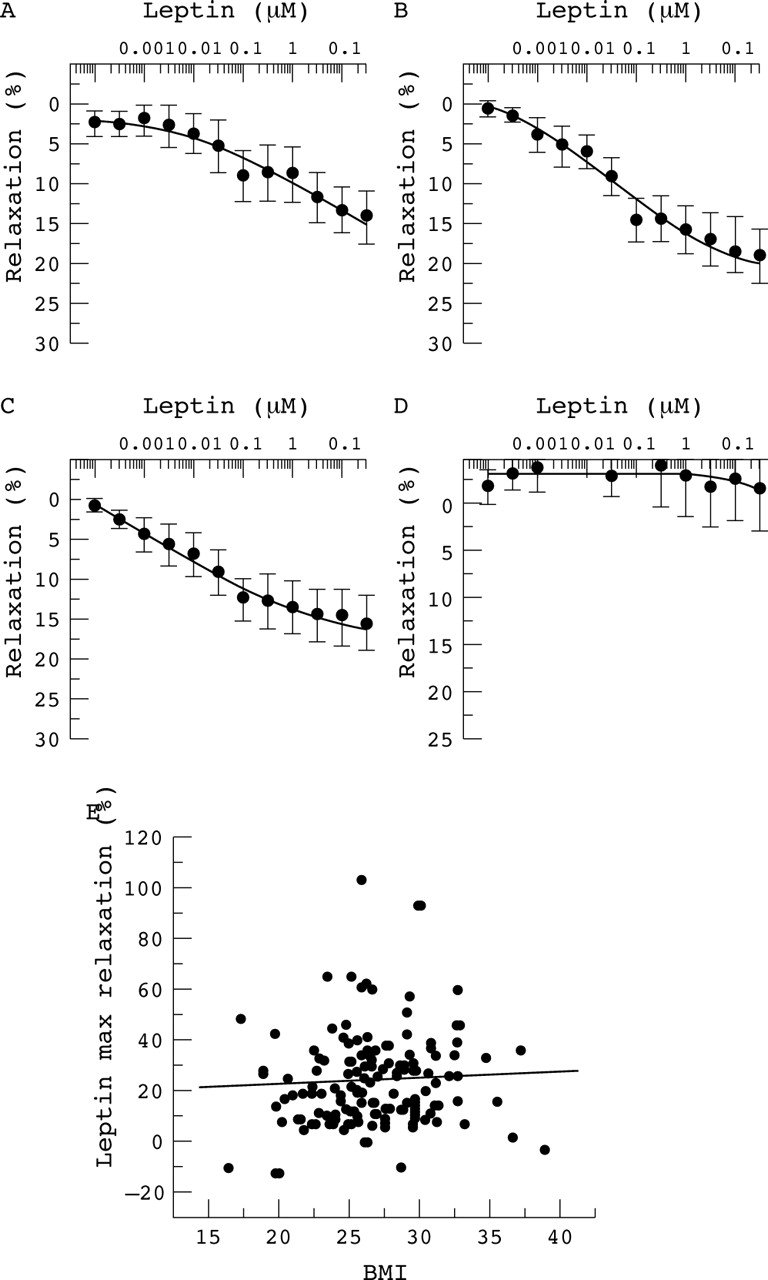{kind=link}
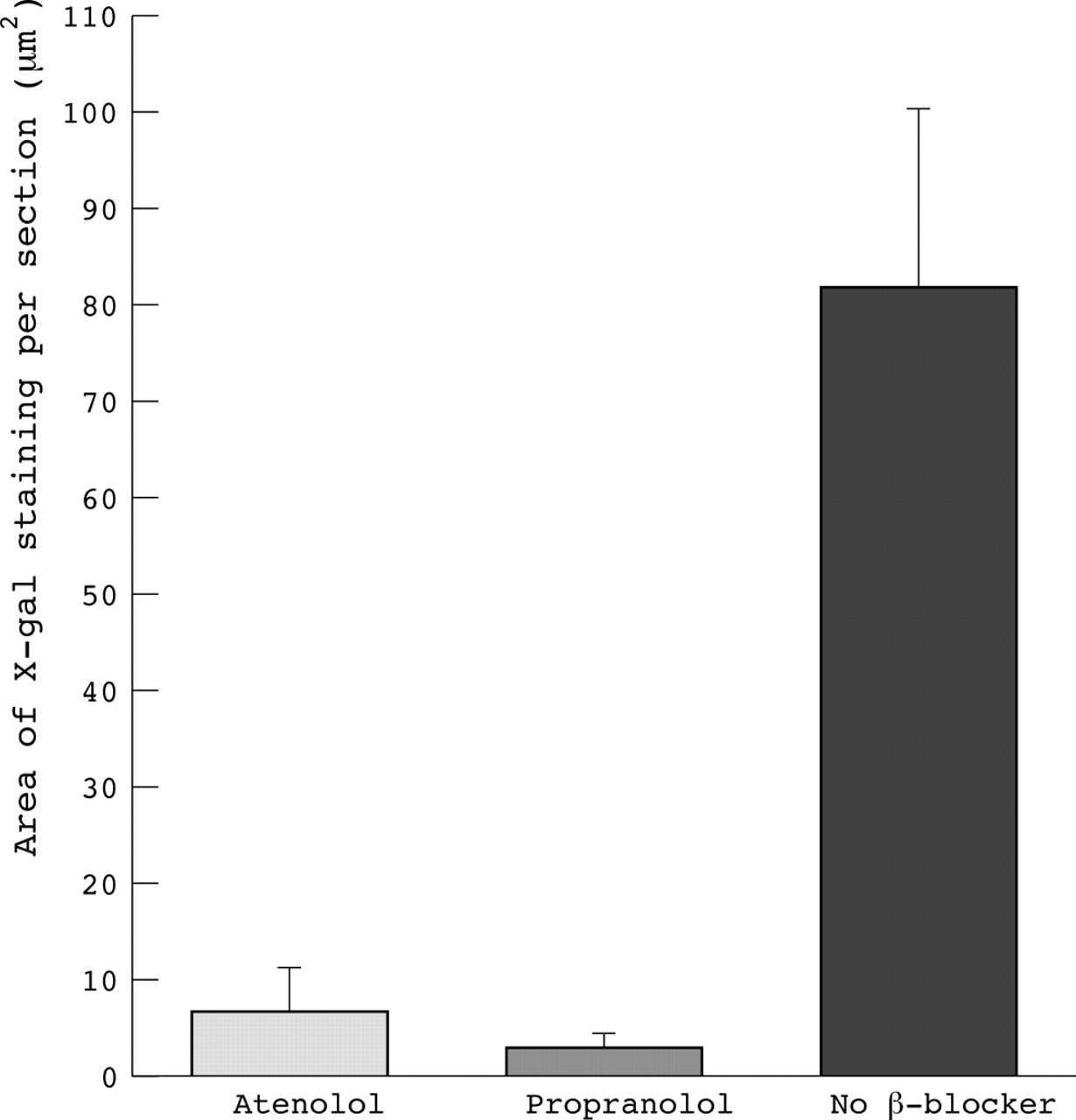{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
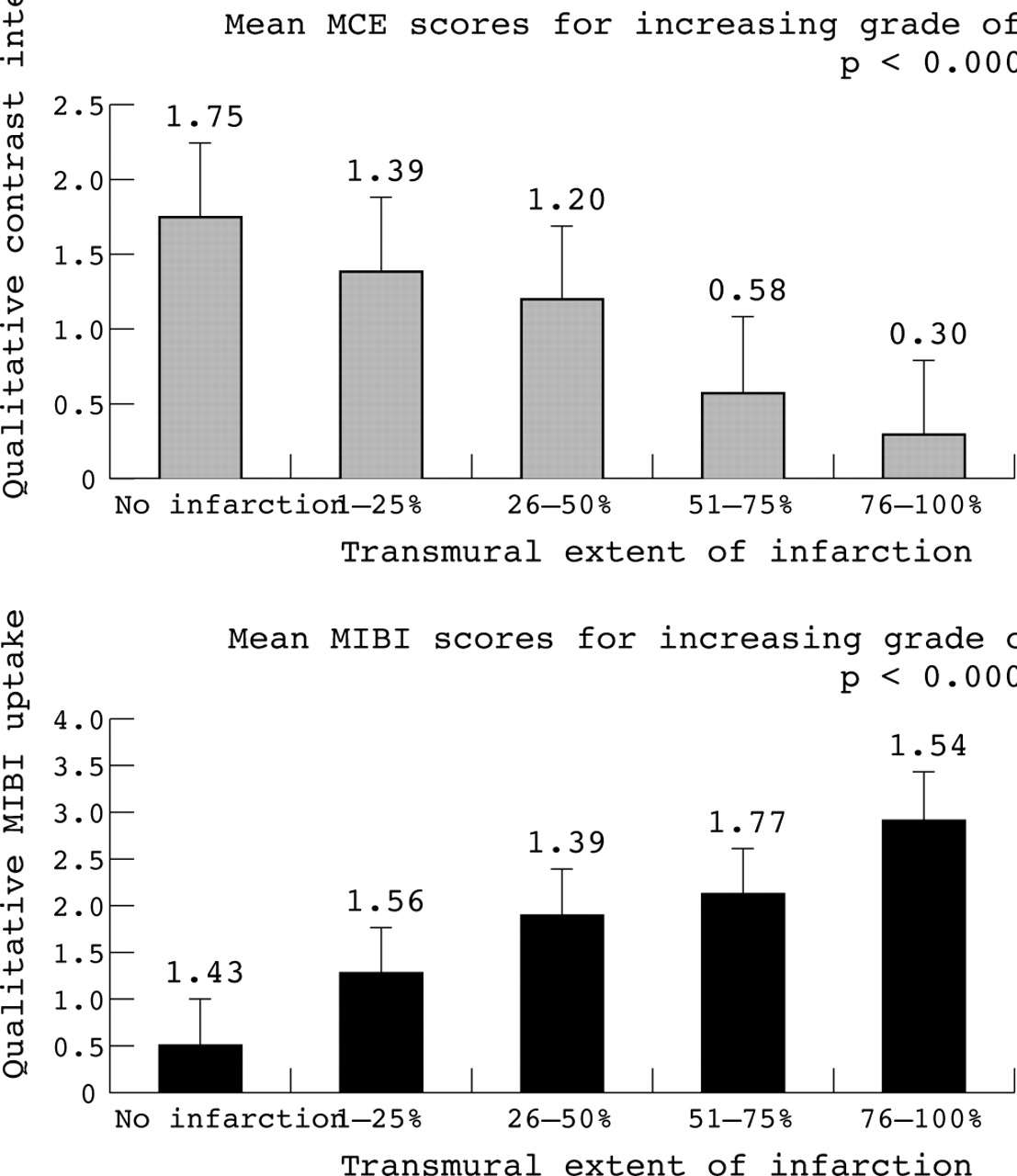{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
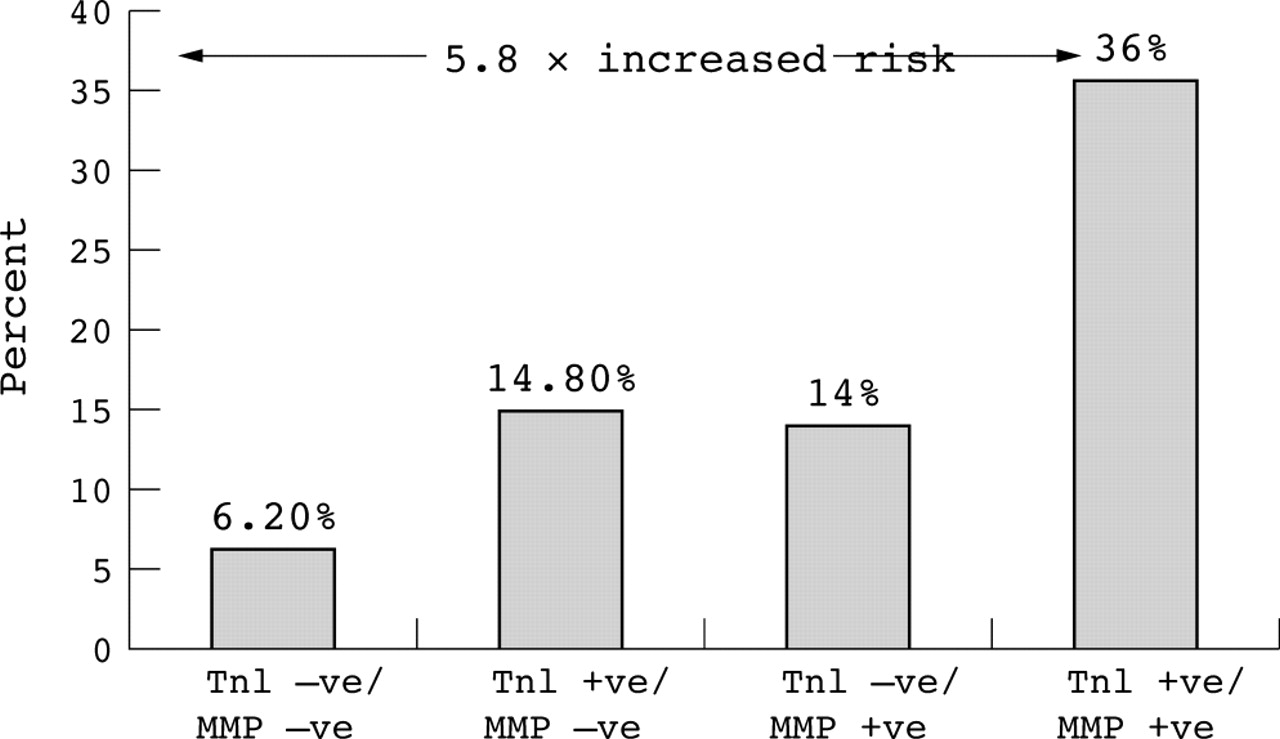{kind=link}
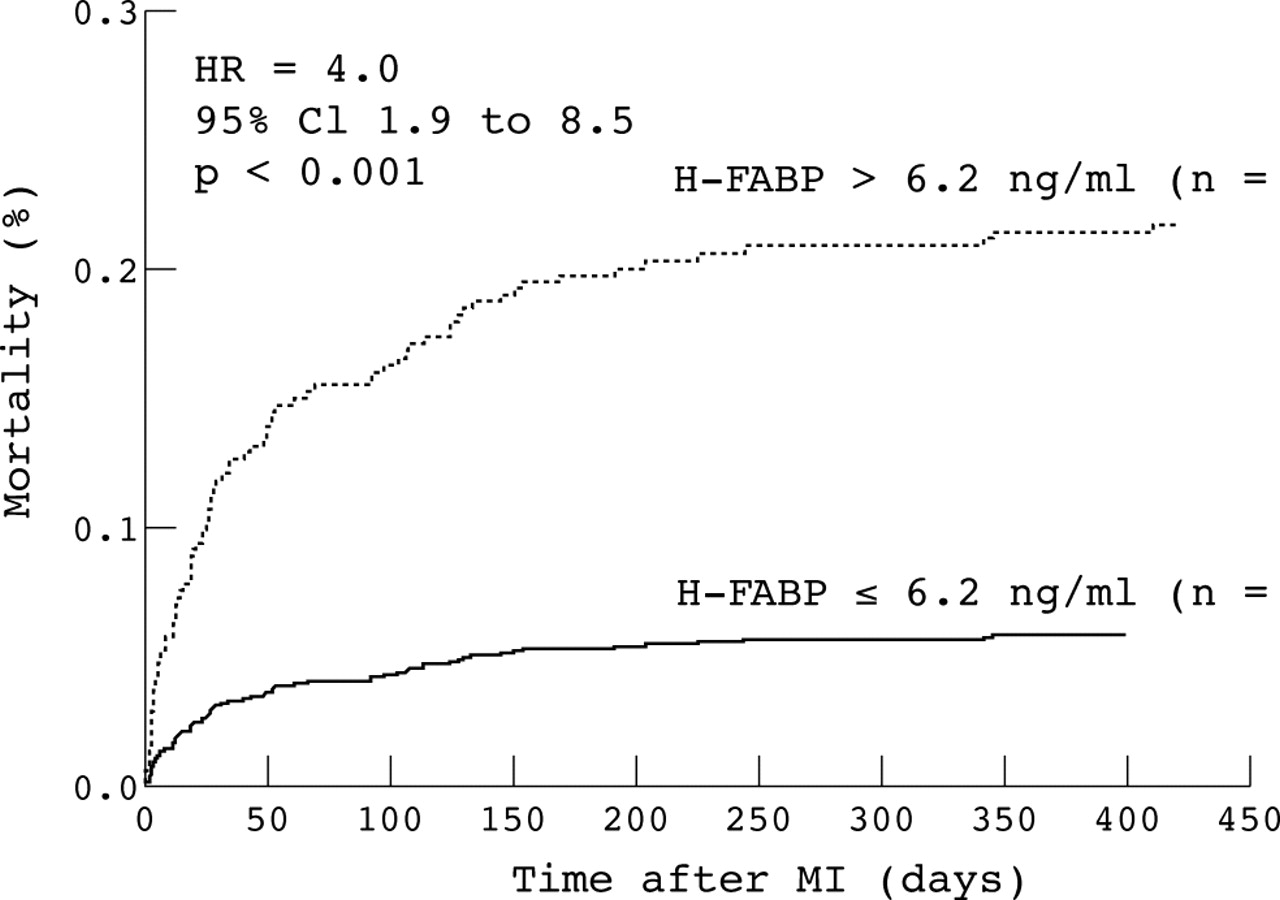{kind=link}
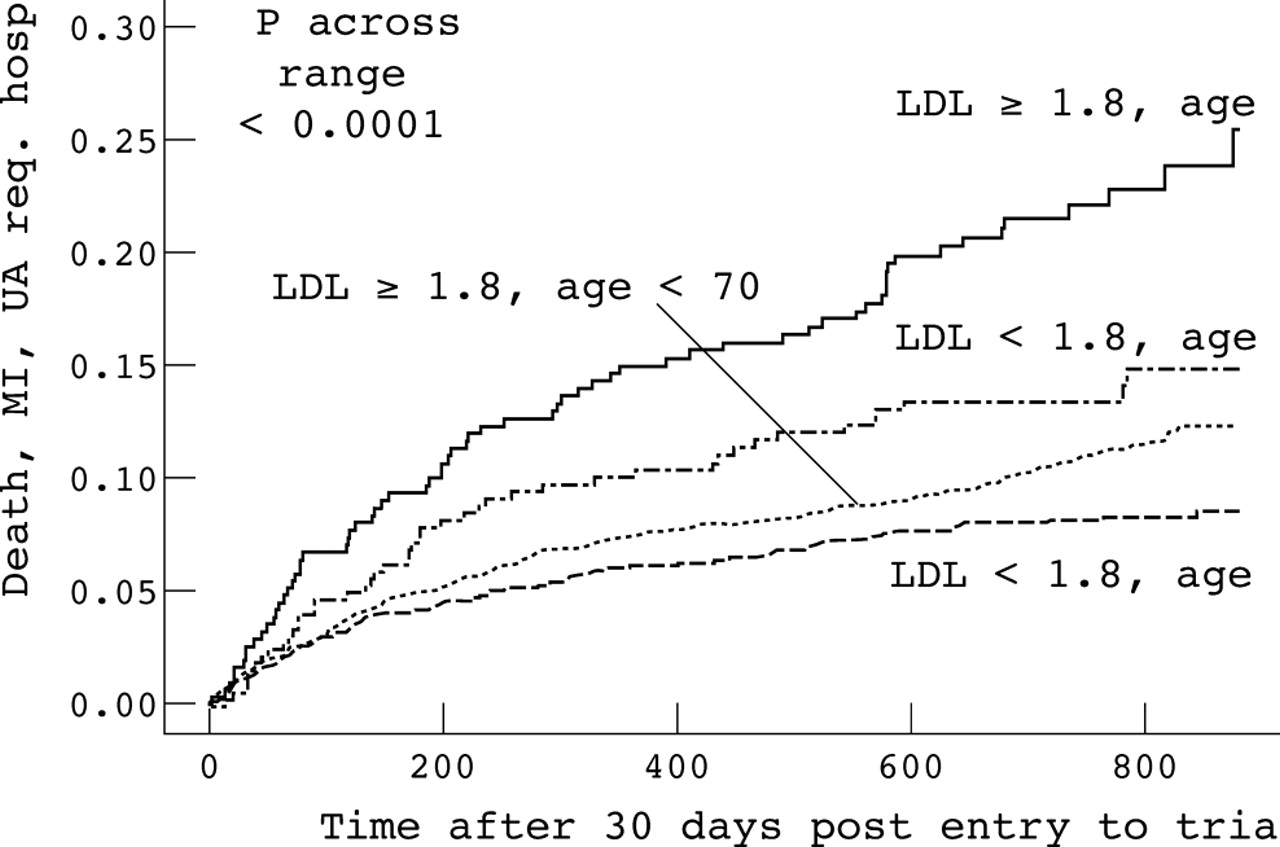{kind=link}
{kind=link}
{kind=link}
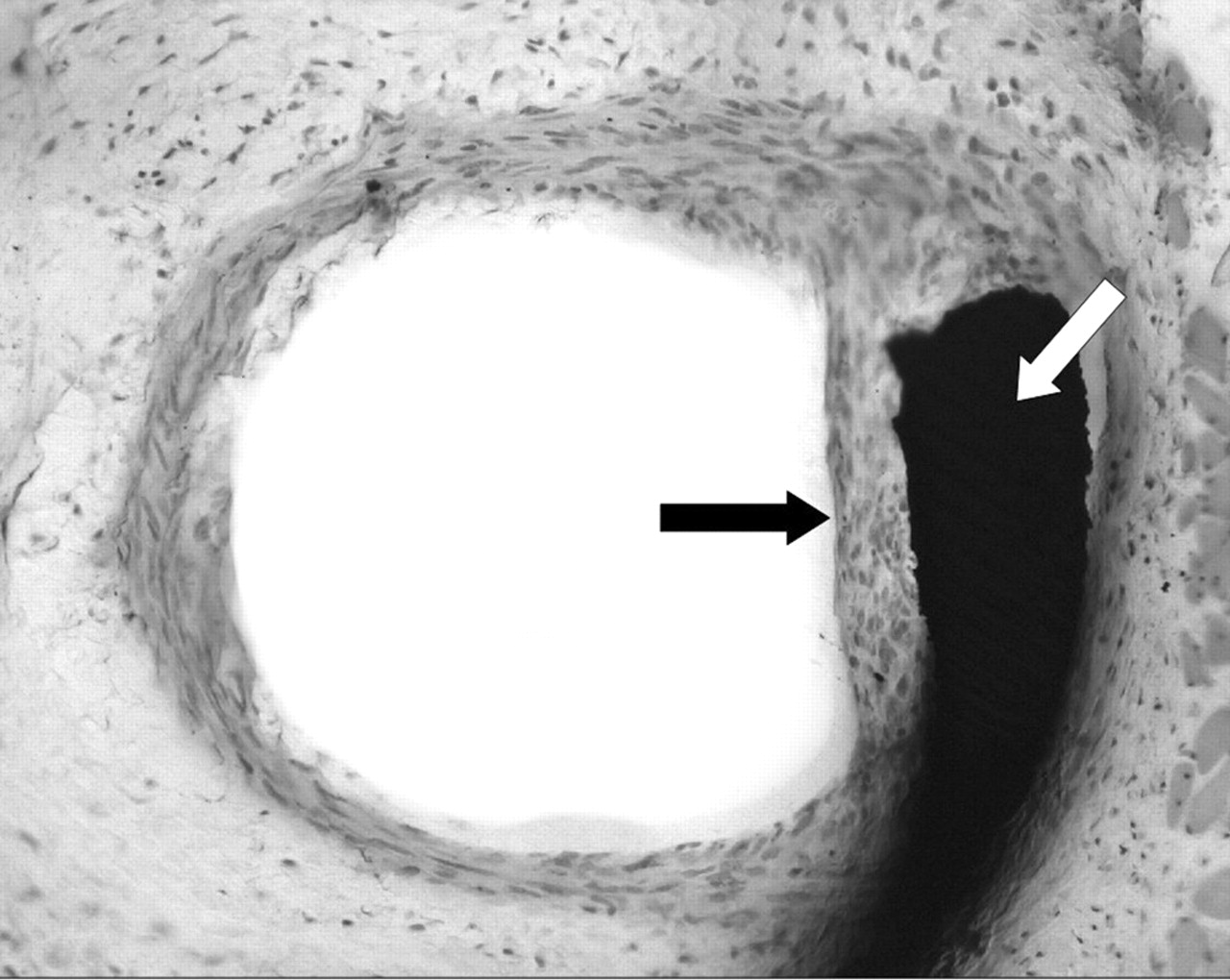{kind=link}
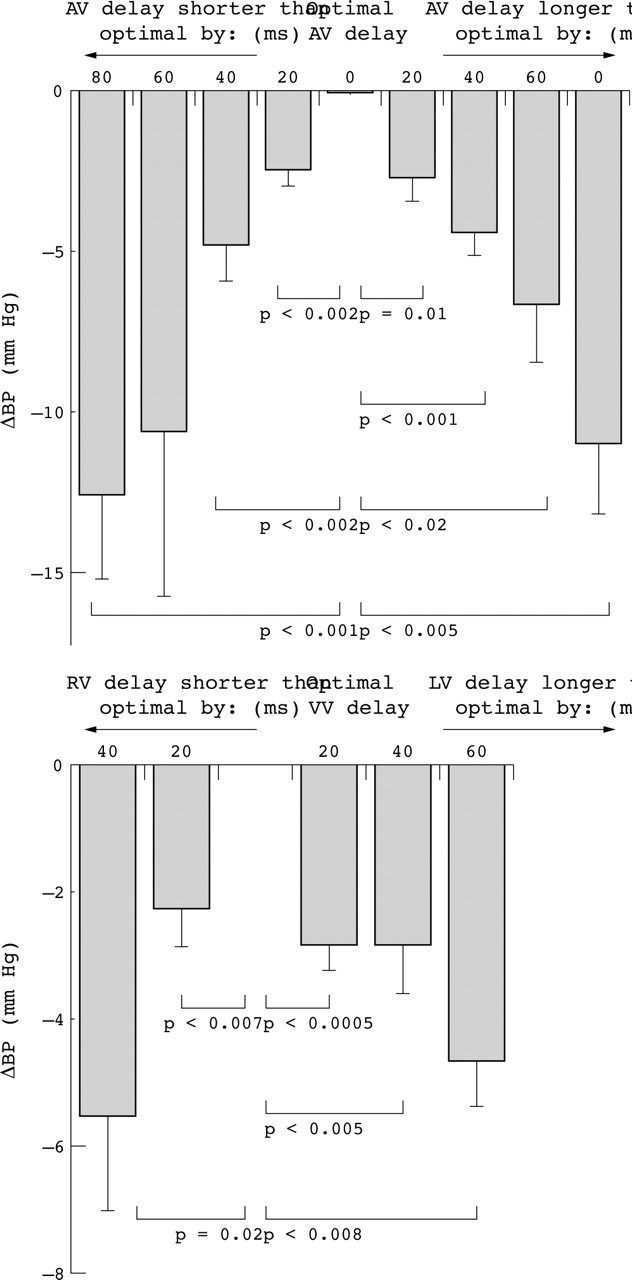{kind=link}
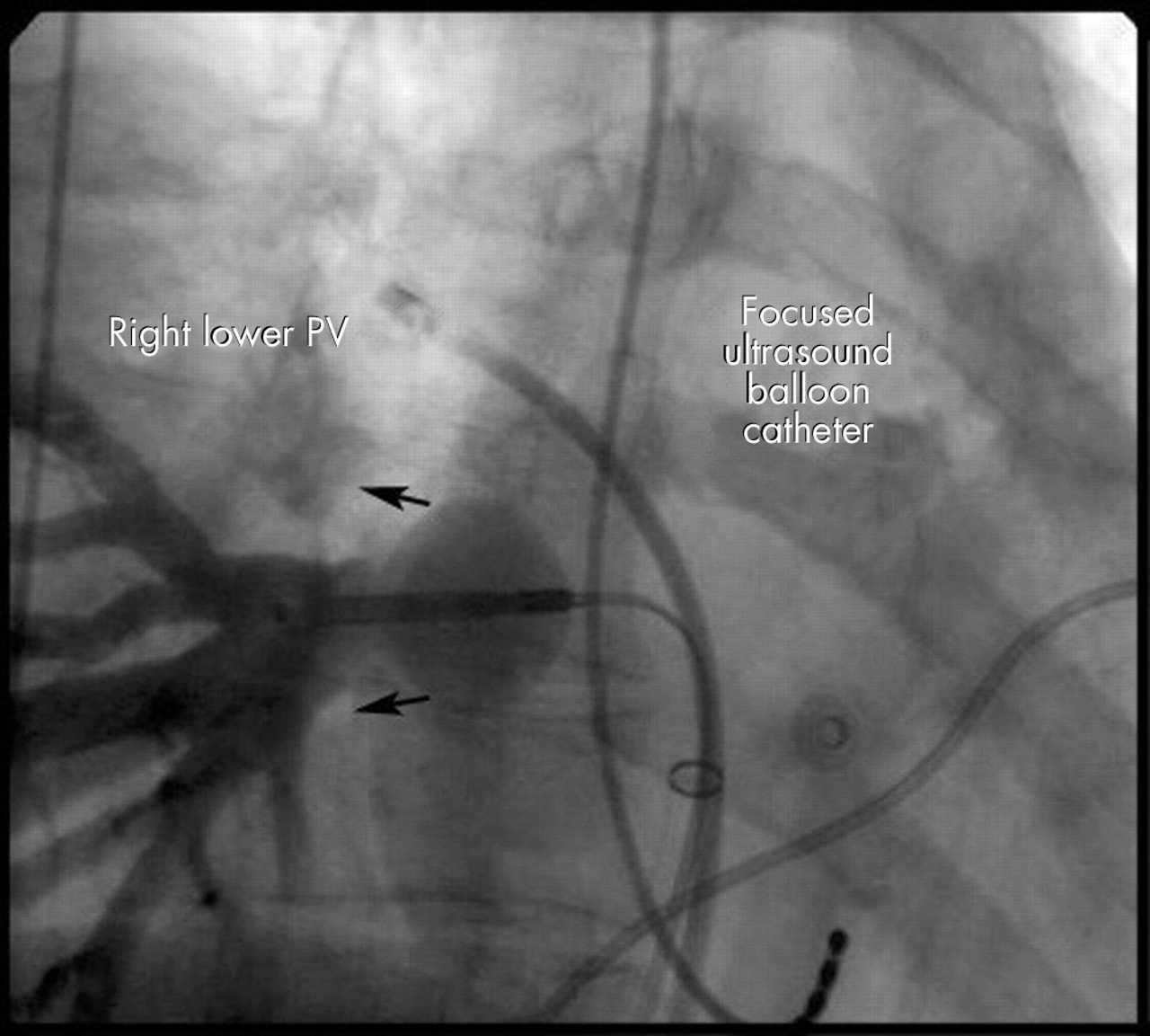{kind=link}
{kind=link}
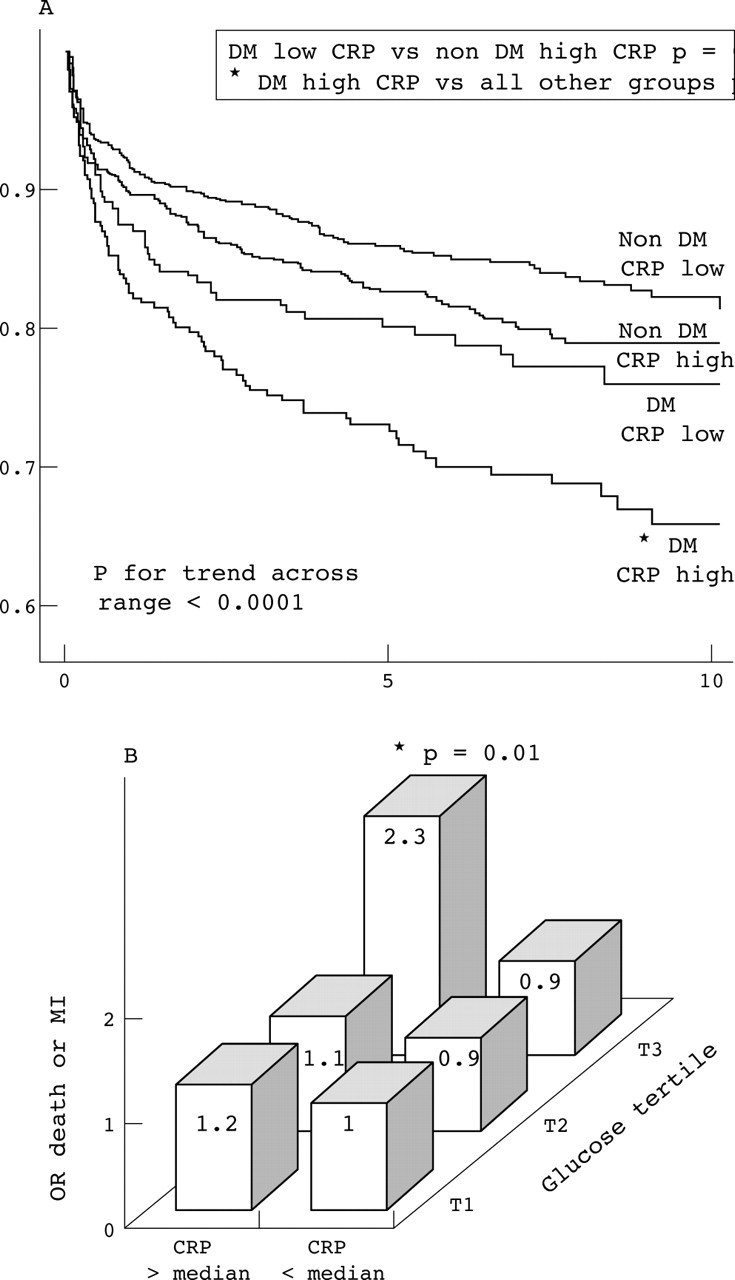{kind=link}
{kind=link}
{kind=link}
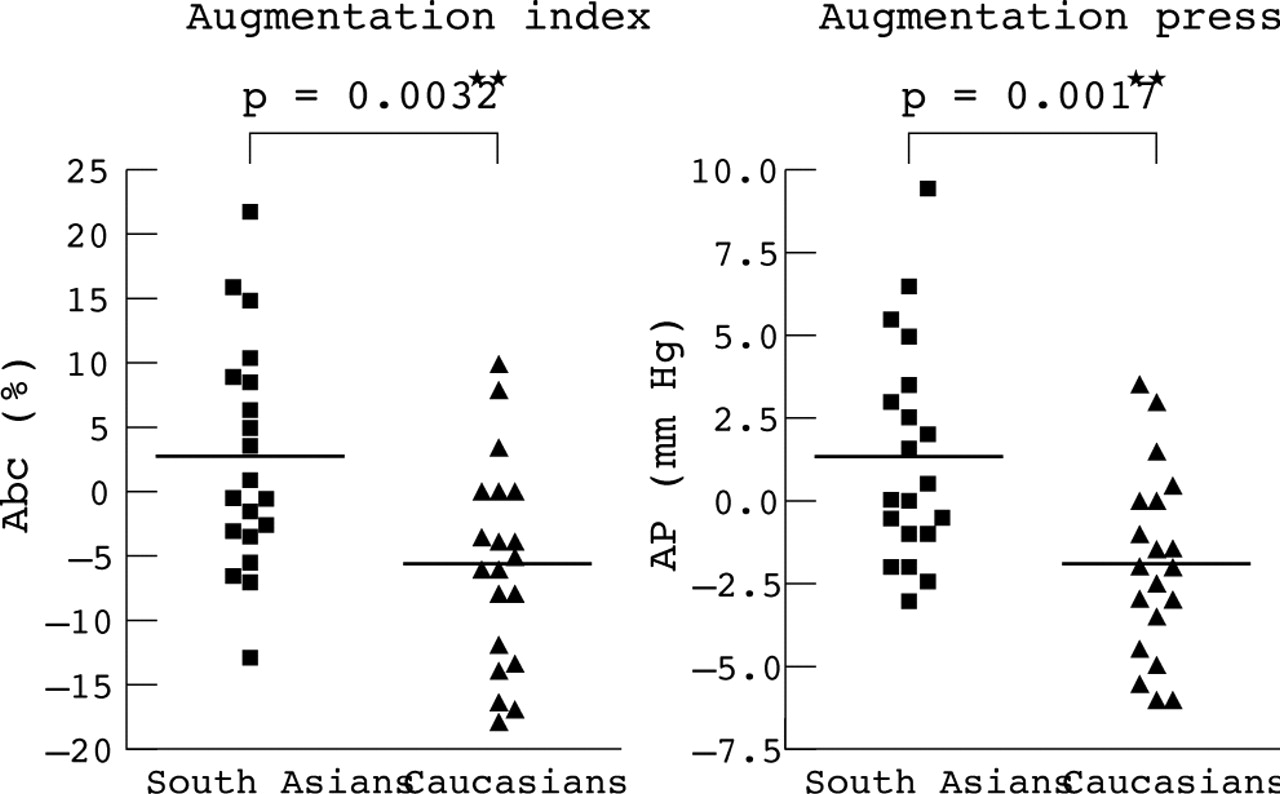{kind=link}
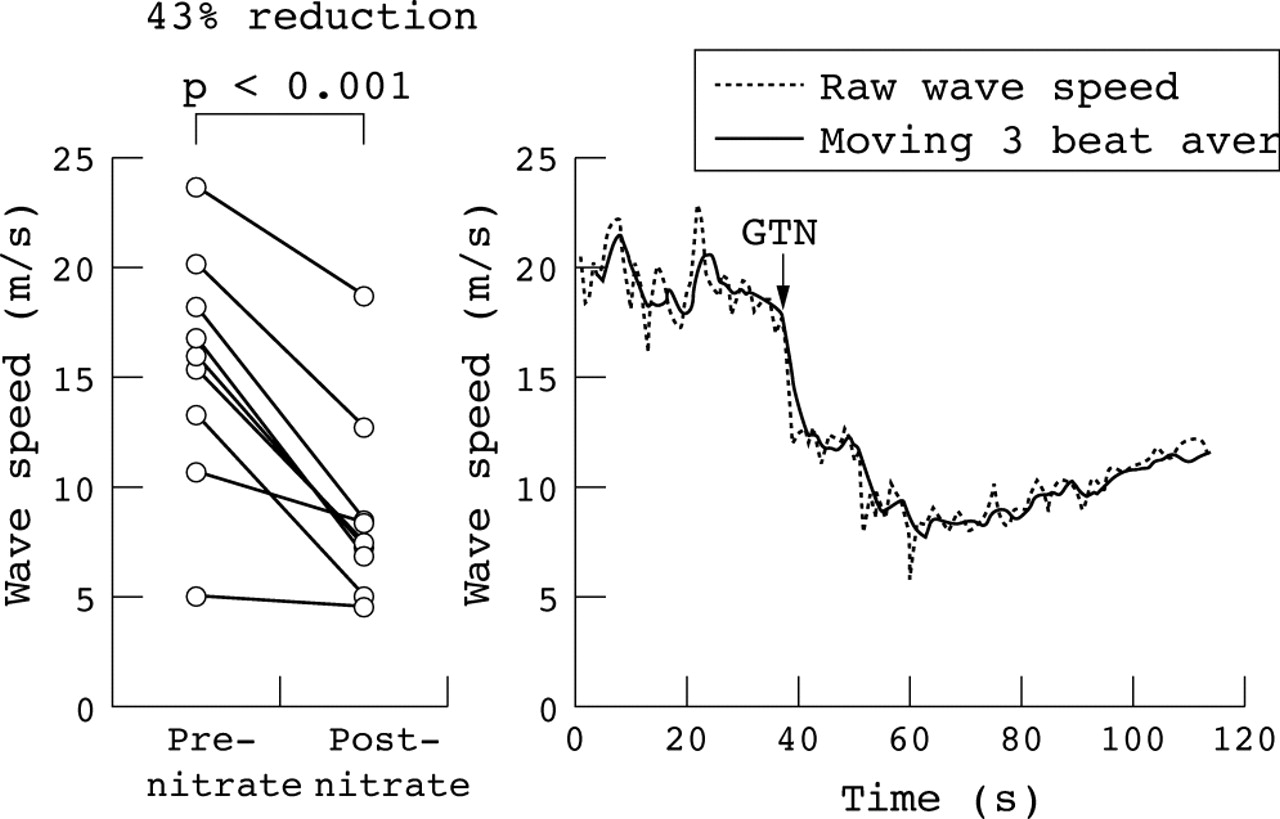{kind=link}
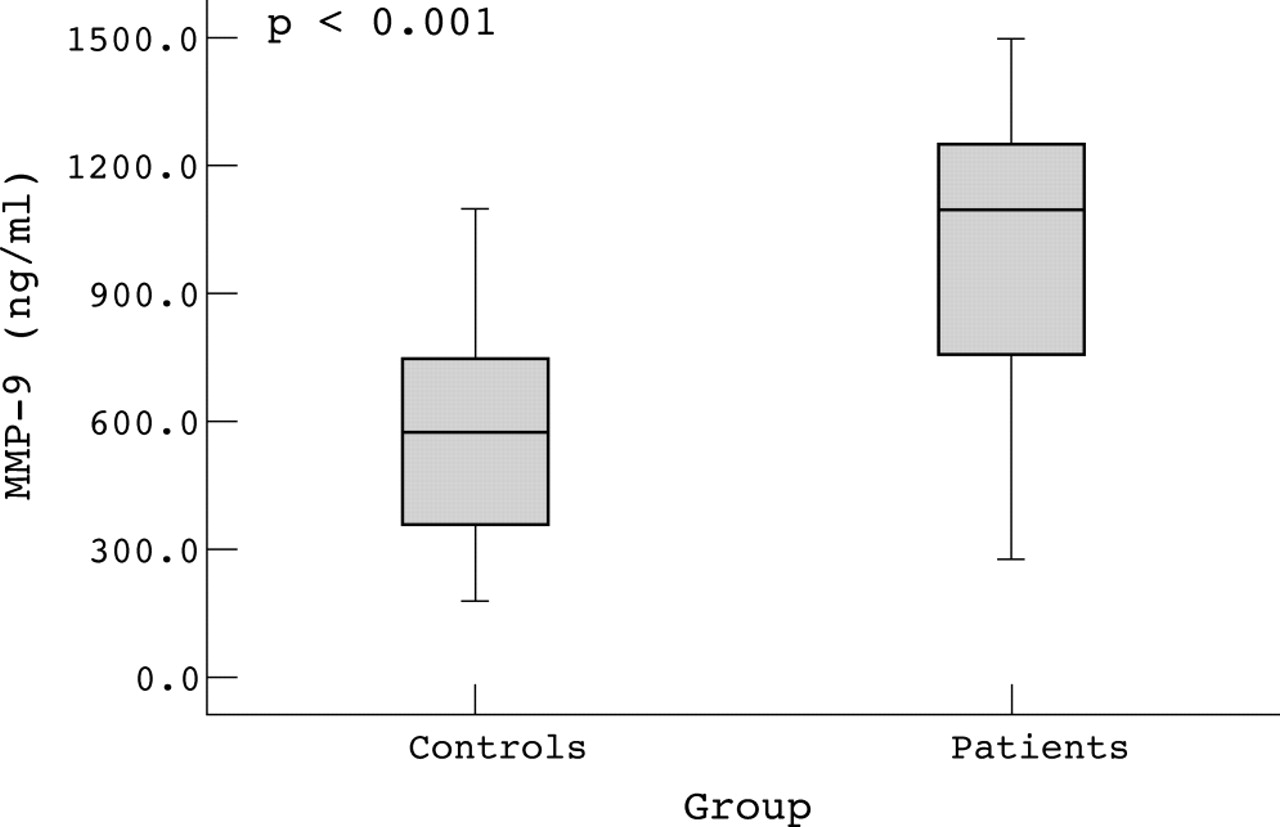{kind=link}
{kind=link}
{kind=link}
Abstract 233
234 SEVERE LEFT VENTRICULAR HYPERTROPHY (LVH) INDICATES THE FAILURE OF MYOCARDIAL ADAPTATION IN AORTIC STENOSIS (AS)
X. Y. Jin, J. R. Pepper.Academic Cardiac Surgery, NHLI, Imperial College, London, UK; Department of Cardiac Surgery, John Radcliffe Hospital, Oxford, UK
Background: The development of LVH has been regarded as an essential and beneficial myocardial adaptation in AS. The present study was aimed to test the hypothesis that the presence of severe LVH is the indicator of myocardial failure in AS patients.
Methods: Trans-oesophageal Echo and high fidelity left ventricular (LV) pressures were recorded immediately before cardiopulmonary bypass in 56 patients (age 63 ± 11 years, 34 males) undergoing aortic valve replacement (AVR) for AS. Transverse LV cavity dimension and wall thickness were derived from mid-cavity M-mode echocardiograms along with LV pressure by digitising. Cardiac index was measured by Swan-Ganz pulmonary catheter. Thus left ventricular mass index (LVMI), wall thickness/cavity radius (T/R), the magnitude and timing (with respect to ECG q wave) of peak systolic wall stress, peak Vcf, and peak myocardial power were all determined. Using 50 percentile of LVMI (160 g/m2) as a cut-off, LV systolic function of 33 patients with mild LVH (LVMI 131 ± 22, g/m2) was compared with that of 23 patients with severe LVH (LVMI 202 ± 31, g/m2).
Results: Age, gender, cardiac index, and aortic valve pressure gradient did not differ between the two groups (all p > 0.05). Left ventricular peak systolic wall stress (221 ± 71 v 216 ± 74, g/cm2) and T/R ratio (0.660 ± 0.22 v 0.70 ± 0.20) did not differ either (both p > 0.05). However, the severe LVH group has significantly lower magnitude and later timing of peak +dP/dt (1336 ± 456 v 1569 ± 404, mm Hg/sec, p = 0.049; 115 ± 20 v 101 ± 16, msec, p = 0.005); peak Vcf (1.63 ± 0.69 v 2.25 ± 0.77, cir/sec, p = 0.003; 263 ± 44 v 235 ± 38, msec, p = 0.013) and peak myocardial power (23.6 ± 10.8 v 29.5 ± 9.4, mW/cm3, p = 0.032; 233 ± 33 v 206 ± 30 msec, p = 0.002); and of lower LV ejection fraction (49 ± 16 v 59 ± 14, %, p = 0.020) when compared with those of the mild LVH group.
Conclusion: In AS, concentrical remodelling is an effective LV adaptation to increased systolic pressure and maintains normal myocardial contraction. The presence of severe LVH is, however, associated with significantly worse myocardial contractile function and should be considered as an indicator of myocardial failure rather than a beneficial LV adaptation in AS.
235 LEFT VENTRICULAR NON-COMPACTION (LVNC): INSIGHTS FROM CARDIOVASCULAR MAGNETIC RESONANCE (CMR) IMAGING
S. Petersen, J. Selvanayagam, F. Wiesmann, M. Robson, J. Francis, R. Anderson, H. Watkins, S. Neubauer.Department of Cardiovascular Medicine, John Radcliffe Hospital, Oxford, UK; Cardiac Unit, Institute of Child Health, University College London, London, UK
Left ventricular non-compaction is characterised by a non-compacted myocardial layer in the left ventricle. Cardiovascular magnetic resonance images this layer with unprecedented quality, particularly in the ventricular apex, where echocardiography has inherent difficulties. We aimed to test the diagnostic accuracy of CMR in distinguishing pathological LVNC from lesser degrees of trabecular layering seen in healthy volunteers, and in those with cardiomyopathies and concentric left ventricular (LV) hypertrophy, potential differential diagnoses. We hypothesised that pathological trabeculation could be distinguished by determining the ratio of non-compacted to compacted myocardium (NC/C ratio) and that right ventricle involvement would be common in LVNC.
Methods: We analysed magnetic resonance (MR) cine images using the 17 segment model in 45 healthy volunteers, 25 athletes, 39 patients with hypertrophic and 14 with dilated cardiomyopathy, 17 with hypertensive heart disease, and 30 with aortic stenosis, as well as images from seven patients previously diagnosed with LVNC in whom the diagnosis was supported by additional features.
Results: Areas of non-compaction were common, and occurred more frequently in all groups studied in apical and lateral, rather than in basal or septal, segments. A NC/C ratio of greater than 2.3 in diastole distinguished pathological non-compaction, with values for sensitivity, specificity, positive, and negative predictions of 86%, 99%, 75%, and 99%, respectively. All patients with LVNC also showed RV non-compaction.
Conclusion: Left ventricular non-compaction is diagnosed accurately with CMR using the ratio of non-compacted to compacted myocardium, and RV non-compaction is typically present. This technique should be valuable in clinical practice for diagnosis and assessment of suspected LVNC.
236 VARIABILITY IN PERICARDIOCENTESIS PRACTICE AMONG CARDIOLOGISTS IN THE UK–NEED FOR GUIDELINES
S. Balmain1, M. C. Petrie2, F. G. Dunn3.1Western Infirmary, Glasgow, UK; 2Royal Infirmary, Glasgow, UK; 3Stobhill Hospital, Glasgow, UK
Background: We performed an audit to evaluate current practice of pericardiocentesis procedures among cardiologists in the UK.
Methods: 640 questionnaires were sent to cardiologists selected from the UK Directory of Cardiology.
Results: Respondents: 274 completed questionnaires returned. Grade: 88% consultant; 9% specialist registrar; 3% staff grade. Workplace: 49% tertiary referral centres (TRCs); 51% district general hospitals (DGHs).
Indication: Unsurprisingly, the main indication for pericardiocentesis procedures performed (83%) was clinical tamponade. However, the majority of respondents (69%) felt that they would undertake pericardiocentesis on the basis of echocardiographic appearances alone. Echocardiographic appearances, which were felt to be an indication for drainage were: right ventricular diastolic collapse (69%); right atrial diastolic collapse (33%); Doppler variation of mitral inflow (7%); and large effusion size (3%). Procedural factors: more than 1500 procedures were performed over the past 2 years—54% in TRCs, 46% in DGHs. Three times as many supervised procedures were performed in TRCs. Forty-three percent of respondents performed five or more procedures and 24% supervised five or more procedures. Eighty-one percent felt that on-site cardiothoracic surgery support was not required. Eighty-seven percent would attempt to drain effusions >15 mm but only 32% would drain smaller effusions. A sub-xiphoid approach was most popular (89%). To guide the procedure, 78% routinely used echocardiography and 48% used fluoroscopy. Twenty percent used the electrocardiogram injury trace. Only a few (10%) injected contrast into the pericardial space. Complications: most commonly reported were ventricular puncture (n = 12, <0.8%), failed drainage (n = 10, <0.7%), and hepatic damage (n = 4, <0.3%). Right coronary artery dissection was reported once, as was splenic artery damage.
Conclusion: Although clinical tamponade is the commonest indication for pericardiocentesis, 69% of clinicians stated that they would drain a pericardial effusion on the basis of echo findings alone. Previous studies suggest that this approach does not positively affect clinical outcome. UK guidelines are required to standardise the indications for and approach to pericardiocentesis.