Article Text

Statistics from Altmetric.com
001 CORONARY FLOW RESERVE IS A POOR MARKER OF CORONARY MICROVASCULAR RESPONSE
N. Melikian1, M. Thomas2, M. Kearney1, B. De Bruyne3, A. Shah1, P. MacCarthy2.1Cardiovascular Division, King’s College School of Medicine at Guy’s King’s College and St Thomas’ Hospitals, London, UK; 2Cardiology Department, King’s College Hospital, London, UK; 3OLV Cardiovascular Center, Aalst, Belgium
Backgound: Coronary microvascular function (Mcor) has important emerging implications in clinical diagnosis, risk stratification, and prognosis of patients and its comprehensive assessment requires information on both endothelium dependent and independent coronary responses. Coronary flow reserve (CFR) is a commonly used index for Mcor, derived from ratio of maximal hyperaemic (often achieved with a non-specific vasodilator, adenosine) to basal coronary flow. We hypothesised that adenosine derived CFR may not adequately interrogate the endothelium dependent component of Mcor.
Methods and Results: A thermodilution technique (using intracoronary pressure wire) was employed to sequentially compare CFR (hyperaemia achieved with adenosine 140 μg/kg/ml via femoral vein) with % change in coronary flow in response to the endothelial agonist substance P (endothelium dependent response—20 pmol/min intracoronary infusion for 2 minutes) in 60 unobstructed coronary arteries of patients undergoing angioplasty to an adjacent vessel. Mean (SD) age of patients studied was 65 (10) years (55% male, 18% diabetic). Mean CFR was 2.9 (1.3) and substance P induced change in blood flow 22.2 (17.4)%. There was no correlation between CFR and coronary endothelial response (r = 0.1, p = 0.1) (fig 1). We then individually studied the relationship between CFR and coronary endothelial response, and established clinical markers of endothelial dysfunction (ED). There was a strong correlation between coronary endothelial response and patient’s Framingham Risk Score (FRS, a surrogate marker for cardiovascular risk factor clustering; hence an indirect measure of ED; r = −0.5, p<0.0001), but no correlation between CFR and FRS (r = 0.01, p = 0.7). Diabetic patients had significantly greater coronary endothelial dysfunction than non-diabetics (p = 0.001). CFR was not influenced by diabetes in this patient cohort (p = 0.4).
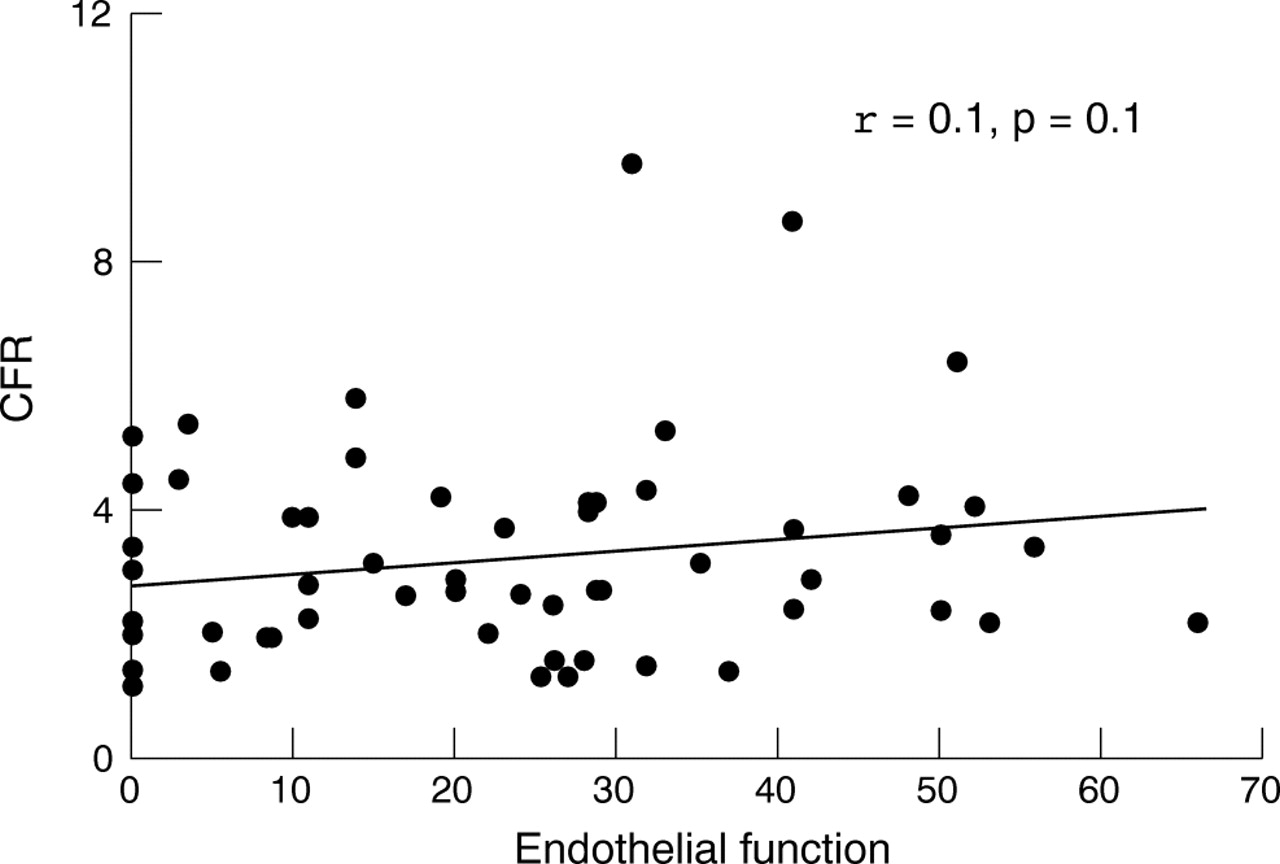
Abstract 001.
Conclusion: Adenosine derived CFR may not adequately interrogate the endothelium dependent component of the coronary microvasculature. We propose that information on both CFR and coronary endothelial function are needed to comprehensively assess Mcor.
coronary microvascular function; coronary flow reserve; coronary endothelial function
002 PRESSURE WIRE ASSESSMENT OF CORONARY ARTERY LESIONS: IS MAXIMAL HYPERAEMIA ALWAYS NECESSARY?
D. Conway, R. Townley.QEII Health Sciences Centre, Halifax, Canada
Background: Previous studies have shown that coronary lesions with a myocardial fractional flow reserve (FFR) >0.75, measured using an intracoronary pressure sensing guidewire during maximal hyperaemia, are unlikely to cause ischaemia and percutaneous coronary intervention (PCI) may be safely deferred for such lesions. Maximal hyperaemia requires administration of intravenous or intracoronary vasodilators, such as adenosine. However, we hypothesised that a “cut off” value might exist in the resting ratio of distal coronary pressure:aortic pressure (Pd:Pa) prior to adenosine, above which post-adenosine FFR is always >0.75. In other words, that adenosine may not always be required to identify haemodynamically insignificant lesions for which PCI can be deferred.
Methods: We performed a retrospective analysis of the procedural database at our cardiac catheterisation facility, identifying all cases undergoing FFR measurement between 1 May 2004 and 31 October 2005, respectively (375 vessels, 288 patients). Intracoronary adenosine boluses were used to achieve hyperaemia in all cases, maximum dose at the operator’s discretion. Using FFR>0.75 as our outcome, we used receiver operating characteristic (ROC) curve analysis to identify sensitivity and specificity of resting Pd:Pa values.
Results: Resting Pd:Pa values were documented for 224 of 375 vessels (60%). Of these, 186 (83%) had an FFR of >0.75, following maximum adenosine boluses of 24–180 μg (median 72 μg). The ROC curve for resting Pd:Pa values and FFR >0.75 is shown in the figure (area under curve = 0.96 (95% confidence interval 0.92 to 0.99)). A resting Pd:Pa value of >0.90 had 85% sensitivity and 95% specificity for FFR >0.75, while a resting Pd:Pa value of >0.96 had 45% sensitivity and 100% specificity for FFR >0.75. Of note, 83 of 224 vessels (37%) in our series had resting Pd:Pa of >0.96.
Conclusions: In our series of 224 vessels, resting Pd:Pa values >0.96 had 100% specificity for FFR >0.75, and were present in approximately 1 in 3 vessels evaluated. We propose that a resting Pd:Pa value of >0.96 indicates a haemodynamically insignificant stenosis and that adenosine administration may be unnecessary in such cases. Prospective studies should be performed to validate our findings and to determine whether PCI may be safely deferred based upon a resting Pd:Pa ratio of >0.96.
coronary; ischaemia; pressure wire

Abstract 002.
003 RAPID ASSESSMENT OF CORONARY ENDOTHELIAL FUNCTION USING AN INTRACORONARY PRESSURE WIRE
N. Melikian1, M. Thomas2, M. Kearney1, B. De Bruyne3, A. Shah1, P. MacCarthy2.1Cardiovascular Division, King’s College School of Medicine at Guy’s King’s College and St Thomas’ Hospitals, London, UK; 2Cardiology Department, King’s College Hospital, London, UK; 3OLV Cardiovascular Center, Aalst, Belgium
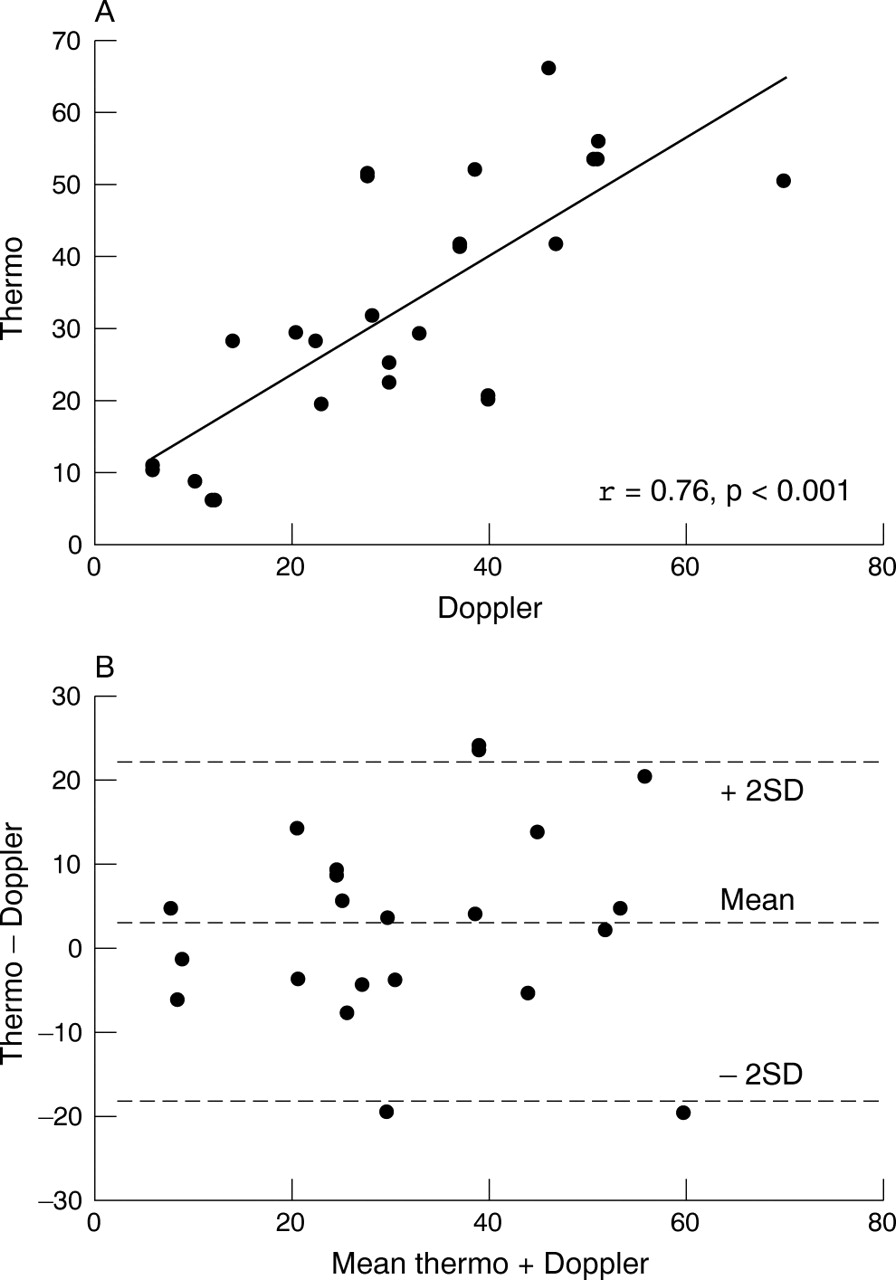
Background: Invasive clinical assessment of coronary endothelial function currently relies on intracoronary Doppler flow measurements (using the FloWire) and quantitative coronary angiography (QCA) to derive % changes in coronary blood flow from baseline in response to endothelial agonists. However, this method can be technically challenging with poor reproducibility. We hypothesised that changes in coronary flow derived by a thermodilution method, using the pressure wire (which can function as an intracoronary dual pressure temperature sensor), could also be used to reliably assess coronary endothelial function. The transit time (Tmn) of a bolus of room temperature saline using the latter technique is known to be inversely proportional to coronary flow.
Methods and Results: Twenty patients (mean age (SEM) 61 (2) years, 80% male) undergoing angioplasty to a single vessel were recruited and an adjacent coronary artery free of significant disease studied. The left anterior descending artery was studied in five, circumflex in eight, and right coronary artery in seven patients. We compared % change in absolute coronary flow from baseline using Doppler/QCA with % reduction in Tmn using thermodilution in response to 2 minute intracoronary infusion of the endothelial agonist substance P (20 pmol/min). The% mean change (range) in coronary blood flow measured by Doppler/QCA was 31.9 (3.8) (8.8–57.6) and thermodilution 33.3 (3.8) (5.5–55.7) (p = NS). There was a close correlation (r = 0.76, p<0.001) between% change in absolute coronary blood flow in response to substance P (measured by Doppler FloWire) and reduction in Tmn (thermodilution - measured with pressure wire) (panel A). Bland-Altman analysis revealed a mean absolute difference of 18 (19)% between the measurements, with 75% of cases having a difference of <20% (panel B).
Conclusion: Thermodilution is a simple and reliable technique for rapid assessment of coronary endothelial function and can be readily applied in routine clinical practice.
pressure wire; thermodilution; coronary endothelial function
Abstract 003.
004 FACILITATION WITH ABCIXIMAB COMPENSATES FOR DELAYS IN TRANSFER FOR PRIMARY PERCUTANEOUS INTERVENTION
E. Smith, A. Jain, R. DePalma, T. Keeble, M. Preston, A. Mathur, C. Knight, M. Rothman.Barts and the London NHS Trust, London, UK
Background: Transfer delays may negate the benefit of primary percutaneous intervention (PPCI). Debate continues as to the role of pharmacological facilitation as a bridge to PPCI. We investigated two access strategies delivering PPCI within a hospital network utilising upstream abciximab therapy.
Methods: Ninety three patients underwent PPCI at a cardiac centre. 52 transferred from a distant emergency department (AET) receiving abciximab in the A&E. 42 were taken directly from the community to the cath lab by ambulance (DA), receiving abciximab on arrival. Median (IQR) time from abciximab to balloon inflation was 74 minutes (65–86) AET versus 21 minutes (1–33) DA, p<0.001. Time from symptoms, call for help, and first hospital arrival to balloon inflation were recorded. TIMI flow and corrected TIMI frame count (cTFC) were assessed pre and post PPCI. Creatine kinase (CK) was measured for infarct size. Median follow up 15 (9–27) weeks.
Results: DA reduced time to reperfusion (table). TIMI flow and cTFC were superior prior to PPCI in the AET group, and similar post PPCI. CK was similar in both groups (Med (IQR): DA 721 iu (370–1451) v AET 800 iu (423–1887), p = 0.48). MACE (death/stroke/non-fatal MI) was 11.5% AET v 12% DA p = NS.
Conclusion: While direct ambulance access significantly reduced time to reperfusion, the two strategies were similar with respect to infarct size and clinical outcome. These data suggest that early facilitation with abciximab may compensate for interhospital transfer delays when this strategy cannot be avoided.
primary percutaneous intervention; pharmacological facilitation; ST segment elevation myocardial infarction
*p<0.05 compared to baseline
Table caption to follow
Abstract 004
005 ADDITION OF CLOPIDOGREL TO ASPIRIN FOLLOWING ACUTE CORONARY SYNDROME IS NOT ASSOCIATED WITH LONG TERM SURVIVAL BENEFIT
K. Bailey1, K. Viswanathan1, N. Artis1, C. Morrell1, R. Das1, N. Kilcullen1, J. Barth2, A. Hall1.On behalf of the EMMACE-2 Investigators. 1University of Leeds, Leeds, UK; 2Leeds General Infirmary, Leeds, UK
On behalf of the EMMACE-2 Investigators.
Objective: To assess the impact of combined antiplatelet therapy following acute coronary syndrome.
Design: Prospective observational registry.
Setting: 11 adjacent hospitals in the West Yorkshire region.
Patients: 2461 consecutive patients with a diagnosis of acute coronary syndrome were enrolled during a six month period. Demographic, clinical, and treatment variables were collected on all patients and their mortality was monitored through the Office of National Statistics. We now have mortality data for two years on all participants.
Results: Antiplatelet treatment was known in 2218 patients. 309 (12.6%) received no antiplatelet treatment, 1023 (41.6%) received aspirin alone, 107 (4.7%) received clopidogrel alone, and 779 (31.7%) received both aspirin plus clopidogrel. Patients receiving aspirin alone or aspirin plus clopidogrel were compared with regards to 30 day and long term all cause mortality. A statistically non-significant reduction in 30 day all cause mortality was observed in patients treated with both aspirin plus clopidogrel (33/779, 4.2%) compared to aspirin alone (62/1023, 6.1%) p = 0.08. Observed two year all cause mortality was significantly lower in those patients treated with both aspirin and clopidogrel (135/779, 17.3%) compared to aspirin alone (246/1023, 24.1%) p<0.01. As patients in the aspirin plus clopidogrel group were on average 4.5 years younger than the aspirin alone group, Cox Regression was performed adjusting for age, baseline heart rate and baseline systolic blood pressure. Following this adjustment there was no difference in all cause mortality at either 30 days or two years HR 1.03 (95% CI 0.83 to 1.28, p = 0.82).
Conclusions: The recent COMMIT trial demonstrated a small (absolute difference 0.9%) but significant reduction in 30 day mortality with addition of clopidogrel to aspirin. We found a similar size (1.9%) but statistically non-significant trend towards reduced mortality at 30 days, however this reduction is not maintained at 2 years when confounding factors (particularly age) are taken into account.
acute coronary syndrome; antiplatelet therapy; mortality
Abstract 005
006 THE SYNERGISTIC EFFECT OF THE ADDITION OF CLOPIDOGREL TO ASPIRIN IN REDUCING FUNCTIONAL ASPIRIN RESISTANCE IN PATIENTS UNDERGOING ELECTIVE PERCUTANEOUS CORONARY INTERVENTION
S. Bhattacharyya, A. Riddell, R. Rakhit.Royal Free Hospital, London, UK
Backgound: Aspirin resistance is an increasingly recognised phenomenon. It has been reported that up to 40% of patients undergoing percutaneous coronary intervention (PCI) may be aspirin resistant and they have a higher incidence of myonecrosis immediately post procedure. It is not known what the long term implications of this are. Patients undergoing PCI are routinely placed on clopidogrel just prior to and following the procedure. In the stroke population, it has been shown that the addition of clopidogrel reduces functional aspirin resistance. We studied the effect of the clopidogrel on aspirin resistance in patients undergoing PCI.
Methods: Sixty patients undergoing elective percutaneous coronary intervention over a three month period were selected. Aspirin resistance was measured using Platelet Function Analyser (PFA -100) before clopidogrel loading. Patients underwent their procedure and were discharged with clopidogrel 75 mg and aspirin. Their platelet function was repeated at 4 weeks using PFA-100. Aspirin resistance was defined as an epinephrine closure time below 170 seconds.
Results: Fifty seven patients were included in the trial. 16 (28%) of patients were aspirin resistant and 42 were not. Of these 16 aspirin resistant patients, at 4 weeks, 14 (88%) were no longer resistant with the addition of clopidogrel. (median closure times pre-clopidogrel: 121.5 (range 59–169), post-clopidogrel: 300 (range 103–300), p<0.0001) (fig).
Conclusion: Clopidogrel has a marked synergistic effect when combined with aspirin in reducing aspirin resistance. The clinical value of knowing aspirin resistance prior to PCI is limited given the effect of clopidogrel in reducing aspirin resistance post procedure.
aspirin; platelets; resistance

Abstract 006.
007 REPERFUSION DAMAGE PREVENTION BY LOCO REGIONAL ABCIXIMAB DURING PRIMARY PCI
B. Baglini.IsMeTT, University of Pittsburgh Medical Center, Palermo, Italy
Background: Prevention of reperfusion damage during PCI for acute myocardial infarction (AMI) represents a potential goal to limit myocardial necrosis and favour muscle salvage. According to previous experiences, it may be obtained by the infusion of specific drugs into the distal coronary bed before coronary reopening.
Aim: The aim of this study was to test the hypothesis that abciximab intracoronary loco regional treatment during AMI, before coronary reopening, can acutely improve angiographic and EKG parameters related to myocardial perfusion.
Patients: Ten patients (8 m, 2 f, mean age 56.3 years) with anterior AMI and proximal LAD occlusion were treated by primary PCI and loco regional infusion of abiciximab intracoronary bolus followed by i.v. infusion (Group 1). They were compared with 10 sex and age matched patients (7 m, 3 f, mean 56.8 years) with AMI and proximal LAD occlusion, who were treated by upstream abciximab i.v. bolus and infusion (Group 2). None of these patients required aortic counterpulsation.
Methods: In Group 1 patients, after crossing the occlusion with a coronary 0.014″ guidewire, a Diver infusion-aspiration catheter was positioned into the distal portion of the vessel and an abciximab bolus was infused. Following this, the catheter was pulled back and PCI was completed with balloon dilatation and stenting. Immediately after completing the procedure, the following parameters were measured: TIMI flow, TIMI corrected frame count, blush grade, arterial pressure, cardiac rate. Furthermore, the rate of EKG ST resolution (T/2) was also measured.
Results: Group 1 patients significantly differed from Group 2 for the following paraneters: TIMI corrected frame count (29±14 frames v 41±22 frames, p<0.01) and T/2 (45±14 sec v 72±37 sec, p<0.01). No significant difference was encountered for arterial pressure, cardiac rate, TIMI flow, and blush grade.
Conclusions: (1) Coronary loco regional therapy by abciximab infusion during primary PCI, before coronary reopening, can acutely improve angiographic and EKG parameters related to myocardial perfusion. (2) This novel approach to intracoronary pharmacologic therapy during AMI deserves further randomised studies.
acute myocardial infarction; PCI; reperfusion damage
008 DISSECTING THE GENETICS OF HEART DEVELOPMENT USING ENU MUTAGENESIS AND MAGNETIC RESONANCE IMAGING
G. Pieles, A. Franklyn, D. Norris, J. Schneider, S. Bhattacharya, D. Szumska.University of Oxford, WTCHG, Oxford, UK
Introduction: Congenital heart disease (CHD) is a frequent cause of death in infancy. To study the genetic mechanisms underlying cardiac malformations in an unbiased manner, we used random chemical mutagenesis with ethylnitrosourea (ENU) in the mouse as the best genetically tractable animal model for heart development. ENU mutagenesis, which results in untargeted point mutations, induces different types of alleles that can be responsible for developmental abnormalities. Because dominant mutations that result in heart malformations cause foetal or neonatal mortality, we studied recessive mutations responsible for abnormal cardiac development. Subsequent phenotype driven screening allowed us to identify mouse lines showing features of inherited heart disease.
Methods: Male Balb/c mice were injected intraperitonially with two doses of ENU (80 mg/kg of body weight). After recovering fertility, they were crossed to C3H females to produce G1 progeny heterozygous for ENU induced mutations. G1 males (50% carrying the mutation) were subsequently crossed to other C3H females and their female offspring (G2) were backcrossed to the male parent. G3 embryos were dissected and analysed using magnetic resonance imaging (MRI) in search of animals showing cardiac defects. MRI was carried out after paraformaldehyde fixation and the result was analysed at a resolution of 25.4×25.4×24.4 mm per voxel. To map the gene mutated in affected embryos we performed a genome-wide screen using pyrosequencing with 72 SNP markers that distinguish between Balb/c and C3H genomes. To follow up interesting lines we identified G2 male carriers and screened their progeny.
Results: We have generated several mutated mouse lines exhibiting various developmental abnormalities. This allowed us to identify novel mutations affecting heart and neural development, one of which was DMS113 ¡V a mutation known to cause exencephaly where, after scanning 155 embryos, we found 15 embryos showing atrial septal, ventricular septal, and outflow tract defects and a thin myocardial compact zone (fig). Using SNP markers and pyrosequencing we mapped the mutated region, linked to the aforementioned phenotype, to mouse Chr8. After screening 21 lines we identified five other lines exhibiting interesting cardiac phenotypes such as: (1 and 2) cervical lymphatic cysts and malpositioned heart, (3) VSD and outflow tract malformations, (4) VSD, ASD, dysplastic valves, renal agenesis, hind limb dysplasia, tail aplasia, (5) L-R patterning defects of heart and lungs. We are currently attempting to map the mutations linked to the above phenotypic abnormalities.
Conclusions: Genome-wide phenotype driven screens are a fast and unbiased tool to dissect the genetics of heart development. The cardiac phenotypes we identified can serve as models for human CHD. By identifying these defects and the causative genes our approach can help to elucidate the aetiology of common cardiac malformations.
congenital heart disease; ENU mutagenesis; atrioventricular defects

Abstract 008 figure 1.

Abstract 008 figure 2.
009 INTRAEMBRYONIC CITED2 IS NECESSARY FOR NORMAL CARDIAC DEVELOPMENT AND LEFT-RIGHT PATTERNING
S. MacDonald, S. Bamforth, C. Farthing, J. Schneider, C. Broadbent, A. Franklyn, S. Bhattacharya.Department of Cardiovascular Medicine, University of Oxford, Oxford, UK
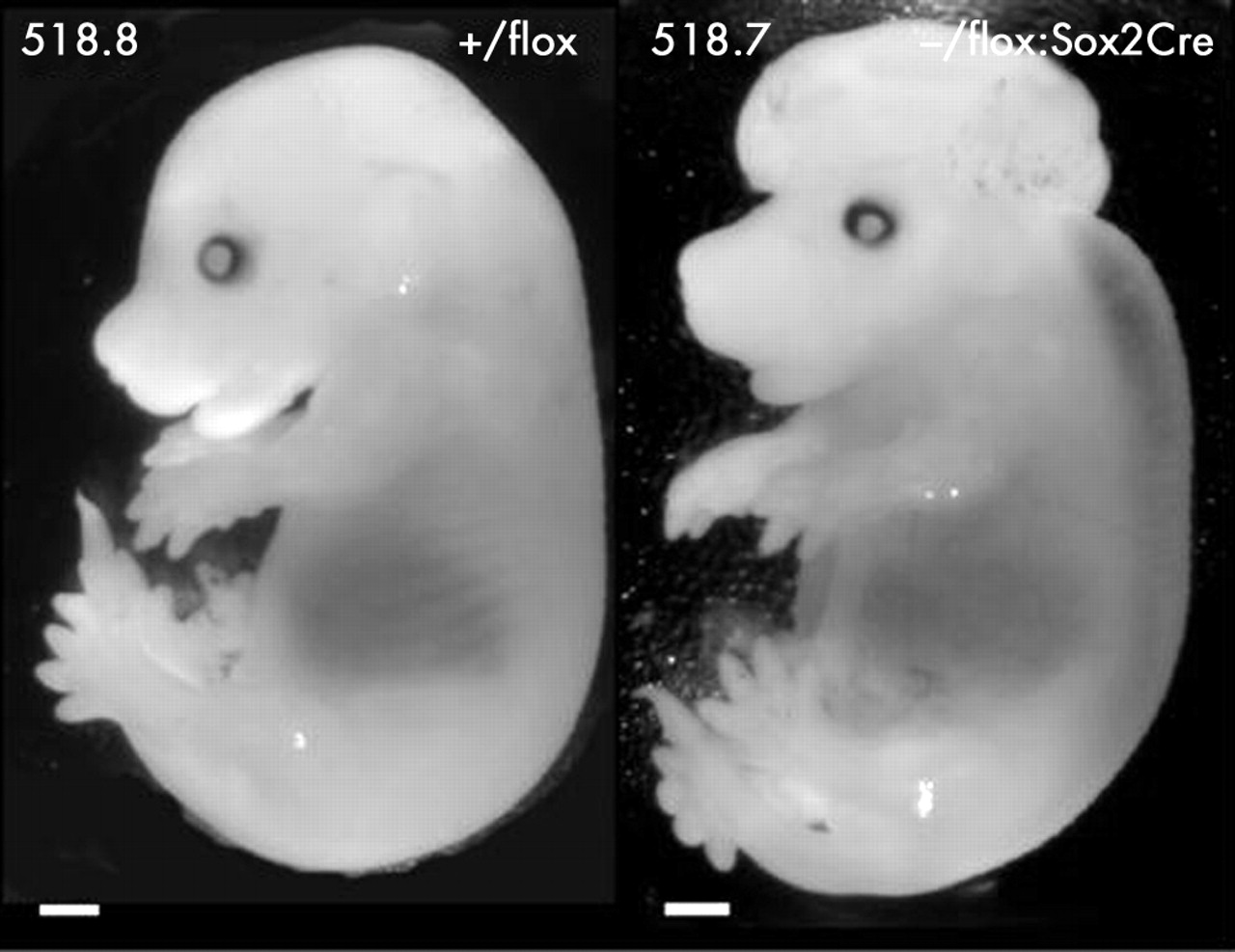
Introduction: Congenital heart disease (CHD) is a major cause of childhood morbidity and death in the West and understanding the developmental processes involved may offer new therapeutic avenues. Mice lacking Cited2, a transcriptional co-activator of transcription factor AP2, die in utero from complex cardiovascular abnormalities, neural tube defects, adrenal agenesis and show left-right cardiac patterning defects due to an abnormal Nodal-Pitx2 pathway. CITED2 variants are associated with CHD in humans (our unpublished data). Cited2 is expressed ubiquitously in the embryo and is also highly expressed in the placenta. The global Cited2 knockout results in loss of Cited2 in both intraembryonic and extraembryonic (placental) tissues. Moreover it replaces Cited2 with a constitutively active PGK-Neo cassette which can have unpredictable effects by activating neighbouring genes. To deconstruct the role of Cited2 in different embryonic tissues and to create a knockout without a residual PGK-Neo cassette, we developed a floxed allele of Cited2 and used cre-mediated recombination to determine the cellular locus of Cited2 function. Placental abnormalities have significant effects on cardiac development and to distinguish the role of intraembryonic versus extraembryonic Cited2 we deleted it in the intraembryonic tissues alone by crossing to Sox2Cre mice.
Methods: A breeding strategy was devised to generate Cited2-/flox:Sox2Cre mice with an expected frequency of 25%. Live born mice and embryos at 15.5 dpc were genotyped and examined macroscopically. Embryos were further analysed by magnetic resonance imaging (MRI). The efficiency of cre-mediated recombination was analysed by beta-galactosidase staining.
Results: All embryos containing the floxed allele and the Sox2Cre transgene stained blue showing recombination occurred correctly. No epiblast specific knock out mice were viable but all embryonic genotypes were present at 15.5 dpc suggesting late embryonic lethality (table 1). Macroscopically Cited2-/flox:Sox2Cre embryos demonstrated oedema, exencephaly, and iris coloboma, characteristics of the global Cited2 knock out phenotype (see fig). Embryo MRI revealed the full spectrum of embryonic defects including atrial and ventricular septal defects, outflow tract abnormalities, and left-right cardiac patterning defects, adrenal agenesis and hypo/asplenia, recapitulating the global knock-out phenotype.
Abstract 009 Genotypes of viable mice and 315.5 embryos.
Conclusions: We thus demonstrate that intraembryonic deletion of Cited2 recapitulates the global knockout phenotype, indicating that Cited2 is required in a cell-autonomous fashion for left-right patterning, cardiac, adrenal, and neural development. In future experiments we will use tissue specific Cre-expressing mice to perform temporal and spatially controlled deletions of Cited2. This will enable us to understand how Cited2 controls cardiac development.
Cited2; congenital heart disease; development
Abstract 009.
010 CITED2 HAPLOINSUFFICIENCY IS ASSOCIATED WITH CONGENITAL HEART DEFECTS IN MOUSE AND MAN: INTRODUCING THE GO-CHD STUDY
J. Bentham1, S. Bamforth1, J. Braganca1, S. Carballo1, A. Michell1, M. Bilski1, C. Broadbent1, C. Farthing1, A. Franklyn1, J. Schneider1, S. Adwani2, K. Devriendt3, B. Keavney4, J. Goodship4, P. Scambler5, H. Watkins1, S. Bhattacharya1.1Department of Cardiovascular Medicine, University of Oxford, Oxford, UK; 2Department of Paediatric Cardiology, John Radcliffe Hospital, Oxford, UK; 3Centrum Menselijke Erfelijkheid, Herestraat, Germany; 4Institute of Human Genetics, Newcastle-upon-Tyne, UK; 5Institute of Child Health, University College London, London, UK
Mutations in TFAP2B (Char syndrome) and CREBBP/EP300 (Rubenstein Taybi syndrome) are associated with cardiac malformations in mouse and man. The transcriptional co-activator CITED2 links transcription factor AP2 to the coactivators CREBBP/EP300 and controls cardiac development via a Nodal-Pitx2c pathway. CITED2 knockout mice also have cardiac malformations including VSDs, ASDs, DORV, TOF, TGA, and truncus arteriosus. Intriguingly, when these mice were bred on a pure genetic background to minimise the effect of genetic modifiers, more complex left-right patterning cardiac lesions were apparent. From this arises the hypothesis that mutations in genes controlling left-right patterning could result in common congenital heart disease (CHD), as a form fruste of a left-right patterning defect.
Here we show that up to 22% of Cited2+/− mice do not survive to weaning and 11% have cardiac defects in utero indicating that Cited2 haploinsufficiency causes CHD in the mouse and is therefore a candidate for human CHD.
To test this hypothesis, we screened 152 patients with different forms of CHD, and identified four with CITED2 variants. Three variants, p.His39del, p.His160Leu, and p.Gly194_Gly195del, were identified in normal controls, but a fourth, p.Thr166Asn, was not observed in a panel of 191 control individuals.
Abstract 010
The p.Thr166Asn variant was inherited from an apparently unaffected parent of the proband. In transient transfection assays, CITED2-p.Thr166Asn was severely defective in TFAP2 co-activation, as was an engineered p.Thr166Ala allele, indicating that the Thr166 residue side-chain plays a specific role in CITED2 co-activation function.
The Thr166 residue is conserved only in placental mammals, suggesting a specific role for this residue in eutherian cardiac development. Our results suggest that CITED2 haploinsufficiency is associated with cardiac malformation in mouse and man, and support the idea that functional variation in genes controlling left-right patterning can result in common congenital heart disease.
We plan to extend this work in collaboration with UK paediatric cardiology and adult CHD centres as part of the Genetic Origins of Congenital Heart Disease Study (GO-CHD Study). The aim of the study is to identify mutations in genes which cause CHD and use these mutations to understand the molecular mechanisms of cardiac development and disease. Using Cited 2 as an example, this abstract demonstrates that this is a powerful approach to understanding the basis of congenital heart disease.
cardiac development; congenital heart disease; Cited 2

Abstract 010.
011 EFFECT OF CHRONIC AFTERLOAD INCREASE ON LV MYOCARDIAL FUNCTION IN PATIENTS WITH CONGENITAL LEFT SIDED OBSTRUCTIVE LESIONS: DOES DISTANCE MATTER?
Y. Lam, M. Kaya, W. Li, O. Goktekin, M. Gatzoulis, M. Henein.Royal Brompton Hospital, London, UK
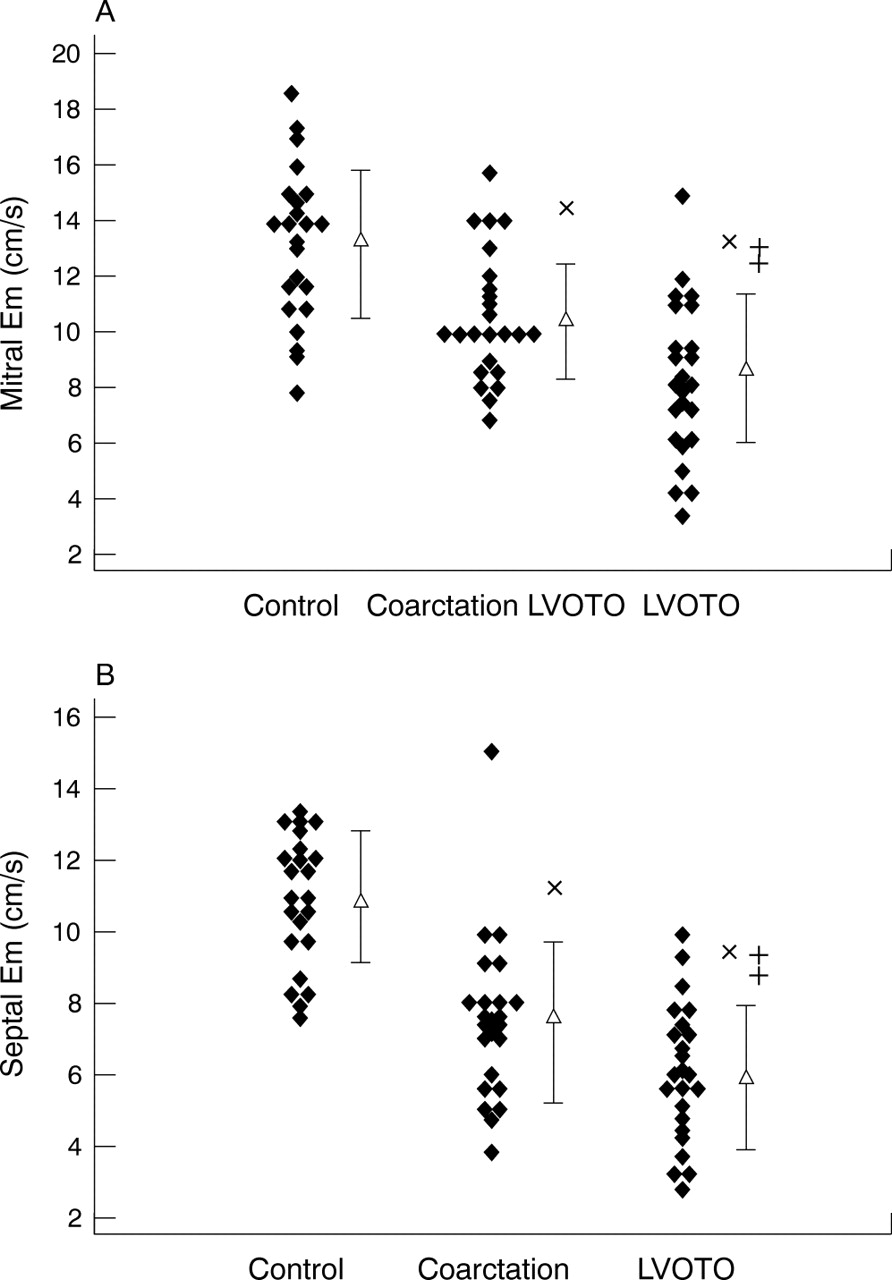
Background: Long axis function that represents the endocardium is sensitive for assessing LV systolic and diastolic behaviour in aortic stenosis. Its clinical role in aortic coarctation patients has not been thoroughly investigated. Furthermore, the effect of pressure overload distance on LV function remains understudied. Methods: We studied 23 consecutive patients with severe LV outflow tract obstructive lesions (subaortic or aortic stenosis) and aortic coarctation and compared them with 23 normal controls. LV long axis motion was recorded by M-mode and TDI techniques.
Results: The TDI lateral and septal long axis systolic velocities (LSm and SSm), early diastolic velocities (LEm and SEm) and M-mode systolic amplitudes (LSE and SSE) were lower in coarctation and LVOTO patients than in controls (LSm, 7.1±2.0 cm/s and 6.7±1.6 cm/s v 9.7±1.9 cm/s; SSm, 6.3±1.4 cm/s and 5.4±1.1 cm/s v 7.7±1.3 cm/s; LEm, 10.5±2.3 cm/s and 8.2±2.8 cm/s v 13.1±2.7 cm/s; SEm, 7.4±2.3 cm/s and 6.0±1.9 cm/s v 10.8±1.8 cm/s, LSE 1.3±0.2 cm and 1.4±0.3 cm v 1.6±0.3 cm; SSE 1.2±0.2 cm and 1.2±0.2 cm v 1.4±0.2 cm, p<0.01 for all). Compared with coarctation patients, LVOTO patients had lower Em velocities and more long axis inco-ordination both at lateral and septal sites (p<0.005 for all). No significant difference in LV fractional shortening, ejection fraction, total isovolumic time, myocardial performance index, or LV filling parameters was seen between groups.
Conclusions: LV long axis function is impaired in patients with chronic increase in afterload. A higher percentage of long axis incoordination and a lower Em velocity independent of systolic function and blood pressure in LVOTO than coarctation patients may suggest difference in coronary flow to the subendocardium as a result of different pressure overload distances.
aortic stenosis and coarctation; overloading distance; diastolic dysfunction
Abstract 011.
012 A VERY HIGH PREVALENCE OF PATENT FORAMEN OVALE IN PATIENTS WITH VARICOSE VEINS
U. Velupandian1, B. Raju1, J. Morris2, S. Ray2, C. McCollum1.1University of Manchester, Manchester, UK; 2South Manchester University Hospitals NHS, Manchester, UK
Introduction: Patent foramen ovale (PFO) has a prevalence of 27.3% in the general population varying from 34.3% in first three decades of life to 25.4% through 4th to 8th decade. It is associated with cryptogenic stroke in young adults, decompression sickness with neurological symptoms in divers and possibly migraine with aura. Isolated cases of stroke have been reported following injection sclerotherapy or surgery for varicose veins.
Methods: We report a study recruiting 60 patients with long saphenous system varicose veins and sapheno-femoral junction incompetence who underwent screening for a venous-to-arterial circulation shunt (vaCS) by TCD or PFO by TTE prior to microfoam injection sclerotherapy. Simultaneous transcranial doppler (TCD) and Transthoracic echocardiogram (TTE) with second harmonic imaging was performed during antecubital intravenous injections of agitated saline-air-blood microbubble contrast using a standardised protocol at rest, during cough and during a Valsalva manoeuvre. If a functionally significant shunt (FSS) was detected by either TCD or TTE further injections were deferred. FSS was defined by TCD as ⩾15 microbubbles within 12 cardiac cycles following injection and by TTE as the appearance of ⩾10 microbubbles in the left atrium within three cardiac cycles of maximum right atrial opacification. All data collected were analysed by observers blind to clinical details and the results of other investigations.
Results: Sixty patients (mean age 47.2 years; range 18.9 to 67.1 years) underwent screening. The frequency of a vaCS by TCD was 51.7% (95% CI 39% to 64%) and a PFO by TTE was 46.7% (95% CI 35% to 59%). These values were significantly higher when compared with reported prevalence of 25.4% in this age group (chi-square goodness of fit tests: p<0.001). Agreement between TTE and TCD was 85% (kappa = 0.701). FSS detected was 27 (45%) by TCD and 20 (33.3%) by TTE. When compared with healthy controls from the YAMIS (n = 210; mean age = 39.2 years) and MEMORY (n = 165; mean age = 76.7 years) case control studies in the same geographical population both of which used TCD for vaCS detection, the frequency of an FSS by TCD for the varicose veins group (45%; 95% CI 33% to 58%) was significantly higher than healthy controls in YAMIS (27.6% ; chi-square test: p = 0.016) and MEMORY (21.8%; χ2 test: p = 0.001).
Conclusion: An unusually high prevalence of PFO was noted in patients with long saphenous varicose veins. The frequency of a functionally significant shunt was significantly higher than in two large populations of healthy controls. This association suggests the possibility that the development of venous valves and the atrial septum may have genetic factors in common.
Abstract 012 table 1: Results of screening of varicose veins patients (total, n = 60)
Abstract 012 table 2: Comparison of varicose veins group with controls from YAMIS and MEMORY case control studies
patent foramen ovale, PFO; shunt, venous to arterial; vacs; veins varicose
013 QRS DURATION AND ITS RELATIONSHIP TO RIGHT VENTRICULAR MECHANICAL ASYNCHRONY IN ADULT PATIENTS AFTER REPAIR OF TETRALOGY OF FALLOT
A. Uebing, S. Babu-Narayan, G. Diller, O. Goktekin, M. Henein, D. Gibson, M. Gatzoulis, W. Li.Royal Brompton Hospital, London, UK
Background: Patients with repaired tetralogy of Fallot (ToF) frequently have right ventricular (RV) dysfunction and greatly prolonged QRS duration (QRSd) and have therefore been considered for cardiac resynchronisation therapy (CRT). However, little is known about the relationship between QRS duration and RV mechanical asynchrony.
Aim: To assess RV mechanical asynchrony in repaired ToF patients and to explore its relationship to QRSd.
Methods: Sixty seven ToF patients (aged 34±12 years; 27±8 years after repair) and 35 age matched controls were studied by Doppler and long-axis echocardiography. The timing of RV mechanical events (pre-ejection time (PET); ejection time (ET), isovolumic relaxation time (IVRT), filling time (FT)) was measured from pulmonary and tricuspid valve Doppler recordings. Long-axis recordings were acquired in all subjects from the RV free wall. In a subset of 62 subjects (37 ToF patients/25 controls) additional long-axis recordings were obtained from the RV outflow tract (RVOT) with M-Mode at the level of the pulmonary valve. To determine mechanical asynchrony the delay between Q-wave and onset of long-axis shortening (qOS) of RV and RVOT was measured.
Results: PET and ET were significantly prolonged in the group of ToF patients whereas FT was reduced (see table; time intervals are expressed in seconds per minute to correct for differences in heart rate).
Abstract 013
There was some correlation between PET and QRSd in ToF patients (r = 0.42; p<0.0001) but PET was within normal limits in 52/67 patients regardless of QRSd. qOS RV correlated with QRSd (r = 0.55; p<0.00001) but was normal in 25/67 ToF patients regardless of QRSd. qOS RVOT and the delay between qOS RVOT and qOS RV correlated closest with QRSd (r = 0.82; p<0.00001 and r = 0.69; p<0.0001, respectively). There was a correlation as well between qOS RVOT and PET (r = 0.52; p<0.001).
Conclusion: Patients after repair of ToF had a prolonged PET and ET and a reduced FT. QRS duration is related to PET and RV free wall shortening but much more so to a delay in shortening of the RV outflow tract. Thus, QRSd reflects abnormalities of the cardiac cycle and abnormal mechanics of the RV free wall and particularly the infundibulum. However, mechanical asynchrony cannot be assumed on the basis of QRSd alone. RV electromechanical interactions studied with echocardiography may help to identify ToF patients potentially suitable for CRT.
tetralogy of fallot; cardiac resynchronisation; mechanical asynchrony
014 SYSTEM BLOOD PRESSURE, LEFT VENTRICULAR MASS, AND FUNCTION AFTER SUCCESSFUL ENDOVASCULAR STENTING OF AORTIC COARCTATION
Y. Lam, M. Kaya, M. Henein.Royal Brompton Hospital, London, UK
Background: The haemodynamic response and clinical outcome late after surgically repaired coarctation of aorta has been well documented in the literature but limited data is available regarding blood pressure control and left ventricular function in patients received endovascular stenting of aortic coarctation.
Objective: We aim to study the effect of endovascular stenting of aortic coarctation on blood pressure control, LV mass (LVM) regression, and LV long axis function. Methods: We performed echocardiographic analysis in 21 patients (age 30+10 years) before and 13+10 months after coarctation stenting from year 2002–04. Measurements of blood pressures, LV mass and LV long axis function were made. The post-stenting results were compared with pre-stenting ones (group 1), 22 patients post-surgical repair (group 2) and 30 normal controls (group 3) Results: The peak systolic gradient across the coarctation site decreased from 55±15 mmHg to 18±8 mmHg after stenting (p<0.001). Systolic and mean blood pressure normalized (147±21 to 135±16 mmHg and 100±12 to 93±9 mmHg, p<0.05 for all), LV mass regressed (257.6±117.8 to 212.2±70.9 g, p<0.05) and LV long axis function improved (LV lateral and septal M-mode long axis amplitudes: LSA 1.2±0.2 to 1.3±0.2 cm, SSA 1.1±0.3 to 1.3±0.3 cm; TDI systolic velocities at lateral and septal sites: LSm, 6.5±1.4 to 7.9±1.7 cm/s; SSm, 5.8±1.2 to 7.3±1.6 cm/s; TDI septal early diastolic velocities: SEm 6.7±1.5 to 7.8±1.9 cm/s; septal E/Em ratio: 14.8±5.3 to 11.8±3.9 p<0.05 for all) after stenting. Compared to normal controls, both stented and surgically repaired patients have higher LV early filling velocities (E), E/Em ratios and lower systolic (Sm) and diastolic (Em) velocities (p<0.01 for all).
Conclusion: Endovascular stenting of aortic coarctation results in better blood pressure control, regression of LVM, and improvement in LV long axis function that may provide insight into long term outcome of the patients. The invaluable use of long axis function in assessing and follow up subendocardial behaviour in patients with either stented or surgically repaired coarctation warrants further studies.
coarctation of aorta; endovascular stenting; LV long axis function
015 PERCUTANEOUS CLOSURE OF BAFFLE LEAKS IN ADULT PATIENTS WITH MUSTARD OR SENNING REPAIRS FOR TRANSPOSITION OF THE GREAT ARTERIES: EARLY EXPERIENCE
K. English, J. Thomson, J. Gibbs, M. Blackburn.Yorkshire Heart Centre, Leeds, UK
Introduction: Mustard and Senning procedures were the operations of choice for infants born with transposition of the great arteries from the mid 1960s, until superseded in the 1980s by the arterial switch operation. The long term outcome of these patients is good, with actuarial survival rates of 90%, and 80% respectively at 10 and 30 years post surgery. Most of these patients lead good quality lives, with 96% in NYHA class I or II. Long term follow up in expert centres is recommended because of problems arising in adulthood. These include brady and tachy arrhythmias, systemic ventricular dysfunction, systemic AV valve regurgitation, and baffle related problems. Baffle leaks in patients following Mustard or Senning operations can be considered as an abnormal connection between the pulmonary venous atrium and the systemic venous atrium. Flow can be either predominantly left to right or right to left depending on minor degrees of baffle stenosis and on ventricular compliance. Patients with significant baffle leaks and right to left shunting are desaturated, particularly on exertion, polycythaemic, and at risk of paradoxical thromboembolisation.
Methods: We describe six patients in whom we planned to close intra-atrial baffle leaks percutaneously. All patients underwent attempted percutaneous closure of their baffle leak(s) under general anaesthetic with transoesophageal echo and fluoroscopic guidance.
Abstract 015 table 1
Results: Baffle leaks were successfully percutaneously closed in 5 of the 6 patients, using 1 (n = 3) or 2 (n = 2) Amplatzer ASD devices of the following sizes; 1×6 mm, 2×12 mm, 2×14 mm, 1×20 mm, 1×22 mm. In one patient (6) the device could not be deployed from the femoral route because of the unfavourable angle. Access from the internal jugular veins was not successful because of previous instrumentation as a child. In one other patient (4) the device was deployed via the right internal jugular vein because of known occlusion of both femoral veins. All other devices were deployed via the femoral vein. Apart from the problems with venous access in patient 6, there were no other peri-procedural complications.
Abstract 015 table 2
Conclusions: Percutaneous closure of baffle leaks in patients with Mustard or Senning operations for TGA is feasible, and can result in dramatic improvements in symptoms and polycythaemia. An important factor to note is whether the coronary sinus was redirected at the time of original surgery to the systemic venous atrium, as benefit may be limited if CS drainage remains in the pulmonary venous atrium. In addition, this procedure should reduce the risk for paradoxical thrombo-embolisation in this group of patients.
mustard; baffle; amplatz
016 CARDIOLOGY SERVICES FOR ADULTS WITH CONGENITAL HEART DIEASE: SECONDARY CARE CARDIOLOGISTS CALL FOR MORE SPECILIST SUPPORT
L. Wilkins1, S. Sethi2.1Stockport NHS Foundation Trust, Stockport, UK; 2Cumbria and Lancashire Specilised Commissioning Team, Preston, UK
Introduction: The prevalence and complexity of congenital heart disease lesions seen in adulthood has increased significantly during the last two decades. As part of a review of adult congenital heart disease (ACHD) services in the North West of England, secondary care cardiologists were asked whether they cared for patients with moderate/complex lesions; about shared care with tertiary services; the adequacy of information transfer between paediatric and adult services and about gaps in current ACHD services.
Methods: In June 2004 a six page questionnaire was sent to all (59) cardiologists working in district general hospitals in the North West of England. 44 (75%) consultants responded. ACHD complexity was categorised into simple or moderate/complex based on the Bethesda classification (floppy mitral valve and non-stenotic congenital bicuspid aortic valve excluded).
Results: Of the respondents: All provided follow up for patients with simple ACHD. 59% had some patients with moderate/complex ACHD. Only 17% estimated they see more than 1–2 patients with moderate/complex lesions per quarter. 34% referred all moderate/complex patients to tertiary care. 55% had some patients whose care is shared with a tertiary centre. One held a dedicated ACHD clinic. 59% felt at the time of transfer, paediatricians “always” or “most of the time” provided adequate information about the past history of patients with moderate/complex lesions but only 33% felt this was true regarding an adequate management plan (simple lesions 75%, 37%). 73% felt secondary care cardiologists are currently caring for ACHD patients who would be better cared for by a specialist service. 23 cardiologists responded to an open question about gaps in current ACHD care. Areas identified included:
-
Lack of ACHD training
-
Difficulty maintaining diagnostic and management skills given ACHD rarity
-
Inability to access paediatric notes
-
Poor information and patients “getting lost” at transfer
-
Fragmented services
-
Poor communication between secondary, tertiary, and paediatric services
-
Insufficient support from tertiary services
-
Limited shared care opportunities
-
No regional specialist service.
Conclusion: Generalist cardiologists are caring for patients with moderate/complex ACHD lesions, but see such patients infrequently, lack training in ACHD, and feel unsupported by tertiary care. Indeed, 73% of respondents felt secondary care cardiologists are currently caring for ACHD patients who would be better cared for by a specialist service. In line with the ESC’s guidelines1 consultants called for support from, and the development of, a specialised regional ACHD centre.
1
adult congenital heart disease; secondary care; consultant survey
017 THE AGE AND GENDER RELATED PREVALENCE OF THE METABOLIC SYNDROME AMONG UK INDIAN ASIANS AND EUROPEAN WHITES: FIRST RESULTS FROM THE LONDON LIFE SCIENCES POPULATION (LOLIPOP) STUDY
J. Chambers1, E. Lim2, P. Jain2, D. Singh2, P. Elliott1, J. Kooner3.1Department of Epidemiology and Public Health, Imperial College, London, UK; 2Ealing Hospital, London, UK; 3NHLI, Hammersmith Hospital, Imperial College, London, UK
Background: The metabolic syndrome of insulin resistance is increasingly recognised as a risk factor for CVD. Previous studies have demonstrated that the metabolic syndrome is more common in Indian Asians compared to European whites. We report the age and gender related prevalence of the metabolic syndrome, and its related disturbances of central obesity, elevated blood pressure, glucose and triglycerides, low HDL cholesterol among participants in the London Life Sciences Population (LOLIPOP) Study.
Methods: The LOLIPOP study is a population based study of Indian Asians (IA) and European whites (EW) aged 35–75 years, identified from the lists of 58 GPs in West London. To date 18 456 participants (IA: 8791 male, 4013 female; EW: 3846 male, 1806 female) have been recruited, with a response rate was 61%. Clinical, cardiovascular and drug history, anthropometric measurements were recorded for each subject, as well as fasting measurements of glucose and lipid profile. The prevalence of the metabolic syndrome was determined using Adult Treatment Panel (ATP) III criteria.
Results: Our results show that the prevalence of the metabolic syndrome increases with age in both Indian Asians and Northern Europeans (table). In each age group, the prevalence of the metabolic syndrome is higher in Indian Asians that Europeans (fig). Compared to European whites, the age adjusted prevalence of the metabolic syndrome is 41% greater in Indian Asian men and 140% greater in Indian Asian women. Furthermore the metabolic syndrome appears to develop almost 10 years earlier among Indian Asian men, and 20 years earlier among Indian Asian women, compared to European white men and women respectively.
Conclusions: Our results show striking differences in the age and gender related prevalence of the metabolic syndrome in Indian Asians than Europeans. Follow up of this cohort will help to determine the extent to which these differences contribute to higher cardiovascular events in Indian Asians compared to European whites.
Abstract 017
Indian Asians; metabolic syndrome; gender

Abstract 017.
018 INVESTIGATION OF CARDIOVASCULAR RISK FACTORS AMONG UK INDIAN ASIANS AND EUROPEAN WHITES: THE LONDON LIFE SCIENCES POPULATION (LOLIPOP) STUDY
J. Chambers1, E. Lim2, D. Singh2, P. Jain2, P. Elliott1, J. Kooner3.1Department of Epidemiology and Public Health, Imperial College, London, UK; 2Ealing Hospital, London, UK; 3NHLI, Hammersmith Hospital, Imperial College, London, UK
Background: Coronary heart disease (CHD) mortality is 50% higher in UK Indian Asians than European whites. Strikingly, CHD risk is threefold higher in Asian men below 40 years compared to Europeans. We describe the London Life Sciences Population Study (LOLIPOP) cohort study, aimed at identifying incident events and contribution of conventional and novel risk factors to CHD in Indian Asians and European whites.
Methods and Results: We have established a collaboration with 58 GPs in West London (Ealing, Hammersmith, and Hounslow) to deliver NSF Standards 3 and 4 in Primary Care. These boroughs are home to one of the largest Asian populations outside India. All men and women aged 35–75 years registered with these GPs (n = 52 236) will be invited for cardiovascular assessment by a trained nurse, including medical and drug history, cardiovascular risk factors, demographic details, physical measurements, (blood pressure, height, weight, waist-hip girth ratio), urinalysis, ECG, and biochemistry including fasting glucose and lipids. The current response rate is 62%, and we expect ∼32 000 people to attend for assessment.
Indian Asian and European white subjects attending for cardiovascular assessment are invited to participate in the LOLIPOP cohort study. Consenting subjects provide additional whole blood, plasma and serum samples (stored for future biochemical/genetic analyses), and permission to obtain outcome data. Over 90% of eligible subjects attending for cardiovascular risk assessment agree to participate in the LOLIPOP cohort study. Recruitment will continue until there are at least 12 000 Indian Asian, and 12 000 European white subjects. LOLIPOP participants will be followed up over every five years for incident cardiovascular events, by reassessment of survivors, interrogation of GP and local hospital records, and through the Office for National Statistics. All data are stored in a dedicated, secure, purpose written LOLIPOP database.
Recruitment to the LOLIPOP study commenced in 2002. To date 30255 people have been invited, and 18 456 people have attended for assessment (see table—Indian Asians (IA), European whites (EW)). LOLIPOP recruitment will be complete by end 2006.
Conclusions: The LOLIPOP cohort study is a large, prospective population study of cardiovascular disease in Indian Asians and European whites in West London aimed at identifying precise, prospective estimates of disease incidence, and accurate assessment of risk relationships. Study of this well characterised cohort combined with novel genomic, metabolomic, proteomic, and bioinformatic will enhance our understanding of cardiovascular disease in the two populations.
Abstract 018
Indian Asians; prospective; population
019 CHRONIC KIDNEY DISEASE AS A CARDIOVASCULAR RISK FACTOR IN UK INDIAN ASIANS COMPARED TO UK NORTHERN EUROPEANS: THE LONDON LIFE SCIENCES PROSPECTIVE POPULATION STUDY (LOLIPOP)
E. Lim1, L. Lightstone2, J. Chambers1, P. Roderick3, M. Mullee3, J. Kooner1.1Imperial College, London, UK; 2Renal Section, Imperial College, London, UK; 3Applied Clinical Epidemiology Group, University of Southampton, Southampton, UK
Background: Coronary heart disease (CHD) mortality is substantially higher in UK Indian Asians (IA) compared to Northern Europeans (NE). The mechanisms underlying this excess risk are not clear. Since chronic kidney disease (CKD) is known to be a powerful cardiovascular risk factor in NE, and the incidence of end-stage renal failure needing dialysis is 3–5 times higher in IA compared to NE in the UK, we systematically investigated the prevalence of CKD in IA compared to NE.
Methods: Male and female subjects aged 35–75 years were recruited from the practice lists of 58 General Practitioners, as part of the London Life Sciences Prospective Population (LOLIPOP) study. Traditional cardiovascular risk factors and GFR was assessed by a trained nurse. Prevalence of CKD (defined as GFR <60 ml/min/1.73 m2) and more severe renal impairment (GFR <45 ml/min/1.73 m2) was estimated using the modified Modification of Diet in Renal Disease (MDRD) formula.
Results: 10 805 men (3068 NE; 7017 IA) and 4181 women (1380 NE; 2801 IA) were enrolled. In IA and NE respectively, the prevalence of DM was 8.2% versus 20.9%; for previously diagnosed hypertension, 31.5% versus 39.3% (p<0.0001 for both). Crude prevalence of CKD is shown in the table.
Abstract 019
In logistic regression models adjusting for age only, IA were no more likely than NE to have CKD (adjusted odds ratio for IA men and IA women 1.17 (CI 0.96 to 1.44) and 0.62 (CI 0.52 to 0.74) respectively). However, IA men were more likely to have GFR<45 ml/min/1.73 m2 (adjusted odds ratio for IA men and women 3.3 (CI 1.9 to 5.9) and 0.98 (CI 0.62 to 1.57) respectively). Findings following adjustment for age, diabetes, hypertension, smoking and known vascular disease were similar. IA were again no more likely than NE to have CKD (adjusted odds ratio for IA men and IA women 1.03 (CI 0.82 to 1.3) and 0.57 (CI 0.46 to 0.72) respectively) and IA men were more likely to have GFR<45 ml/min/1.73 m2 (adjusted odds ratio for IA men and women 2.49 (CI 1.35 to 4.61) and 0.74 (CI 0.41 to 1.32) respectively).
Conclusion: Prevalence of CKD (MDRD GFR<60 ml/min/1.73 m2) is lower in UK IA compared to NE. Since the incidence of ESRF needing dialysis is 3–5 times higher in IA compared to NE, it is possible that IA with CKD are at higher risk of progression to ESRD than IA. Similarly, it is possible that CKD may be associated with a higher risk of incident CHD and CHD mortality in IA compared to NE. Validation of the modified MDRD formula for GFR in this population, and longitudinal study will be required to confirm these hypotheses.
Indian Asian; chronic kidney disease; coronary heart disease
020 METABOLIC SYNDROME IS INDEPENDENTLY ASSOCIATED WITH SUBCLINICAL LEFT VENTRICULAR DYSFUNCTION IN ASYMPTOMATIC NORTHERN EUROPEANS AND INDIAN ASIANS AGED 35 TO 75: A GENERAL POPULATION STUDY
T. Lim1, E. Lim2, J. Kooner2, R. Senior1.1Northwick Park Hospital, Harrow, UK; 2Ealing Hospital, London, UK
Background: Metabolic syndrome (MS) identifies individuals with elevated risk for development of atherosclerotic cardiovascular disease. Tissue Doppler imaging (TD) during echocardiography allows improved assessment of global left ventricular (LV) systolic and diastolic function compared to conventional echocardiography. As Indian Asians are at high risk of MS, the aim of this study was to evaluate the relationship between MS and parameters of LV function in asymptomatic Northern Europeans and Indian Asians.
Methods: Asymptomatic Northern Europeans and Indian Asians aged 35–75 from West London were randomly invited to participate. Each underwent 2D and TD echocardiography (Sonos 7500, Phillips). The AHA 2005 definition of MS was used. Systolic parameters assessed were left ventricular ejection fraction (LVEF) and longitudinal function (average of peak medial, lateral, inferior and anterior mitral annular S’ waves). Diastolic parameters assessed were Doppler mitral E/A, TD mitral annular e’, ratio of E/e’ and left atrial volume index (LAVI).
Results: Accordingly, 453 subjects (137 Northern European and 316 Indian Asian) participated (80% male, mean age 51±10 years) of which 101 (22%) had MS. Of the 101 subjects with MS, 84 (83%) were Indian Asian and 17 (17%) were Northern European (p = 0.001). MS correlated with ethnicity (r = 0.14; p = 0.003), diastolic parameters (E/e’: r = 0.23; p<0.001, LAVI: r = 0.13; p = 0.004, e’: r = −0.25; p<0.001 and E/A: r = −0.24; p<0.001), longitudnal LV function (S’: r = −0.11; p = 0.02), LV mass index (r = 0.17; p<0.001) and LV wall thickness (r = 0.23; p<0.001). In regression analyses, MS was found to be an independent predictor of the parameters of diastolic and longitudinal systolic dysfunction, even after adjusting for the effect of blood pressure and hypertension.
Conclusion: Prevalence of MS was found to be significantly higher in Indian Asians compared to Northern Europeans and is independently associated with asymptomatic LV dysfunction.
metabolic syndrome; subclinical left ventricular dysfunction; asymptomatic
021 COMMON CAROTID INTIMA-MEDIA THICKNESS CORRELATES WITH FRAMINGHAM RISK SCORE EQUALLY IN ASYMPTOMATIC NORTHERN EUROPEANS AND INDIAN ASIANS
T. Lim1, E. Lim2, J. Kooner2, R. Senior1.1Northwick Park Hospital, Harrow, UK; 2Ealing Hospital, London, UK
Background: Indian Asians are at high risk of coronary artery disease (CAD) compared to Northern Europeans, but the underlying reasons are not clear. Carotid intima-media thickness (CIMT) is a measure of atherosclerosis that has been used to assess CAD risk. Framingham risk scores (FRS) are also widely used to determine CAD risk. The aim of this study was to evaluate the relationship between FRS and CIMT in Indian Asians compared to Northern Europeans.
Methods: Randomly selected asymptomatic individuals aged 35–75 years from the community with no prior history of CAD were invited to participate. Standard cardiovascular risk factors were determined and the FRS derived. All subjects then underwent B mode carotid duplex ultrasound (Sonos 7500, Phillips). Mean CIMT at the far wall of both left and right common carotid arteries was determined off-line during diastole using an automated edge detection algorithm (Q-lab 3, Phillips).
Results: 453 individuals (137 Northern Europeans and 316 Indian Asians) were studied. Prevalence of males (82%/71%; p = 0.02) and diabetes (17%/4%; p = 0.0002) were higher in Indian Asians compared to Northern Europeans, however the latter showed a higher prevalence of smokers (54%/20%; p = 0.0001) and higher total cholesterol levels (5.6/5.3 mmol/l; p = 0.01). No significant differences were observed in age (50.1/50.8 yrs) and systolic blood pressure (127/128 mmHg). Predicted 10-year cardiovascular risk using Framingham estimates was similar in both groups: 8.8%/8.6% (p = NS). Mean CIMT was identical in Northern Europeans and Indian Asians: 0.58±0.11 mm for both groups. The correlation coefficient between FRS and CIMT was not significantly different between Northern Euopeans and Indian Asians (r = 0.55 (p<0.0001) v 0.44 (p<0.0001) respectively).
Conclusion: In this UK population of asymptomatic Northern Europeans and Indian Asians, CIMT was similar in both ethnic groups. Also, CIMT correlates equally well with FRS in both ethnic groups. Whether CIMT predicts CAD mortality equally in the two ethnic groups remains to be determined.
Carotid intima-media thickness; framingham risk score; coronary artery disease
022 COUNCIL TAX BAND IS MORE SENSITIVE THAN INDEX OF MULTIPLE DEPRIVATION IN PREDICTING INCIDENCE OF CORONARY HEART DISEASE IN A DEPRIVED COMMUNITY
I. Findlay1, A. Cunningham2, C. Krawczyk2, E. Garman3, P. Dochery2, M. Flood2, C. Napier2.1Royal Alexandra Hospital, Paisley, UK; 2Have a Heart Paisley, Paisley, UK; 3Argyll+Clyde Health Board, Paisley, UK
Recent publications from the Renfrew-Paisley Midspan Study, and a specially commissioned research for SIGN using data from SHHEC (Scottish heart health extended cohort) confirm that deprivation is significantly related to mortality from coronary heart disease (CHD).
The Scottish Index of Multiple Deprivation (SIMD) 2004 identifies the most deprived areas across Scotland. It is based on 31 indicators (in the six domains of Current Income, Employment, Housing, Health, Education, Skills and Training, and Geographic Access to Services and Telecommunications). SIMD 2004 is presented at data zone level (average 500 people), enabling small pockets of deprivation to be identified, but crucially does not identify the more affluent individual living in that deprived area. We postulated that using the council tax band (A to H) of an individual’s residence might provide a more sensitive indicator of deprivation and thereby lead to a more targeted delivery of therapy.
To test this theory we used data from a central disease register for patients with CHD developed as part of a Scottish Executive health demonstrator project (Have a Heart Paisley). This is a live data repository with feeds from all GP practices, local hospital and regular statistical updates from the Information Services Division of the Scottish Executive. We noted important differences at patient level, where SIMD could rationalise a relatively more affluent patient (based on Council Tax) into “compulsory” treatment should this be determined by this measure of deprivation, and vice versa. For example 19% (14 598) of HaHP residents are in Council Tax A-rated accommodation. Of these, 10 199 (70%) are rated within the most deprived 20% according to SIMD 2004—so 30% fall outwith the “worst areas” classification using SIMD. Similarly over 2000 people living in Council Tax Band D-H accommodation fell within the worst 20% by SIMD classification and would receive “compulsory” treatment despite living in relatively affluent houses.
The relationship between CHD incidence and SIMD/council tax band is shown below. The correlation coefficient between SIMD score and CHD incidence for all ages was SIMD 2004 = 0.71 and Council Tax = 0.89. The correlation coefficient for those aged 45–60 was 0.90 and 0.98 respectively. There was a significant relationship between council tax band and CHD incidence across the quintiles of age between 35 and 75 with the strongest relationship seen in those aged 55–59.
Use of council tax should be explored as simple measure to individualise the correction that needs to be applied to standard risk calculators to account for the influence of deprivation on CHD risk.
deprivation; heart disease; scottish index of multiple deprivation
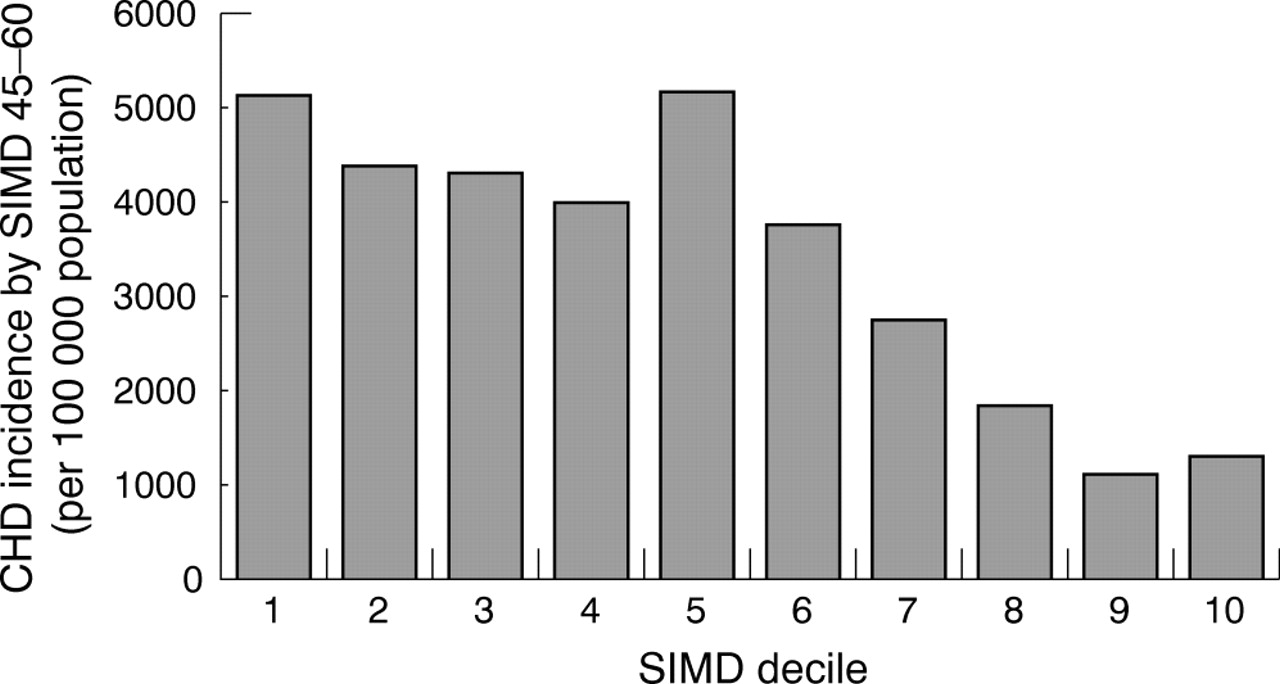
Abstract 22 figure 1.
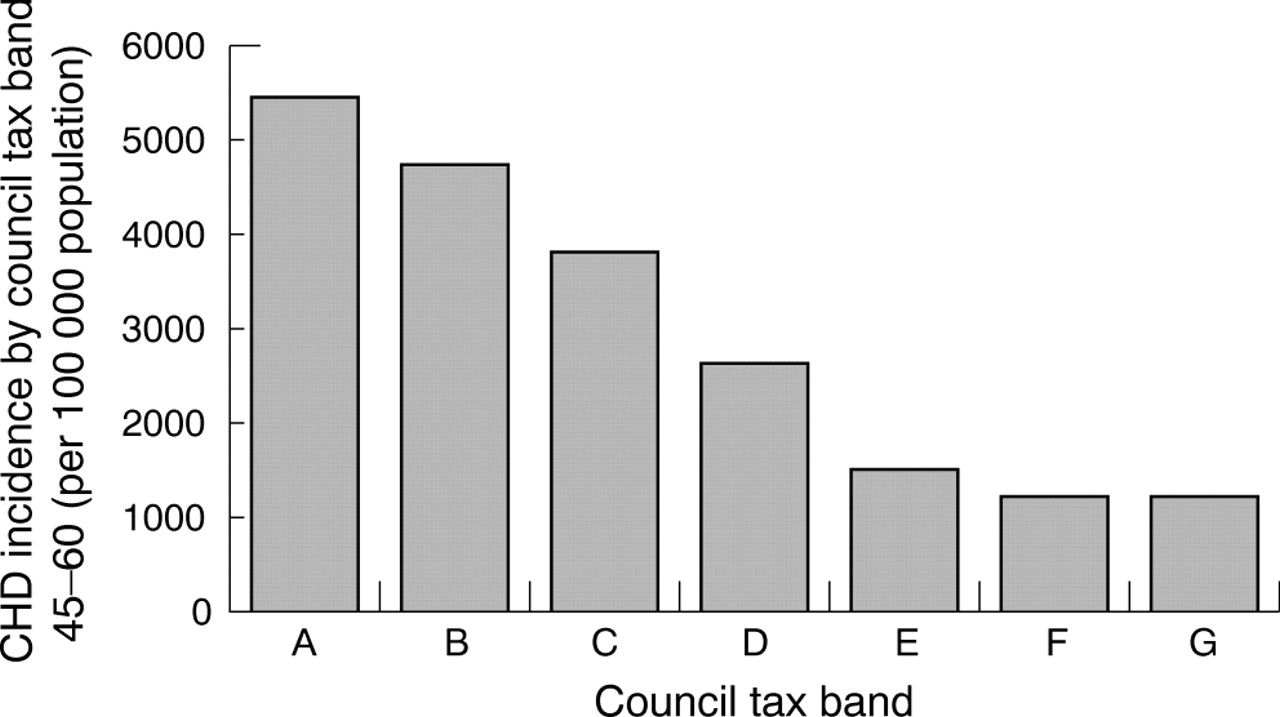
Abstract 022 figure 2.
023 DO HOSPITAL ADMISSIONS FOR HEART DISEASE REFLECT PREVALENCE OF DISEASE OR QUALITY OF CARE IN GENERAL PRACTICE?
R. Ryan, R. McManus.Department of Primary Care and General Practice, University of Birmingham, Birmingham, UK
Introduction: National data on the prevalence and management of coronary heart disease (CHD) and left ventricular dysfunction (LVD) in individual general practices has recently been released as part of the Quality and Outcomes Framework for the new GMS contract in general practice (QOF) and provides an opportunity for comparison with data on hospital activity from the Hospital Episode Statistics (HES). This study aimed to compare variations in prevalence and quality score for CHD and LVD in primary care with hospital inpatient activity, and to evaluate variations in practice data in terms of age and deprivation.
Methods: Primary care QOF data for the West Midlands (population 5.6 million) concerning practice disease registers and quality scores was aggregated by PCT and compared to Hospital Episodes (HES) data for admissions using the Spearman Rank Correlation Coefficient. A descriptive analysis of disease prevalence in general practices was performed with adjustment of crude prevalence to take account of the age distribution of the practice populations, and the relative deprivation of the wards in which they are located.
Results: There was a strong linear relationship between the prevalence of CHD and LVD in primary care at the beginning of 2005 and the number of admissions for CHD and heart failure in the previous year (r = 0.9 and 0.8 respectively, p<0.001). There was approximately one hospital admission for CHD for every six cases of CHD in primary care (33 627/203 781) and one admission for heart failure for every three cases of LVD in practice (8618/26 450). There was no linear relationship between quality scores for CHD or LVD and hospital admissions. The crude prevalence of CHD and LVD in general practices ranged from 0.1% to 10.2% and from 0.0% to 2.0%, respectively. Part of this variation could be reduced by adjustment for the age distribution of each practice but not for deprivation.
Conclusions: Hospital workload in terms of CHD and heart failure admissions appears to reflect underlying disease prevalence in primary care but in contrast there is no such relationship between achieved general practice quality points and hospital admissions for CHD or LVD. This may reflect a poor ability to discriminate by the QOF (many practices achieved close to maximum points) or may reflect historical practice behaviour with changes taking time to impact in secondary care. Variation between practices in disease prevalence other than by age, may be due to factors such as disease diagnosis rates, practice computerisation, and individual rather than ward deprivation. The annual release of QOF and HES data with linkage at individual practice level will offer further opportunities to explain and perhaps predict the relationship between the prevalence of disease in the community, the care provided in general practice, and hospital activity.
heart disease; general practice
024 SURVIVAL AND QUALITY OF LIFE IN CHILDREN WITH SEVERE PULMONARY HYPERTENSION
S. Haworth1, Y. Flynn2, A. Hislop3.1Great Ormond Street Hospital for Children/Institute of Child Health, UCL, London, UK; 2Great Ormond Street Hospital for Children, London, UK; 3Institute of Child Health, UCL, London, UK
We report the four year experience of the UK Pulmonary Hypertensive Service for Children. In children with Idiopathic Pulmonary Arterial Hypertension (IPAH) the median survival without treatment is 10 months (Barst, Circulation 1999;99:1197). Using new, specific therapies survival can be greatly improved. Between April 2001 and June 2005 we treated 49 patients with IPAH, mean age at presentation 7.99 years (range 0.1–19.7). 18 were male and 31 female, the female predominance being less than in adults. All were in WHO Functional Class III or IV with a pulmonary arterial pressure equal or greater than systemic arterial pressure. Mean pulmonary vascular resistance (PVR) was 21.65 units.m2 (range 2.5–49). 46 children were treated with specific therapies; epoprostenol, bosentan and/or sildenafil in the presence of a fixed PVR (unresponsive to NO at cardiac catheterisation) and 4 positive responders were given nifedipine. The Kaplan-Meier survival estimates for our population were 84% at 1 year and 76% at 3 years. Five children received a bilateral lung or heart/lung transplantation and are alive and well. 10 children died (2 untreated). The mean survival was 3.41 of our 4.17 year study period. Treatment with epoprostenol alone gave a mean survival of 2.73 years while epoprostenol plus bosentan gave a better survival of 4.11 years. Children returned to school. The results of a quality of life (QOL) survey for children (SF10) showed a median score of 27.15 (range 0–48.5) for physical ability and a median psychosocial score of 45.3 (range 19.6–60.7). A score >50 is considered normal, <47 shows substantial adverse impact. The psychosocial score was almost always greater than the physical score. Over the same time period we treated 124 patients with pulmonary arterial hypertension associated with a variety of disorders. Survival was 89% at 1 year and 79% at 3 years. Specific therapies were given to 72%. The two largest subgroups were those with congenital heart disease and sustained postoperative PAH (38) and those with Eisenmenger Syndrome (29). 76% of these two groups of children were on specific therapy. None died in the Eisenmenger group but nine died in the postoperative group. For the entire postoperative group the mean survival was 3.14 years. For those on therapy, mean survival on epoprostenol (4) was 2.47 years and on bosentan (23) 2.14 years from initiation of treatment. The median QOL for the postoperative group was 33.8 (range 4.5–53.2) for physical ability and 43.6 (range 19.6–57.3) for psychosocial assessment. Eisenmenger patients received bosentan (15) or sildenafil (6). Median QOL scores were 20 (range 0–45) physical and 34.5 (range 16.1–57.3) psychosocial. For both IPAH and associated pulmonary hypertension, QOL scores did not relate to PVR, age at presentation or length of time treated. In conclusion, treatment improved survival in children with IPAH and in all cases of pulmonary hypertension psychosocial well-being improved in the face of physical restriction.
paediatric pulmonary hypertension; survival; quality of life
025 IMPROVING SURVIVAL IN THE POPULATION WITH SCLERODERMA ASSOCIATED PULMONARY HYPERTENSION
D. Bloore1, C. Handler1, C. Das1, J. Smee1, C. Denton2, C. Black2, J. Coghlan1.1National Pulmonary Hypertension Service, Royal Free Hospital, London, UK; 2Academic and Clinical Department of Rheumatology, Royal Free Hospital, London, UK
Scleroderma associated pulmonary arterial hypertension (SSc-PAH) is associated with severe functional disability and a poor prognosis due to progressive cardiac failure. Advanced therapies, including endothelin antagonists, prostanoids and phosphodiesterase-5 inhibitors, added to basic treatments, have improved functional class and time to clinical worsening in multicentre trials, but their effects on long term survival are unclear. We have shown that patients who meet the BREATHE-1 criteria for oral therapy show improved survival with modern therapies. However, to date, there are no reports of a general improvement in survival for all patients with this condition.
Survival in patients with SSc-PAH treated before the widespread availability of disease modifying therapies, was compared to survival using current management strategies. Survival in the whole population of patients with SSc-PAH, improved significantly (p = 0.031) from 74%, 56%, and 43% at 1, 2, and 3 years respectively between 1996–2001 (n = 127), to 80%, 69%, and 63%, between 2002–05 (n = 145). The greatest benefit was seen in patients who fulfilled criteria for disease-modifying therapies, in whom survival improved from 69%, 48%, and 37% between 1996–2001 (n = 67), to 81%, 68%, and 64%, between 2002–05 (n = 93) (p = 0.016). Prognosis was also dramatically influenced by WHO class at diagnosis with a one year mortality of 0% in class I, 4% in class II, 25% in class III, and 42% in class IV. Mortality in groups III and IV was significantly greater (p<0.01) than in groups I and II.
The introduction of multiple advanced therapies has improved the outcome for the population with SSc-PAH.
systemic sclerosis; pulmonary hypertension; survival
026 STATINS MODULATE THE GROWTH OF HUMAN PULMONARY SMOOTH MUSCLE CELLS THROUGH THE MEVALONATE PATHWAY
O. Ali, E. Growcott, J. Wharton, M. Wilkins.1Imperial College London, London, UK
Introduction: Pulmonary arterial hypertension (PAH) is a progressive disease that is characterised by the aberrant regulation of distal pulmonary artery smooth muscle cell (PASMC) proliferation and apoptosis. Statins, such as simvastatin are powerful inhibitors of cholesterol synthesis with wide ranging pleiotropic effects including; anti-inflammatory, anti-oxidant, anti-proliferative, and immunomodulatory properties. Simvastatin has been shown to attenuate experiemntal pulmonary hypertension in rats. Importantly, simvastatin reversed vascular remodelling by reducing proliferation and increasing apoptosis of vascular smooth muscle cells in the pulmonary arteries of treated rats. We therefore sought to establish whether simvastatin and other lypophilic and lypophobic statins modulate proliferation and apoptosis in isolated human distal PASMCs.
Methods: Isolates of PASMCs were derived from distal human pulmonary arteries (n = 11). Anti-proliferative effects of lypophilic (simvastatin, atorvastatin, and mevastatin) and lypophobic (pravastatin) statins were determined by measuring [3H-methyl]-thymidine uptake, cell proliferation and matrix metalloproteinase-9 (MMP-9) production. Effects of statins on apoptosis and endothelin-1 (ET-1) release were also assessed be measuring cytoplasmic histone associated DNA fragments and transforming growth factor-β1 (TGF-β1) stimulated ET-1 in conditioned culture medium respectively. Intracellular signalling was explored using mevalonate (MVA), geranylgeranylpyrophosphate (GGPP), and farnesylpyrophosphate (FPP) and inhibitors of geranylgeranyl transferase (GGTI-2133) and farnesyl transferase (FTI-277).
Results: Treatment of PASMCs with lypophilic statins attenuated DNA synthesis and cell prloiferation in a concentration-dependent manner (10−8 to 10−5 M), but differences were observed. Thus, pravastatin had no apparent effect whereas simvastatin (10−6 M) for example induced gretaer reduction in DNA synthesis (43.0 (5.9)% inhibition, mean (SEM), n = 5 isolates, p<0.001) comapred to atorvastatin (8.8 (2.2)% inhibition, n = 5). Simvastatin and atorvastatin increased DNA fragmentation over 48 hours. Both statins also displayed a concentration dependent inhibitory effect on endogenous ET-1 and MMP-9 production. The inhibitory effects of simvastatin and atorvastatin were reversed by addition of either MVA (10−4 M) or GGPP (10−5 M), but not FPP, and were mimicked by GGTI-2133 (10−5 M, p<0.05) rather than FTI-277, consistent with the involvement of mevalonate pathway and signalling via geranyl-geranylated proteins.
Conclusion: Lypophilic statins including simvastatin have direct anti-proliferative and pro-apoptotic effects in human distal PASMCs. These pleiotropic effects may be relevant to the future management of patients with PAH.
statins; pulmonary arterial hypertension; pulmonary artery smooth muscle cells
027 NON-INVASIVE ASSESSMENT OF PULMONARY ARTERY PULSATILITY IN IDIOPATHIC PULMONARY HYPERTENSION WITH CARDIAC MAGNETIC RESONANCE
J. Strange1, M. Westwood2, R. Mohiaddin3, J. Gibbs4.1The London Chest, London, UK; 2The Heart Hospital, London, UK; 3The Royal Brompton, London, UK; 4Hammersmith Hospital, London, UK
Introduction: The assessment of pulmonary artery morphology in pulmonary arterial hypertension (PAH) has been limited in the past to analysis of CT still images or invasive methods including pulmonary angiography, intravascular ultrasound (IVUS) and histology of biopsies. Advances in CMR allow non-invasive detailed imaging of the pulmonary tree and the use of cardiac gating may allow analysis of response to haemodynamic change. Pulsatility is a functional measure of vessel compliance. It has been shown before in patients with idiopathic as well as associated causes of PAH to be reduced compared to normal populations using intravascular ultrasound (IVUS). It has also been previously shown to have prognostic value, with patients with a lower pulsatility having a higher morbidity and mortality.1 A previous report has demonstrated in idiopathic PAH that pulsatility increases in response to prostacyclin infusion when measured by IVUS.
Methods: Patients with NYHA class III idiopathic PAH had CMR imaging at baseline and 3 months. 13 patients were treated with sildenafil 50 mg tds (a selective PDE5 inhibitor) for this period. Both pulmonary trunk and aortic root pulsatility were calculated at baseline and 3 months by tracing around the blood-vessel interface in both systole and diastole (the largest and smallest diameter respectively). Pulsatility was then calculated from the formula:
Pulsatility = (Areasystole−Areadiastole)/Areadiastole×100, being expressed as a percentage.
Results: Pulmonary trunk pulsatility increased by 50% compared with baseline (from 7.6% to 11.4%, p = 0.04) (fig).
Discussion: All patients in this group had baseline pulsatility of less than 13% (μ = 7.6%). This is lower than in previously reported series. Whether this is due to our population having more advanced disease or the difference in values obtain from the different imaging modalities it is impossible to say. It is, however, encouraging to see that pulsatility improved with the same magnitude as the previously published data where epoprostenol was the therapeutic agent. No correlation existed between change in pulsatility and cardiac index in this population, although there was a significant improvement in both indices. Aortic pulsatility demonstrated no significant change from baseline. This therefore suggests that the change is due not just to the improvement in haemodynamics, but possibly due to a direct positive effect on the vasomotor properties of the wall of the pulmonary trunk. This is an exciting finding, previously only demonstrated with invasive IVUS techniques and epoprostenol therapy. Not only has it highlighted the value of CMR in haemodynamic monitoring but also possibly revealed evidence of positive remodeling by the therapeutic agent sildenafil.
pulmonary; magnetic resonance; pulsatility

Abstract 027.
028 CHARACTERISATION OF THE VASODILATORY ACTION OF TESTOSTERONE IN THE HUMAN PULMONARY CIRCULATION
A. Smith1, R. Bennett2, T. Jones3, M. Cowen2, K. Channer1, R. Jones4.1Royal Hallamshire Hospital, Sheffield, UK; 2Castle Hill Hospital, Hull, UK; 3Barnsley District General Hospital, Barnsley, UK; 4University of Sheffield, Sheffield, UK
Aim: This study was carried out to assess for the first time, the vasodilatory effect of testosterone in the human pulmonary circulation. The influence of gender upon the response to testosterone was studied in isolated human pulmonary arteries and veins and in isolated perfused whole lungs.
Methods: Isolated human pulmonary arteries and veins were studied by wire myography. Vessels were obtained from male (n = 7, age 65±3 years) and female (n = 6, age 56±7 years) patients. Vessels were preconstricted with U46619 (1 μM) and endothelial integrity was tested with acetylcholine (1 μM). Vessels were then washed before the addition of U46619 (1 μM) prior to exposing them to either testosterone or ethanol vehicle. Isolated lungs were studied in a ventilated and perfused model (methodology described in (Bennett et al, 2004)). Lung samples (n = 12) were obtained from male (n = 6, age 62±7 years) and female (n = 6, age 66±4 years) patients. They were exposed to potassium chloride (KCl) (100 mM), prior to the addition of either testosterone (1 nM–100 μM) or ethanol vehicle.
Results: In the isolated human pulmonary arteries, testosterone caused significant vasodilatation (table). Results from the isolated perfused human lung model showed greater responses to testosterone than the pulmonary arteries (table). There was however no significant difference in the magnitude of the response to testosterone between the sexes.
Abstract 028
Conclusion: Testosterone acts as an efficacious vasodilator in the human pulmonary circulation, with no marked differences observed in the response dependant on sex. Testosterone may therefore be a potential novel agent in the treatment of pulmonary vascular disease, namely pulmonary hypertension.
testosterone; pulmonary circulation; human
029 REDUCTION IN CARDIOVASCULAR RISK FACTORS CAN BE ACHIEVED WITH A STRUCTURED, MULTIDISCIPLINARY WEIGHT LOSS PROGRAMME COMBINING DIET, EXERCISE, AND ORLISTAT (XENICAL) IN PATIENTS WITH CHRONIC KIDNEY DISEASE
H. MacLaughlin1, S. Cook2, D. Kariyawasam1, M. Holesgrove1, G. Newell2, I. Macdougall3.1Department of Nutrition and Dietetics King’s College Hospital, London, UK; 2Department of Physiotherapy King’s College Hospital, London, UK; 3Department of Renal Medicine King’s College Hospital, London, UK
Cardiovascular disease (CVD) is the leading cause of death in patients with chronic kidney disease (CKD). Obesity is well recognised as a risk factor for CVD, but appears to have a protective effect against mortality in haemodialysis patients. Conversely, obese patients (body mass index (BMI)>30 kg/m2) with CKD are often excluded from kidney transplantation waiting lists. To determine whether obese patients with CKD could succeed in reaching an acceptable weight for transplantation, a multidisciplinary weight management clinic (WMC) was established. 27 (18M; 9F) patients with CKD (8 non-dialysis; 19 dialysis) of stable or increasing weight (BMI range 31.3–47.3 kg/m2) commenced the programme of individualised diet and exercise regimens plus Orlistat (Xenical) therapy for 6 months. All patients attended at least 3 individual appointments with the Dietitian and Physiotherapist in the 6 month period. Body weight (BW) and a range of CVD risk factors were measured.
Mean BW reduced from 106.0 kg to 101.2 kg at 3 months (p<0.05), and to 99.5 kg (−6.2%), at 6 months (p<0.05 from 3 months). At 6 months, waist circumference decreased by 13.6 cm from 115.8 cm to 102.2 cm and systolic blood pressure decreased from 155 mmHg to 141 mmHg (p<0.05). Diastolic blood pressure and cholesterol were unchanged. To date, six patients have been listed for kidney transplantation since reaching predetermined weight loss goals set by the transplant surgeon.
Significant reduction in body weight, waist circumference and systolic blood pressure may equate to reduction in CVD risk, including risk of myocardial infarction (MI). Based on epidemiological research, a reduction in waist circumference of 12 cm reduces the risk of MI (odds ratio 0.84)1 and decreasing systolic blood pressure by 10 mm Hg is associated with an 11% reduction in risk of MI.2 Thus, successful intentional weight loss of 6% in CKD patients may contribute to a reduction in CVD related morbidity through associated changes in parameters related to CVD risk, and possibly allow them the opportunity of, and the potential benefits associated with, kidney transplantation.
1
2
weight reduction; exercise; diet
030 SELECTIVE IF INHIBITION WITH IVABRADINE IS A NOVEL AND EFFECTIVE APPROACH TO REDUCE HEART RATE IN DIABETIC PATIENTS WITH STABLE ANGINA
J. Doig1, K. Fox2, J. Borer3, W. Ruzyllo4, J. Barton5.1North Tyneside General Hospital, North Shields, UK; 2Royal Brompton National Heart and Lung Hospital, London, UK; 3New York Presbyterian Hospital, New York, USA; 4National Institute of Cardiology, Warsaw, Poland; 5Portiuncula Hospital, Ballinasloe, UK
Background: Diabetes is common in patients with angina, often affecting the autonomic nervous activity and potentially compromising the anti-anginal and anti-ischaemic effectiveness of heart rate reducing agents. Ivabradine is the first selective If inhibitor that reduces heart rate without negative inotropic effects. We aimed to compare the efficacy and tolerability of ivabradine among diabetic and non-diabetic patients with angina.
Methods: Data were pooled from five studies performed in patients with stable angina and documented coronary artery disease who received ivabradine (5, 7.5, and 10 mg bid) for 3 to 4 months. Heart rate reduction, anti-anginal efficacy and overall tolerability were compared between the overall poulation (n = 2340) and the diabetic population (n = 441).
Results: At baseline, heart rate tended to be higher in diabetic patients. Ivabradine reduced heart rate identically in the two populations (table) and produced a significant anti-anginal efficacy in diabetic and non-diabetic patients as well as in the overall population. Angina attacks per week were reduced by 60.6% compared to 61.1%; NS. Compared to baseline, ivabradine 7.5 mg bid increased total exercise duration at trough of drug activity by 87±129 seconds in the overall population (n = 300), and by 96±134 seconds in the diabetic patients (n = 62). Overall, ivabradine was well tolerated in both groups and the presence of diabetes did not affect its tolerability or side effect profile. In 266 diabetic patients who were followed for one year, ivabradine did not modify fasting glucose levels.
Abstract 030
Conclusion: In patients with stable angina, selective If inhibition with ivabradine is a valuable and well tolerated novel medical treatment slowing heart rate and controlling angina in diabetic and non-diabetic patients.
ivabradine; sinus node inhibition; angina
031 SPECTRAL ANALYSIS OF ATRIAL FIBRILLATION USING NON-CONTACT MAPPING TO STUDY THE IMPACT OF CIRCUMFERENTIAL ABLATION
J. Jarman, T. Wong, H. Spohr, P. Kojodjojo, J. Davies, D. Francis, D. Davies, V. Markides, N. Peters.St Mary’s Hospital & Imperial College, London, UK
Introduction: Although wide area circumferential ablation (WACA) is extensively used to treat persistent atrial fibrillation (AF), it is unclear by which mechanisms it affects the AF, which often persists immediately after ablation. We studied the impact of WACA on left atrial (LA) activation during AF by performing spectral analysis of simultaneous global LA signals.
Methods: Patients with persistent AF underwent WACA whereby pairs of unilateral pulmonary veins were encircled and mitral valve isthmus and roof lines added. A noncontact multielectrode array was deployed in the LA and used to guide ablation and record persistent AF before and after WACA. Signals were filtered at 1 to 150 Hz. Virtual unipolar electrograms from 256 evenly distributed LA sites were sampled at 1200 Hz and exported for analysis. The far field ventricular component was subtracted from the raw signals and the output subjected to Hanning windowing and fast Fourier transformation. The highest power frequency in the 3 to 15 Hz range was selected as the dominant frequency (DF) and plotted on a 3-dimensional map of the LA. Three consecutive 7 second segments of AF were analysed before and after WACA in each patient.
Results: Six patients were completed the protocol and AF persisted in all patients immediately after WACA. Mean DF of all 256 sites was reduced by WACA (5.5 (0.2) to 4.8 (0.2) Hz (mean (SE)); p = 0.03). LA surface area supporting the highest frequency activation, defined as 90% or more of the maximal DF seen before ablation, was also reduced (34.3 (9.4) to 12.1 (3.4) cm2, p = 0.03). In contrast, the maximal DF did not change significantly following ablation (7.3 (0.1) to 7.6 (0.5) Hz, p = 0.75). Before WACA high DF areas were usually located near the pulmonary veins and base of the left atrial appendage. Following WACA the septum and base of the left atrial appendage (areas not encircled) were the most common site of high DFs.
Conclusions: These findings provide important new insights into the impact of WACA on AF. Although the area of left atrial substrate sustaining high frequency activation is reduced, the highest frequencies persist at alternative locations, usually in areas which are not encircled. Targeting these remaining high DF areas may improve clinical success rates in treating persistent AF.
atrial fibrillation; spectral analysis; noncontact mapping

Abstract 031.
032 THE FIRST UK DISTRICT GENERAL HOSPITAL EXPERIENCE OF A “ONE STOP” RAPID ACCESS ATRIAL FIBRILLATION SERVICE
T. Keeble, D. Sevant, D. Marshall, S. Mazhar, T. Nageh, P. Kelly, A. Khokar.Southend General Hospital, Southend, UK
Introduction: Atrial fibrillation (AF) is the commonest chronic arrhythmia, and is associated with increased risk of thrombo-embolic disease. Important considerations include prompt diagnosis, risk stratification, anti-coagulation, and DC cardioversion (DCC). In 2003 the mean wait from outpatient clinic review to DCC at Southend General Hospital was 44 weeks. In January 2004 we established a nurse-led rapid access AF (RAAF) clinic in an attempt to improve management of patients with AF.
Methods: This is a prospective study to assess the service improvement and clinical outcomes of the new multidisciplinary RAAF service designed to assess, risk stratify, manage, and follow up patients with AF. We included all patients referred by their general practitioner or secondary care provider with AF confirmed on a 12 lead ECG over a period of one year. All patients underwent a one stop nurse-led assessment and individual risk stratification, in addition to transthoracic echocardiography prior to a decision regarding anti-arrhythmics, anticoagulation, and consideration of DCC.
Outcome measures included time from referral to assessment, number of patients pharmacologically cardioverted, number of patients successfully DC cardioverted, time to DCC, maintainance of sinus rhythm at six weeks, and the rate of thrombo-embolic events.
Results: A total of 323 patients were referred to the RAAF service from January 2004 to December 2004, 182 of whom were assessed during this time. The mean age was 71 years and 37% of patients were female. The mean time between referral and DCC was 22 weeks, and by 2005 it was 12 weeks. Of the 182 patients assessed, thirty (21%) cardioverted pharmacologically with amiodarone and at 6 weeks follow up, 89% of these remained in sinus rhythm (SR). A total of 114 patients were DC cardioverted with a 90% procedural success rate. During 2004 we changed from an external monophasic defibrillator to a biphasic machine. All 35 (100%) patients were successfully cardioverted to SR. Table 1 below shows the the DC cardioversion rates.
Abstract 032
Sinus rhythm was maintained in 65% of DC cardioverted patients at six weeks follow up. Two (1.4%) patients suffered thrombo-embolic events during follow up.
Conclusions: A nurse-led, multidisciplinary RAAF clinic is an innovative, safe, and practical approach to efficiently managing patients with a new diagnosis of AF. We have shown that patients can be fully evaluated in one consultation including echocardiography resulting in early risk stratification, appropriate initiation of warfarin, anti-arrhythmics, and DC cardioversion if appropriate. The time from clinic assessment to cardioversion has been cut from 44 weeks to 12 weeks, and our rates of DCC procedural success are comparable with larger studies. Our patients also have robust follow up at six weeks and one year, where anti-arrhythmics and anti-coagulation can be reviewed.
atrial fibrillation; rapid access clinic; DC cardioversion
033 DO REPEAT CARDIOVERSIONS INCREASE LONG TERM MAINTENANCE OF SINUS RHYTHM IN PATIENTS WITH ATRIAL TACHYARRHYMIAS?
A. Arya, J. Silberbauer, F. Arif, N. Sulke.Eastbourne General Hospital, Eastbourne, UK
Background: The role of recurrent cardioversion for atrial fibrillation (AF) and atrial tachyarrhythmias (AT) is unclear. A retrospective case notes analysis of patients undergoing direct current cardioversion under sedation (DCCV) for atrial tachyarrhythmias between 1997–2005 at Eastbourne DGH was undertaken.
Methods: 916 patients were analysed for immediate, six week, and long term sinus rhythm following DCCV. The AHA classification of AF was used along with an additional category, mixed AF, for patients that had both PAF progressing to persistent AF at long term follow up. The outcomes of immediate (SR at discharge), medium term at six weeks and long term success, defined as sinus rhythm at greater than one year, were analysed in patients that had had one, two, or multiple cardioversions.
Results: In this cohort, 63.8% were male, mean age (SD) 70.9 (10.0). 96.1% of patients had DCCV for AF, 3.9% for atrial flutter. 177 patients with one, 59 with two, and 41 with multiple DCCV were followed up long term. 84.6% of patients were in SR at discharge, 41.1% at six weeks, and 19.9% at one year. Long term SR was achieved in 16%, 20%, and 13% of pts after their first, second and multiple DCCVs. 77%, 68%, and 81% patients respectively remained in persistent or permanent AF. PAF regressing to persistent AF was detected in 1% of patients at one, 6% at two, and 3% at multiple DCCVs (fig). There were no differences in age, gender, or left atrial diameter between the groups. The use of anti-arrhythmic drugs was significantly greater at second and third DCCV than other groups, p = 0.005. There was no significant difference in the likelihood of maintaining longterm SR with repeated DCCVs. The use of amiodarone rather than betablockers was associated with higher rates of sinus rhythm, p = 0.004, at second DCCV but not at first or multiple DCCV.
Conclusion: Repeat DCCV does not improve the longterm maintenance of SR. Sustained SR was greatest after 2nd DCCV associated with use of amiodarone.
atrial fibrillation; direct current cardioversion; sinus rhythm
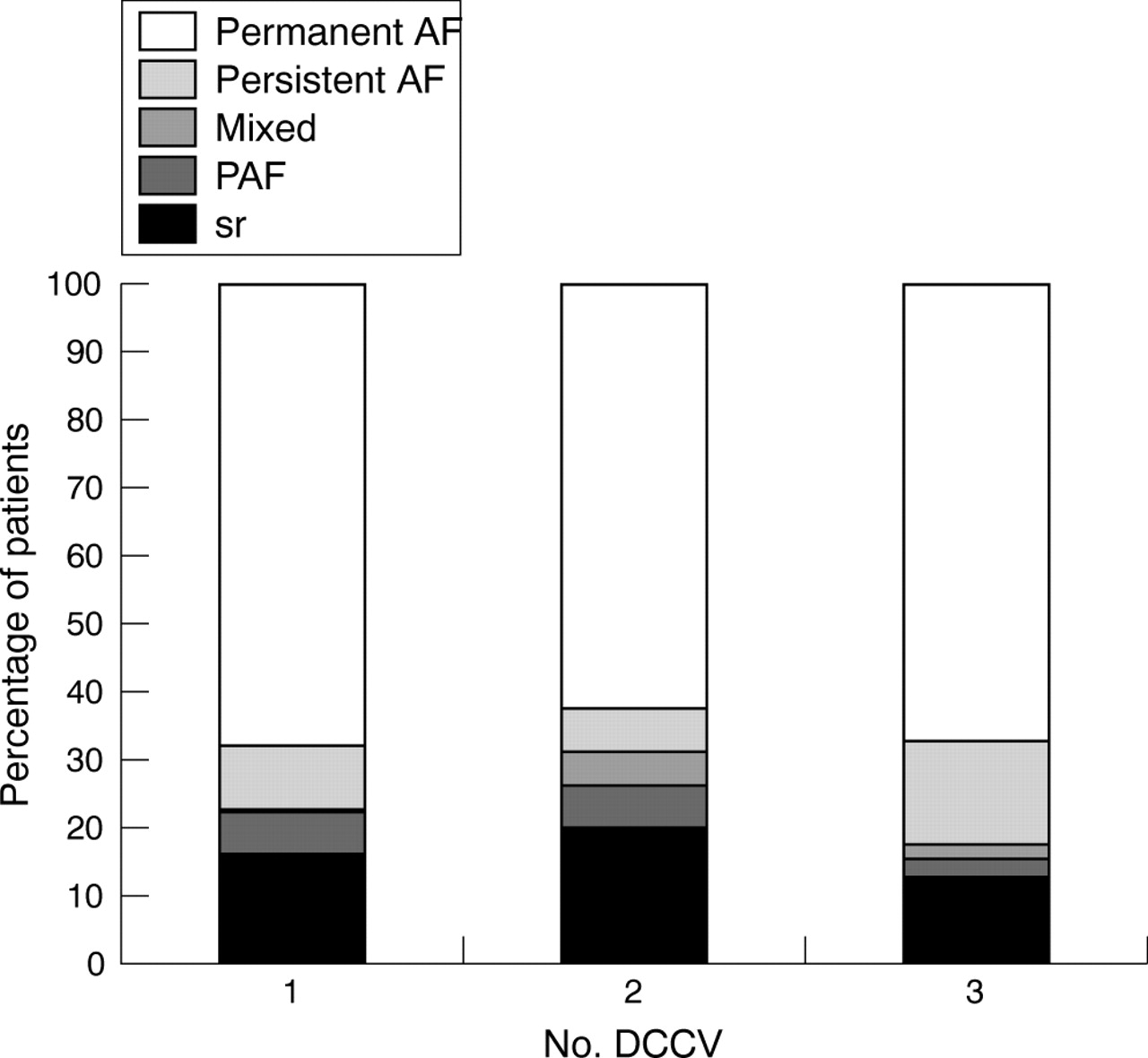
Abstract 033.
034 THE IMPACT OF CT IMAGE INTEGRATION INTO AN ELECTROANATOMIC MAPPING SYSTEM ON CLINICAL OUTCOMES OF CATHETER ABLATION OF ATRIAL FIBRILLATION
K. Rajappan1, P. Kistler1, M. Earley1, S. Harris1, D. Abrams1, D. Gupta1, M. Jahngir1, S. Ellis2, S. Sporton1, R. Schilling1.1The Department of Cardiology, St Bartholomew’s Hospital and Queen Mary University, London, UK; 2The Department of Radiology, St Bartholomew’s Hospital and Queen Mary University, London, UK
Introduction: A detailed appreciation of the LA/PV geometry may be important in improving the safety and success of catheter ablation for AF. The aim of the study was to determine the effect of CT image integration into a 3D mapping system on the clinical outcome of patients undergoing catheter ablation for AF.
Methods: Seventy five patients (table) with symptomatic AF underwent wide encirclement of ipsilateral PV pairs using irrigated ablation with the aim of electrical isolation. Ablation was guided by 3D mapping alone (carto 20, NAVX 17) in 37 (3DM group) patients and CT image integration (Cartomerge) was used in the next 38 (CT group) patients. In persistent AF (44), linear ablation of the LA roof, cavotricuspid isthmus, mitral isthmus and fractionated electrograms was also performed. Cardioversion was performed in 54% in the 3DM group and 58% in the CT group (p = NS) when AF did not terminate during ablation.
Results: see table. Successful PV electrical isolation did not differ between the two groups. CT image integration resulted in a reduction in fluoroscopy (p = 0.05) and procedure (p = 0.04) duration. A trend to a reduction in arrhythmia recurrence was demonstrated in the CT group. In 22 symptomatic patients (13 3DM and 9 CT gp) repeat procedures for AF (7 in 3DM gp and 5 CT gp) and AT (5 in 3DM gp and 5 CT gp, p = NS) were performed. PV reisolation was required in 22/22(100%). 17 ATs in 10 patients terminated with linear ablation in 14 and focal in three. Overall success on 7 day monitor off antiarrhythmic drugs was achieved in 59% in the 3DM group compared with 82% in the CT group (p<0.05) at a standardised follow up of 25±9 weeks.
Conclusion: Catheter ablation guided by CT integration into an EAM system is associated with reduced fluoroscopy and procedure times. The integration of CT to perform ablation of AF was associated with improved clinical success.
Abstract 034
catheter ablation; atrial fibrillation; image integration
035 INTERNAL CARDIOVERSION OF ATRIAL FIBRILLATION USING A NOVEL BIPHASIC WAVEFORM FROM A RADIOFREQUENCY POWERED DEFIBRILLATOR
B. M. Glover1,2, M. J. Roberts1, J. McC. Anderson3, A. A. J. Adgey1.1Regional Medical Cardiology Centre, Royal Victoria Hospital, Belfast; 2Queens University, Belfast; 3University of Ulster, Jordanstown, UK
Purpose: The optimal waveform for the transvenous direct current cardioversion of atrial fibrillation (AF) is unknown. Conventional devices for internal atrial defibrillation employ a capacitor based discharge with considerable tilt. We have addressed these issues by developing a novel biphasic waveform with no tilt. This is of 6/6 msec duration and phase 2 peak voltage is 50% of phase 1 similar to the conventional tilted biphasic waveform. The novel waveform is delivered from a unique radiofrequency (RF) powered defibrillator (140 KHz), which does not have a built in battery or capacitor. The purpose of this study was to compare this novel waveform with a conventional capacitor based trapezoidal biphasic waveform of equivalent duration and voltage.
Methods: Patients with persistent AF referred for an elective DC cardioversion and patients with inducible AF during a routine electrophysiology study were randomised to receive either the novel waveform or a conventional trapezoidal waveform. Bipolar defibrillation electrodes were positioned in the right atrial appendage (cathode) and distal coronary sinus (anode) under fluoroscopic guidance. Phase 1 peak voltage was increased in stepwise progression from 50–300V for both waveforms. The voltage, current, energy, and impedance were recorded for each shock using a digital oscilloscope. Success was defined as return of sinus rhythm for ≥30 seconds.
Results: A total of 178 shocks (RF = 88, conventional = 90) were delivered to 45 patients (25 persistent AF, 20 inducible AF). The novel waveform performed significantly better than the conventional waveform for the cardioversion of persistent AF. Cardioversion was successful in 10 of 13 patients (77%) using the novel waveform v 2 of 12 patients (17%) using the conventional waveform (p = 0.002). Of patients with inducible AF, 9/11(82%) were successfully cardioverted at 100 V or less with the novel waveform v 2/9 (22%) with the conventional waveform (p = 0.008). The mean leading edge voltage for the novel waveform was 223 V (persistent AF) and 90 V (inducible AF), and for the conventional waveform was 270 V (persistent AF) and 158 V (inducible AF). No significant arrhythmias, sinus pauses or episodes of hypotension occurred. There was no elevation of cardiac enzymes.
Conclusions: The novel biphasic waveform has a superior efficacy at a lower voltage compared with the conventional waveform for the transvenous cardioversion of AF. There were no arrhythmic, haemodynamic complications or elevation of cardiac enzymes. The transfer of RF energy in order to generate the waveform was successful in all cases. This technology could be incorporated into an implantable device (ventricular ICD or pacemaker incorporating AF suppression with passive defibrillation) with enhanced battery life. This highly efficacious waveform may also have uses beyond atrial defibrillation and could be studied in ventricular arrhythmias.
atrial fibrillation; novel biphasic waveform; radiofrequency energy transfer
036 VALIDATION OF 3-DIMENSIONAL CARDIAC IMAGE INTEGRATION: USE OF INTEGRATED CT IMAGE INTO ELECTROANATOMIC MAPPING SYSTEM TO PERFORM CATHETER ABLATION OF ATRIAL FIBRILLATION
K. Rajappan1, P. Kistler1, M. Earley1, S. Harris1, D. Abrams1, D. Gupta1, M. Jahngir1, S. Ellis2, S. Sporton1, R. Schilling1.1The Department Of Cardiology, St Bartholomew’s Hospital and Queen Mary University, London, UK; 2The Department Of Radiology, St Bartholomew’s Hospital and Queen Mary University, London, UK
Introduction: Accurate visualisation of the complex left atrial (LA) anatomy and the location of an ablation catheter within the chamber is important in the success and safety of ablation for AF. We describe the integration of CT into an electroanatomic mapping (EAM) system and its validation in patients undergoing catheter ablation for AF.
Methods and Results: Forty seven patients (59±8 years, 38M) with paroxysmal (23) and persistent (24) AF underwent ablation by wide encirclement (WE) of PV pairs using CT image integration into an EAM system. CT registration using the PVs as markers (landmark) was achieved with an error of 6.2±2.4 mm with repeat registration required in two patients. The PV registration errors were smaller for: RSPV 5.3±2.8 mm and RIPV5.4±2.6 mm compared with LSPV 6.7±3.2 mm and LIPV 6.9±4 mm (p<0.05). Registration of the CT by best fit to an EA geometry (surface) using 35±14 points was achieved with an error of 2.4±0.5 mm. In a subset of 30 patients the regional LA registration error at superior (1.7±0.7 mm), inferior (2.2±1.4 mm), septal (1.7±0.8 mm), and lateral (1.7±0.7 mm, p–0.13) sites was determined. Similarly there was no difference in the circumference of PV antra as measured by CT (right 13.9±1.5 cm and left 14.5±1.6 cm) compared with EAM (right 14.2±1.9 cm and left 14.4±2.4 cm, p = NS). Cardiac rhythm at the time of CT did not have a significant effect on registration accuracy (table). The integrated CT was used to guide encirclement of the PVs in pairs with electrical isolation achieved by maintaining ablation along the ablation line in 90 of 94 PV pairs. Post procedural PV angiography did not demonstrate significant stenosis.
Conclusion: CT image integration into an EAM system was successfully performed in patients undergoing catheter ablation for AF. With a greater appreciation of the complex and variable nature of the PV and LA anatomy this new technology may improve the efficacy and safety of the procedure.
Abstract 036
catheter ablation; atrial fibrillation; electroanatomic mapping
037 DO SYMPTOMS PREDICT ATRIAL FIBRILLATION EPISODES IN PAF PATIENTS?
R. Veasey1, J. Silberbauer1, J. Vrahimides1, A. Arya1, W. Taggu1, V. Paul2, A. Sulke1.1Eastbourne District General Hospital, Eastbourne, UK; 2St Peter’s Hospital, Chertsey, UK
Background: Using diary cards in conjunction with beat to beat pacemaker Holters, correlation between symptoms and atrial fibrillation (AF) episodes and duration is possible.
Methods: Eighty seven symptomatic paroxysmal atrial fibrillation (PAF) patients with AF burden of 1 to 50% were assessed. 46 pts were excluded due to incomplete diary cards or sensing aberrancy. Holters and corresponding symptom diary cards were analysed from the 41 remaining patients (age 71 +/−9, 58.5% male). Patients accurately documented time and duration of their symptoms and this was correlated with device Holter AF episodes. Symptoms without corresponding AF, asymptomatic AF, and symptomatic AF could then be described.
Results: 1960 days (5.4 years) of corresponding Holter and symptom diaries were analysed. 194 symptom episodes without AF, 333 symptom episodes with AF, and 4274 episodes of asymptomatic AF were recorded. Overall 92.8% of AF was asymptomatic. 36.8% of reported symptoms were not AF related. 63.2% of symptoms exactly correlated with episodes of AF (fig 1). The majority of patients identified less than 10% of their AF episodes.
The mean episode length of symptomatic AF (297.9+/−867.5 min) episodes was significantly longer than asymptomatic AF (66.7+/−324.6 min) episodes (p<0.0001). The distribution of AF episode onset time showed a double peak suggesting vagal triggers, however, the majority of symtomatic AF was initiated during daytime hours (fig 2).
Conclusions: In highly symptomatic PAF patients the majority of symptoms are due to AF episodes. However, the majority of AF detected by the devices was asymptomatic. Thus trials suggesting therapeutic efficacy of drugs and other interventions must be interpreted with caution, without complete beat to beat information.
atrial fibrillation; symptoms; Holter monitoring

Abstract 037 figure 1.
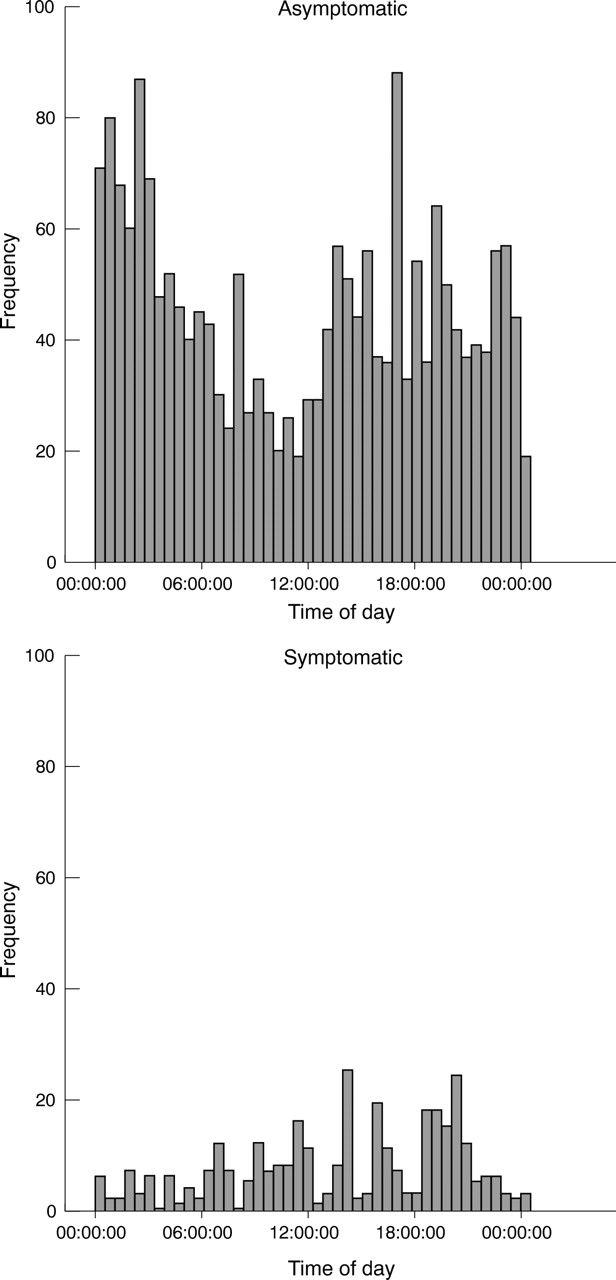
Abstract 037 figure 2.
038 RELATIONSHIP BETWEEN ANAEMIA AND QUALITY OF LIFE IN PATIENTS WITH HEART FAILURE
L. Tin, S. Nabb, K. Goode, H. Loh, J. Windram, P. Velavan, R. Shelton, J. Cleland.University of Hull, Hull, UK
Introduction: Anaemia may have an adverse effect on quality of life in patients with heart failure but the relationship is poorly described.
Method: 610 consecutive patients attending an outpatient specialist heart failure clinic with left ventricular ejection fraction (LVEF)<45% were asked to complete the Euro heart failure quality of life questionnaire which includes questions on overall and health related quality of life, oedema, fatigue and dyspnoea, memory, social life, hobbies, and mood. At the same clinic appointment, patients were also weighed and had blood pressure measurements, electrocardiogram, echocardiogram, full blood count, and biochemical profile done. Patients were divided into those without anaemia (by WHO criteria anaemia was defined as haemoglobin (Hb)<13 g/dl in men and <12 g/dl in men, those with mild anaemia (Hb up to 1.5 g/dl below WHO), moderate (1.5–3 g/dl below WHO) and severe (>3 g/dl).
Results: 71.1% were male. Mean age was 69.8 (10.3) years. Mean LVEF was 32.8 (10.4)%. Mean Hb was 13.7 (1.57) g/dl for men and 12.7 (1.47) g/dl for women. 30% of patients were found to be anaemic by WHO criteria. The anaemic patients had worse quality of life scores on heart failure symptoms of breathlessness and fatigue (p<0.05). Anaemia was also associated with poor appetite (p<0.05), inability to carry on with hobbies (p<0.01), reduced sexual activity (p<0.05), dizziness and falls (p<0.01), muscle fatigue (p<0.01), and loss of social interaction due to unwillingness or inability to leave the house (p<0.01). The difference in quality of life was consistent when those with mild anaemia (as defined above) were compared to those without anaemia. Compared to those with mild anaemia, those with severe anaemia were more likely to describe themselves as depressed (p<0.01), stressed (p<0.05), or suffering from insomnia (p<0.05).
Conclusion: Even mild degrees of anaemia have a significant impact on symptoms, ability to carry out daily activities and social interactions in the heart failure population, and thus needs to be investigated and treated.
heart failure; anaemia; quality of life
039 BETA-BLOCKER THERAPY IS ASSOCIATED WITH IMPROVEMENT OF RENAL FUNCTION AND ANAEMIA IN PATIENTS WITH HEART FAILURE
W. Khan, S. Deepak, A. Borg, T. Coppenger, C. Waywell, L. Harper, S. Williams, N. Brooks.South Manchester University Hospital NHS Trust, Manchester, UK
Introduction: Chronic renal impairment (CRI) and anaemia are both common comorbidities associated with chronic heart failure (CHF) and are independent predictors of poor prognosis. Angiotensin converting enzyme inhibitors are potentially nephrotoxic and cause worsening of anaemia. We aimed to assess the effect of beta-blocker (BB) therapy on renal function and anaemia in CHF patients.
Methods: A retrospective case-note study of 134 consecutive patients with stable CHF (with ejection fraction <45%) attending our heart failure clinic between 2002 and 2004 was performed. Serum creatinine and haemoglobin (Hb) levels checked 12 months before and 12 months after the initiation of BB treatment were recorded. Patients with anaemia due to an alternate cause or those on anaemia treatment were excluded from the study. CRI was considered to be present when serum creatinine level was ⩾ to 120 mmol/l, and anaemia if serum Hb level was ⩽ to 13.0 g/dl. Creatinine clearance (Cr) was calculated by Cockcroft-Gault formula. The South Manchester University Hospitals Trust ethics committee approved the study. Data are expressed as mean and standard deviations (SD). Statistical analysis was by the paired Student’s t test. p<0.05 was considered statistically significant.
Results: Of the 134 patients, 106 (79%) were male, mean (SD), age 68.76 (10.54); range 41–88 years, mean LVEF 31.54 (8.81)%, with a median (IQR) NYHA of II (I–III). One hundred and nineteen patients (93 (78%) men, mean age 68.29 (10.54); range 42–88 years) were treated with BBs. Fifteen patients (10 men (67%), mean age 72.5 (9.68); range 50–87 years, had contraindications to BB therapy. These subjects served as the control arm of this study. Among the 119 patients in the BB treatment group, 55 (46%) had CRI (46 male, 82%) and 42 (35%) were anaemic (31 male, 72%). Twenty three (19%) patients had both CRI and anaemia. Among the 15 patients in the control group, 10 (66%) had CRI, and eight (53%) had both CRI and anaemia. In patients who were receiving BB treatment, there was a significant 8.1% increase in creatinine clearance from 41.2 (13.2) to 44.5 (17.9) ml/minute (mean (SD)), p = 0.007. In comparison, in the 10 patients with CRI in the control group, there was significant 17.7% reduction in creatinine clearance from 46.9 (11.7) to 38.6 (6.5) ml/minute, P = 0.04. The 23 anaemic patients also favourably responded to beta-blocker treatment with significant 6.7% increase in mean Hb levels from 11.9 (1.1) to 12.7 (1.2) g/dl, p = 0.001. However, in the eight patients with anaemia in the control group, there was a 15.4% significant reduction in Hb from 13.6 (1.7) to 11.5 (1.3) g/dl, p = 0.03.
Conclusion: This study has shown that BB treatment is associated with an improvement in CRI and anaemia. Further large scale studies are needed to confirm our findings and to investigate the underlying mechanisms.
heart failure; anaemia; chronic renal failure
040 ANAEMIA OF UNKNOWN ORIGIN IN CHRONIC HEART FAILURE IS A CONSEQUENCE OF IMMUNE MEDIATED SUPPRESSION OF ERYTHROID COLONY FORMATION AND ERYTHROPOIETIN RESISTANCE
D. Okonko1, S. Marley2, M. Gordon2, P. Poole-Wilson1.1Clinical Cardiology, NHLI, Imperial College & Royal Brompton Hospital, London, UK; 2Haematology Department, LRF Centre for Adult Leukaemia, Hammersmith Hospital, Imperial College, London, UK
Background: Anaemia is a common and adverse phenomenon in chronic heart failure (CHF), but its origins are elusive in 50–60% of patients.
Hypothesis: We hypothesised that anaemia of unknown origin in CHF may be a consequence of CD34+ haematopoietic stem cell depletion, immune-mediated suppression of erythroid progenitor cell (BFU-E) colony formation, and a diminished responsiveness of erythroid cells to erythropoietin (EPO).
Methods: We studied 61 consecutive CHF patients (age 66±1 years, LVEF 30±1%, 82% male) and 20 healthy controls (63±2 years, 77% male). Circulating CD34+ cells, surface EPO receptors and intracellular EPO signal transducers (STAT5) were quantified by flow cytometry. Peripheral blood BFU-Es were cultured in methylcellulose, in the presence and absence of monocytes, sera, and anti-tumour necrosis factor (TNF) antibody, and with escalating doses of EPO.
Results: Compared to non-anaemic patients (n = 40) and controls (n = 20), anaemic patients (n = 21) had lower CD34+ cells and BFU-Es, and poorer BFU-E proliferation and colony cellularity (all p<0.001). Monocyte depletion enhanced BFU-E numbers by 35±8%, and BFU-E proliferation by 41±12% only in anaemics (all p<0.05). Only anaemic monocytes and sera suppressed BFU-E colony formation when co-cultured with autologous anaemic or allogeneic control T-cell depleted BFU-Es (n = 8, p<0.01). Serum levels of pro-inflammatory cytokines (TNF, soluble TNF receptor 1 and 2, interleukins 1β and 6) were higher in anaemic patients than non-anaemic patients and controls (all p<0.05). Only soluble TNF receptor-2 levels correlated to BFU-E proliferation (r = −0.60, p = <0.0001). Anti-TNF antibody partly abrogated the suppressive effect of anaemic sera on normal BFU-Es (p<0.05). Whereas control and non-anaemic BFU-E numbers significantly increased with 3 U/ml EPO, anaemics required 9 U/ml EPO (p<0.01). Anaemic patients had higher EPO receptor and baseline STAT5 expression than non-anaemics or controls (all p<0.01), but did not display an increase in STAT5 levels after EPO stimulation.
Conclusion: The pathophysiological features of anaemia of unknown origin in CHF mirror that seen in anaemia of chronic disease. Anaemic CHF patients demonstrate depleted circulating haematopoietic stem and erythroid progenitor cells that proliferate poorly and are relatively resistant to EPO. Activated monocytes suppress erythroid differentiation and proliferation, partly via the elaboration of TNF. Relative EPO resistance results from deranged EPO signal transduction. While residual EPO responsiveness can be explored clinically with erythropoietic agents, optimal anaemia correction in CHF may require additional strategies that dampen aberrant monocyte activity.
anaemia; heart failure; cytokines
041 BOTH STATIN USE AND AN ELEVATED CHOLESTEROL CONFER A PROGNOSTIC BENEFIT IN PATIENTS WITH HEART FAILURE
J. Windram, P. Loh, L. Tin, A. Rigby, A. Clark, J. Cleland.Hull Royal Infirmary, Hull, UK
Background: An elevated hsCRP has been shown to confer a poor prognosis in patients with systolic heart failure. The use of statin therapy as anti-inflammatory therapy has been advocated by some. Paradoxically an elevated cholesterol level confers a better prognosis in such patients. Cholesterol may protect patients from increased inflammation secondary to endotoxins. We aimed to see if elevated cholesterol was protective and if statin therapy was safe in patients with heart failure.
Methods: A group of 888 patients with left ventricular systolic impairment were followed up for a period of three and a half years. All had a baseline assessment which included a full clinical history and examination. A full biochemical and haematological profile was taken, which included a total cholesterol and hsCRP sample. An ECG and an echocardiogram were also performed.
Results: The mean age of the population was 71 (SD 10) years. 635 (72%) were men. 462 (52%) of the patients were receiving statin therapy. In our population the median value of CRP was 5 (interquartile range 2.8 to 11). For total cholesterol we had a median value of 4.7 (interquartile range 4.1 to 5.5). Those receiving a statin had a better prognosis than those who did not receive one. The relative risk (RR) being 0.93 (confidence interval, 0.88 to 0.99, p = 0.03) in the statin group. To examine how CRP and cholesterol interacted we graded patients into four groups using the population medians of CRP and cholesterol to act as the points at which we would describe the values as high or low. We found that those with a high CRP and low cholesterol had the highest RR of 1.28 (1.18 to 1.40). Those with a high CRP and high cholesterol though still at a higher risk of death with a RR of 1.17 (1.08 to 1.27) had an improved survival compared to the high CRP low cholesterol group. In both groups with a CRP lower than the population median survival was better. The higher cholesterol group had the greater relative risk of 1.03 (0.96 to 1.09) though this was not significant. When examining the effect of statin therapy in each of these groups we did not see a difference in relative risk except for those in the worst prognostic group (high CRP, low cholesterol). The use of a stain in this group indicates a strong trend toward a protective benefit with a relative risk of 0.86 (0.74 to 1.01, p = 0.096).
Conclusion: In patients with systolic heart failure raised CRP and low total cholesterol confers a poorer prognosis. Increased total cholesterol appears to be protective in patients with an increased inflammatory response. Interestingly the use of statins in those with a low cholesterol and high CRP appears to improve prognosis. The use of statins in the other groups showed little significant benefit. Further studies are required to determine at what level cholesterol may be protective in the setting of an elevated CRP. In future we may have to consider the balance between CRP and cholesterol when we titrate statin therapy.
hsCRP; cholesterol; heart failure
042 THE INCREASED INFLAMMATORY RESPONSE SEEN IN HEART FAILURE IS RELATED TO THE SEVERITY OF TRICUSPID REGURGITATION RATHER THAN THE SEVERITY OF LEFT VENTRICULAR IMPAIRMENT
J. Windram, L. Tin, P. Loh, A. Rigby, A. Clark, J. Cleland.Hull Royal Infirmary, Hull, UK
Background: The acute phase protein C-reactive peptide (CRP) is primarily produced within the liver. A raised CRP has been shown by several groups to confer a poor prognosis in patients with systolic dysfunction. It has been postulated that oedema within the bowel wall allows bacterial endotoxins to enter the bloodstream thereby inducing an inflammatory response. We aimed to examine the relationship between the inflammatory response and liver congestion secondary to left ventricular impairment and the severity of tricuspid regurgitation.
Methods: A group of 917 patients with left ventricular systolic impairment were assessed in our outpatient clinic. All had a baseline assessment which included a full clinical history and examination. A full biochemical and haematological profile was taken, which included a full set of liver function tests and hsCRP sample. An ECG and an echocardiogram were also performed. Results The mean age of the population was 71 (SD 10) years. 660 (72%) were men. HsCRP was not related to left ventricular function. No difference was noted between those who had mild left ventricular impairment (median 4.85, interquartile range 2.7 to 12) and those that had severe impairment (5.4, IQR 3 to 11) p = 0.96. When we looked at those patients who had tricuspid regurgitation we found that as the severity increased so did the CRP levels. Those with mild to moderate regurgitation had a median CRP value of 5 (IQR 3 to 12) whereas those with severe regurgitation had a median of 9.8 (IQR 5.4 to 21) p = 0.014. When we examined changes in liver function tests between those with mild and moderate left ventricular impairment we noted a significant rise in bilirubin (mild LV impairment median bilirubin 14 (IQR 12 to 18), severe LV impairment median bilirubin 17 (IQR 14 to 22), p<0.0001) but no change in alkaline phosphatase levels. However when we looked at those who did not have tricuspid regurgitation and those with severe regurgitation we found significant changes in both bilirubin (no TR median bilirubin 14 (IQR 12 to 19), severe TR 20 (IQR 16 to 26] p = 0.002) and alkaline phosphatase (no TR median ALP 66 (IQR 56 to 82) severe TR median ALP 89 (70 to 117) p<0.0001). In addition those with severe tricuspid regurgitation had a reduced serum albumin (no TR median albumin 38 (IQR 37 to 41) severe TR 35 (IQR 33 to 38) p<0.0001).
Conclusion: The inflammatory response in heart failure is related to the severity of tricuspid regurgitation. No change is observed in hsCRP between those with mild and severe left systolic impairment. As the severity of tricuspid regurgitation increases we see an increase in hsCRP. Those with severe tricuspid regurgitation show the greatest degree of inflammation. Despite our observations the primary trigger for CRP production in heart failure patients remains unknown. Further studies are needed to determine whether cholestasis induced by venous congestion is the cause or whether it is driven by endotoxins from oedema of the bowel wall.
inflammation; heart failure; prognosis
043 PATIENTS WITH CHRONIC HEART FAILURE HAVE REDUCED FOOD INTAKE AND POORER NUTRITIONAL INTAKE COMPARED WITH HEALTHY VOLUNTEERS
C. Hughes1, C. Mc Gartland2, G. Cran2, M. Roberts1, D. Nicholls1, P. McKeown2.1Royal Victoria Hospital, Belfast, UK; 2Queen’s University, Belfast, UK
Introduction: Cardiac cachexia is a recognised complication of chronic heart failure, with weight loss and muscle wasting similar to that seen in cancer patients. It occurs in heart failure patients irrespective of left ventricular ejection fraction but is an independent predictor of morbidity and mortality. The cause of cardiac cachexia is not well understood but higher metabolic rate and increased cytokine and endocrine activation are proposed contributory mechanisms. Decreased appetite in heart failure patients may also plat a role but there are very few published data on dietary intake and nutrition in these patients.
Aims: The aim of this study was to establish if there is a significant difference in nutritional content of typical diets of heart failure patients compared to those of control subjects.
Methods: In this study we compared dietary intake of chronic heart failure patients with normal control subjects. Each subject completed a four day food intake diary, which was then reviewed by the investigator and analysed using WISP nutritional analysis software. All patients were given detailed instruction on how to fill in the diary and the completed diary was reviewed by the investigator using a standard food atlas to confirm portion sizes on the day after completion. Patients were requested not to change their dietary intake during the recording of the food diary. Left ventricular systolic dysfunction was confirmed by echocardiogram.
Results: Food diaries were completed by 37 heart failure patients (32 male, mean age 68 (SD 10) years) and 27 controls (21 male, mean age 60 (SD 9) years). There were 18 New York Heart Association (NYHA) class II, 15 NYHA III, and 4 NYHA IV heart failure patients. Statistical analysis (using the Wilcoxon Sign Rank test) showed significant differences in median total daily energy consumption (1852 v 2211 kcal, p = 0.002), total fat (73.6 v 89.8 g, p = 0.007) and saturated fat intake (25.3 vs 33.5 g, p = 0.012), protein consumption (71.1 v 84.8 g, p = 0.020), carbohydrate intake (194 v 260 g, p = 0.001) and daily dietary micronutrient levels (see table). There was also a statistically significant difference in median alcohol consumption (p = 0.019)
Abstract 043
There was no significant difference in selenium or vitamin B12 intake between the two groups.
Conclusion: Chronic heart failure patients have significantly lower energy intake and dietary micronutrient consumption than normal control subjects. This may in part contribute to the cardiac cachexia syndrome in some heart failure patients. Improving the nutritional intake of chronic heart failure patients should be investigated as a therapeutic intervention.
heart failure; nutrition; cachexia
044 ELEVATED GLYCATED HAEMOGLOBIN IS A STRONG PREDICTOR OF MORTALITY IN PATIENTS WITH SUSPECTED HEART FAILURE
J. John, K. Goode, A. Rigby, P. Reddy, A. Clark, J. Cleland.Castle Hill Hospital, Hull, UK
Background: Heart failure (HF) is associated with impaired glucose metabolism. Abnormal glycemic control indicated by elevated glycated haemoglobin (HbA1c) levels has a linear relationship with cardiovascular risk and total mortality in the general population, but no such data exist on at risk populations with a prior diagnosis of HF.
Aim: We sought to identify the relationship between HbA1c and cardiovascular mortality in a heart failure population with and without diabetes mellitus (DM).
Methods: Data were collected from 1119 consecutive patients seen in the HF clinic. All underwent full clinical examination, echocardiogram, 12-lead electrocardiogram (ECG), 6-minute walk test, pulmonary function test, and comprehensive biochemical and haematological profiles including HbA1c. Descriptive data are presented as either means with standard deviations (SDs) or as percentages. Diabetic groups were compared by analysis of variance (ANOVA) or by the χ2 test for continuous and categorical variables respectively. Age adjusted odds ratios were calculated by logistic regression. The Cox proportional hazards model was used to determine the independent contributions of HbA1c and DM to all-cause mortality after adjusting for age, BMI, current cigarette smoking, total cholesterol, history of IHD, and vascular disease.
Results: The mean age of all patients was 70.6 years (range 25–96 years); 37% of patients (n = 416) were aged >75 years of age; 58% (n = 645) were men. 215 (19.2%) patients had DM. Those with known DM had higher concentrations of HBA1c (7.8%, SD = 1.5%) than the rest of the study sample (6.2%, SD = 0.8%). They were slightly younger (69.2 years) but had a higher body mass index; a greater proportion had vascular disease and ischemic heart disease. Patients had a poorer 12 month mortality in the presence of a moderately raised baseline HbA1c (6.5 – 7.5%) compared to those with normal (<6.5%) or significantly raised (>7.5%) levels. This was shown to be statistically significant at the p = 0.05 level using bootstrap analysis. Mortality peaked at 17% with an HbA1c of approximately 7% compared to 5% mortality for normal HbA1c levels, irrespective of the presence or absence of DM.
Discussion: These data supports, in HF population, a graded and moderate increase in total mortality with increasing levels of HbA1c in persons with and without diabetes mellitus. After inclusion of HbA1c in the Cox regression model DM no longer remained significant (p = 0.06 for women; p = 0.75 for men), suggesting that all the risk is probably mediated through elevated HbA1c, even below threshold commonly accepted for the diagnosis of DM and independent of age. The reasons for this finding are not clear and require further evaluation.
heart failure; diabetes mellitus; glycated haemoglobin
045 PARAMEDICS’ PERCEPTIONS OF THEIR ROLE IN PROVIDING THROMBOLYTIC TREATMENT IN ACUTE MYOCARDIAL INFARCTION: QUALITATIVE STUDY
H. Cox1, J. Albarran1, T. Quinn2, K. Shears3.1University of the West of England, Bristol, UK; 2Coventry University, Coventry, UK; 3Wiltshire Ambulance Service NHS Trust, Chippenham, UK
Background: Thrombolytic therapy is provided by the majority of ambulance services in England following publication of the National Service Framework for Coronary Heart Disease. The effectiveness of prehospital administration in terms of all-cause mortality reduction and time saved has been confirmed by meta-analysis. Little is known, however, about how paramedics perceive additional responsibilities associated with thrombolytic administration.
Objectives: To describe ambulance paramedics’ perceptions of their role and impact in delivering thrombolytic treatment in the prehospital setting.
Setting: Rural ambulance service in the South West of England serving an estimated population of 600 000.
Participants and Methods: Twenty paramedics participated in focus groups. Results: Five themes emerged following the analysis of transcripts, these included: drivers for change; duty of care; perceptions of professional image; role expansion; and preparedness for practice. These themes captured a range of professional image and political issues which were triggered in response to paramedics’ role expansion.
Discussion: Paramedics’ perceptions of their role in relation to prehospital thrombolysis were mixed. Active engagement of paramedics in operationalising key changes to healthcare delivery is essential to effective implementation and to promote a sense of ownership by those delivering care.
paramedics; thrombolytic treatment; reperfusion
046 CLIENT CENTRED RISK FACTOR INTERVENTION IN FIRST DEGREE RELATIVES OF PATIENTS WITH PREMATURE MYOCARDIAL INFARCTION
J. Oliver, M. Farrer.Sunderland Royal Hospital, Sunderland, UK
Aim: To assess cardiovascular risk factors in first degree relatives of patients with a premature (less than 60 years) myocardial infarct (MI) within two months of the index event and to offer client centred interventions for each risk factor identified.
Methods: The families of 122 patients with premature MI included 437 first degree relatives. 298 (68%) attended a nurse led clinic at baseline. 241 of these (114 male, 127 female, 123 siblings, 118 children) have been followed up at 6 and 12 months. At baseline risk factors were assessed, health promotion advice was given and client centred interventions were offered. Risk factors and attitudes to their health were reassessed at 6 and 12 months.
Results: At baseline 64.4% had at least one important modifiable risk factor; current smoker (33.2%), diabetes (2.9%), high cholesterol >8 mmol/l (3%), hypertension (systolic >160 mmHg or diastolic >100 mmHg) (12.9%), BMI>30 (29.9%).
Siblings were older than children (47.6 (SD 10.8) v 28.8 (6.7) years) had higher body fat (30.8% (8.8) v 24.6% (9.1) p<0.001), were more likely to be hypertensive (17.1% v 8.5% p<0.001), and had higher cholesterol (5.65 mM (1.2) v 5.14 (1.0) p<0.001). Males consumed more alcohol than females (21.1 units (19.1) v 8.16 (12.9) p<0.001), smoked the same, had higher systolic blood pressure (131 mmHg (16.3) v 124 mmHg (20.5) p<0.005), higher triglycerides (2.21 mM (1.8) v 1.5 (1.0) p<0.001) and lower HDL (1.23 mM (0.3) v 1.37 (0.3) p<0.001). At baseline 130 (53.9%) were not satisfied with their health, 61% wanted to improve their lifestyle overall. 48% thought their family was at an increased risk of MI, 34% thought their own risk of MI was increased. Of the smokers 80% wanted to stop.
178 (74%) were reassessed at 6 months and 168 (70%) at 12 months. Fewer smokers presented for follow up. In those followed up, changes from baseline to twelve months occurred in alcohol consumption (14 units (17) to 12 (14) p<0.001), portions of fruit and vegetables eaten (2.5 (1.7) to 3.6 (1.7) p<0.001). HDL (1.30 mM (0.3) to 1.45 (0.3) p<0.001), triglycerides (1.85 mM (1.5) to 1.71 (1.1) p<0.005), although total cholesterol, BMI, and blood pressure remained unchanged. Numbers smoking decreased (33% to 25% p<0.017). Of those returning to clinic at 12 months 4.8% had an increase in the number of significant risk factors, 62.7% had no change and 32.5% had fewer significant risk factors (p<0.001). Exercise scores were unchanged. Anxiety scores fell (HAD anxiety 7.7 (4.1) v 5.7 (3.6) p<0.005).
Conclusion: Using a simple screening and intervention model it was possible to significantly improve risk factor profiles in 1st degree relatives of patients with a recent premature MI.
CHD prevention; risk factors; high risk patients
047 EUROACTION: A CARDIOVASCULAR PREVENTION AND REHABILITATION PROGRAMME
C. Jennings1, A. Mead1, J. Jones1, A. Holden1, K. Kotseva1, S. Connolly1, D. Wood1, G. De Backer2, D. De Backer2, on behalf of the EUROACTION Study Group.1Imperial College, London, UK; 2Department of Public Health, University of Ghent, Belgium
Introduction: EuroAction is a cluster randomised controlled trial of a preventive cardiology programme in general hospitals in six countries. The intervention is a nurse led, multidisciplinary, family based programme for coronary patients, their partners and the first degree relatives of patients with premature disease. The aim of the programme is to manage patients and their families to the European lifestyle, risk factor, and therapeutic targets for cardiovascular disease prevention.
Methods: One pair of matched hospitals in each country was randomised to the EuroAction programme or usual care. Consecutive coronary patients were actively recruited by the EuroAction nurses with a first presentation of coronary disease: myocardial infarction (MI), unstable angina or stable angina. All patients and partners were invited to attend a 16 week programme addressing lifestyle, risk factor management and cardio-protective medications.
Results: 1060 (67%) of all eligible coronary patients, 48% with acute myocardial infarction and 52% with angina were recruited to the programme. 637 (77%) partners of coronary patients also attended the programme. 713 (83%) patients completed the programme attending at least 6–8 group educational sessions (68%), and physical activity sessions (77%). At the end of the programme 58% of patients smoking prior to their event were not smoking, 16% had relapsed, and 26% continued to smoke. Proportions of patients (and partners) eating <10% of total energy as saturated fat increased significantly by 18% (8%); % fruit and vegetable consumption >400 g/day also increased significantly by 23% (25%); % eating fish >3 times per week increased significantly by 20% (15%). Proportions of patients (and partners) who became regularly active (Caspersen and Powell classification) increased significantly from 47% (50%) to 81% (64%). The proportion of patients (and partners) who were overweight (BMI>25 kg/m2) or obese (BMI>30 kg/m2) at baseline was 78% (64%). The initial weight loss target was 5–10% and the proportion of patients and (partners) achieving ≥ 5% in those who were overweight was 15% (11%) and 18% (16%) for the obese. Proportions of patients (and partners) with a waist circumference above action level 2 (≥ 102 cm for men and ≥ 88 cm for women) decreased from 34% men (45% female partners) and 60% women (20% male partners) to 27% men (39% female partners) and 56% women (17% male partners).
Conclusions and Implications: This nurse led, multidisciplinary, family based preventive cardiology programme successfully recruited a large majority of coronary patients and their families in their local hospitals, and most completed the programme. These families made healthy changes by stopping smoking, modifying their diets, and increasing physical activity levels which will reduce their risk of further cardiovascular disease.
preventive cardiology; nurse-led; EuroAction
048 IMPACT OF EARLY HEALTH EDUCATION AND RISK FACTOR ADVICE FOR PATIENTS WITH UNSTABLE ANGINA
K. Roche1, J. Goodfellow1, C. Jones1, R. West2.1Princess of Wales Hospital, Bro Morgannwg NHS Trust, Bridgend, UK; 2Wales Heart Research Institute, Cardiff, UK
Background: Research in cardiac rehabilitation (CR) is mostly restricted to patients with myocardial infarction. Few trials have focussed on patients with unstable angina (UA). CR is advocated for patients with UA, but the programme often commences weeks after the event. However, UA patients face a high initial risk of mortality or further event, and could benefit from much earlier education and behavioural change. We have undertaken a randomised controlled trial (RCT) to identify the psychological and behavioural consequences of early nurse-led education in UA.
Methods: A RCT compared early health education with usual care in 200 patients with a working diagnosis of UA in one district general hospital. Patients were invited to enter the trial if they had not undertaken a CR programme in the previous six months and were not immediately referred for revascularisation. Intervention involved two CR sessions, one as an in-patient and one within two weeks of discharge, focussing on coronary risk factor knowledge. Structured interviews were used to evaluate independently the primary outcomes of change in knowledge of disease at six weeks, and risk factor modification, and psychological status at six months.
Results: Baseline measures of health related quality of life (HRQoL, McNew questionnaire), knowledge and understanding of UA, and modifiable risk factors were comparable in the two groups. Treatment in hospital and medication on discharge were comparable. At six weeks, knowledge of coronary heart disease increased significantly in both intervention and control groups (modified York score, 30 (SD 8) before v 26 (SD 10) after, p<0.01 for both groups). At six months, smoking prevalence had also reduced similarly (29% before v 17% after, p<0.01 in both groups), and global HRQoL scores improved similarly (global score 3.2 (SD 0.8) before and 5.5 (SD 1.2) after, p<0.01 in both groups). There was little overall difference between the intervention and usual care groups.
Conclusion: UA is followed by significant beneficial changes in some aspects of of risk related behaviour and HRQoL, presumably due to good quality usual care on the wards and in primary care. Early, brief but intensive advice on risk factor management for patients with UA appears to have little additional impact on knowledge of coronary disease and risk related behaviour. Further analysis will show if this early intervention can be targeted to patients most likely to benefit.
health education; unstable angina; randomised controlled trial
049 HEART FAILURE AND PALLIATIVE CARE: THE DIFFERENCES IN ASSESSMENT OF HEART FAILURE PATIENTS
N. Rahman1, D. O’Hanlon2, D. McCarthy1, D. Segal1, J. Gibbs1.1Hammersmith Hospitals NHS Trust, London, UK; 2Trinity Hospice, London, UK
Introduction: The supportive and palliative care needs of heart failure patients are currently not being met despite the poor prognosis, which is worse than many cancers. Patients have a poor quality of life and suffer intense debilitating symptoms such as pain, dyspnoea, nausea and low mood, which are not acknowledged or managed effectively by heart failure services, despite the knowledge base available from palliative care.
Objectives: The aim of the study was to identify the differences between a heart failure and palliative care nurse specialist assessment of the palliative care needs of a heart failure patient. To develop a holistic assessment tool that effectively identifies their palliative care needs.
Method: Action research—a systematic enquiry designed to obtain practical results to improve a specific aspect of practice.
-
Sequential patient sample
-
10 patients, 8 = male, 2 = female; aged 36–97 years
-
New York Heart Association classification (NYHA) II–III
-
Three heart failure nurse specialists
-
One palliative care nurse specialist
-
Heart failure assessment tool.
An initial home assessment was carried out with two heart failure and one palliative care nurse specialists. Each nurse identified the patient’s problems and devised a management plan that was discussed and the differences documented by the 3rd heart failure nurse. Concurrently the assessment tool was reviewed and modified and the new version used for the subsequent patients.
Results: Initially the heart failure nurses focussed more on the management of the condition, specifically education, titration of medication and physical symptoms such as oedema and breathlessness. In contrast the palliative care nurse identified other symptoms such as nausea, constipation, and pain and also paid more attention to their social, spiritual, and psychological needs. As the study progressed, the heart failure nurses identified more palliative care needs for their patients and through discussion with the palliative care nurse felt more confident in medication advice and suggesting non-pharmacological input such as hospice day care and psychological review.
Conclusion: This research identified that there are differences in the assessment of supportive and palliative care needs of heart failure patients between heart failure and palliative care nurse specialists. The development of an effective assessment tool and working with a palliative care nurse, can teach heart failure nurses to identify generic palliative care issues and provide appropriate management.
Recommendations: Education and training for heart failure nurses in the assessment and symptom control of generic palliative care, also communication skills. Developing a referral criteria and pathway for specialist palliative care and collaboration between the services to provide supportive and end of life care for heart failure patients.
heart failure; palliative care; nurse
050 PATIENTS WITH NON-CARDIAC CHEST PAIN: HOW A SIMPLE INTERVENTION MAY HELP
T. Lennox, A. MacDermott, D. Phelps, P. Adams, C. Baker, I. Haq.Royal Victoria Infirmary, Newcastle upon Tyne, UK
Background: Approximately one third of patients referred to the Newcastle Rapid Access Chest Pain Clinic present with non-cardiac chest pain. Despite the good prognosis in this group, many people remain concerned about their symptoms and this may adversely affect quality of life and lead to repeated hospital contacts. We hypothesised that providing these people with a short structured interview would address their concerns, increase understanding of their symptoms, and reduce the emotional impact of the “illness”.
Methods: Patients with non-cardiac chest pain were assigned to “usual care” or structured feedback. People with a history of angina or myocardial infarction were excluded. Patients completed the chest symptom perception questionnaire (CSPQ) sent by post prior to the clinic appointment. This is a modified and validated version of the illness perception questionnaire which includes measures on “illness coherence” (how much they understand their symptoms) and “emotional representation” (the emotional impact of the illness). A structured informational package was developed between consultant cardiologists and the chest pain nurse based on established cognitive behavioural principles. This consisted of a five minute consultation conducted by the chest pain nurse covering psychological and physical aspects of the symptoms, patients’ concerns and expectations, and possible non-cardiac diagnoses. Abnormal beliefs were discussed and corrected, and a self-help plan about how to cope and return to normal activities were covered. A random sample of interviews were recorded and assessed by a consultant clinical psychologist to ensure adherence to the written protocol. Written information was also provided. Patients then completed the CSPQ after the consultation. Data were analysed by ANCOVA using baseline measures as covariates. A sample size of 39 in each group was necessary to detect a medium effect (d = 0.65) with 80% power at alpha 0.05.
Results: Forty patients were assigned to usual care and 41 people to intervention. 22% versus 21% of patients were men (p = 0.31). Mean age (years) was 55 versus 56; p = 0.80. Percentage of patients who underwent an exercise test was 34% versus 21%; p = 0.90. There was no significant difference in level of health anxiety between the two groups. Mean scores for illness coherence changed from 18.4 to 16.6 in the usual care group, and from 18.0 to 13.8 in the intervention group (F(1,78) = 7.1, p = <0.01). Mean scores for emotional representation changed from 19.5 to 16.1 in the usual care group, and from 17.9 to 14.2 in the intervention group (F(1,78) = 1.04, p = 0.32).
Conclusion: A brief discussion based on cognitive behavioural principles with patients presenting with non-cardiac chest pain is feasible as part of everyday practice. Patients who received this understood their symptoms significantly better than those receiving usual care, although the emotional impact of the illness was not significantly altered.
non-cardiac chest pain; illness perception; structured feedback
051 A DISTRICT GENERAL HOSPITAL’S EXPERIENCE OF IMPLEMENTATION OF THE NSF, CHAPTER 8, ARRHYTHMIA, AND SUDDEN CARDIAC DEATH. THE FIRST TWO YEARS’ EXPERIENCE OF AN INNOVATIVE NURSE-LED RAPID ACCESS ATRIAL FIBRILLATION CLINIC
D. Sevant.Southend Hospital, Southend, UK
Introduction: Cardiac Arrhythmia affects more than 700 000 people in England and is consistently in the top 10 reasons for hospital admission. Atrial fibrillation (AF) is the commonest cardiac arrhythmia. AF either complicates or causes many other medical conditions, such as stroke. Treatment strategies include ventricular rate control or restoration of sinus rhythm by direct current cardioversion (DCC). DCC is a cost effective approach to the management of AF (Catherwood et al, 1999). The likely success of DCC depends on the duration of the AF, therefore rapid DCC will increase the chances of restoring sinus rhythm.
Method: Prior to the development of a Rapid Access Atrial Fibrillation/Flutter Clinic (RAAF) it had been identified that referral to treatment times for DC cardioversion were in excess of 44 weeks. Success of DC cardioversion was 75%. Furthermore there were no care pathways to provide continuity of care, no follow up of these patients, and no audit to define long term outcomes. In January 2004, with the support of the consultant cardiologists, a nurse-led service was piloted providing prompt referral for investigation and treatment of patients with new onset Atrial fibrillation or flutter (AF). Patients are booked for rapid access assessment with electrocardiogram (ECG), echocardiogram, and Nurse Specialist consultation. Anticoagulation is initiated if not already done and an appropriate decision regarding defibrillation is made with the patient fully informed. Following cardioversion, undertaken by the nurse specialist, the patients are reviewed in a six week follow up clinic and subsequently an ECG repeated after one year. An evidence based pathway for treatment and follow up has been developed in order to provide seamless care.
Results: Improvements to patient care since development of the RAAF service include referral to treatment now 16 weeks, preassessment clinic, and cardioversion now undertaken by the nurse specialist, DCC success rate 100%. Direct access has reduced referral to clinic wait to four weeks, aiming to be two weeks by March 2006. Outcome data are being used to inform practice. Further audit will be undertaken in January 2006 to demonstrate further service improvements for 2005, demonstrating timely, supportive treatment for patients with new onset atrial fibrillation.
Conclusion: The first two years of our service development have clearly improved outcomes for patients with new onset atrial fibrillation and flutter using a nurse-led approach. Key documents, such as the NSF and recent NICE Guidance for treatment of atrial fibrillation/flutter further support these developments. There is a need for sharing of good practice and development of similar services for district general hospitals nationally in order to address the needs of the arrhythmia NSF.
atrial fibrillation; rapid access; DC cardioversion
052 NURSE-LED PRESCRIPTION OF LOW MOLECULAR WEIGHT HEPARINS FOR ACUTE CORONARY SYNDROMES IMPROVES SAFETY
L. Hudsmith1, S. Haldar2, S. Bull2, N. Chahal2, M. Brunton2, C. Mckenna2, W. Orr2.1Department of Cardiovascular Medicine, the John Radcliffe Hospital, Oxford, UK; 2Department of Cardiology, the Royal Berkshire Hospital, Reading, UK
Background: Patients presenting with acute coronary syndrome (ACS) represent a large and undoubtedly high risk group. The use of low molecular weight heparin (LMWH) has revolutionised the treatment of these patients. High risk patients are also treated with aggressive antiplatelet therapy, often combining glycoprotein IIb/IIIa inhibitors with aspirin and clopidogrel. Failure to prescribe the correct weight adjusted dose is associated with increased morbidity and mortality, either because of overtreatment leading to haemorrhagic complications, or recurrent ischaemia due to inadequate antithrombotic effect.
Method: We investigated the accuracy of LMWH dosing of patients admitted as an emergency with an acute coronary syndrome (ACS). 64 inpatients (56% male) with ACS were identified and weighed within 24 hours of admission (67 (SD 13) years, 74 (SD 13) kg). Patient demographics and the dose of dalteparin prescribed and received were noted. The correct weight adjusted dose for each patient was calculated and compared to the actual dose received. After a two month period of education of doctors, nurses, and pharmacists involved, including the presentation of the results from the Group 1 audit, and with the initiation of nursing staff weighing patients and highlighting the appropriate dose of LMWH, a further 43 patients with a diagnosis of ACS were identified (Group 2) and data were collected in the same way.
Results: In Group 1 53% of the patients received an inappropriate dose of LMWH: 19% (12) overtreated and 34% (22) undertreated. Two months later, after staff education and with the introduction of nurse-led prescription, a highly significant improvement in the safe prescribing of LMWH was seen, 77% of patients in Group 2 receiving a therapeutic dose, 23% being overdosed, and none undertreated. The mean dosing error was reduced from 779 (SD 640) IU in Group 1 to 86 (SD 181) IU in Group 2 (p<0.001).
Discussion: Emergency care of patients with acute coronary syndrome requires early identification of those at increased risk and prompt commencement of a number of highly effective evidence based therapies. These patients may receive thrombolysis, LMWH, aspirin, clopidogrel, and glycoprotein IIb/IIIa antagonists, all of which at correct dosage convey an increased risk of bleeding, especially when vascular procedures are undertaken. This risk of bleeding is greater still in the increasingly elderly population now presenting to hospital with ACS. Inaccurate prescribing of LMWH and other antithrombotic agents will further increase the risk haemorrhagic complications or fail to give full protection against ongoing ischaemia. We have demonstrated that formal involvment of cardiac nursing staff in the prescription of LMWH brought about a significant improvement in dosing accuracy and illustrates the importance of a multidisciplinary team approach to the care of patients with ACS.
acute coronary syndrome; low molecular weight heparin; audit
053 NEUROCOGNITIVE FUNCTION, CEREBRAL EMBOLI, AND S100β AFTER ON-PUMP AND OFF-PUMP CORONARY ARTERY BYPASS SURGERY: A RANDOMISED STUDY
R. Motallebzadeh1, J. Bland2, H. Markus3, J. Kaski4, M. Jahangiri1.1Department of Cardiothoracic Surgery, St George’s Hospital Medical School, London, UK; 2Department of Health Sciences, York University, York, UK; 3Department of Clinical Neurosciences, St George’s Hospital Medical School, London, UK; 4Department of Cardiological Sciences, St George’s Hospital Medical School, London, UK
Introduction: Neurocognitive impairment can be a debilitating complication following coronary artery bypass surgery (CABG). Cardiopulmonary bypass, in particular cerebral emboli, has been implicated. Neurocognitive function, cerebral emboli and a serum marker of cerebral injury, S100β, were measured in patients undergoing on-pump and off-pump CABG.
Methods: 212 patients admitted for elective CABG were randomised to on-pump (n = 104) and off-pump (n = 108) surgery. Embolic signals (ES) were detected with bilateral transcranial Doppler ultrasound of the middle cerebral artery. A battery of neurocognitive tests was administered preoperatively, on discharge from hospital, at six weeks, and six months following surgery. Serum S100β was measured before surgery, intraoperatively, and at 48 hours. Composite neurocognitive scores were derived using principal component analysis and were compared between the two groups, using analysis of covariance to adjust for baseline values.
Results: At discharge from hospital, the adjusted composite neurocognitive score was 0.25 standard deviations (SDs) greater in the off-pump than on-pump group (95% CI 0.05 to 0.45; p = 0.01). There was no significant difference at six weeks (0.09 SDs, 95% CI −0.11 to + 0.30; p = 0.4) and six months (−0.002 SDs, 95% CI −0.23 to +0.23; p = 1.0). Median number of ES was 1065 (751–2473) during on-pump and 9 (4–27) in off-pump CABG (p<0.001). Age, length of education, and on-pump status were independent predictors of the pre-discharge neurocognitive score. The ratio of mean intraoperative S100β in on-pump to that in off-pump was 1.92 (95% CI 1.64 to 2.25, p<0.001). After 48 hours, the ratio was 1.01 (95% CI 0.91 to 1.14, p = 0.9). Only the 48 hour S100β level for off-pump surgery correlated with neurocognitive score at discharge (Kendall’s taub = −0.16, p = 0.03).
Conclusions: Cerebral emboli are more prevalent during on-pump CABG. At discharge from hospital, neurocognitive function is better after off-pump surgery, although we cannot conclude that this is due to the lower embolic load. However, the difference in neurocognitive function does not persist at 6 weeks and 6 months. S100β cannot be reliably used to predict neurocognitive function.
on-pump; off-pump; emboli
054 THE ASSOCIATION BETWEEN SYSTEMIC INFLAMMATION, STATIN THERAPY, AND SAPHENOUS VEIN ENDOTHELIAL FUNCTION IN PATIENTS UNDERGOING CORONARY ARTERY BYPASS SURGERY
N. Melikian1, A. Momin1, S. Wheatcroft2, D. Grieve1, L. John3, A. El Gamel3, M. Marrinan3, J. Desai3, C. Driver4, R. Sherwood4, A. Shah1, M. Kearney1.1Cardiovascular Division, King’s College School of Medicine at Guy’s King’s College and St Thomas’ Hospitals, London, London, UK; 2Cardiology Department, King’s College Hospital, London, UK; 3Department of Cardiothoracic Surgery, King’s College Hospital, London, UK; 4Department of Clinical Biochemistry, King’s College Hospital, London, UK
Background: Systemic inflammation and endothelial dysfunction (ED) are independent predictors of future cardiovascular (CV) events. Statins, used to treat high cholesterol levels, improve ED, and reduce systemic inflammation. We investigated the association between C-reactive protein (CRP—a marker of systemic inflammation) and saphenous vein (SV) endothelial function in patients optimally treated with statins undergoing coronary artery bypass surgery.
Methods and Results: Seventy six patients with optimal LDL cholesterol levels (1.6 (SD 0.05) mmol/l) secondary to regular treatment with a minimum of simvastatin 40 mg were recruited. 26% had CRP levels in the “high risk” range (>3.0 mg/l) despite statin therapy. Acetylcholine (ACh) induced relaxation was assessed ex vivo in harvested SV rings. There was a negative linear correlation between ACh- induced SV relaxation and CRP (r = −0.30, p = 0.02), and waist circumference (r = −0.21, p = 0.03). In a multivariate regression model CRP (p = 0.02) was the only independent predictor of Ach induced venous relaxation (Panel A). In turn correlates of CRP were assessed. There was a correlation between CRP and angiographic estimates of coronary atherosclerotic burden (A-burden r = 0.46, p<0.0001), BMI (r = 0.26, p = 0.03), glucose (r = 0.31, p = 0.01), and waist circumference (r = 0.29, p = 0.01). Using multivariate analysis A-burden (p<0.0001) was the only independent predictor of CRP (Panel B).
Conclusion: In patients with coronary artery disease, treated with statins to achieve optimal LDL cholesterol levels, a sizable proportion had CRP levels within the “high risk” range. CRP was the only independent predictor of impaired SV endothelial function.
saphenous vein endothelial function; C-reactive protein; statins

Abstract 054 (A) Panel A; (B) Panel B.
055 CLINICAL OUTCOMES FOLLOWING COMPOSITE ARTERIAL CORONARY ARTERY BYPASS SURGERY: A SINGLE CENTRE EXPERIENCE
M. Naffati, D. Ramsdale, A. Alahmar, M. Pullan, B. Fabri.The Cardiothoracic Centre, Liverpool, Liverpool, UK
Introduction: Composite arterial coronary artery bypass graft surgery (CABG) is thought to have significant short and long term advantages over conventional CABG using saphenous veins. However, few data are available from the UK to support the efficacy of this surgical approach.
Aim: This study was designed to assess the clinical outcomes of a large cohort of patients who underwent CABG using an off-pump composite arterial grafting technique.
Methods: Between 01/01/00 and 31/12/03, all patients who underwent off-pump coronary surgery without aortic manipulation using composite grafting with the left internal mammary artery (LIMA) and radial artery (RA) were studied. Clinical and procedural data, in-hospital complications and clinical follow up information including details of any repeat angiography were documented.
Results: There were 862 patients. Mean (SD) age was 63 (9.1) years and 651 (76%) were male. Preoperatively, five (0.6%) patients were in angina class I, 211 (24.4%) class II, 625 (72.5%) class III, and 21 (2.4%) class IV (Canadian Cardiovascular Society). None had single vessel disease, 117 (13.6%) two vessel disease and 745 (86.4%) three vessel disease. One hundred and twenty one patients (14%) had two grafts and 741 (86%) three grafts for a mean graft rate 2.9 grafts per patient. The LIMA was anastomosed to the LAD in 852 (98.8%) and to first diagonal (DG1) in six (0.7%). The RIMA was anastomosed to the LAD in four (0.5%). The RA was grafted to DG1 in 98 (11.4%), obtuse marginal(s) in 486 (56.3%), distal circumflex in 35 (4.1%), and the right coronary artery (usually the posterior descending branch) in 612 patients (71%). In-hospital complications included Q-wave myocardial infarction in nine (1%), serious cardiac arrhythmias in four (0.3%), atrial fibrillation in 102 (11.8%), and focal neurological deficit in 1 (0.1%). Six patients (0.7%) died in hospital. The intensive care and in-hospital stay averaged 1 and 7 days respectively. After a mean follow up of 12 months, two (0.2%) patients were in angina class I, six (0.7%) class II, 2 (0.2%) class III, and 1 (0.1%) class IV; 826 (95.8%) were asymptomatic. During follow up, 11 patients (1.2%) underwent repeat coronary angiography for recurrent angina. The LIMA was patent in all patients. Six radial grafts were occluded. In four patients these were single grafts while the other two had one limb of a sequential graft occluded. Percutaneous coronary intervention was undertaken in six patients and five were treated medically. There was no requirement for repeat surgery.
Conclusion: CABG using composite arterial grafting is a safe technique resulting in effective relief of angina. Symptom recurrence is uncommon during short/medium term follow up. In the few patients with recurrent angina, loss of a RA graft or poor antegrade flow is seen in over half of those patients studied but the LIMA is invariably patent.
composite graft surgery; radial artery coronary artery bypass graft surgery; left internal mammary artery bypass graft surgery
056 THE EFFICACY OF SHORTENING CARDIOPLEGIC ARREST TIME DURING COMBINED CORONARY AND VALVULAR SURGERY
R. Ascione.Bristol Heart Institute, University of Bristol, Bristol, UK
Background: Combined valvular and coronary surgery remains a challenge with high in-hospital mortality and morbidity due to prolonged cardiopulmonary bypass (CPB) and cardioplegic arrest (CA) time. We set to shorten markedly the CA time and to assess any related clinical implications.
Methods: Twenty patients underwent on-pump beating heart coronary surgery prior induction of CA to treat the valvular disease during 2004 (hybrid group). They were matched (operation type, date, age, gender, ejection fraction, number of grafts, and operative priority) with other 20 patients undergoing conventional combined surgery (conventional group). Data were compared using methods for paired data and quantified using odds ratios.
Results: 80% of patients in each group underwent aortic valve replacement, 15% mitral valve surgery, and 5% both. Patient characteristics were similar between groups. There were neither deaths nor neurological events. Cross clamp times were significantly shorter in the hybrid group (median difference −32 minutes, p = 0.0004). There was no difference in CPB time. Fewer patients in the hybrid group experienced an MI, arrhythmia, or required pacing or inotropes for more than 12 hours postoperatively (odds ratio for these events 0.63 (95% CI 0.38 to 1.02, p = 0.11). 40% of patients in the hybrid group did not experience any major postoperative complication as compared to 20% in the conventional group. Ventilation times, blood loss, haemodynamics, lactate, ICU, and hospital stay were similar (p30.21). Transfusion requirements were reduced in the hybrid group (red cells: 55% v 80%).
Conclusion: The hybrid approach to combined coronary and valvular surgery led to a significantly shortened cardioplegic arrest time and fewer postoperative complications. A larger study is needed to explore the feasibility and outcomes further.
combined valvular and coronary surgery; cardioplegic arrest time; in-hospital outcome
057 POOR POSTOPERATIVE BLOOD GLUCOSE CONTROL INCREASES IN-HOSPITAL MORTALITY AND MORBIDITY FOLLOWING CARDIAC SURGERY
C. Rajakaruna, C. Rogers, G. Angelini, R. Ascione.Bristol Heart Institute, University of Bristol, Bristol, UK
Objective: To investigate the effect of postoperative blood glucose levels (BGL) on in-hospital clinical outcomes following cardiac surgery.
Methods: BGL was routinely measured at 1, 12, 36, and 60 hours postoperatively. Patients were grouped according to BGLs as: good (BG⩽11.0 mmol/l); moderate (BG>11.0 £13.9 mmol/l) and poor (BG⩾13.9 mmol/l). Logistical regression model was used to investigate the effect of BGLs on early outcome.
Results: 8344 patients operated on between April 1996 and March 2004 were classified as good (85.3%), moderate (10.5%), and poor (4.2%). Patients with poor BGL were more likely to be diabetics, and to undergo combined coronary and valve surgery or aortic procedures (all p<0.001). In-hospital mortality was 1.6%, 4.2%, and 8% in the good, moderate and poor groups respectively. Regardless of the diabetic status, patients with poor BGLs suffered more postoperative MI, pulmonary, neurological, renal, infective, and gastrointestinal complications (all p<0.001). Moderate and poor BGLs levels were both strong predictors of in-hospital death, postoperative MI, pulmonary complications, renal complications, and multisystem failure (all p<0.001). Diabetic status was associated with renal complications (p<0.01) but not with in-hospital mortality or any other morbidity.
Conclusion: Poor postoperative blood glucose level rather than diabetic status is associated with significantly higher in-hospital mortality and morbidity in patients undergoing cardiac surgery.
postoperative blood sugar control; in-hospital outcome; cardiac surgery
058 A PROSPECTIVE LONGITUDINAL EVALUATION OF THE BENEFITS OF EPICARDIAL LEAD PLACEMENT FOR CARDIAC RESYNCHRONISATION THERAPY
A. Patwala1, P. Woods2, J. Kendall1, D. Goldspink2, L. Tan3, A. Oo1, D. Wright1.1The Cardiothoracic Centre, Liverpool, UK; 2RISES, Liverpool John Moores University, Liverpool, UK; 3Academic Unit of Molecular Vascular Medicine, University of Leeds, LGI, Leeds, UK
Background: It is now widely accepted that cardiac resynchronisation therapy (CRT) leads to significant improvement in the morbidity and mortality in patients with severe heart failure and evidence of electromechanical dyssynchrony. However the endovascular placement of the left ventricular (LV) lead in the coronary sinus can be difficult. All the major trials have shown an 8–12% failure rate, for this group epicardial placement of the LV lead is one option however its effect on clinical outcomes has not yet been effectively assessed compared to successful endovascular implantation.
Methods: Seventeen patients in whom endovascular placement of the LV lead had failed were recruited. After giving written consent they underwent epicardial LV lead placement via a left lateral mini-thoracotomy. The patients were assessed pre, three months, and six months post epicardial placement. At each visit initially triplicate readings of resting cardiac output measurements were made using the equilibrium method of Collier. A modified Bruce protocol treadmill was then carried out to assess peak VO2 and peak cardiac output was measured at maximal exertion using the exponential method of Defares. After 24 hours’ rest a further maximal test was carried out with a further measurement of peak cardiac output. The resting and peak cardiac output readings were then averaged. Peak and resting cardiac power output (CPO) were calculated using the formulae: CPO = CO × Mean Arterial Pressure × 2.22×10−3. Cardiac reserve (CR) was calculated by subtracting Rest CPO from peak CPO. The results were compared to a control group who were age, sex, and peak VO2 matched and had received CRT via the endovascular route. A repeated measures ANOVA was used to look for improvements between the baseline and post tests. Paired t tests were used to look for differences between the control and epicardial group.
Results: At baseline there was no significant difference in any variables between the two groups. By three months both groups had shown significant improvements in NYHA class, exercise duration, peak CPO and CR. Peak VO2 was also significantly improved in the endovascular group at three months while in the epicardial group the improvement was only significant at six months. There were no statistically significant differences in measured variables between the two groups at any stage (see table, results shown as mean (SE)).
Abstract 058
Conclusion: Epicardial left ventricular lead placement is a viable option for patients in whom endovascular lead placement fails. The improvements seen in all measures at six months are very similar to those seen after endovascular implantation. Peak VO2 improvement does appear to be delayed in the epicardial group and this is likely to be due to the more invasive surgery and longer recovery time required, however reassuringly by six months the epicardial group have caught up in terms of improvement.
epicardial lead; cardiac resynchronisation therapy; peak cardiac power output
059 ENDOVASCULAR REPAIR OF TYPE B AORTIC DISSECTION WITH END-ORGAN DAMAGE IS FEASIBLE IN A DISTRICT GENERAL HOSPITAL SETTING WITH A MULTIDISCIPLINARY APPROACH, AND MAY BE LIFE SAVING
J. Boullin, D. Shepherd, L. Wijesinghe, W. Butcher, S. Parvin, M. Schuster-Bruce, R. Radvan.Royal Bournemouth Hospital, Bournemouth, UK
Background: Type B aortic dissection with end organ damage has an appalling mortality (50–87%). It has an operative mortality of 39% with conventional surgical repair. If end-organ damage exists, few cardiothoracic surgical centres in the UK offer a surgical solution for this condition. Although randomised controlled trial data are awaited, endovascular stent grafting appears to be a superior treatment with a published mortality of 16–20%.
Methods: Since 2000 we have evaluated all acute type B aortic dissections deemed to be inoperable by the local regional cardiothoracic surgical centre, for endovascular stent grafting. All patients had end organ damage. Eight patients underwent endovascular repair over five years (mean age 64 years, range 38–82, five male, three female). All patients received multislice CT with 2D, and 3D reconstruction, and TOE prior to intervention. Five patients had type B dissection, two with associated rupture. Two patients presented with class 4 penetrating thoracic ulcers and one had secondary aortic rupture. (A total of four patients had life threatening haemorrhage). One patient presented with recurrent dissection following incomplete surgical repair for a type B dissection two years previously, with spinal cord ischaemia. Four patients had lower limb ischaemia, and three had renal ischaemia. Endovascular stent graft repair was carried out by a multidisciplinary team (vascular surgeon, interventional radiologist, and cardiologist). Angiography was performed from the radial route, and device deployment from the femoral route (direct exposure), under general anaesthesia. Fluoroscopy and on-table TOE imaging was used to guide deployment from the left subclavian (occluding this vessel). The target for therapy was complete thrombosis of the false lumen. In a total of 11 procedures, 13 devices from three manufacturers were used, including one staged aortic reconstruction with five stents. There was one death (mortality 12.5%), due to device failure/mal-deployment. Two patients have undergone additional surgical carotid-subclavian bypass. In the seven patients in whom the procedure was successful (87.5%) the mean time from deployment to discharge was 12 days (range 7 to 21). All are still alive, active, and independent. Complete thrombosis of the false lumen has occurred in 71% (five patients) and almost complete thrombosis in the remainder.
Conclusions: (1) Our results compare favourably with a published mortality for this condition with both medical and surgical management, as well as with the current non-randomised data for endovascular stent grafting.(2) Endovascular stent grafting is a safe and potentially life saving technique in a district general hospital setting in patients with type B dissection and end organ damage. If successful, patients make a rapid recovery and return to independence.
aortic dissection; endovascular stenting; descending aorta
060 GENDER SPECIFIC REGULATION OF PHYSIOLOGICAL HYPERTROPHY IN MICE IN RESPONSE TO VOLUNTARY EXERCISE
J. de Bono1, D. Adlam1, D. Paterson2, K. Channon1.1Department of Cardiovascular Medicine, University of Oxford, Oxford, UK; 2Department of Physiology, University of Oxford, Oxford, UK
Introduction: Pathological cardiac hypertrophy occurs in response to multiple stimuli including aortic stenosis, hypertension and genetic disorders. It is associated with poor prognosis and increased cardiac events. In contrast physiological hypertrophy seen in elite athletes is not associated with adverse prognosis. There is a need to develop mouse models to further study the different molecular and genetic mechanisms underlying pathological and physiological hypertrophy. The majority of mouse models of physiological hypertrophy rely upon forced exercise regimes involving either swimming or treadmill running and have studied a single time point. The aversive stimuli used in these models may result in different physiological and molecular responses in comparison to voluntary exercise. We describe the development of cardiac hypertrophy in a new model of mouse voluntary wheel running.
Methods and Results: Ten week old inbred C57Bl/6 mice of both sexes were singly housed with either a fixed or freely rotating running track and sacrificed after three or six weeks of voluntary running. C57Bl/6 mice ran considerable distances with females running further than males (males 10.3 (SD 0.6) km/day, females 14.6 (SD 0.8) km/day in week 3, p<0.001). After three weeks of exercise there was a significant increase in left ventricle (LV) mass in both males (10.0%, 11 mg, p = 0.03) and females (17.4%, 15 mg, p<0.001) when compared with sedentary littermates. However after six weeks’ exercise, cardiac hypertrophy had almost completely resolved in male mice with a significant reduction in LV mass (107 (SD 3) mg) after six weeks in comparison with three weeks (117 (SD 3) mg, p = 0.04) despite continuous wheel running. Cardiac hypertrophy persisted in females even at six weeks (13.6%, 12 mg increase compared to sedentary controls, p = 0.003). Adjustment of LV weight for body length did not alter the results in either sex. However when adjusting LV mass for body weight, exercising male mice showed a significant increase in the ratio of LV mass: body weight at both three weeks (12.5% increase, p<0.001) and six weeks (9.5%, p = 0.003). This is despite no change in absolute LV mass at six weeks and is explained by a significant decrease in body weight in response to exercise (7%, 2.0 g at 6 weeks, p = 0.001). The data in females were unaffected by adjustment for body weight and there was no significant difference in body weight in response to exercise at either three or six weeks.
Conclusion: Physiological hypertrophy in response to voluntary wheel running is a transient gender specific phenomenon. Future studies of physiological hypertrophy should use both sexes and multiple time points to make valid comparisons. Care should be taken using LV mass:body weight ratio as a marker of cardiac hypertrophy as male mice show a significant decrease in body weight in response to exercise but female mice do not. This model will provide insight into the different molecular and genetic mechanisms underlying physiological and pathological hypertrophy.
cardiac hypertrophy; mouse models; gender differences

Abstract 060.
061 IDENTIFICATION AND FUNCTIONAL ANALYSIS OF CARDIAC TROPONIN I AS A NOVEL DISEASE GENE IN AUTOSOMAL DOMINANT FAMILIAL DILATED CARDIOMYOPATHY
S. Carballo, C. Redwood, P. Robinson, E. Blair, H. Watkins.Department of Cardiovascular Medicine, University of Oxford, Oxford, UK
Familial dilated cardiomyopathy (DCM) has a prevalence of 1:2500 and accounts for as much as 50% of idiopathic dilated cardiomyopathy in adults. Inheritance is usually autosomal dominant, often with incomplete penetrance. A causative mutation is identified in only 10–25% of affected individuals. Recently, mutations in genes coding for sarcomeric proteins have been shown to cause DCM. As part of a systematic study, DNA was obtained from 103 consecutive families with with cardiomyopathy (61 HCM, 26 DCM, and 16 mixed/complex phenotypes) and coding exons of the gene encoding cardiac troponin I (TNNI3) were screened by temperature modulated heteroduplex analysis. Exons with aberrant profiles were sequenced and variants confirmed by restriction digestion, segregation analysis, and study of normal controls. Here we report a novel TNNI3 missense mutation, Lys36Gln, which was identified in a 15 year old individual with severe DCM; echocardiographic LV ejection fraction 15–20%, LV end-systolic diameter 57 mm, and LV end-diastolic diameter 70 mm. Family history indicated autosomal dominant transmission and hence these findings potentially implicated TNNI3 as a novel disease-gene for autosomal dominant DCM; however, no surviving affected members were available to test for segregation of the mutation. Instead, functional analysis was carried out to determine whether the Lys36Gln variant is disease causing. The Ca2+ regulation of Actin-Tropomyosin-activated Myosin S-1 ATPase by wild-type and mutant troponin I was compared in an in vitro assay using reconstituted recombinant thin filament proteins. The mutant showed decreased maximum ATPase activity. The maximum ATPase rate reached with the Lys36Gln mutant troponin I was 138% of the actin-tropomyosin rate, compared with 200% obtained with the addition of wild type troponin. The filaments containing 100% Lys36Gln troponin I mutant also produced a decreased Ca2+ sensitivity of ATPase activation (ΔpCa50 −0.24). A 50:50 Lys36Gln/wild type mixture, representing the likely in vivo ratio, also decreased the Ca2+ sensitivity, albeit to a lesser degree (ΔpCa50 −0.15). The nature and extent of the in vitro functional effects of this mutant (decreased Ca2+ sensitivity and lower maximum ATPase activity) mirror closely those found in proven DCM mutations in other thin filament proteins. Because thin filament DCM mutants produce a consistent biophysical phenotype we can conclude that this novel variant, also, is disease causing. This is the first reported dominant DCM-causing mutation in TNNI3. As such it expands the spectrum of disease causing genes that lead to either HCM or DCM depending on the specific mutation.
familial dilated cardiomyopathy; troponin I; autosomal dominant
062 PHYSIOLOGICAL UPPER LIMITS OF LEFT ATRIAL DIAMETER IN HIGHLY TRAINED ADOLESCENT ATHLETES
S. Basavarajaiah1, J. Makan1, M. Wilson2, G. Jackson1, S. Sharma1.1University Hospital of Lewisham, Lewisham, UK; 2Olympic Medical Centre, London, UK
Background: The differentiation between physiological left ventricular hypertrophy (LVH) and hypertrophic cardiomyopathy (HCM) in a highly trained athlete can be challenging for even the most able cardiologists. The echocardiographic differentiation between physiological LVH and HCM is based on left ventricular cavity size and indices of diastolic function. A recent study in adult athletes has shown that left atrial diameter may be used as an additional parameter enabling differentiation between the two entities. There are no data on physiological upper limits of left atrial diameter in adolescent athletes, in whom deaths from HCM are highest.
Methods: Between 2002 and 2005, 1000 highly trained adolescent athletes (75% male; mean body surface area of 1.75 +/0.16 m2) participating in 14 sporting disciplines and 250 sedentary age, gender, and size matched controls underwent 2D echocardiography. Left atrial and ventricular dimensions were measured using conventional methods
Results: Adolescent athletes had a mean left atrial diameter of 31 +/4.8 mm (range 19–45 mm). Left atrial diameter in athletes was 6% greater than that in healthy controls. Based on upper limits derived from the control group, 120 (12%) athletes had a greater than predicted left atrial diameter. Of the 1000 athletes, 48 (4.8%) athletes had a left ventricular wall thickness resembling those observed in patients with morphologically mild HCM (range 11–14 mm). The left ventricular cavity size in the 48 athletes ranged from 52–60 mm. Indices of diastolic function were normal and as follows: - E wave 0.87 +/0.16 m/sec (range 0.6–1.8 m/sec), A wave 0.41 +/0.1 m/sec (range 0.2–0.9 m/sec), E/A ratio 2.25 +/0.7 (range 1.0–5.5). We considered all 48 athletes to have physiological LVH based on the absence of a family history of HCM and normal diastolic function. None of the 48 athletes with LVH had a left atrial diameter exceeding 45 mm.
Conclusion: Our observations suggest that in highly trained adolescent athletes, left atrial diameter is modestly increased compared with non-athletes; however a diameter >45 mm is exceedingly rare and may represent a useful index in differentiating physiological LVH from HCM in a trained adolescent athlete with LVH. This value is considerably less (5 mm; 11%) than that observed in adult athletes.1
1
left atrial diameter; hypertrophic cardiomyopathy; adolescent athletes
063 DERANGEMENT OF CARDIAC HIGH ENERGY PHOSPHATE METABOLISM IN PATIENTS WITH LEFT VENTRICULAR NON-COMPACTION AND PRESERVED EJECTION FRACTION
S. Petersen1, M. Scheuermann-Freestone1, L. Hudsmith1, J. Francis1, D. Tyler2, M. Robson1, R. Anderson3, H. Watkins1, S. Neubauer1.1John Radcliffe Hospital/Department of Cardiovascular Medicine/University of Oxford, Oxford, UK; 2Oxford Metabolism Research Group/Department of Physiology/University of Oxford, Oxford, UK; 3Institute of Child Health/Cardiac Unit/University College London, London, UK
Background: Left ventricular non-compaction (LVNC) is characterised by the presence of an extensive non-compacted layer of myocardium, which can lead to chronic cardiac failure. The non-compacted myocardium likely represents an embryological arrest of normal myocardial compaction, albeit that the pathophysiological mechanisms leading to cardiac failure remain unknown. One attractive mechanism which may underlie the progression into cardiac dysfunction may be altered metabolism of cardiac high energy phosphates, since similar changes have been described in patients with dilated or hypertrophic cardiomyopathy. If this was the case, there would be two clinical implications. Firstly, it would suggest treatment strategies aimed at improving myocardial energetics. Secondly, altered cardiac energetics may potentially serve to distinguish patients with non-compaction at low and high risk of developing complications, analogous to the situation in dilated cardiomyopathy. We aimed to investigate cardiac energy metabolism in a group of patients with preserved cardiac function in the setting of ventricular non-compaction.
Methods: We studied seven patients (5 male, mean age 39 (SD 13) years) with clear evidence of non-compaction, comparing them with seven age and sex matched controls (5 male, mean age 37 (SD 16) years). Left ventricular end-diastolic, end-systolic, stroke volumes, and ejection fraction (EF) and mass were determined using magnetic resonance (MR) imaging, and cardiac high energy phosphate metabolism (phosphocreatine to ATP ratios, PCr/ATP) was measured in the compacted basal anterior myocardium using 31Phosphorus-MR spectroscopy. The fitted amplitudes of the spectral peaks were individually corrected for blood contamination and saturation effects using T1 and contamination values from the literature.
Results: Patients with LVNC had preserved EF (68 (5) v 72 (4)%, p = 0.16) and no evidence of abnormalities of regional wall motion, but showed significantly increased end-diastolic (146 (33) v 116 (16) ml, p = 0.049) and end-systolic (46 (11) v 33 (8) ml, p = 0.019) volumes when compared to controls. The cardiac PCr/ATP ratio was significantly reduced by 19% in LVNC (1.81 (0.10) v 2.25 (0.36), p = 0.005). The figure shows typical 31P-magnetic resonance spectra of a healthy volunteer and a patient with non-compaction with a decrease of the ratio of PCr to ATP in the patient. There was no correlation between LV end-diastolic volumes and PCr/ATP ratio, suggesting that LV dilation was not responsible for the derangement of cardiac energetics.
Conclusions: The metabolism of cardiac high energy phosphate is deranged in patients with non-compaction and preserved ejection fractions. This is the first study to show such abnormal findings, suggesting that derangements in cardiac energetics may precede the development of cardiac dysfunction in non-compaction. Future long term follow up studies are needed to test whether the deranged metabolism has prognostic value.
left ventricular non-compaction; magnetic resonance spectroscopy; high energy phosphates

Abstract 063.
064 EVIDENCE FOR REDUCED TROPONIN I PHOSPHORYLATION AND ALTERED TROPONIN FUNCTION IN PATIENTS WITH HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
A. Jacques1, A. Messer1, V. Tsang2, W. McKenna2, S. Marston3.1Royal Brompton Hospital & National Heart & Lung Institute, London, UK; 2The Heart Hospital, London, UK; 3National Heart & Lung Institute, London, UK
Introduction: Hypertrophic obstructive cardiomyopathy (HOCM) has been shown to be caused by mutations in sarcomeric proteins, but how genotype ultimately causes phenotype remains unanswered. Here we propose that post-translational modifications in cardiac contractile proteins, independent of genotype may also contribute to the disease phenotype. We have investigated troponin, since this is the key regulatory contractile protein in the thin filament, inhibiting myocardial contraction at diastolic levels of calcium.
Methods: Troponin was isolated from five non-failing donor hearts and from five patients with HOCM after septal myectomy (mean septal wall thickness = 23.1 (SD 2.7) mm; mean left ventricular outflow tract gradient = 105.2 (SD 18.1) mmHg), using a human anti-Troponin I monoclonal affinity column. Phosphorylation levels of human cardiac Troponin I (TnI) and troponin T (TnT) were assayed in SDS-PAGE gels using Pro-Q diamond phosphoprotein stain normalised to total protein in each band. The same troponin samples were tested in thin filaments reconstituted with human cardiac tropomyosin and rabbit skeletal actin by in vitro motility assay.
Results: TnT from non-failing heart troponin contained 3.05 SD 0.2) molPi/mol and TnI contained 2.25 (SD 0.36) molPi/mol. In HOCM troponin the level of TnT phosphorylation was the same (3.11 (SD 0.42) molPi/mol) but the level of TnI phosphorylation was very low (0.11 (SD 0.15) molPi/mol, n = 5, p<0.001) with three of the five HOCM TnI samples showing no detectable phosphorylation. Comparison of thin filaments from non-failing and HOCM heart troponin in dual chamber motility cells demonstrated no difference in filament sliding speed at maximally activating Ca2+ concentrations and no change in Ca2+ sensitivity despite the highly significant difference in TnI phosphorylation levels. In view of this unexpected observation non-failing and HOCM troponin were dephosphorylated with acid phosphatase. This produced a marked increase in Ca2+ sensitivity and a decrease of 15% in filament sliding speed in non-failing compared to HOCM troponin.
Conclusion: HOCM muscle samples show both reduced troponin I phosphorylation and a new molecular phenotype for unphosphorylated troponin. This is unlikely to be a direct effect of HOCM causing mutations but could be a secondary effect of a mutation or a direct response to pressure overload.
hypertrophic cardiomyopathy; troponin; phosphorylation
065 LIMITATIONS OF STANDARD TRANSTHORACIC ECHOCARDIOGRAPHY TO ASSESS CARDIOVASCULAR CONSEQUENCES OF TRANSFUSIONAL IRON OVERLOAD IN THALASSAEMIA MAJOR
S. Nair1, M. Tanner2, R. Galanello3, D. Pennell2, J. Walker1.1University College Hospital, London, UK; 2Royal Brompton Hospital, London, UK; 3Hospital Microcittemi, Cagliari, Italy
Introduction: Patients with thalassaemia major are at risk of cardiomyopathy due to transfusional iron overload. Despite the introduction in the 1960s of desferrioxamine, a parenteral iron chelating agent which is the current standard treatment, the mortality remains 50% by the age of 35, with 70% being of cardiovascular origin. The annual incidence in this population of heart failure is approximately 7%. Cardiac MRI T2* assessment has emerged as a method for quantifying cardiac iron load. T2*>20 milliseconds (ms) = no significant myocardial loading; 12–20 ms = mild myocardial loading; 8–12 ms = moderate myocardial loading; <8 ms = severe myocardial loading. MRI has limited availability in countries of greatest need with high prevalence of thalassaemia major and hence there remains a reliance on standard echocardiographic techniques.
Aim: To investigate the relationship between cardiac iron levels and the prevalence of abnormalities on standard transthoracic echocardiography (TTE), in a discreet population of Sardinians with thalassaemia major undergoing regular blood transfusion and on desferrioxamine chelation.
Methods: 166 patients (mean age 29 years, range 18–41 years) underwent TTE and cardiac MRI T2* assessment to quantify cardiac iron load as part of screening criteria for inclusion in a trial investigating combination chelation regimes. All patients were on a regular blood transfusion programme and on desferrioxamine iron chelation.
Results: Twenty nine patients (17.4%) had left ventricular ejection fractions (LVEF) of <55% (from apical 4 chamber, single plane, Simpsons estimation). Of the 29, only 3 had normal cardiac iron assessments on MRI. Nine patients (5.4%) had left ventricular diastolic dimensions of greater than 5.6 cm. Of these nine patients four had significant cardiac iron loading. In three patients the enlarged left ventricular dimensions were associated with reduced left ventricular function. LA size was increased in 13 patients (7.8%) from cross sectional area in apical view. Only 72 patients (43.4%) had completely normal valve function. 28 patients (16.9%) had greater than trivial TR or MR with seven being more than mild. The majority of the 28 had cardiac iron present (22). Pulmonary artery pressures of greater then 25 mmHg occurred in 12 patients (7.2%) of which eight had cardiac iron loading.
Conclusions: Cardiac abnormalities on echocardiography are commonly present in this patient group particularly in those patients with significant cardiac iron loading. With the exception of reduced LVEF (positive predictive value 90% for iron) the other parameters analysed have poor ability in predicting current cardiac iron loading. Work is required to determine if more advanced echocardiography techniques including tissue Doppler analysis can identify patients with cardiac iron loading at an earlier phase prior to reduction in LVEF.
cardiac iron; LVEF; MRI T2*
066 OUTCOMES FOLLOWING IMPLANTABLE CARDIOVERTER-DEFIBRILLATOR THERAPY IN CHILDREN WITH HYPERTROPHIC CARDIOMYOPATHY
J. Kaski1, M. Tome Esteban2, M. Lowe2, S. Sporton1, P. Rees1, J. Deanfield1, W. McKenna2, P. Elliott2.1Great Ormond Street Hospital, London, UK; 2Great Ormond Street Hospital/The Heart Hospital UCLH, London, UK
Introduction: Some children with hypertrophic cardiomyopathy (HCM) are at an increased risk of sudden cardiac death (SCD). In adults with HCM, implantable cardioverter-defibrillators (ICD) are highly effective at preventing SCD. The experience with ICDs in children and adolescents is limited.
Methods: Between December 1993 and July 2005, 142 consecutively referred patients with HCM aged 16 years and younger were evaluated in a dedicated clinic. Patients underwent history and examination, electrocardiography, echocardiography, ambulatory electrocardiography, and cardiopulmonary exercise testing as part of a risk stratification protocol. Serial follow up data were collected at outpatient clinic visits and by communication with patients and their general practitioners. All patients who underwent ICD implantation during this period were included in this study.
Results: Nineteen patients underwent ICD implantation (mean age 13.7 (2.2) years); 14 as primary prophylaxis following identification of two or more clinical risk factors, four following a resuscitated cardiac arrest, and one following sustained polymorphic ventricular tachycardia. Median follow up time was 14.6 months (range 7.7 months to 11.6 years). All patients were alive at the end of the study period. Four patients (21.1%) received a total of 15 appropriate ICD therapies. Three patients in the secondary prevention group (60%), and one patient in the primary prevention group (7.1%) received appropriate discharges. The median time to first appropriate shock was 3.3 months (range 1.4 to 10 months). The annual appropriate discharge rate was 21.3%. Five year shock-free survival rate was 77.7% (95% confidence intervals 58.3 to 97.2) for the whole group, 92.9% (73.5 to 112.2) for the primary prevention group and 40% (−2.9 to 82.9) for the secondary prevention group. Three patients (15.8%) received inappropriate ICD therapies (n = 5). Device related complications included one postoperative haematoma, and one infective endocarditis.
Conclusions: Appropriate ICD discharge rates are higher in children with HCM than those reported in adults and inappropriate discharge rates are lower than previously reported in children. The ICD should be considered the treatment of choice for the prevention of SCD in this population.
hypertrophic cardiomyopathy; implantable cardioverter-defibrillator; sudden cardiac death
067 DIAGNOSTIC AND THERAPEUTIC UNCERTAINTIES IN ACUTE CORONARY SYNDROMES WITH LEFT BUNDLE BRANCH BLOCK: SHOULD REPERFUSION THERAPY BE GIVEN TO ALL?
D. Tomlinson, T. Betts, Y. Bashir.John Radcliffe Hospital, Oxford, UK
Background: Patients presenting with symptoms suggestive of AMI and a LBBB ECG pattern create a diagnostic dilemma. Pharmacological reperfusion therapy (RT) has been demonstrated to provide the greatest absolute mortality reduction in such cases and current ACC/AHA guidelines recommend its administration as a priority. However, when the clinical diagnosis of AMI is in doubt, concern over potential bleeding complications may result in this treatment being inappropriately withheld.
Methods: Retrospective analysis of all consecutive patients admitted to this institution with symptoms suggestive of AMI and LBBB from April 2003–05. Exclusion criteria were: “silent” AMI, contraindication to RT, and late presentation. AMI was diagnosed using a laboratory troponin I assay from blood drawn at least 12 hours after the onset of symptoms. Patients were stratified into three groups according to troponin I concentration. Those given RT were compared with their non-reperfused counterparts to identify factors that may have influenced decision making.
Results: LBBB was the presenting ECG in 67 patients. Of these, RT was administered to 24.
Conclusions: No clinical parameter measured accurately predicted AMI in patients with LBBB. In a significantly greater proportion of patients administered RT therapy, AMI was excluded by subsequent biochemical analysis. This may be associated with an increase in late mortality. Further studies in this area are required to more accurately identify patients with LBBB and AMI.
left bundle branch block; acute myocardial infarction; guidelines

Abstract 067 figure 1.

Abstract 067 figure 2.
068 MANAGING ACUTE CORONARY SYNDROMES IN A DISTRICT GENERAL HOSPITAL WITH INTERVENTIONAL FACILITIES: A FUTURE MODEL OF CARE?
J. Martins, L. Tapp, D. Connolly, R. Davis, P. Cadigan, R. Ahmad.Sandwell and West Birmingham Hospitals NHS Trust, Birmingham, UK
Background: The majority of patients with an acute coronary syndrome (ACS) present to a district general hospital (DGH). Recent clinical trials have demonstrated the superiority of an early invasive strategy over a conservative approach to the management of patients with high risk ACS. In these trials coronary angiography was performed 2–7 days after hospitalisation. However, in the UK, many patients presenting to a DGH with a high risk syndrome often wait up to three weeks in hospital before transfer to a tertiary centre for potential revascularisation.
Aims: To investigate the management of ACS patients presenting to a DGH with onsite interventional facilities—specifically to evaluate the use of angiography and percutaneous coronary intervention (PCI) in high risk patients.
Methods: A four month prospective audit was carried out on all consecutive patients presenting with a suspected ACS to Sandwell General Hospital, West Bromwich, West Midlands, a DGH serving a population of 300 000. The hospital has four Consultant Cardiologists, two of which undertake coronary intervention. Baseline characteristics, initial pharmacological management, Thrombolysis In Myocardial Infarction (TIMI) risk score, use of angiography, length of hospital stay, and mortality were audited.
Results: From November 2003 to February 2004 there were 239 admissions with ACS, 46 with ST elevation myocardial infarction (STEMI) and 193 with non ST-elevation ACS (NSTE-ACS). The mean age was 62.3 years (range 22–99), 59% were male and 37% had diabetes mellitus. For NSTE–ACS, 97 (50%) patients were stratified as low risk and 96 (50%) as high risk, based on the ECG, Troponin I and TIMI score. In the high risk group 73 patients (76%) underwent coronary angiography. The median wait (IQR) for angiography was 2 days (1,4); 40 patients had PCI, nine were referred for coronary artery bypass grafting, and 23 were treated medically. For STEMI patients, 32 (70%) underwent angiography, of which 28 had PCI. The median time to intervention was three days. The median length of hospital stay for all ACS patients was three days, for NSTE-ACS five days and for STEMI six days. In-hospital mortality was 4.6% (11 patients).
Conclusion: These data demonstrate that a DGH with interventional facilities delivers optimal, cost effective management for patients presenting with an ACS. Lengthy in-hospital stays were avoided, and the waiting times for angiography and coronary revascularisation replicated those in clinical trials, unlike the current service provision for the majority of ACS patients presenting to a DGH. The mortality rate was low, and compares very favourably to those quoted in intervention trials and registries. We believe that this model of care for ACS patients should be expanded nationally, to allow the best possible evidence based care to be delivered promptly to the local population.
acute coronary syndrome; district general hospital; percutaneous coronary intervention
069 IMPACT OF PARAMEDIC DELIVERED PREHOSPITAL THROMBOLYSIS IN DORSET
P. Foley1, S. Winterton2, J. Radvan3, I. Simpson1, A. McLeod4.1Wessex Cardiac Centre, Southampton, UK; 2Dorset County Hospital, Dorchester, UK; 3Royal Bournemouth Hospital, Bournemouth, UK; 4Poole General Hospital, Poole, UK
Introduction: Dorset combines both rural and metropolitan areas and has a population of 700 000. In view of the long distances from hospital, prehospital thrombolyis has been implemented. This programme is currently the second largest in the UK. We studied the impact of prehospital thrombolysis in Dorset.
Methods: Data were prospectively collected on patients admitted with acute ST elevation myocardial infarction (STEMI) to the Dorset Hospitals (Poole General Hospital, Royal Bournemouth Hospital and Dorset County Hospital) over a three year period (2003–05) using the Myocardial Infarction National Audit Project definitions. Thrombolysis was delivered by Paramedics (group P) or in hospital (group H). The primary outcomes assessed were in hospital mortality and length of stay. Additional data collected was the peak creatine kinase (CK) level, time from ambulance arrival to hospital arrival, and patients requiring coronary angiography as an inpatient.
Results: 923 patients were thrombolysed for STEMI and admitted to the Dorset Hospitals. Only three patients underwent primary percutaneous coronary intervention and are not included in this analysis. 96 (10%) patients were in group P compared with 827 (90%) in group H. There was no significant difference in the in hospital mortality between the group P (6.3%) compared with group H (10.4%). Data were missing for mortality in 69 patients in group H. There was no difference in the mean length of stay between group P (10 (SD 7) days, n 88) compared with group H (10 (SD 7) days, n = 177, p = NS). The mean peak CK level was similar compared with group P (1486 U/l) compared with group H (1397 U/l, p = NS). Mean travelling time to hospital was similar in group P (39 (SD 15) minutes, n = 87) compared with group H (37±11, n = 641, p = NS). Overall the mean travelling time to hospital for both groups was 37±7 minutes and 5% of patients took over one hour to reach hospital after ambulance attendance. Significantly more patients underwent coronary angiography in group P (58%) compared with group H (28%, p<0.001).
Conclusions: Ten per cent of patients in Dorset with Acute STEMI received out of hospital thrombolysis delivered by paramedics. These patients were thrombolysed earlier and there was a trend to lower mortality. On average, 37 minutes of travelling time delay may be avoided if paramedics deliver thrombolysis and in 5% this may be reduced by over an hour. There was no evidence that paramedic delivered thrombolysis delayed arrival at hospital. The difference between the coronary angiography rates is unexplained.
prehospital care; acute myocardial infarction; thrombolysis
070 IMPACT OF EARLY DIABETIC TREATMENT ON MORTALITY OF HYPERGLYCAEMIC PATIENTS PRESENTING WITH ACUTE CORONARY SYNDROMES
J. Birkhead, C. Weston, L. Walker.National Audit of Myocardial Infarction, London, UK
Introduction: Patients not known to be diabetic who are hyperglycaemic on presentation with an acute coronary syndrome (ACS) have a poorer prognosis that those who are normoglycaemic. The impact of immediate diabetic treatment is not known. In an observational study we examined the impact of treatment on 7 day and 30 day mortality for patients with an admission glucose ⩾11 mmol, who were either not previously known to be diabetic or had previously been treated for diabetes by dietary means only.
Methods: An observational study of early mortality outcome for 1719 patients (784 ST elevation infarction) entered into the MINAP database in 2003–05 with a troponin positive acute coronary syndrome and who were either not previously known to be diabetic (n = 1453) or had recognised diabetes controlled by diet (n = 266). We examined outcome in relation to diabetic treatment received during hospital stay and after discharge for patients for whom treatment status was known and who had an admission blood glucose ⩾11.0 mmol.
Findings: Of 1719 patients with an admission glucose ⩾11 mmol, 1027 (59.6%) were given treatment for probable diabetes, 838/1719 (48.7%) insulin, and 188 (10.9%) oral medication, while the rest, 693 (40.4%) received no treatment. Treatment after discharge was inconsistent; only 272 (32.4%) continued any insulin, 249 (29.6%) were transferred to oral medication and the rest had no diabetic treatment. When patients receiving any treatment, either insulin or oral medication, in hospital and continuing after discharge were compared with those receiving none, crude mortality was; 7 days (treated first) 11.5% v 14.8%, 30 days 17.3% v 20.1%. Using multivariate analysis, adjusting for age, gender, admission glucose, and comorbidity, the odds ratio of death at 7 days for those having no treatment (treated group = 1) was 1.49 (95% CI 1.08 to 2.05), p = 0.014, and at 30 days 1.21 (0.92 to 1.6), p = 0.17.
Conclusion: Treatment with diabetic medication was associated with a lower early mortality for patients with ACS presenting with blood glucose >11. A trend towards benefit persisted at 30 days although this was no longer significant. Interpretation. Patients having ACS presenting with glucose >11 mmol are likely to be diabetic. Evidence of the early benefit of treatment presented here suggests that all patients presenting with blood glucose >11 mmol should receive immediate treatment.
hyperglycaemia; diabetic treatment; acute coronary syndrome
071 IMPROVEMENTS TO INTERHOSPITAL TRANSFER TIMES FOR PATIENTS WITH ACUTE CORONARY SYNDROMES IN THE UNITED KINGDOM. RESULTS FROM THE NHS HEART IMPROVEMENT PROGRAMME NATIONAL AUDIT
A. Bakhai1, K. Redfern2, S. Machin2, M. Dancy2, R. Levy3, S. Livesey4, S. Hall2, R. Boyle2, R. Murray5.1Barnet & CHase Farm NHS Trust, London, UK; 2NHS Heart Improvement Programme, Leicester, UK; 3South Manchester University Hospital, Manchester, UK; 4Southampton University Hospitals NHS Trust, Southampton, UK; 5Heart of England NHS Foundation Trust, Birmingham, UK
Background: The majority of UK district general hospitals do not have facilities for coronary interventions. Patients admitted with acute coronary syndromes (ACS) may incur delay before they can be transferred to a centre with appropriate facilities.
Methods: Data sent to the HIP were analysed from 193 and 136 hospitals in March 04 and November 05 respectively on patients pending or undergoing interhospital transfer (IHT) as part of a national survey. Reasons for transfer, age, gender, and various dates were collected to ascertain duration of stay prior to transfer.
Results: See table.
Abstract 071
Conclusion: Patients requiring IHT from district general hospitals incur substantial delays prior to being referred for transfer and waiting transfer. While national investment in coordinated referral pathways and more invasive facilities has led to substantial reductions in time to transfer, efforts now need to be directed to earlier assessment and referral of appropriate patients.
acute coronary syndromes; interhospital transfer; economics
072 CLINICAL AND BIOCHEMICAL PREDICTORS OF SIGNIFICANT CORONARY ARTERY DISEASE AND NEED FOR REVASCULARISATION IN PATIENTS WITH UNSTABLE CORONARY SYNDROMES: A REAL WORLD PERSPECTIVE
R. Smith, A. Asherson, M. Al-Obaidi, M. Al-Bustami, A. Mitchell, C. Ilsley, M. Mason.Harefield Hospital, Middlesex, UK
Background: Current guidelines suggest that an early invasive strategy should be employed in patients with cardiac troponin positive, non-ST segment elevation unstable coronary syndromes (UCS). There is doubt, however, whether this strategy translates to improved overall mortality compared to less invasive approaches. In addition, adherence to these guidelines in “real world” settings is not always practical.
Methods: We studied 459 consecutive UCS transfers to a tertiary centre between January 2001 and January 2002. We recorded admission troponin levels, dynamic ECG changes (ECG), exercise tolerance testing (ETT) results, previous cardiac history (hCAD), diabetes mellitus, renal function, duration of symptoms, angiographic findings, and subsequent revascularisation. After a mean follow up of 41.9 (SD 9) months, all recorded deaths (n = 34, 7%) were verified by the United Kingdom Office for National Statistics.
Results: Mean age was 62.6 (SD 10.5) years, 325 male. A total of 385 patients (84%) had significant coronary disease (lesion of ⩾70%, CAD) and 311 received revascularisation (68%). Univariate predictors of CAD were positive troponin (p<0.001), dynamic ECG changes (p = 0.001), positive ETT (p = 0.002), and male sex (p = 0.01). Multivariate logistic regression analysis revealed only ECG changes and positive ETT to be predictive (p<0.05); troponin was not (p = 0.35). Univariate predictors of revascularisation were positive ETT, troponin, normal renal function, younger age and absence of hCAD (p<0.05). Only younger age was predictive by logistic regression (p = 0.006). Both the sensitivity and specificity for troponin prediction of CAD (LR 1.8) and revascularisation (LR 1.3) were less than 70%. Increasing age, hCAD, and renal impairment (all p<0.01), but not troponin, were predictive of three-year mortality by multivariate logistic regression analysis.
Conclusion: This study suggests that risk stratification of UCS patients should not rely on troponin level alone. Rather, consideration should be given to multiple other factors including presenting ECG, ETT, and age at presentation. This supports the construction of algorithms incorporating these factors to select patients at highest priority for invasive investigation.
unstable coronary syndromes; troponin; risk stratification
073 A RANDOMISED STUDY TO EVALUATE THE IMPACT OF AN EDUCATION PROGRAMME ON USE OF EVIDENCE BASED TREATMENTS IN PATIENTS WITH NON-ST ELEVATION ACUTE CORONARY SYNDROMES: PROMIS UK
J. Booth1, N. Delahunty1, P. Newlands2, F. Nugara1, A. Bakhai3, M. Khan4, K. Fox5, J. Adgey6, A. Taneja7, U. Mallick8, M. Flather1 on behalf of PROMIS UK1Royal Brompton & Harefield NHS Trust, London, UK; 2Royal Brompton & Harefield NHS Trust, London, UK; 3Barnet General Hospital, London, UK; 4St Thomas & Guys NHS Trust, London, UK; 5Royal Infirmary, Edinburgh, UK; 6Royal Victoria Hospital, Belfast, UK; 7The Heart Hospital, London, UK; 8Royal Free Hospital, London, UK
Introduction: Improving the quality of care, and provision of cost effective evidence based treatments (EBT), is a priority. To date there has been no formal randomised study of the effect on quality of care of a structured education programme in acute coronary syndromes (ACS). We evaluated if an education programme delivered to health care professionals could improve the use of EBT.
Method: All UK acute care trusts were invited and those hospitals that agreed to participate and were able to obtain all the necessary approvals for the study were allocated to a structured education programme (education sessions, copies of ESC guidelines, and a simple care pathway) or a control group. The control group received no additional educational input. A cluster randomised method was used. Hospitals were stratified for availability of PCI and requested to enrol 30 consecutive patients. The study had MREC approval and patients gave written informed consent. Patients were eligible if they were admitted with non-ST elevation ACS. Patients were followed up to six months. The primary outcome was a comparison of EBT use: aspirin, clopidogrel, heparin, beta-blocker, and statin (maximum score per patient = 5). Secondary outcomes included use of angiography, coronary revascularisation, risk stratification, and lifestyle modification.
Results: A total of 501 patients were enrolled from 20 centres in the control group and 508 patients were enrolled from 18 centres in the education group. Baseline characteristics were similar in both groups, mean age was 65 years, 71% were male and 16% were diabetics. Median time from pain onset to presentation was three hours. About 44% of patients were admitted to CCU. An MI associated with admission symptoms occurred in 54% control group versus 49% education group. Rates of use of aspirin, clopidogrel, heparin, beta-blocker, and statins were (control v education) 85 and 90%, 69 and 77%, 93 and 97%, 75 and 80%, and 93 and 97% respectively. The mean scores of hospital EBT were 4.14 control group versus 4.38 education group, difference 0.24 (95% CI 0.03 to 0.45), p = 0.028. At six months the mean EBT (minus heparin) score was 2.89 control group versus 3.18 education group, difference 0.29 (95% CI 0.03 to 0.55), p = 0.028. In-hospital rates of angiography were 33% in the control group and 34% in the education group patients, and PCI was 13 and 11% respectively.
Conclusion: Patients participating in PROMIS appeared to represent a “well treated” group with EBT. In spite of this, a simple education programme provided measurable improvements in the use of EBT in-hospital and at six months. These findings may have greater impact in hospitals where the standard of care is lower, and should help to stimulate more systematic education, training, and audit for ACS management.
acute coronary syndrome; evidence based treatments; education programme
074 NON-UNIFORMITY OF REGIONAL LEFT VENTRICULAR MYOCARDIAL DEFORMATION AND GEOMETRY IN HYPERTENSION
A. Baltabaeva, M. Marciniak, B. Bijnens, E. Visagie, G. MacGregor, G. Sutherland.St George’s Hospital, London, UK
Background: Cardiovascular risks in hypertension (HTN) can be identified by distinct patterns of left ventricular (LV) remodeling. However they do not reflect the complexity of the regional reorganisation of the LV architecture in response to pressure overload in essential HTN. The sigmoid septum, known to develop in some extend with age, is particularly inclined to progress in HTN and its development seems to be reduced by effective blood pressure (BP) control. The presence of localised geometrical changes in the LV suggests the presence of alterations in regional LV function and deformation. Studying these changes could offer a possibility for the early identification of structural and functional changes related to increased afterload.
Objectives: This study was performed to examine regional left ventricular geometry and systolic performance in previously untreated HTN patients by use of echocardigraphic strain/strain rate (S/SR) derived from Doppler myocardial imaging (DMI).
Methods: Seventy five HTNs (BP 150/92 mmHg) with conventional parameters of LV systolic function and LV mass within normal limits were compared to data obtained from 35 age matched normotensives (NTN, BP 113/71 mmHg). All had 2D wall thickness measurements and DMI data obtained from three segments for four LV walls with subsequent S/SR analysis of longitudinal LV wall deformation (LD). The LD was compared to office and ambulatory BP.
Results: The observed regional geometrical changes and LD abnormalities in HTN were not uniform. Despite significant increase in wall thickness in all segments in HTN patients, there was a more prominent basal septal hypertrophy (12.1 v 8.2 mm, p<0.0001). In HTN, when compared to age matched normals, regional deformation was significantly reduced in this segment when measured by total strain (p<0.0001) and peak systolic S/SR (PSS/PSSR) (p<0.0001). However, the apical segments of the septum, had increased S/SR (p<0.02) when compared to normals. In the lateral wall there was an increase in the contribution of the basal segments to systolic longitudinal shortening as demonstrated by an increase in SR (p<0.002), However, S did not increase significantly in this segment. The geometrical remodelling and the increased BP in the mostly affected basal septal segment showed a strong correlation with the reduction in regional deformation. The basal septal PSS correlated both with mean arterial pressure (r = 0.48; p<0.0001) and the basal septal wall thickness (r = 0.38, p<0.0002).
Conclusions: (1) Regionally differing geometrical remodelling occurs in the early stage of HTN, prior to the development of significant LV hypertrophy. (2) S/SR are highly sensitive markers for detecting early changes in regional deformation in HTN hearts. (3) The basal LV septum is likely to play an important role in the pathological process showing a clear reduction in regional peak systolic strain and strain rate, which is partially compensated by inverse changes in other regions of the LV.
hypertension; LV remodelling; echocardiographic strain rate imaging

Abstract 074.
075 THE ROLE OF WAVE REFLECTION IN THE PATHOPHYSIOLOGY OF HYPERTENSION: ASSESSED USING NON-INVASIVE WAVE INTENSITY ANALYSIS
C. Manisty, J. Davies, Z. Whinnett, D. Francis, A. Zambanini, S. Cunningham, S. Thom, A. Hughes, J. Mayet.International Centre for Circulatory Health, Imperial College and St Marys Hospital, London, UK
Introduction: Vascular stiffening with age is said to lead to increased and earlier wave reflection, with wave reflection peaking in systole rather than diastole and therefore impeding cardiac function. Currently, augmentation index is used as a marker of wave reflection, however there is no direct measurement of wave reflection. Wave intensity analysis (WIA) analyses vascular haemodynamics in terms of travelling energy waves and allows us to identify the direction, type and amplitude of individual waves and therefore to recognise the reflection wave (fig 1).

Abstract 075, figure 1.
We investigated the following hypotheses: (1) The effect of age and blood pressure on wave reflection (a) timing and (b) magnitude in normal subjects using WIA; (2) The effect of different antihypertensive medications on wave reflection; (3) Does wave reflection move from diastole to systole with increasing age and blood pressure?
Methods: We measured wave intensity in two subject groups: (1) normal subjects (n = 51 mean age 47 (SD 17) years). To ensure a “true” normal group, subjects with hypertension were excluded; (2) patients with treated hypertension (n = 255 mean age 64 (SD 8) years) recruited from a substudy of the ASCOT trial.
Results: In normal subjects, both carotid intimal medial thickness (r = 0.61, p<0.0001), and wavespeed (r = 0.23, p = 0.05) increased with age, indicating that arterial stiffness rises with age irrespective of blood pressure. The arrival of the reflected wave from both the head (r = −0.38, p = 0.001) and the body (r = −0.42, p = 0.002) were inversely correlated with age in the normal group (fig 2).
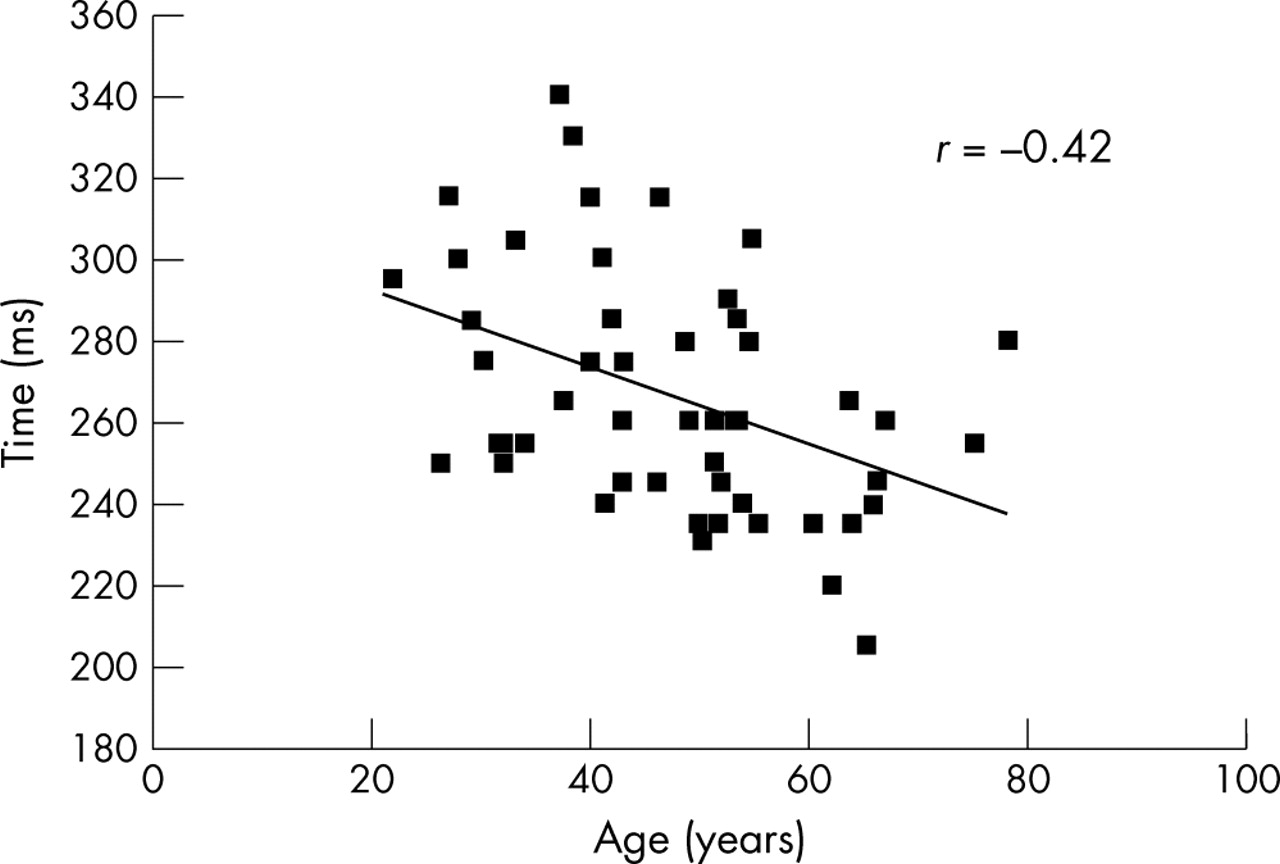
Abstract 075, figure 2.
The magnitude of wave reflection was unrelated to age (p = 0.22). In the treated hypertensive subjects, those randomised to amlodipine+/−perindopril had lower blood pressures than the bendrofluazide+/−atenolol group and a lower reflection coefficient (20 v 23% p = 0.05), but there after correction for heart rate there was no significant difference in reflection wave timing (p = 0.15). The end of systole ends can be identified using WIA by the peak of the expansion wave during protodiastole. In all subjects, irrespective of age, reflection wave intensity peaked prior to the expansion wave.
Conclusions: We have demonstrated that wave reflection occurs earlier in the cardiac cycle with age, but that it is always confined to systole. In normal subjects there is no increase in magnitude of wave reflection with age, and therefore there must be other mechanisms involved in systolic pressure augmentation with ageing. Treatment with amlodipine+/−perindopril reduces wave reflection to a greater extent than bendroflumethiazide+/−atenolol. Reduction in wave reflection may contribute to the superior effects amlodipine+/−perindopril on CVD mortality reported in the ASCOT study.
wave reflection; wave intensity analysis; hypertension
076 CHANGES IN REGIONAL LEFT ATRIAL DEFORMATION IN HYPERTENSIVE PATIENTS
A. Baltabaeva1, M. Marciniak1, B. Bijnens2, E. Visagie1, G. MacGregor1, G. Sutherland2.1St George’s, University of London, London, UK; 2St George’s Hospital, London, UK
Background: As a result of raised left ventricular (LV) filling pressure, hypertension (HTN) can result in left atrial (LA) dysfunction due to chamber dilation and increased peak wall tension during the LA active contraction. This makes the atrium prone to develop acute and chronic atrial fibrillation and other complications. Currently there are no clinical methods to assess LA contractile function. Strain (S) and strain rate (SR) imaging (S/SRI) can be use for the assessment of LA regional deformation.
Objectives: To assess LA regional deformation during the active LV filling in hypertensive patients.
Methods: In 75 HTN patients and 35 age matched normotensive (NTN) subjects (mean age 49 (SD 1.4) v 45.5 (SD 2.19) years old, NS) standard echocardiography was performed and S/SR were measured in the lateral LA wall in a four chamber view during late diastole. LA S was calculated as the difference between maximum and minimum S during late diastole. In all subjects, office and 24 hour blood pressure (BP) were measured.
Results: HNT patients had a significantly increased office (150/92 (1.2/1) v 113/71 (2.7/1.2) mmHg, p<0.0001) and 24 hour ambulatory BP (140/86 (1.2/1.2) v 118/72 (1.6/0.9) mmHg, p<0.0001). In the HTN group there was a significant increase in atrial S (−23.7 (1.3) v −12.47 (1.5)%, p<0.0001) and SR (−4.95 (0.2) v −2.7 (0.2) 1/s, p<0.0001) compared to NTN. BP correlated significantly with atrial S (r = 0.35, p<0.0005) and SR (r = 0.43, p<0.0001) during late LV filling.
Conclusions: LA deformation during late diastole was significantly increased in hypertension. The degree of changes in active LA deformation relates to the degree of elevation in BP in HTN.
hypertension; left atrial function; strain rate echocardiography

Abstract 076.
077 ETHNICITY AND LEFT VENTRICULAR DIASTOLIC FUNCTION IN HYPERTENSION: AN ASCOT SUBSTUDY
A. Sharp1, S. Thom1, D. Francis1, A. Hughes1, A. Stanton2, A. Zambanini1, E. O’Brien2, S. Lyons2, S. Byrd1, N. Poulter1, P. Sever1, J. Mayet1.1International Centre for Circulatory Health, St Mary’s Hospital and Imperial College, London, UK; 2Department of Clinical Pharmacology, Royal College of Surgeons of Ireland, Dublin, Ireland
Background: African-Caribbeans are known to have a higher prevalence of heart failure than White Europeans, although it is unclear whether this is a result of the increased prevalence of known cardiovascular risk factors (such as degree of hypertension, diabetes, and left ventricular hypertrophy). Tissue Doppler echocardiography (TDE) now allows more accurate quantification of diastolic function, which is recognised as an important factor in the development of heart failure. We investigated whether diastolic function is abnormal in hypertensive individuals of African-Caribbean origin compared with Europeans, and whether any differences could be explained by known risk factors.
Methods: Participants in the Hypertension Associated Cardiovascular Disease (HACVD) substudy of the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT) comprising 878 subjects with hypertension, but no clinical evidence of heart failure, were studied. Left ventricular structure and function were measured using conventional echocardiography and TDE. Diastolic function was assessed using the transmitral Doppler early filling wave (E), the tissue Doppler early diastolic velocity (E′) and the ratio between them (E/E′).
Results: In African-Caribbeans, E′ was significantly reduced (6.5 v 7.5 cm/s, p = 0.002) and E/E′ was significantly increased (10.5 v 8.6, p<0.0001). Despite adjusting for known risk factors such as age, sex, blood pressure, left ventricular hypertrophy and diabetes in a multivariate model, the effect of African-Caribbean ethnicity persisted (E′ lower by 1.00 cm/s in African-Caribbeans, p = 0.002; E/E′ increased by 1.87 in African-Caribbeans, p<0.0001 after adjustment for the above variables). The effect of ethnicity on diastolic function was greater than those of a 30 year age increase.
Conclusion: Diastolic function is significantly worse in hypertensive subjects of African-Caribbean origin than Europeans. This appears due to decreased relaxation during diastole and increased filling pressures. The ethnic difference in diastolic performance is not explained by known risk factors, and may account for the increased prevalence of heart failure in the African-Caribbean population.
hypertension; ethnicity; diastolic function

Abstract 077.
078 THE ABILITY OF TISSUE DOPPLER ECHOCARDIOGRAPHY TO PREDICT FUTURE CARDIOVASCULAR EVENTS IN A HYPERTENSIVE POPULATION: AN ASCOT SUBSTUDY
A. Sharp1, S. Thom1, D. Francis1, A. Hughes1, A. Stanton2, A. Zambanini1, E. O’Brien2, S. Lyons2, C. Lang1, S. Byrd1, N. Poulter1, P. Sever1, J. Mayet1.1International Centre for Circulatory Health, St Mary’s Hospital and Imperial College, London, UK; 2Department of Clinical Pharmacology, Royal College of Surgeons of Ireland, Dublin, Ireland
Background: Hypertension is a leading cause of cardiovascular disease (CVD) and it would be valuable to further risk stratify hypertensive patients as accurately as possible. This study assessed whether tissue Doppler echocardiography has prognostic value in predicting CVD in patients with well controlled hypertension.
Methods: 488 patients who were part of the Hypertension Associated Cardiovascular Disease (HACVD) substudy of the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT) underwent detailed cardiovascular assessment including standard and tissue Doppler echocardiography (TDE). Patients were hypertensive with at least three other cardiovascular risk factors with no clinical evidence of ischaemic heart disease or heart failure. Over a mean follow up period of 2.6 years 87 subjects experienced a cardiovascular event, defined as cardiovascular death, non-fatal myocardial infarction (MI), fatal coronary heart disease, silent MI, non-fatal or fatal stroke, transient ischaemic attack (TIA), revascularisation procedures, peripheral arterial disease, diabetes mellitus. Data were analysed using a Cox proportional hazards model to estimate time to CVD event. Comparisons of survival curves between categories were made by the log rank test.
Results: Baseline TDE indices were the only independent predictor of first events, this was unaffected by adjustment for age, sex, study drug, diabetes, smoking, heart rate systolic blood pressure body mass index, total or HDL cholesterol on multivariate analysis. For each unit increment in Lateral E/E′, the hazard ratio (HR) for events was 1.12 (95% CI 1.03 to 1.20, p = 0.01) in the unadjusted model, or after adjustment for covariates HR 1.10 (95% CI 1.01 to 1.20; p = 0.028). Left ventricular mass index, ejection fraction, left atrial size, transmitral E/A ratio, or TDE E′ alone did not significantly predict events. When tertile analysis was performed, those in the uppermost tertile for E/E′, indicating those with highest left atrial filling pressures (Lat E/E′ ⩾7.30), were at greater risk than those in the middle tertile (Lat E/E′ 5.78–7.30), who in turn were at greater risk than those in the lowest tertile (Lat E/E′<5.78); log rank testing, p = 0.035. For those subjects in the uppermost tertile of E/E′ values, risk of subsequent first event was double that of those in the lowest and middle tertile combined (log rank testing, p = 0.012).
Conclusion: The ratio of early diastolic transmitral flow velocity (E) to early mitral annular velocity (E′) is a strong predictor of future events in a hypertensive population. E/E′ was a more sensitive predictor than accepted cardiovascular risk indicators such as raised LVMI, ejection fraction and left atrial size. E/E′ is an indicator of left atrial filling pressures and hence the severity of diastolic dysfunction, and is a simple screening tool for identifying at-risk patients amongst a treated hypertensive population.
hypertension; tissue Doppler; diastolic

Abstract 078.
079 CORONARY BLOOD FLOW IS NOT AUGMENTED BY AORTIC WAVE REFLECTION: AN INVASIVE ASSESSMENT USING WAVE INTENSITY ANALYSIS
J. Davies1, Z. Whinnett1, D. Francis1, C. Manisty1, K. Willson2, R. Foale1, I. Malik1, A. Hughes1, K. Parker3, J. Mayet1.1International Centre for Circulatory Health, Imperial College & St Mary’s Hospital, London, UK; 2Department of Clinical Engineering, Royal Brompton Hospital, London, UK; 3Department of Bioengineering, Physiological Flow Unit, Imperial College, London, UK
Introduction: Coronary artery blood flow occurs largely in diastole, when compression of the coronary microcirculation is relieved by relaxation of the myocardium. It is widely assumed that in addition to this mechanism, diastolic blood flow is augmented, by a series of waves reflecting back into the coronary arteries from the distal aorta. These waves are said to be advantageous in youth (arriving in diastole)—increasing coronary blood flow, and disadvantageous in old age (arriving in systole)—inhibiting coronary blood flow. However, until recently it was not possible to clearly identify theses reflected waves in the aorta. Our new approach of wave intensity analysis makes it possible to test this conventional wisdom by identifying these reflected waves unambiguously, and assessing their impact on coronary blood flow
Method: In 19 subjects (age 54 (SD 10) years, female 13), simultaneous measurement of pressure and Doppler velocity were made at 10 cm intervals along the aorta using intra-arterial sensor-tip catheters. Wave intensity analysis was used to separate forward travelling (incident) waves from wave reflected from distal arterial sites.
Results: The mean transit time of the incident wave from the aortic root to the distal aorta (50 cm) was 55 ms, the transit time between each interval was 11 (SD 3) ms. The reflected wave was found to closely parallel the timing of the incident wave along the entire length of the aorta. The mean time interval between the incident and reflected wave was 46 (3) ms (fig). In each subject the reflected wave arrived back in the proximal aorta in systole, and its timing was not significantly altered by age (r = 0.14, p = 0.57).
Conclusions: Using wave intensity analysis, it is possible to unambiguously identify forward and backward travelling waves in the human aorta. In all subject reflected waves arrive in the proximal aorta in systole. Wave reflection does not augment diastolic coronary blood flow—even in young subjects.
wave reflection; wave speed; coronary blood flow

Abstract 079 figure 1.

Abstract 079 figure 2.
080 LONG QT PEAK: A NOVEL ECG CRITERION FOR LEFT VENTRICULAR HYPERTROPHY
K. Wong1, S. McSwiggan2, S. Wong2, A. Gavin2, R. MacWalter2, A. Struthers2.1Cardiothoracic Centre-Liverpool NHS Trust, Liverpool, UK; 2Tayside Institute of Cardiovascular Research, Ninewells Hospital and Medical School, Dundee, UK
Introduction: In small studies in hypertensive subjects1 and patients with suspected coronary artery disease,2 QT peak prolongation was associated with left ventricular hypertrophy (LVH). This relationship however was not present in teenage professional footballers whose LVH was more likely to be physiological, characterised by myoctye hypertrophy with minimal or no myocardial fibrosis. The purpose of this study was to test the hypothesis that QT peak predicts echocardiographic LVH in stroke survivors.
Methods: 202 patients (122 male, mean age 66 (SD 9.4), mean blood pressure (BP) 145/80 (SD 21/11) mmHg) who made a good recovery and were at least one month after a cerebrovascular event were recruited into the study. QT peak measurements were made in lead I and were heart rate corrected using Bazett’s formula (QTpc = QTp/√RR). ECGs were digitised by a single observer blinded to the echocardiographic data. Echocardiographic LVH was defined as left ventricular mass index (LVMI) ⩾134 g/m2 in men and 110 g/m2 in women.
Results: Echocardiographic LVH was present in 26.2% of patients. 11.9% had repolarisation abnormalities on the ECG. 3% had LVH by gender specific Cornell Voltage. 8% had LVH as evidenced by Cornell Product ⩾243.6 mV.ms.
QT peak correlated with LVMI (as continuous variables—Spearman r = 0.3, two-tailed p = 0.004). In patients with LVH, QT peak was significantly longer (mean 334 ms (95% CI 326 to 342 ms) v 322 ms (95% CI 317–327 ms); UNIANOVA p = 0.012). If QT peak is prolonged to 320 ms or more, positive predictive value was 32% and negative predictive value was 85%. (Fisher’s exact 2p = 0.037, Mantel-Haenszel Common Odds Ratio Estimate = 2.7, 95% CI 1.1 to 6.4, 2p = 0.028.) ROC curve area = 0.65, 95% CI 0.55–0.76, p = 0.011. Using a cut-off value of 300 ms, no cases of LVH would be missed. (Fisher’s exact test two-sided p = 0.037).
Conclusions: QT peak prolongation predicts left ventricular hypertrophy in stroke survivors. In hypertension, regression of LV mass during treatment is a favourable prognostic marker.[3] Future work should test the hypothesis that reducing BP to achieve shortening of QT peak not only results in regression of LV mass but also improvement of the prognosis of stroke survivors who are at high risk of cardiac death.
1
2
3
left ventricular hypertrophy; QT peak; stroke
081 LOW UROTENSIN II LEVELS PREDICT RISK OF REINFARCTION IN POST MI PATIENTS
S. Khan, D. Kelly, J. Davies, L. Ng.University of Leicester, Leicester, UK
Background: Urotensin II (UII) is a potent vasoactive peptide present in human myocardium acting via the GPR14 receptor. We have previously shown UII to be raised after an acute myocardial infarction (AMI) suggesting a pathophysiological role for this endogenous peptide. The aim of this study was to see if UII levels could be used to predict risk of reinfarction in post MI patients.
Methods: We studied 504 patients (383 men, mean age 64.8 (SD 12.5) years, 80% STEMI, 20% NSTEMI) with AMI. Serial blood measurements were made at 24 hourly intervals for a median of five days after onset of chest pain. Samples were extracted using standard C18 Sep-Pak columns and UII was assayed using an in-house competitive chemiluminescent immunoassay. Comparison was made with N terminal B-type natriuretic peptide (NT-BNP). There was 100% patient follow up and reinfarction was defined as readmission to hospital with ECG changes and a troponin rise above the 99th centile for our population.
Results: Median follow up was 352 days (range 0–644) and 42 reinfarctions were noted over this time. Peak UII levels were lower in patients who reinfarcted compared to those who did not (median (range) fmol/ml, 0.77 (0.29–11.0) v 1.6 (0.29–34.7), p = 0.01). Using a multivariate binary logistic model peak UII (OR 0.49, 95% CI 0.27–0.89, p = 0.018) and peak NT-BNP (OR 1.71, 95% CI 1.0–2.96, p = 0.05) independently predicted reinfarction. On the Cox proportional hazards model however the only independent predictor of reinfarction was peak UII (HR 0.51, 95% CI 0.29–0.89, p = 0.019). The Kaplan-Meier survival curve revealed a significantly better clinical outcome in patients with UII above the median compared with those with UII below the median (log rank 6.30, p = 0.012). The receiver operating curve for peak NT-BNP yielded an area under the curve (AUC) of 0.59 (95% CI 0.51–0.67, p = 0.03); for peak UII the AUC was 0.61 (95% CI 0.53–0.68, p = 0.01).
Conclusion: Peak UII but not NT-BNP is better able to independently predict reinfarction in patients post MI. Patients with a poor outcome mount a lower UII response suggesting a possible cardioprotective role for this peptide and target for future therapy. The role of UII in affecting plaque stability remains to be established.
Urotensin II; myocardial infarction; NT-BNP
082 THE COST EFFECTIVENESS OF PERINDOPRIL IN REDUCING CARDIOVASCULAR EVENTS IN PATIENTS WITH STABLE CORONARY ARTERY DISEASE USING DATA FROM THE EUROPA STUDY
A. Briggs1, B. Mihaylova2, M. Sculpher3, A. Hall4, J. Wolstenholme5, M. Simoons6, R. Ferrari7, W. Remme8, M. Bertrand9, K. Fox10.1University of Glasgow, Glasgow, UK; 2Oxford Outcomes Ltd, Seacourt Tower, West Way, Oxford, UK; 3University of York, York, UK; 4University of Leeds, Leeds, UK; 5University of Oxford, Oxford, UK; 6Erasmus University Medical Centre, Rotterdam, Netherlands; 7University of Ferrara, Ferrara, Italy; 8Sticares Cardiovascular Research Institute, Rotterdam, Netherlands; 9Hôpital Cardiologique de Lille, Lille, France; 10Royal Brompton Hospital, London, UK
Background: The EUropean trial on Reduction Of cardiac events with Perindopril in stable coronary Artery disease (EUROPA) trial has recently reported. The aim of this study is to assess the cost effectiveness of perindopril in stable coronary heart disease in the UK, based on data taken from this trial.
Methods: Clinical and resource use data were taken from the EUROPA trial. Costs included all medications and hospitalisations. Health related quality of life values were not collected inthe trial and these were therfore taken from published sources. Cost effectiveness analysis is presented as a function of the risk of a primary event (non-fatal myocardial infarction, cardiac arrest, or cardiovascular death) in order to identify individuals for whom treatment offers greatest value for money.
Results: The median incremental cost per QALY gained of perindopril across the heterogeneous population of EUROPA was estimated as £9500 (interquartile range: £6500–£14,400). Overall, 89% of the EUROPA population had a point estimate of incremental cost per QALY below £20,000 and 97% below £30,000. For a threshold value of cost effectiveness of £30,000 per QALY gained, individuals representing the 25th, 50th (median), and 75th percentiles of the cost effectiveness distribution for perindopril have probabilities of 0.99, 0.98, and 0.92 of being cost effective, respectively. Cost effectiveness was strongly related to higher risk of a primary event under standard care.
Conclusions: Whether the use of perindopril can be considered cost effective depends on the health care systems’ threshold values of cost effectiveness. For the large majority of patients included in EUROPA, the incremental cost per QALY gained is lower than the apparent threshold used by the National Institute for Health and Clinical Excellence in the UK.
cost effectiveness; ACE inhibitors; economic analysis
083 THE RELATIONSHIP BETWEEN ATRIAL LEAD TYPE AND THE ACCURACY OF ARRHYTHMIA DISCRIMINATION
J. Silberbauer1, A. Arya1, N. Freemantle2, V. Paul3, N. Patel1, G. Lloyd1, N. Sulke1.1Eastbourne General Hospital, Eastbourne, UK; 2University of Birmingham, Birmingham, UK; 3Ashford and St Peters Hospital, Chertsey, UK
Introduction: Accurate atrial arrhythmia discrimination is important for dual chamber pacemakers and defibrillators. Vitatron T70 and Selection 9000 pacemakers allow detailed analysis of oversensing and undersensing of atrial arrhythmias using device derived detailed onset reports (DOR).
Methods: Patients with at least three symptomatic episodes of PAF (Paroxysmal Atrial Fibrillation) in the last month and refractory to at least two drugs were recruited. 182 patients (72 (SD 9) years, 55% male) enrolled. Patients were included in the study if they had an AF burden of 1–50% during the monitoring phase. 87 patients fulfilled these criteria and were followed for at least five months with monthly Holter review. 24 atrial leads were active and 63 passive fixation (majority in right atrial appendage, all steroid eluting). Patients were classified as having short (<10 mm), medium (10–13), or long (14–18) atrial tip-to-ring (TTR) distances. Every DOR was reviewed to allow analysis of malsensing/aberrancy.
Results: 2883 DORs were analysed, 730 (25%) demonstrated malsensing aberrancy. 6% was due to farfield R wave (FFRW) oversensing and 19% due to undersensing sometimes occurring in the same study patient and phase. Specific anti-AF algorithm review showed that ventricular rate stabilisation (VRS) increased ventricular pacing from 50% to 60% when turned on (p<0.0001). FFRW oversensing increased from 4% to 8% (p = 0.0035) during this phase. FFRW oversensing occurred in no patients with a short TTR distance (p<0.05). Undersensing due to sensitivity fallout was 18% (short), 23% (medium), and 20% (long) (p = NS). Undersensing due to pacemaker blanking was 11% (short), 11% (medium), and 12% (long) (p = NS). Active fixation electrodes did not affect sensing.
Conclusion: Even with the best modern devices up to 25% inaccuracy in detection of atrial arrhythmias occur. Algorithms increasing V pacing will increase FFRW oversensing but this can be completely eliminated using bipolar atrial electrodes with short (<10 mm) tip to ring distance and should be used in all devices requiring accurate arrhythmia discrimination.
atrial electrode; arrhythmia; sensing

Abstract 083.
084 PERCUTANEOUS EXTRACTION OF PACING AND DEFIBRILLATOR LEADS: CONVENTIONAL/NON-LASER METHODS ARE BOTH SAFE AND EFFICACIOUS
S. Gieowarsingh, T. Ali, G. Ng, P. Stafford, J. Skehan.Glenfield Hospital, University Hospitals of Leicester, Leicester, UK
Background: Extraction of pacing/ICD leads is a difficult task and with expansion of device therapy it has become an incresingly important procedure in the optimal management of device related complications. We aimed to determine the current indications, safety, and efficacy of lead extraction at our institute.
Methods: Retrospective analysis of 135 procedures from October 1999 to September 2005 attempting removal of 253 leads (90 atrial, 163 ventricular including 15 ICD, eight coronary sinus) in 131 patients (ages 6–95, mean 63 years). Patients were identified from catheter lab screening log books and data were collated from case notes.
Results: Lead age was 1–354 months (mean 57), 72% ⩾12 months. Indications were pocket infection/erosion 46%, sepsis 13%, endocarditis 16%, lead failure 18%, and other 7%. Of the 101 cases indicated because of infection the majority (60%) were preceded by a secondary pacing operation such as box change 11%, pocket revision 23%, lead revision/upgrade/new system 26%. Two senior operators performed the majority of procedures (75%). A superior approach via the implant vein was used for 89% of leads. An inferior approach via the femoral vein was used in one case and a combined approach was utilised for 10.5% of leads. Of the 253 leads attempted 30% were removed with simple traction, 34% with locking stylets, 25% with the addition of dilator sheaths, retrieval devices were required in 11%, and in nine cases electrocautery sheaths were used. Lead removal was complete in 91%, partial in 5% and failed in 4%. Major perioperative complications occured in five cases (3.7%, with two deaths 1.4%). These were: one cardiac tamponade, one severe mitral regurgitation, one entrapment of snare requiring surgery, one death from atrial rupture, and one death from pulmonary embolism. Minor complications were observed in six (4.4%) cases. Emergency surgery occured in three cases because of complications and one patient had elective surgical extraction.
Conclusion: We found that with experienced operators conventional techniques and tools for lead extraction afforded a high success rate with few major complications. These data should be used as a baseline against which new technologies can be tested. Of the group undergoing extraction because of infection the majority followed secondary pacing procedures. Senior input to pacemaker reoperation is recommended as this may offer some preventative benefit.
extraction; lead; pacemaker
085 ADVERSE CORONARY VENOUS ANATOMY FREQUENTLY PREVENTS OPTIMAL LEFT VENTRICULAR PACING LEAD POSITIONING
A. Ryding, J. Timperley, D. Tomlinson, Y. Bashir, T. Betts.John Radcliffe Hospital, Oxford, UK
Background: Large trials indicate an 85–95% success rate at implanting transvenous left ventricular (LV) leads for biventricular pacing. An optimal lead position on the lateral LV wall is desired as this may maximise patient response. The proportion of LV leads that are positioned at the optimal pacing site and the reasons for suboptimal positioning, are not known.
Methods: A consecutive series of patients undergoing transvenous biventricular pacing were studied. Optimal lead position was defined as LV lead tip position between the anterolateral (North-East) and posterolateral (South-East) quadrants in the radiographic LAO view and in the mid-third between base and apex in the RAO view. Adverse events that challenged optimal lead position were grouped into (1) difficult coronary sinus (CS) cannulation, (2) phrenic nerve stimulation, and (3) poor target vessels in the optimal segment.
Results: Fifty five procedures were performed on 50 patients (45 male, mean age 63 (SD 11) years). All patients were discharged with “successful” LV pacing. 34/55 (62%) procedures ended with the LV lead in the optimal position. Two procedures were initially abandoned due to failure to cannulate the CS. Two procedures were repeated due to late phrenic nerve stimulation and one due to late lead dislodgement. 34/53 (64%) completed procedures ended with the LV lead in the optimal position and 21/53 (36%) in a suboptimal position. 18/55 (33%) procedures had no adverse events, with all leads placed in the optimal position. 37/55 (67%) procedures were subject to an adverse event, with 16/35 (48%) completed procedures ending with the lead in an optimal position and 21/35 (52%) completed procedures in a suboptimal position. 11/55 (20%) procedures had difficult CS cannulation, with two procedures abandoned. 20/53 (38%) procedures suffered phrenic nerve stimulation, 13 leading to suboptimal lead position. 14/53 (26%) procedures had poor quality target veins, contributing to suboptimal lead positioning in 12. After a mean FU of 252 (SD 155) days, 76% of patients were classed as responders. There was no difference in response to biventricular pacing between patients with optimal and suboptimal lead positions.
Conclusion: Although almost every patient undergoing CRT has a “successful” LV lead implant, two thirds will have adverse coronary venous or phrenic nerve anatomy, resulting in a suboptimal lead position in 36% of completed procedures. Despite this, patients with suboptimal LV lead positions are as likely to respond to biventricular pacing as those with an optimal lead position.
cardiac resynchronisation therapy; biventricular pacing; complications
086 THORACOSCOPIC IMPLANTATION OF LEFT VENTRICULAR EPICARDIAL PACING LEAD FOR BIVENTRICULAR PACING IN HEART FAILURE
R. Jutley, I. Loke, D. Waller, D. Chin, P. Stafford, J. Skehan, T. Spyt.University Hospitals of Leicester, Leicester, UK
Introduction: Percutaneous LV lead placement through the coronary sinus is the technique of choice for biventricular pacing in heart failure. The technique has a failure rate of 8–10% due to lead displacement, variable anatomy and high thresholds. We describe our initial experience of thoracoscopic implantation of LV epicardial pacing lead in patients where the percutaneous technique failed.
Methods: The procedure was performed under general anaesthesia and single-lung ventilation. The LV free wall was accessed via three 2 cm incisions without rib spreading. A 2 cm pericardiotomy was performed under transoesophageal echocardiography guidance and the pacing lead was placed in the area between the first diagonal and first obtuse marginal arteries.
Results: Eleven patients (median age 64 years (range 54–82); 9 male; 2 female; 2 with previous open cardiac surgery) were evaluated. Indications for biventricular pacing included dilated cardiomyopathy in eight; ischaemic cardiomyopathy in three. All patients had a QRS duration of >120 msec and fulfilled echocardiographic criteria for dyssynchrony. Mean ejection fraction was 26.8% (range 15–40%) and the median garde of mitral regurgitation was 1. All patients had undergone a standard transvenous implantation of a biventricular pacing device and leads under routine fluoroscopic guidance. Subjects had either unsatisfactory left ventricular lead position or lead displacement following their initial procedure. All patients had a satisfactory thorascopic procedure whereby a satisfactory LV lead position was obtained. Conversion to minithoracotomy was necessary in one patient (previous CABG). Median procedure time was 70 minutes (55–135). Median time to chest drain removal was one day (1–3) and hospital stay two days (2–8). All patients reported symptomatic improvement with median NYHA score change from III (III–IV) to II (0–II) postoperatively. Satisfactory lead thresholds and impedances on median follow up of 120 days were maintained in all but one patient (previous CABG).
Conclusions: Thoracoscopic LV pacing lead placement offers an excellent solution to LV lead placement in biventricular pacing. The method is feasible, reproducible and in our small sample, free of significant complications. Large scale randomised trails would be necessary to evaluate this approach which offers an attractive alternative to the percutaneous technique.
biventricular; heart failure; thorascopy
087 PERCUTANEOUS EPICARDIAL IMPLANTATION OF LEFT VENTRICULAR PACING LEADS: A FEASIBILITY STUDY IN HUMANS
D. Gupta, R. Schilling.St Bartholomew’s Hospital, London, UK
Background: Conventional implantation of the left ventricular (LV) pacing lead via the Coronary sinus may be limited by anatomical constraints. The alternative surgical approach to LV lead implantation is invasive and requires general anaesthesia. Percutaneous access to the pericardial space under local anaesthesia has recently been utilized for epicardial ablation.
Methods: We investigated the feasibility of using a percutaneous xiphisternal approach to implant the LV pacing lead in five patients undergoing CRT. We could access the pericardial space in four patients who received an active fix pacing lead on the mid lateral epicardial surface of the LV guided by pre-procedure tissue Doppler imaging. Simultaneous coronary angiography confirmed a safe distance of the lead tip from the coronary vasculature. The LV lead was tunnelled up to the subcutaneous pectoral pocket where it was connected to the generator box. The right atrial and right ventricular leads were inserted transvenously in the conventional fashion. The final position of the epicardial LV lead in one of the patients is shown in the figure. (A = tip of epicardial lead, B = site of suture on the pre-rectus fascia, C = subcutaneous tunnel to the pectoral pocket).
Results: Percutaneous access to the pericardial space could not be achieved in one patient with prior bypass surgery due to dense pericardial adhesions. Of the four patients with successful LV epicardial lead implantation, one patient needed lead explantation as it had caused gastric perforation while the other three patients had lead displacements after a mean period of six days.
Conclusions: While technically possible, percutaneous epicardial LV lead implantation has an unacceptably high lead dislodgement rate. There is also the risk of abdominal visceral perforation. Further attempts using this technique must await improvement in hardware.
epicardial; biventricular pacing; heart failure

Abstract 87.
088 LOCATION OF THE CORONARY SINUS USING ENDOCARDIAL TEMPERATURE SENSORS: A NEW APPROACH FOR CORONARY SINUS CANNULATION
D. Fox1, R. Receveur2, S. Petkar3, V. Larik2, N. Davidson4, B. Miller3, A. Fitzpatrick3.1Manchester Heart Centre, Manchester, UK; 2Bakken Research Centre, Maastricht, Netherlands; 3Manchester Heart Centre, Manchester Royal Infirmary, Manchester, UK; 4North West Regional Cardiac Centre, Wythenshawe Hospital, Manchester, UK
Introduction: Cannulation of the coronary sinus (CS) for cardiac resynchronisation therapy (CRT) can be time consuming. A high contrast load may be needed to identify the CS and pre-existing renal dysfunction may be exacerbated by contrast induced nephropathy.
Hypothesis: We hypothesised that sensitive temperature sensors (TS) could assist in identifying the CS for cannulation. Previous studies have identified venous blood exiting the CS as being approximately 0.15°C warmer than right atrial blood due to the intense metabolic activity of the heart.
Methods: Four male patients receiving CRT were recruited. We developed a sensitive (0.01°C) and responsive (80 msec) endocardial temperature measurement device (TS) that can accurately display real time temperatures from within the heart. The TS had an audible tone, the pitch of which increased at higher temperatures. The device had a TS on a pacing electrode which was deployed down the CS guide catheter. The TS was deployed under x ray control, 2 mm outside the guide catheter ostium for cannulating the CS. Multiple cannulations of the CS were performed per patient, with a delay of 1 minute between each cannulation.
Results: All patients had a rise in both temperature and audible tone on entering the ostium of the CS. An average of 7.5 measurements were taken per patient (range n = 1–10). Results are the mean increase in temperature (in °C): Patient (P) 1 mean 0.19 SEM n/a, P2 mean 0.1 SEM 0.06, P3 mean 0.1 SEM 0.02, P4 mean 0.1 SEM 0.03. The ability to enter the CS without the use of contrast was seen in all patients, with subsequent confirmation of CS location with contrast. Mean CS blood temperature was significantly warmer than right atrial blood (p<0.0001). The rise in temperature was seen at the CS ostium. Mean increase of all the measurements was 0.12°C, SD 0.04.
Conclusions: A TS deployed as an adjunct to a guide catheter may reduce the amount of contrast required and speed up cannulation of the CS. This is the first reported use of a TS as an adjunct to left heart lead placement for patients undergoing CRT.
cardiac resynchronisation therapy; coronary sinus; temperature sensor
089 RADIOGRAPHIC ASSESSMENT AND ELECTROCARDIOGRAPHIC FEATURES OF LEAD POSITION IN RIGHT VENTRICULAR OUTFLOW TRACT PACING
A. McGavigan1, K. Roberts-Thomson2, R. Hillock2, I. Stevenson2, H. Mond2.1Glasgow Royal Infirmary, Glasgow, UK; 2Royal Melbourne Hospital, Melbourne, Australia
Introduction: Pacing from the right ventricular (RV) apex is associated with long-term adverse effects on left ventricular function. This has fuelled interest in alternative pacing sites, the most common being the RV outflow tract (RVOT). Acute and chronic studies of RVOT pacing have provided conflicting results which may be explained in part by the poor definition and heterogeneity of pacing sites within the RVOT. We sought to characterise the pacing site in an unselected series of patients undergoing RVOT lead placement and to investigate the role of the 12 lead ECG in predicting the site of implantation.
Methods: In 150 patients undergoing pacemaker implantation for a standard indication, implanters were asked to place the lead in the RVOT. No further instruction was given. Radiographs were performed in the antero-posterior (AP) and 40° right and left anterior oblique (RAO/LAO) projections post procedure. Fifty six also had left lateral radiographs. Three researchers independently categorised lead position using AP and RAO to confirm RVOT placement and LAO to distinguish free wall from septal aspects. Disagreements were resolved by consensus opinion. A 12-lead ECG was performed during ventricular pacing.
Results: In 18 patients (12%) the leads were below the RVOT. In the remaining 132 cases, the majority (94%) were in the inferior/low RVOT. 81/132 were classified as septal and 51 as free wall. Septal sites were associated with a shorter QRS duration (134 v 143 ms, p<0.02). Free wall sites displayed more frequent notching of the inferior leads (p<0.01). Lead I was a useful discriminator between sites, with a negative deflection providing a positive predictive value of 90% for septal sites. Of the 56 with left lateral radiographs, a posterior projection of the lead was 100% specific for septal placement.
Conclusions: This study demonstrates the diversity of placement of leads within the RVOT as determined by standard radiography, which has implications when planning future studies. Septal and free wall sites display characteristic ECG patterns which may be used to aid placement. The left lateral radiograph is useful in confirming a true septal location.
pacing; outflow tract; lead position
090 AUTO-TITRATING CONTINUOUS POSITIVE AIRWAY PRESSURE IN PATIENTS WITH OBSTRUCTIVE SLEEP APNOEA AND CHRONIC HEART FAILURE: A RANDOMISED PLACEBO CONTROLLED TRIAL
L. Smith1, M. Vennelle2, R. Gardner3, T. McDonagh3, M. Denvir1, N. Douglas2, D. Newby1.1Cardiovascular Research, University of Edinburgh, Edinburgh, UK; 2Sleep Centre, University of Edinburgh, Edinburgh, UK; 3Scottish Cardiopulmonary Transplant Unit, Glasgow, UK
Introduction: Obstructive sleep apnoea (OSA) is highly prevalent in patients with chronic heart failure (CHF). OSA may contribute to CHF progression by causing nocturnal hypoxia, increased sympathetic nervous system activity and adverse cardiac performance. This study aimed to determine whether treatment of OSA by regular nocturnal continuous positive airway pressure (CPAP) would improve symptoms, functional capacity and objective measures of CHF severity.
Methods: Twenty six patients (age 61 (2) (mean (SE)) years) with stable symptomatic CHF (left ventricular ejection fraction (LVEF) 29 (2)%) and OSA (apnoea/hypopnoea index 36 (4) events/hour slept) were randomised to nocturnal auto-titrating CPAP (Autoset Spirit; ResMed, Sydney, Australia) and sham CPAP for six weeks each in a crossover design. Investigators were blinded to treatment modality. Study endpoints were changes in LVEF, peak VO2, VE/VCO2 slope, 6 minute walk distance (6MW), quality of life (Epworth Sleepiness Scale (ESS), SF-36, Minnesota Living with Heart Failure), N-terminal pro-brain natriuretic peptide (NT-proBNP), and plasma norepinephrine (NE) concentrations.
Results: Twenty three patients completed the study. Mean (SD) nightly CPAP (mean pressure 7 (2) cm H2O) and sham CPAP usage were 3.5 (2.5) and 3.3 (2.2) hours/night respectively (p = 0.31). CPAP treatment was associated with improvements in daytime sleepiness (ESS 7 (1) v 8 (1), p = 0.04) but not in other quality of life measures. There were no differences in objective measures of cardiac function, exercise capacity or neurohormonal activation (table).
Abstract 90
Conclusions: In patients with OSA and CHF, nocturnal auto-titrating CPAP improves daytime sleepiness but not other subjective or objective measures of CHF severity. These data suggest that the potential therapeutic benefits of CPAP in CHF are achieved by alleviation of OSA rather than by improvement in cardiac function.
chronic heart failure; sleep apnoea; CPAP
091 HARNESSING PHYSIOLOGICAL CARDIORESPIRATORY INTERACTION TO MODULATE VENTILATION BY DYNAMIC CHANGES IN CARDIAC OUTPUT
C. Manisty1, J. Davies1, K. Willson2, Z. Whinnett1, A. Hughes1, J. Mayet1, D. Francis1.1International Centre for Circulatory Health, Imperial College and St Mary’s Hospital, London, UK; 2International Centre for Circulatory Health, Imperial College, London, UK
Background: A proportion of patients with left ventricular dysfunction have unstable cardiorespiratory control which manifests as periodic breathing, driven by fluctuating carbon dioxide levels. There are multiple factors contributing to the pathophysiology, but chemoreflex delay and gain have been proven to be significantly greater in patients with unstable cardiorespiratory control. It is possible to manipulate cardiac output in patients with cardiac pacemakers by changing the programmed heart rate. We therefore used patients with pacemakers to test the possibility that changes in cardiac output can affect the delivery of carbon dioxide into the lung reservoir, and via the chemoreflex thereby acutely influence ventilation.
Method: We studied the effect of repeated alternations in heart rate of increment 30 bpm and period 60 seconds, on cardiorespiratory parameters in 16 subjects with implanted cardiac pacemakers and stable breathing patterns (eight with normal ventriclular function and eight with systolic heart failure). End tidal carbon dioxide (ETCO2) and ventilation were stable before and after intervention (mean ETCO2 4.29 (0.8) kPa, mean ventilation 7.62 (2.2) l/min).
Results: During intervention, both ETCO2 and ventilation exhibited consistent sinusoidal oscillations with a period of 60 seconds (ETCO2—mean peak 4.37 kPa, mean trough 4.21 kPa, p<0.0001; ventilation—mean peak 7.98 l/min, mean trough 7.2 l/min, p<0.0001) (fig 1).
The mean amplitude of oscillations in ETCO2 with the heart rate alternations was 3.5 (1.7)%, with a mean ventilation amplitude of 11.4 (7.5)%. This represents a peak to trough change in ETCO2 of 7% and ventilation of 22.8% with this dynamic pacing intervention. There was no significant difference between the patients with impaired and normal ventricles in either ETCO2 (p = 0.42), or ventilatory (p = 0.74) response to cardiac output manipulation. The magnitude of the respiratory oscillations generated was correlated to the cardiac output changes generated by the pacing protocol (r = 0.53, p = 0.035) (fig 2).
Conclusions: Cardiovascular modulation via dynamic programmed cardiac pacemaker interventions can elicit consistent oscillations in carbon dioxide and thus ventilation in patients with stable cardiorespiratory control. The size and pattern of respiratory response is very consistent within individual subjects, however intersubject variation is due to differing cardiac output responses to the programmed heart rate increments. Potentially this mechanism could be harnessed and timed appropriately to counteract the fluctuations in carbon dioxide and ventilation occurring with periodic breathing, hence dynamically stabilising respiratory control.
cardiorespiratory control; periodic breathing; heart failure

Abstract 091, figure 1.

Abstract 091, figure 2.
092 THE EFFECT OF DIURETICS ON PEAK OXYGEN CONSUMPTION IN PATIENTS WITH COMPENSATED LEFT VENTRICULAR DYSFUNCTION
S. Gupta1, N. Gandhi1, N. Clayton1, C. Waywell1, T. Coppinger1, N. Brooks1, L. Neyses2.1Wythenshawe Hospital, Manchester, UK; 2University of Manchester, Manchester, UK
Introduction: Diuretics are commonly used in patients with left ventricular dysfunction and chronic heart failure (CHF). In clinically congested patients, diuretics alleviate symptoms and improve exercise capacity. There is no data available on the effects of diuretics on exercise capacity and peak oxgen consumption (pVO2) in CHF patients who are clinically not congested. It has, however, been hypothesised that reducing end diastolic pressures with diuretics may improve cardiac output and hence exercise tolerance. The aim of our study was to assess whether diuretics are superior to placebo in improving exercise capacity and peak oxygen consumption in patients with proven left ventricular dysfunction but who are clinically not congested.
Method: The Manchester Water Study was a randomised double blind, placebo controlled, crossover study. 30 patients with echocardiographic evidence of left ventricular dysfunction (left ventricular ejection fraction of less than 45%) were recruited. All patients were on maximum tolerated doses of ACE inhibitors and beta blockers. None were routinely taking any diuretics and none had any evidence of congestion on clinical examination. All patients performed a symptom limited cardiopulmonary exercise test to measure their peak oxygen consumption and were then randomised to receive either Torasemide 5 mg daily or placebo for three months (Phase A). At the end of this period, pVO2 measurements were repeated and study medications were stopped for a washout phase of two months. After the washout phase, patients were crossed over for a further threemonths (Phase B) with pVO2 measurements before and after.
Results: Completed data were available in 27 patients (24 male, 3 female). Two patients dropped out of the study and one was unable to perform a cardiopulmonary test during phase B. The majority of patients were in NYHA class 1 (n = 6) or 2 (n = 20) at the beginning of the study. Mean age was 59.4 years (range 32 to 80 years). Analyses of variance (incorporating carry over and period effects) appropriate for a two period crossover design were used to assess the effect of the active treatment. No significant effect of carry over or phase was found. Mean pVO2 at the beginning of Phase A was 16.6 ml/kg/min (range 9.3–25)) and at beginning of Phase B was 17.1 ml/kg/min (range 8.4–28.4). Mean pVO2 fell by 0.04 ml/kg/min on placebo and by 0.13 ml/kg/min on active treatment. This difference was not statistically significant—F(1, 25) = 0.04; p = 0.84.
Conclusion: Diuretics are not superior to placebo in improving peak oxygen consumption and exercise capacity in patients with left ventricular dysfunction who are clinically not congested.
diuretics; heart failure; peak oxygen consumption
093 DIABETES MELLITUS LOWERS SIX MINUTE WALK TEST PERFORMANCE IN PATIENTS WITH CHRONIC HEART FAILURE
L. Ingle, A. Clark, J. Cleland.University of Hull, Hull, UK
Introduction: Recent studies have shown that patients with diabetes mellitus and left ventricular systolic dysfunction (LVSD) have a lower peak oxygen uptake than patients with LVSD alone. Peak oxygen uptake provides important information on risk stratification, and can be used to guide management. However, tests involve cycling- or walking-based protocols of increasing speed, gradient or resistance, are not well tolerated in some patients with LVSD. The six minute walk test (6-MWT) is an alternative, and widely used method of assessing functional capacity; it is simple and cost effective to perform, is safe because patients are self-paced during exertion, and previous reports suggest it is a reliable test provided it is well standardised in patients with heart failure. However, to our knowledge the impact of diabetes mellitus on 6-MWT performance has not been investigated previously.
Methods: Patients were recruited from a local community heart failure clinic, inclusion criteria were: stable medical therapy, and evidence of LVSD, defined as a left ventricular ejection fraction (LVEF) of <40%. Patients who met the inclusion criteria underwent clinical history and physical examination, together with ECG, echocardiogram, and routine blood samples. Glycosylated haemoglobin was measured in all patients. The 6-MWT was conducted following a standardised protocol after usual medication.
Results: We identified 256 patients with CHF and diabetes among 756 patients with LVEF <40% in our clinic. We then matched these patients for age and sex to the remaining 500 non-diabetic patients. We found age and sex matches for 88 patients who were selected as our patient cohort. 6-MWT performance was lower in diabetic (238 (124) m) than in non-diabetic patients (296 (131) m; p = 0.005). Diabetic state remained an independent predictor of impaired 6-MWT performance after controlling for haemoglobin, NT-proBNP, hypertension, ischaemic heart disease, severe renal impairment, atrial fibrillation (AF), ejection fraction, and glycosylated haemoglobin. Glycosylated haemoglobin was higher in the diabetic patients (p = 0.001). Stature, BMI, haemoglobin, NT-proBNP, COPD, hypertension, renal impairment, AF, and heart failure medication were similar in both groups.
Conclusions: While 6-MWT performance is compromised in patients with LVSD compared to aged matched controls, the addition of diabetes mellitus to LVSD is likely to further reduce functional capacity. Diabetic patients with LVSD have a poorer 6-MWT performance than LVSD alone. Diabetic state is an independent determinant of poorer walking performance in patients with LVSD.
diabetes; CHF; 6-min walk test
094 THE EFFECT OF WEEKLY ALCOHOL INTAKE ON LEFT VENTRICULAR SIZE AND FUNCTION
G. Galasko, A. Lahiri, R. Senior.Department of Cardiovascular Medicine, Northwick Park Hospital, Harrow, UK
Introduction: Heart failure is a common chronic disorder with high associated morbidity, mortality and cost, with left ventricular systolic dysfunction (LVSD) underlying most treatable cases. Alcohol is a myocardial depressant with chronic excess culminating in LVSD and heart failure. With increasing government concern that alcohol misuse is on the increase, potentially costing £20 bn a year in the United Kingdom alone, this study was undertaken to further evaluate the effect of weekly alcohol intake on markers of left ventricular size and function.
Methods: Accordingly, 1392 general population subjects ⩾45 years of age were randomly selected from the computer records of seven representative local general practices and invited to attend. A further 210 subjects, 30 per practice, were also randomly selected from the same computer records from those with a history of heavy alcohol intake and invited to attend. Attending subjects underwent echocardiography with measurements taken including left ventricular end-systolic (ESV) and end-diastolic volumes (EDV) and left ventricular ejection fraction (LVEF) using Simpson’s apical biplane method, the average of three readings. LVSD was defined as LVEF <50%. LV mass index was calculated using the Devereux modified American Society of Echocardiography equation. Height and weight were measured.
Results: 734 general population subjects (53%) and 115 heavy drinkers (55%) attended. LVEF was calculable in 816 cases (96%), 44 of whom (5.4%) had LVSD. The prevalence of LVSD stratified by weekly alcohol intake showed a J-shaped relationship. The prevalence of LVSD was 4.2% in those drinking <21 units/week v 17.1% in those drinking ⩾56 units/week. In those who drank alcohol, there was a significant increase in LVSD with increased alcohol intake (p<0.001, χ2 test for trend). Mean LVEF fell with increased alcohol intake (p = 0.06, ANOVA). Mean left ventricular EDV index (stratified per unit body area) (p<0.0001, ANOVA), ESV index (p<0.0001, ANOVA), and left ventricular mass index (p = 0.0003, ANOVA) all rose progressively as weekly alcohol intake increased.
Conclusion: Thus left ventricular function deteriorates as weekly alcohol increases, with a progressive increase in the prevalence of LVSD, in end-diastolic volume index, end-systolic volume index and left ventricular mass index and a progressive decrease in left ventricular ejection fraction. As the prevalence of excess alcohol intake in the United Kingdom is increasing, this study may be a harbinger of an increased prevalence of alcoholic cardiomyopathy too with its high associated morbidity and mortality.
heart failure; left ventricular dysfunction; alcohol
095 MAGNETIC RESONANCE IMAGING AND SURGICAL LEFT VENTRICULAR RESHAPING FOR ADVANCED ISCHAEMIC CARDIOMYOPATHY
R. Ascione.Bristol Heart Institute, University of Bristol, Bristol, UK
Background: Surgical left ventricular reshaping SLVR reduces left ventricular (LV) volume and creates a more elliptical shape of the LV by excluding scar in either akinetic or dyskinetic segments. Optimal positioning of LV reshaping purse strings suture is of paramount importance. The aim of this study was to investigate the early and mid-term outcome in a series of patients undergoing cardiac magnetic resonance imaging (MRI) guided SLVR.
Methods: Sixteen patients (13 males, age 62 years (50–75) underwent SLVR post large antero-lateral myocardial infarction since 2003. Cardiac MRI was performed before and three months after surgery. Cine images were acquired using an electrocardiographic gated steady state free precession pulse sequence. Indication for SLVR was based on information from baseline MRI on extension of asynergy, remore muscle, and LV volume. Intraoperative positioning of two reshaping purse string suture was also directed by baseline MRI evaluation of the extent and location of the hyperenhancing myocardial scar (non-viable), obtained 10–15 minutes after contrast (gadodiamide) injection. Early and late functional and clinical outcomes were examined.
Results: Baseline NYHA class was II in 12.5%, III in 25%, and IV in 62.5%. Concomitant procedures included coronary artery bypass grafting in 93.7%, mitral valve repair in 25%, ablation of AF in 12.5%, tricuspid annuloplasty and ICD insertion in 12.5%. Intraventricular patch was needed in 56.5%. Overall 30 day mortality and stroke was 0%. One patient (6.25%) suffered acute renal failure and another one (6.25%) was reopened for bleeding. Postoperative IABP was used in all patients to minimise LV suture line stress, and in 50% also to facilitate weaning from CPB. Median hospital stay was 10 days (range 7–21). Baseline and follow up MRI was available for all patients. At follow up there was a significant improvement in global systolic function, decrease in left ventricular volume, and improvement of the ejection fraction (all p<0.01). Median follow up was 18 months (range 1–28). Mid-term NYHA class was I in 56.5% and II in 43.5%. Overall two year survival was 100%.
Conclusions: Surgical left ventricular reshaping improves ventricular function and is highly effective. Cardiac MRI is a useful tool for surgical planning and provides accurate information about scar extent and myocardium viability.
heart failure; MRI; surgical left ventricular reshaping
096 PREDICTING LEFT VENTRICULAR SYSTOLIC DYSFUNCTION IN PATIENTS WITH SYMPTOMS AND SIGNS OF HEART FAILURE IN THE COMMUNITY
S. Jeyaseelan, T. Fahey, B. Goudie, S. Pringle, P. Donnan, F. Sullivan, A. Struthers.University of Dundee, Dundee, UK
Background: Diagnosing left ventricular systolic dysfunction (LVSD) in the community is a challenge for general practitioners (GPs). Access to echocardiography, which is essential for diagnosis, is limited in many healthcare systems. A clinical prediction rule based on clinical history, examination and electrocardiogram (ECG) was developed so that referral for echocardiography might be targeted more efficiently at those symptomatic patients most likely to have LVSD.
Methods: We performed a prospective cohort study of 458 symptomatic patients, referred from 26 general practices in Scotland, whom were suspected of having LVSD. All patients underwent a structured clinical examination and an ECG. They all had an echocardiogram performed to establish presence of LVSD. Unvariate analysis was performed using key elements of the history and clinical examination to establish significant associations with LVSD. Multivariate analysis was preformed between those elements with significant associations with LVSD. The effect of the ECG classification as either normal or abnormal was then included in the multivariable analysis.
Results: Four elements from the clinical history and examination—male sex (adjusted odds ratio 2.5, 95% CI 1.1 to 5.0), presence of orthopnoea (OR 5.4, 1.9 to 13.8) history of MI (OR 5.6, 2.3 to 13.6), and elevated jugular venous pressure (OR 15.1, 4.6 to 49.3) were all independently associated with LVSD. Addition of ECG (OR 20.6, 2.7 to 158.6) provides important diagnostic information in terms of probability of LVSD. A clinical prediction rule based on the presence or absence of these five elements will generate probabilities ranging from 1% to 97% for LVSD when applied to an individual patient.
Conclusion: The clinical prediction rule provides a quantitative estimate of post-test probability for LVSD in patients presenting to their GP with suspected heart failure. It can thus aid in the decision making process by helping to identify patients in whom echocardiography should be performed.
heart failure; left ventricular systolic dysfunction; clinical prediction rule
097 QUANTITATIVE ASSESSMENT OF CONTRAST ENHANCED DOBUTAMINE STRESS ECHOCARDIOGRAMS USING A SEMI-AUTOMATIC BOUNDARY DETECTION WITH TEMPORAL INFORMATION
J. Timperley1, H. Thibault2, M. Mulet-Parada3.1John Radcliffe Hospital, Oxford, UK; 2Centre Hospitalier de Bordeaux, Bordeux, France; 3Mirada Solutions, Oxford, UK
Introduction: Dobutamine stress echocardiography (DSE) is a routinely used technique for the assessment of coronary artery disease and is sensitive enough to detect regional wall motion abnormalities (RWMA) prior to ECG evidence of ischaemia. However, visual assessment of RWM relies on the interpretation of both spatial and temporal information leading to significant observer variability.
Methods: We assessed a semi-automatic boundary detection (ABD) technique for interpretation of contrast DSE performed using Power Modulation and an infusion of Sonovue in 71 patients compared to an expert observer. We also assessed its accuracy in a subgroup of 30 patients undergoing coronary angiography. Regional function was assessed for the presence of a RWMA by the observers and using the endocardial excursion in each region using ABD. The mean regional excursion for each coronary vascular territory was calculated and compared to the expert observer for the presence of at least a 70% coronary stenosis. Receiver operating characteristic (ROC) curves were generated.
Results: The mean age of the study group was 65 (9) years with 44 males. ABD was possible in 100% of two- and four-chamber views, 93% of three-chamber views and 77% of short axis views giving 1626 regions at rest and 1597 regions at peak stress. The overall sensitivity, specificity, and area under the ROC curves (AUC) for the presence of a RWMA compared to the expert observer were at rest 81.5%, 73%, 81.5% and at peak 85.5%, 74.6%, and 82.4%. For the presence of a 70% epicardial coronary stenosis, the mean endocardial excursion had sensitivity, specificity and AUC of 72.7%, 55.6%, and 69.7% for the circumflex artery, 93.8%, 61.5%, and 77.2% for the left anterior descending and 84.6%, 62.5%, and 80% for the right coronary artery. The relatively poor accuracy in the circumflex territory was assocaited with significantly poorer image quality in this region (p<0.05).
Conclusions: ABD with incorporation of temporal information of DSE provides good detection of coronary artery disease in good quality contrast images and also of regional wall function at both rest and peak compared to an expert observer.
contrast; stress echocardiography; coronary artery disease
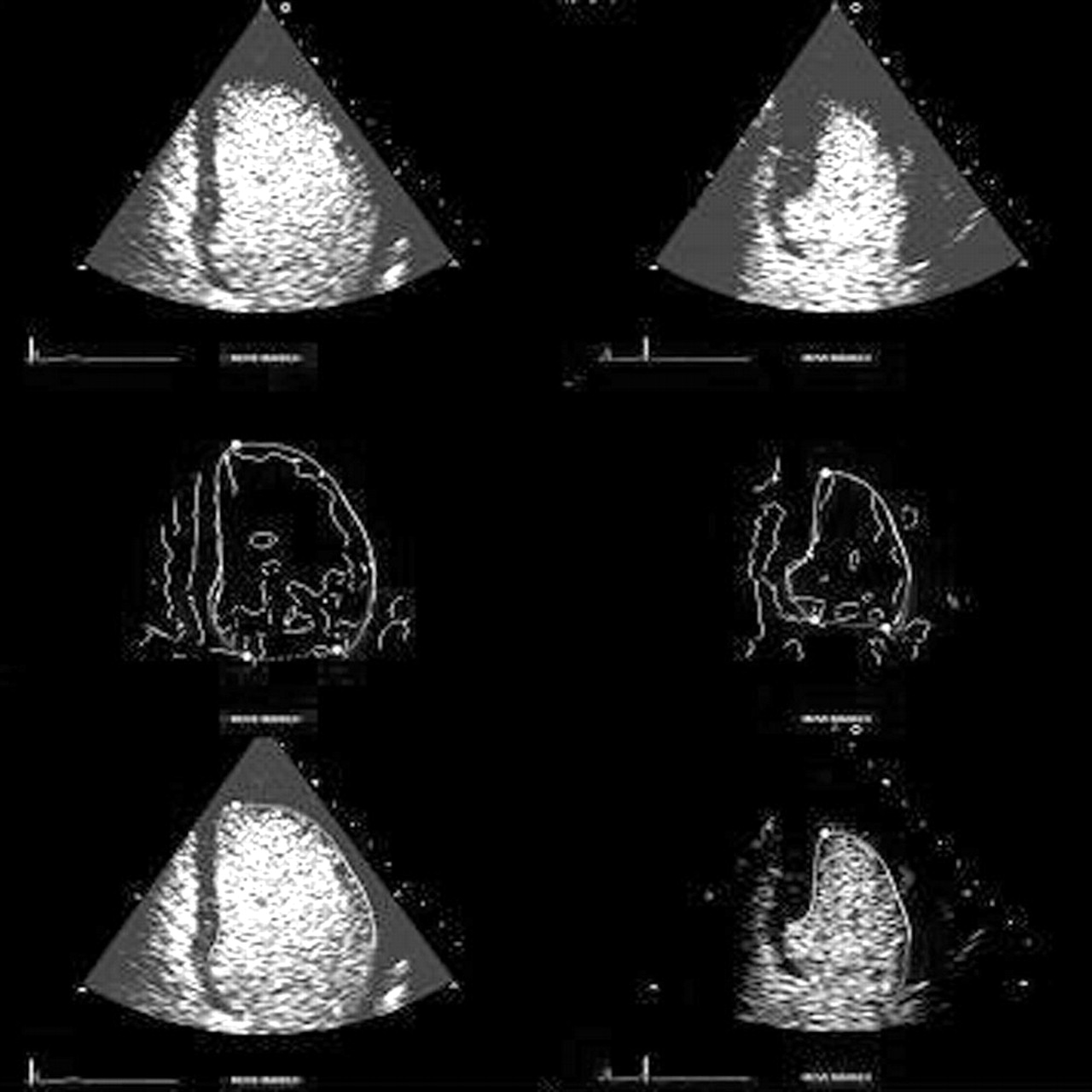
Abstract 097.
098 MULTIPLANE IMAGING FOR TREADMILL STRESS ECHOCARDIOGRAPHY: DOES REDUCED IMAGING TIME MEAN REDUCED IMAGE QUALITY?
T. Stuart, S. Kapatenakis, E. Ho, M. Monaghan.King’s College Hospital, London, UK
Introduction: Treadmill stress echocardiography is a widely used, well validated technique for the assessment of suspected coronary disease. Due to the rapid fall in heart rate (HR)/myocardial demand following exertion, up to 40% of ischemic wall motion abnormalities can resolve before sequential scan plane acquisition is complete. Recently developed matrix transducers allow the simultaneous acquisition of two imaging planes from a single precordial position (biplane (BP) imaging). This study investigated the affect of BP imaging on acquisition time and image quality in an unselected group of outpatients referred with chest pain.
Methods: 100 patients were randomly allocated to either BP or single plane (SP) imaging. The acquisition time and heart rate for apical 4, 2 chamber and parasternal long, short axis planes was recorded. Blinded analysis of the images was performed.
Results: There was no difference between the groups in terms of age, gender, resting heart rate, peak heart rate, or heart rate at first image. Total image acquisition time was significantly less for the BP group and end-image heart rate significantly higher (78+/−4 v 89 = +/−6 seconds, p = 0.03; 71% v 63% age predicted maximum HR, p = 0.01). There was a significant difference between modalities in terms of subjective image quality. There was no difference between the methods in terms of scans regarded as uninterpretable.
Conclusion: Biplane stress echocardiography, in the clinical setting, reduces scanning time and allows image acquisition at higher heart rates albeit at the expense of a reduction in subjective image quality without an increase in uninterpretable segments. This has the potential of improving the sensitivity of stress echocardiography.
matrix transducers; stress echo; treadmill
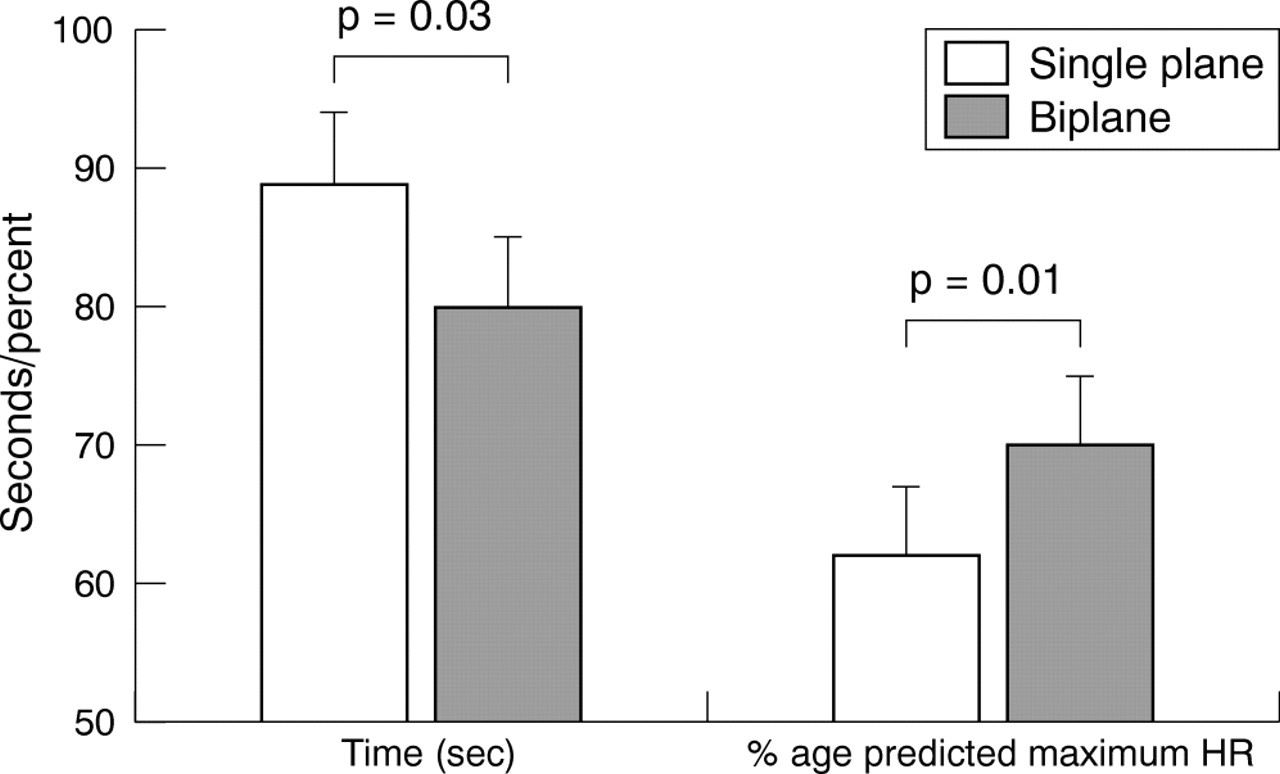
Abstract 098.
099 EFFECT OF STRESS ON DYSSYNCHRONY IN NORMAL INDIVIDUALS
S. Chattopadhyay1, C. Madler2, N. Payne2, G. Derumeaux3, A. Fraser2.1University Hospital of Wales, Cardiff, UK; 2University of Wales College of Medicine, Cardiff, UK; 3Hopital Charles Nicolle, Rouen, France
Introduction: Intraventricular mechanical dyssynchrony is common in patients with heart failure and left ventricular systolic dysfunction and dyssynchrony on exercise may contribute to symptoms and be a target for revascularisation. But the effect of stress has not yet been reported in a large, well characterised, normal white population.
Method: 105 subjects (55.9 (10.4) years, 50.5% male) from the MYDISE study with non-cardiac chest pain and low probability of IHD without history of myocardial infarction, diabetes or hypertension, with normal clinical examination, ECG, echocardiogram, dobutamine stress echocardiogram (DSE), and angiogram were recruited. Colour tissue Doppler images were acquired in the apical 4 and 2 chamber views for two cardiac cycles. Times to peak velocity (Ts) were measured from the onset of the QRS complex to the peak of the systolic velocity in eight non-apical segments of the septal, lateral, anterior, and inferior walls at rest and all stages of the DSE (5, 10, 20, 30, 40 μg/kg/min and after atropine if required). Ts were corrected for the heart rate using the Bazett’s formula (Ts-cor). Standard deviation of Ts (Ts-SD) and Tscor (Tscor-SD) and the difference between maximum and minimum Ts (Tsdiff) and Tscor (Tscordiff) measured eight non-apical were measured. Student’s t test was used to compare continuous variables. p<0.05 was considered significant.
Results: The Ts and Tscor of each segment shorten (fig) and Ts-SD, Tscor-SD, Tsdiff, and Tscordiff decrease (table) with stress.
Abstract 099
Conclusion: In a well characterised population of normal individuals, the times to peak velocity shorten and the dyssynchrony indices reduce with stress. This may form the basis assessing dyssynchrony in patients at rest and stress.
dyssynchrony; stress echocardiography; mydise
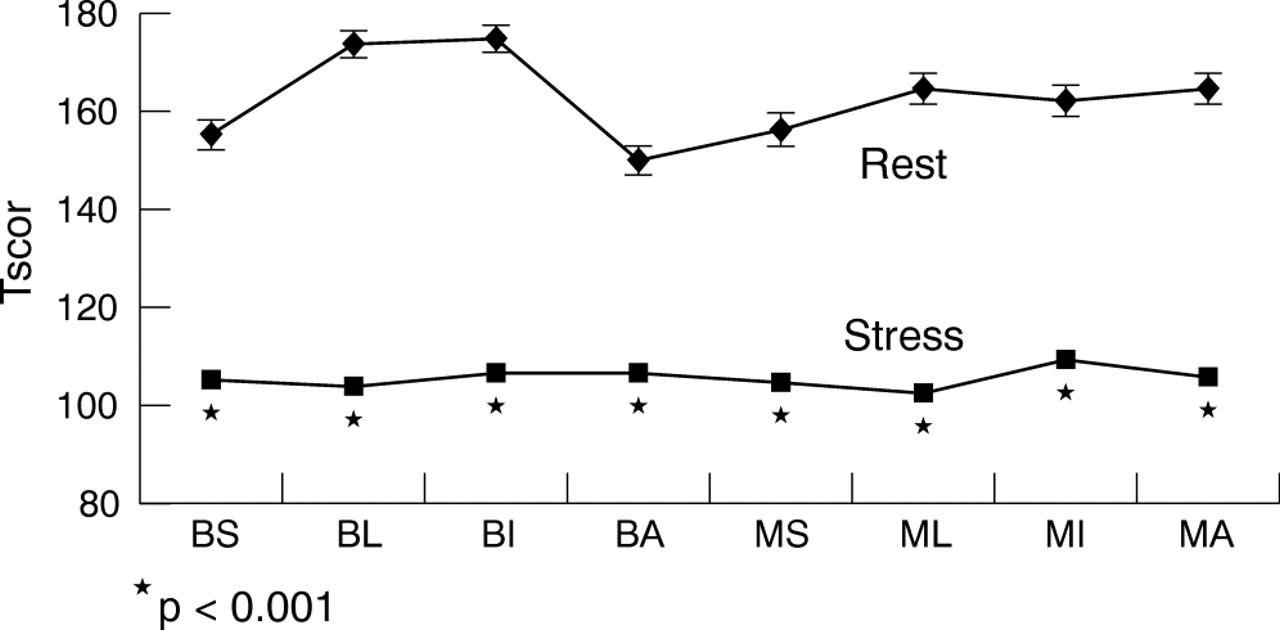
Abstract 099.
100 VASODILATOR MYOCARDIAL CONTRAST ECHOCARDIOGRAPHY IS SUPERIOR TO BOTH TIMI RISK SCORE AND EXERCISE ELECTROCARDIOGRAPHY FOR RISK STRATIFYING PATIENTS PRESENTING TO THE HOSPITAL WITH ACUTE CHEST PAIN AND NEGATIVE TROPONIN
P. Jeetley, L. Burden, K. Greaves, R. Senior.Northwick Park Hospital, Harrow, UK
Background: Vasodilator myocardial contrast echocardiography (MCE) is a new bedside technique that facilitates the diagnosis of coronary artery disease (CAD). We hyopthesised that vasodilator MCE will be superior to both TIMI risk score and exercise electrocardiography (ExECG) to risk stratify patients with coronary risk factors presenting to hospital with acute chest pain, non-diagnostic ECGs, and negative 12 hour troponin.
Methods: All subjects underwent standard clinical tests for risk stratification. Subsequently low power MCE was performed using SonoVue as a continuous infusion at rest and following vasodilator stress. Patients were recommended management plans by treating physicians, blinded to MCE results on the basis of standard tests for risk stratification.
Results: Of a total of 148 patients undergoing MCE, at a median of nine days after admission, follow up data were obtained in 145 patients at 8 (SD 5) months. Of the 27 patients with abnormal MCE 16 (59%) had cardiac events (death, acute myocardial infarction and revascularisation) compared to only eight (7%) out of 118 (p<0.0001) who had normal MCE. Hard cardiac events were only four (3%). Cardiac events in patients with normal v abnormal MCE in the low risk TIMI were 0/25 (0%) v 2/3 (66%), p<0.0001, in the intermediate TIMI group were 6/86 (7%) v 13/22 (59%), p<0.0001 and in the high risk group were 2/7 (29%) v 1/2 (50%), p = NS. Of the patients undergoing ExECG (88 patients), 86 patients had follow up data. Cardiac events in pts with normal vs abnormal MCE in patients with ischaemic ECG were 2/7 (29%) v 7/7 (100%), p = 0.005), in patients with no ECG changes were 4/63 (6%) v 5/7 (71%), p<0.0001.
Conclusions: MCE accurately classified patients presenting to the hospital with coronary risk factors but troponin negative chest pain into high and low risk groups. A normal MCE confers an excellent prognosis in such patients. Furthermore, MCE provided incremental information over TIMI risk score and was superior to ExECG.
contrast echocardiography; acute coronary syndrome; electrocardiography
101 IDENTIFICATION OF HIBERNATING MYOCARDIUM: CAN MYOCARDIAL CONTRAST ECHOCARDIOGRAPHY REPLACE SINGLE-PHOTON EMISSION COMPUTED TOMOGRAPHY?
M. Hickman, C. Kinsey, L. Burden, R. Senior.Northwick Park Hospital, Harrow, UK
Background: Prediction of hibernating myocardium in patients with ischaemic cardiomyopathy has both prognostic and therapeutic implications. Myocardial contrast echocardiography (MCE) is a new bedside technique that can assess microvascular perfusion thus hibernating myocardium during a single breath-hold. We hypothesised that MCE, by virtue of its temporal and spatial resolution, would at least be equivalent to single-photon emission tomography (SPECT) for the assessment of hibernating myocardium in this patient group.
Methods: Accordingly, 27 patients (aged: 68 (SD 4) years; LVEF = 30 (10)%) scheduled for revascularisation with symptomatic ischaemic cardiomyopathy, underwent simultaneous resting MCE with SonoVue infusion and 99mTc-Sestamibi SPECT. All scans were reported independently of one another by blinded experts using a 17 segment left ventricular model using a semi-quantitative score (1 = normal; 4 = absent for MCE and 0 = normal and 4 = absent for SPECT). A perfusion score index was also calculated. Hibernating myocardium was assessed in all segments that were akinetic at baseline (MCE score ⩽3; SPECT SCORE <3) and determined to be truly present when either there was improvement in resting systolic function, or the presence of contractile reserve with low dose dobutamine, 3–6 months following revascularisation. In addition, to assess global function, a wall motion score index was calculated for each patient at baseline and follow up.
Results: Of the 147 segments that were akinetic at rest, 102 (69%) were deemed viable at follow up. MCE and SPECT detected Hibernating myocardium with sensitivities of 85% and 82% and specificities of 55% and 49%, respectively (p = NS). Both MCE and SPECT scores were significantly (p<0.0001) worse in non-viable segments (3.3 (SD 0.9)) and (2.1 (1.46)) compared with hibernating myocardium (2.1 (1.06)) and (1.0 (1.36)), respectively. Homogenous MCE perfusion predicted hibernating myocardium in 36 (95%) out of 38 akinetic segments. Linear regression analysis demonstrated a significant relationship between an improvement in wall motion score index and perfusion score index with MCE (p = 0.024) but not SPECT.
Conclusions: MCE is a bedside test that has comparable accuracy to SPECT at detecting hibernating myocarium in ischaemic cardiomyopathy at segmental level, but was superior to SPECT for the prediction of global hibernating myocardium.
myocardial hibernation; contrast echocardiography; heart failure
102 ACCURACY OF LOW POWER CONTRAST ECHOCARDIOGRAPHY FOR THE ASSESSMENT OF LEFT VENTRICULAR REMODELLING COMPARED WITH SINGLE-PHOTON EMISSION COMPUTED TOMOGRAPHY FOLLOWING ACUTE MYOCARDIAL: COMPARISON WITH CARDIOVASCULAR MAGNETIC RESONANCE IMAGING
T. Lim1, L. Burden1, R. Janardhanan1, G. Dwivedi1, P. Chai2, J. Moon2, D. Pennell2, R. Senior1.1Northwick Park Hospital, Harrow, UK; 2Royal Brompton Hospital, London, UK
Background: Assessment of left ventricular remodelling following acute myocardial infarction (AMI) has both therapeutic and prognostic implication. Low power contrast echocardiography has the advantage of simultaneously assessing myocardial perfusion and left ventricular remodelling. We aimed to evaluate the accuracy of low power contrast echocardiography to assess left ventricular remodelling following AMI compared with Technetium-99m sestamibi gated single photon emission computed tomography (SPECT).
Methods: Accordingly, 36 consecutive patients underwent SPECT, CE (SonoVue) and cardiovascular magnetic resonance imaging (CMR) 7–10 days after AMI. Left ventricular ejection fraction (LVEF), left ventricular end-systolic volume (LVESV) and left ventricular end-diastolic volume (LVEDV) were assessed.
Results: Absolute differences for LVEF and LVEDV between CMR and contrast echocardiography were significantly smaller than that between CMR and SPECT (table). Contrast echocardiology estimate of LVEF more accurately classified patients into LVEF<35%, 35–45%, >45% (agreement = 83%, κ = 0.66 with CMR) compared with SPECT (agreement = 61%, κ = 0.36 with CMR).
Abstract 102
Conclusion: Low power contrast echocardiography agrees more closely with CMR as compared with gated SPECT for the estimation of left ventricular remodelling after AMI.
echocardiography; SPECT; left ventricular remodelling
103 REDUCED SEPTAL WALL THICKNESS NOT HYPOPERFUSION IS THE CAUSE OF PERFUSION DEFECTS ON SINGLE PHOTON EMISSION COMPUTED TOMOGRAPHY IN PATIENTS WITH LEFT BUNDLE BRANCH BLOCK WITHOUT CORONARY ARTERY DISEASE: COMPARISON WITH MYOCARDIAL CONTRAST ECHOCARDIOGRAPH
S. Hayat, G. Dwivedi, T. Lim, A. Jacobsen, R. Senior.Northwick Park Hospital, Harrow, UK
Background: Complete left bundle branch block (LBBB) may be associated with organic heart disorders including ischaemic heart disease. Perfusion abnormalities have been noted to occur both at rest and during vasodilator stress on single photon emission computed tomography (SPECT) even in the absence of flow limiting coronary artery disease (CAD). The mechanism underlying this remains unclear. We hypothesised that the likely mechanism of such defects could be due to partial-volume effect rather than true myocardial perfusion abnormalities.
Methods: Accordingly 24 patients (mean age 66 (SD 8) years, mean LVEF (43 (18) %) with LBBB and no evidence of flow limiting CAD on coronary arteriography underwent 2D echocardiography, and simultaneous vasodilator 99mTc-sestamibi SPECT and myocardial contrast echocardiography (MCE). Patients were assessed for left ventricular volumes (systolic and diastolic), left ventricular ejection fraction (LVEF), and left ventricular wall thickness (septal and posterior walls) on 2D echocardiography. Myocardial perfusion was assessed by MCE using a destruction-replenishment low power technique during Sonovue infusion. Perfusion defects, both at rest and stress, were scored by independent blinded observers on a matching 17 segment left ventricular model for both imaging modalities.
Results: Of the 24 patients only one demonstrated a perfusion abnormality on MCE compared with 10 (42%) undergoing SPECT (p=0.02). Of these 10 patients nine demonstrated septal perfusion abnormalities. MCE demonstrated normal perfusion in all these 10 patients. Among the 2D echocardiography parameters assessed only interventricular septal wall thickness was significantly (p=0.01) lower (0.99 ((0.08) cm) in patients with SPECT perfusion defects compared with those without (1.19 (0.23) cm). There was no significant difference in posterior wall thickness, LVEF and left ventricular volumes between those with or without perfusion defects.
Conclusions: : SPECT perfusion abnormalities are common in patients with LBBB without CAD in absence of true myocardial perfusion defects as assessed by MCE. The likely explanation of this defect appears to be a partial volume effect.
104 MYOCARDIAL VELOCITIES DURING DOBUTAMINE STRESS ECHOCARDIOGRAPHY FOR CORONARY ARTERY DISEASE DIAGNOSIS AND PREDICTING MORTALITY IN END STAGE RENAL DISEASE: A TISSUE DOPPLER IMAGING STUDY
R. Sharma1, S. Brecker1, D. Gaze1, P. Collinson1, R. Mehta2, D. Pellerin3.1St Georges Hospital, London, UK; 2Southampton General Hospital, Southampton, UK; 3The Heart Hospital, London, UK
Background: Dobutamine stress echocardiography (DSE) is advocated for coronary artery disease (CAD) diagnosis in end stage renal disease (ESRD). However, the technique is limited by image quality and subjective interpretation of regional wall motion abnormalities (RWMA). This study aimed to determine whether a quantitative tissue Doppler measurement of peak systolic velocity (PSV) during DSE predicts severe CAD and mortality in patients with ESRD.
Methods: 140 renal transplant candidates (mean age 52 (12) years, 90 male, mean creatinine 608 (272) mmol/l) were studied prospectively. A standard DSE protocol was used. An ischaemic response defined by the development of a new RWMA in one or more resting normal segments or deterioration of wall motion score in one or more resting hypokinetic segments. Colour tissue Doppler images (TDI) were acquired in digital cine-loop format. The mean PSV in the basal and mid segments of apical 2, 3, 4 chamber views were measured off-line by an independent operator. Mean PSV was compared with visual wall motion and the presence of severe CAD at coronary angiography (defined as luminal stenosis in one or more coronary artery >70% by visual estimation).
Results: 41 (30%) patients developed an ischaemic response during DSE and 40 patients (29%) had severe CAD. Out of 1661 segments analysed, 138 demonstrated an ischaemic response during DSE as determined by visual analysis. Segments identified as having normal and abnormal wall motion showed significant differences in mean PSV (8.1 (3.6) cm/s and 5.6 (− 3.1) cm/s respectively; p = <0.001). Mean PSV increased >100% in those segments without an ischaemic response compared with a 40–70% rise in ischaemic segments. From Receiver Operator Characteristic curve analysis, failure of the baseline PSV to rise by 50% predicted an ischaemic response with sensitivity 86% and specificity 90% (Area Under Curve 0.79, p = 0.01). Using this TDI cut off value, 42 (31%) patients developed ischaemia during DSE. The sensitivity, specificity and accuracy values for visual analysis of DSE to detect severe CAD were 86%, 92% and 89%. The same values for TDI assessment were 88%, 93%, and 90%, respectively. There were 21 deaths over a mean follow-up period of 2.2 (0.7) years. A positive DSE result, as defined by TDI analysis, was associated with significantly increased mortality (p = 0.001, log rank test).
Conclusion: A fully quantitative interpretation of DSE, using tissue Doppler velocities, accurately predicts severe CAD and mortality in patients with ESRD.
tissue doppler imaging; dobutamine stress echocardiography; end stage renal disease
105 AN ECHOCARDIOGRAPHY DERIVED PROGNOSIS SCORE TO PREDICT MORTALITY AFTER RENAL TRANSPLANTATION
R. Sharma1, E. Chemla1, M. Tome2, S. Brecker1, R. Mehta3, D. Pellerin2.1St Georges Hospital, London, UK; 2The Heart Hospital, London, UK; 3Southampton General Hospital, Southampton, UK
Background: Cardiovascular disease is the leading cause of death after renal transplantation. The aim of this prospective observational study was to identify preoperative parameters that best predict mortality after renal transplantation in a group of patients with end stage renal disease (ESRD).
Methods: 203 renal transplant recipients (mean age 47 (SD 12) years, 141 male, mean creatinine 745 (382) mmol/l, 183 on dialysis) were prospectively studied over a mean follow-up time period of 3.6 (1.8) years after transplantation. Clinical, biochemical, echocardiography and exercise test data were collected prior to renal transplantation. The primary end point was all-cause mortality.
Results: There were 22 deaths over the follow-up period, 12 of which were cardiac. Non survivors were significantly older (p< = 0.001), had larger left ventricular end systolic (LVESD) diameter (p = <0.001) and end diastolic (LVEDD) diameter (p = <0.001), and lower left ventricular ejection fraction (p = <0.001) when compared with survivors. Left ventricular mass index (p = 0.001), left ventricular maximal wall thickness (LVMWT, p = 0.006) and the proportion of patients with mitral annular calcification (MAC, p = 0.001) were all significantly higher in the non survivors. Traditional cardiovascular risk factors, exercise test data, serum haemoglobin, creatinine, the proportion on dialysis were not significantly different in the two groups. Multivariate analysis by Cox regression techniques identified four preoperative independent predictors of mortality after renal transplantation: age >50 years (p = 0.002), LVESD >3.5 cm (p = 0.002), LVMWT >1.4 cm (p = 0.014), and MAC (p = 0.036). There was a progressive decrease in survival with an increasing number of prognostic risk factors. Patients with no prognostic factor had an estimated 5-year survival rate of 96%. The corresponding 5-year estimates for 1, 2 and 3 prognostic factors were 86%, 68% and 38%. None of the patients had four prognostic factors.
Conclusions: Preoperative age >50 years, LVESD >3.5 cm, LVMWT >1.4 cm and the presence of MAC are independent predictors of mortality after renal transplantation. A model based on a combination of these risk factors is a better predictor of outcome than any single parameter.
prognosis score; renal transplantation; mortality
106 RESCUE ANGIOPLASTY V CONSERVATIVE MANAGEMENT FOR FAILED FIBRINOLYSIS IN ACUTE MYOCARDIAL INFARCTION: A META-ANALYSIS
B. Kunadian, K. Vijayalakshmi, D. Muir, A. Sutton, R. Wright, J. Hall, M. de Belder.The James Cook University Hospital, Middlesbrough, UK
Background: Individual trials of rescue angioplasty were not powered to detect a mortality advantage or difference in the individual end points. We therefore performed a meta-analysis of the available 30-day and 6-month outcome results of the randomised trials comparing rescue angioplasty with conservative management for failed thrombolysis.
Methods and results: We identified five clinical trials including 800 patients and mean follow-up time of 30 days. At 30 days rPCI was associated with a significant benefit for reduced rates of death (OR 0.64; 95% CI 0.41 to 1; p = 0.048), reinfarction (OR 0.48; 95% CI 0.25 to 0.94; p = 0.033) and additional unplanned revascularisation (OR 0.37; 95% CI 0.22 to 0.63; p = <0.01) and a non-significant trend towards reduction in heart failure (OR 0.72; 95% CI 0.51 to 1.01; p = 0.06). Rescue angioplasty was associated with more strokes (OR 3.81; 95% CI 1.09 to 13.25; p = 0.04). The combined analysis of the results from the MERLIN and the REACT trial showed no mortality benefit at 6 months (OR 0.68; 95% CI 0.39 to 1.19).
Conclusion: This meta-analysis suggests that rPCI compared with CM results in reduced mortality at 30 days, less reinfarction, and less unplanned intervention, but an increased rate of strokes. A reduction in heart failure has not been conclusively established. At 6 months, the current available information does not confirm mortality benefit with rescue angioplasty. Although it is reasonable to offer rescue angioplasty to suitable patients, a larger randomised study is required.
STEMI; rescue angioplasty; meta-analysis

Abstract 106
107 THE COST-EFFECTIVENESS OF PRIMARY ANGIOPLASTY COMPARED WITH THROMBOLYSIS FOR THE TREATMENT OF ACUTE MYOCARDIAL INFARCTION
Y. Bravo, C. Asseburg, S. Palmer, E. Fenwick, M. Sculpher.Centre for Health Economics, York, UK
Objectives: To evaluate the cost-effectiveness of primary angioplasty v hospital-administered thrombolysis for patients with acute myocardial infarction, using a Bayesian approach.
Methods: A probabilistic model was developed to evaluate the life-term cost-effectiveness of primary angioplasty. A UK NHS perspective was adopted with outcomes estimated using Quality-Adjusted Life Years (QALYs). Evidence on short-term event rates was obtained by updating a recent meta-analysis of randomised trials comparing angioplasty with thrombolysis (Lancet 2003;361:13–20). A Bayesian random-effects meta-regression model was used to fit the aggregated data from the 22 trials. This approach enabled the simultaneous estimation of posterior distributions and correlation structure for: (1) major cardiovascular events including death, re-infarction and stroke and (2) different time endpoints (1 month and 6 months). The impact of PCI time-delay to treatment was analysed using mean time delay compared with initiation of treatment with thrombolytics. Long-term costs and QALYs were estimated using a Markov model populated from UK registry data.
Results: For all outcomes, the mean probability of an event occurring is lower for patients randomised to primary angioplasty. Angioplasty significantly reduces one month mortality for the observed average time-delay in the trials (54 min; OR 0.68; 95% CI 0.46 to 1.01). For non-fatal re-infarction, the odds ratio is 0.32 (95% CI 0.20 to 0.51); and for non-fatal stroke it is 0.24 (95% CI 0.11 to 0.50). Statistically significant benefits on 6 month mortality due to angioplasty are seen for delays up to 45 minutes and for non fatal outcomes up to 90 min (OR 0.55; 95% CI 0.29 to 1.27 for reinfarction; OR 0.79; 95% CI 0.08 to 1.43 for stroke). Based on the average time delay reported in the trials, primary angioplasty resulted in a mean gain of 0.29 QALYs and an additional cost of £2680 compared with thrombolysis. The associated incremental cost-effectiveness ratio (ICER) was £9241 per QALY. At conventional levels of cost-effectiveness considered by UK decision makers to provide value for money to the NHS (aproximately £30 000 per QALY), the probability that primary PCI is cost-effective is 0.95. Adjusting the time delay resulted in considerable variation in the cost-effectiveness estimates. For a shorter delay of 30 min the ICER was £6850 per QALY; increasing the time delay to 90 min resulted in a marked increase in the ICER to £64 750 per QALY (99% and 45% probability of being cost-effective at £30 000, respectively).
Conclusions: Primary angioplasty is shown to be cost-effective for delays up to 60 min in a UK decision context. This study also demonstrates the importance of time delay when considering the cost-effectiveness of primary angioplasty, and the advantages of using Bayesian approaches to model multiple endpoints, treatment effects and baseline event rates.
primary angioplasty; cost-effectiveness; time-delay
108 COMPARISON BETWEEN MIDDLESBROUGH EARLY REVASCULARISATION TO LIMIT INFARCTION TRIAL (MERLIN) AND RESCUE ANGIOPLASTY V CONSERVATIVE THERAPY OF REPEAT THROMBOLYSIS (REACT) TRIALS: 6 MONTHS RESULTS
B. Kunadian, K. Vijayalakshmi, A. Sutton, D. Muir, R. Wright, J. Hall, M. de Belder.The James Cook University Hospital, Middlesbrough, UK
Background and Methods: Randomised trials of rescue angioplasty (rPCI) have seemingly variable results. We compared the demographic and logistical results of the Middlesbrough early revascularisation to limit infarction trial (MERLIN) and rescue angioplasty v conservative therapy of repeat thrombolysis (REACT) trials to identify possible results for the different outcomes.
Results: Streptokinase was used more commonly in the MERLIN trial 96% v 60% in REACT. The patients in the MERLIN trial were older (63 v 61 years). The recruitment rate in MERLIN was 30.7 patients per centre per year v 3.3 in REACT. In the rPCI arm, time from symptom to lysis was longer in MERLIN (170 v 140 min), but lysis to angiography time shorter (140 v 274 min), with a longer mean treatment time (327 v 414 min). In the conservative arms, 6-month mortality was greater in REACT (18% v 12%); 25% in MERLIN underwent unplanned revascularisation v 20.7% in REACT. In the rPCI arm, reinfarction rates were higher in MERLIN (7.8% v 4%), possibly because of lower rates of stenting (50.3% v 87.5%) and use of glycoprotein IIb/IIIa inhibitors (3.3% v 55.4%). There were more strokes in the conservative arm of the REACT trial (4%) compared with 1.3% in the MERLIN trial. Thus, the greater incidence of strokes seen in the rescue arm of the MERLIN trial might have been the result of unexpectantly lower rates of strokes in its conservative arm. The two trials used different definitions of heart failure.
Conclusion: These trials differ in various aspects. The MERLIN trial is widely applicable to patients receiving streptokinase and had no age limit. REACT patients were younger and were enrolled more selectively. Although some outcomes were similar, differences in patients recruited and the protocols may have accounted for the different mortality rates at 6 months.
Abstract 108
STEMI; PCI; rescue angioplasty
109 3 MONTH CLINICAL OUTCOME OF DRUG-ELUTING STENTS IN RESCUE ANGIOPLASTY
T. Wells, N. Curzen, A. Calver, I. Simpson, H. Gray, K. Dawkins.Southampton University Hospital, Southampton, UK
Introduction: Current European and US guidelines recommend rescue percutaneous coronary intervention (PCI) as the treatment of choice for patients with ST-elevation myocardial infarction (STEMI) who fail to reperfuse with thrombolysis or develop cardiogenic shock. There are limited “real-world” data on the use of drug-eluting stents (DES) in the setting of rescue PCI for failed thrombolysis.
Methods: We analysed the records of 112 consecutive patients who underwent rescue PCI, within 24 hours of failed thrombolysis, using the paclitaxel-eluting TAXUS stent between May 2003 and May 2005. All patients received both aspirin and clopidogrel prior to their intervention followed by maintenance dual anti-platelet therapy post-procedure. Adjunctive glycoprotein IIb/IIIa inhibitor (GPIIb/IIIa) therapy was given at the discretion of the operator.
Results: Mean age was 60.9 (SD 10.4) years. Seventy nine per cent were male, 36% hypertensive, 37% current smokers, 79% had dyslipidaemia, 13% had diabetes and 3% had either previous PCI or coronary artery bypass grafts. The mean time from diagnosis of failed reperfusion to balloon inflation was 226 (224) min (range 15 to 1344). A total of 169 stents were inserted, mean 1.5 stents per patient, with a mean stented segment length of 24.3 (10.0) mm (range 12 to 52). 7.1% of patients were in cardiogenic shock at the time of procedure. Multivessel disease (significant lesions of ⩾70% in non-infarct related artery) was present in 40 patients (35.7%) of whom eight had total revascularisation. Pre-procedure, 38.4% had TIMI-0 flow and post-procedure TIMI-3 flow was achieved in 87.5%. Intra-luminal thrombus was identified in 82.1% of cases. In 65.2% the culprit vessel was the left anterior descending artery. Direct stenting was carried out in 21.4%. Adjunctive GPIIb/IIIa therapy was given in 95.5%. Six patients (5.4%) died in hospital; three from cardiogenic shock, one from pneumonia and two as a direct result of bleeding complications (one acute intracerebral bleed and one uncontrolled internal haemorrhage from the site of vascular access with subsequent multi-organ failure). In all, 11.6% had bleeding complications (4.5% major and 7.1% minor). No patient had reinfarction or required further target lesion revascularisation (TLR) prior to discharge. At follow up, mean duration of 106 (60) days, there were no further deaths, reinfarction or TLR. Two patients (1.9%) with angina required intervention to a non-infarct related vessel identified at the time of initial angiography. Thus, both actuarial and MACE-free survival was 94.6%.
Conclusions: Use of the paclitaxel-eluting TAXUS stent in the highly thrombogenic setting of an acute STEMI and rescue PCI is safe with no incidence of acute stent thrombosis. However, the risk of bleeding is relatively high in such patients who have received thrombolysis, anti-platelet therapy and adjunctive GPIIb/IIIa therapy.
ST-elevation myocardial infarction; rescue angioplasty; drug-eluting stents
110 NO LATE BENEFIT OF RESCUE ANGIOPLASTY v conservative treatment in patients with failed fibrinolysis: final results of the Middlesbrough early revascularisation to limit infarction (MERLIN) randomised trial
B. Kunadian1, A. Sutton1, K. Vijayalakshmi1, P. Campbell1, R. Graham1, D. Price1, J. Gray1, E. Grech1, J. Hall1, A. Harcombe1, R. Wright1, R. Smith2, A. Shyam-Sundar2, M. Stewart1, A. Davies1, N. Linker1, M. de Belder1.1The James Cook University Hospital, Middlesbrough, UK; 2North Tees Hospital, Stockton, UK
Background: 30-day and 6-month outcomes in trials comparing rescue angioplasty (rPCI) with conservative treatment for failed fibrinolysis complicating ST segment elevation myocardial infarction (STEMI) have shown variable results. Whether early rPCI confers late (up to 3 years) clinical benefits is not known.
Methods: The MERLIN trial compared rPCI and a conservative strategy in patients with failed fibrinolysis complicating STEMI. Thirty day and 1 year results have been reported. Results to 3 years follow up are presented. Patients in cardiogenic shock were excluded.
Results: 3-year mortality in the rPCI and conservative arms, respectively was 17.6% v16.9%; p = 0.86; risk difference (RD) −0.76%; 95% confidence interval (CI) −9.3 to 7.8. Death rates were similar (3.9% v 3.3%) between 1 and 3 years follow up. The composite end point occurred less often in the rPCI arm (51% v 64.3%; p = 0.02; RD 13.3%; 95% CI 2.2 to 24.1). There was no significant difference in the rate of reinfarction (1.3% v 3.9%) or heart failure (1.3% v 2.6%) between 1 and 3 years. The incidence of subsequent unplanned revascularisation at 3 years was higher in the conservative arm (32.5% v 14.4%; p<0.01; RD 18.1%; 95% CI 8.7 to 27.3), most of which occurred by 30 days; the rates between 1 and 3 years was 2.6% in the conservative v 2% in the rPCI arm. There was a trend towards fewer strokes in the conservative arm at 3 years (2.6% v 6.5%; p = 0.98; RD −3.9%; 95% CI −9.4 to 0.8), with similar stroke rates (1.3% v 1.3%) between 1- and 3-year follow-up.
Conclusion: Early rPCI did not confer a late survival advantage at three years, compared with those managed more conservatively. The composite end point occurred less often in the rPCI arm, mainly because of fewer unplanned revascularisation procedures in the early phase of follow up. The highest risk of clinical events in patients with failed reperfusion is in the first year; beyond 1 year the occurrence of events is low.
STEMI; failed fibrinolysis; rescue angioplasty

Abstract 110
111 ADVERSE CLINICAL OUTCOME AND PROGNOSTIC FACTORS IN PATIENTS WITH NON-ST SEGMENT ELEVATION ACUTE CORONARY SYNDROMES AND ELEVATED TROPONIN T
A. Ramsewak, S. Murray, A. Dhanasekeran, A. Robinson, A. Khan, U. Velupandian, G. Viswanathan, E. Rodrigues, P. Wong.University Hospital Aintree, Liverpool, UK
Introduction: The use of troponin assays has become an integral part of clinical practice in the diagnosis and risk stratification of patients with suspected acute coronary syndromes (ACS). We compared the in-hospital and 6-month total mortality in patients who had non-ST segment elevation acute coronary syndromes (NSTEACS) and elevated troponin T (TnT) with those having ST segment elevation myocardial infarction (STEMI), and investigated the prognostic factors affecting 6-month survival.
Methods: Consecutive patients admitted to a large university hospital over an 8-week period (5 January to 29 February 2004) with elevated TnT (⩾0.01 ug/l) were identified and their case notes reviewed to confirm the diagnosis of ACS. TnT level was routinely measured at 12 hours after symptom onset.
Results: Of 195 patients with ACS and elevated TnT, 150 had NSTEACS and 45 had STEMI (ratio 3.3:1). NSTEACS patients were older (75 years (SD 12) v 67 (13); p<0.001), and had a higher Charlson’s co-morbidity score (CCS) (25/50/75th centiles 1/2/3 v 0/1/1; p = 0.001) than those with STEMI. Despite having a smaller rise in TnT (25/50/75th centiles 0.07/0.23/0.84 v 0.88/2.27/5.83 ug/l; P<0.001), in-hospital (21% v 11%; P = NS) and 6-month total mortality (33% v 13%; P<0.01) were higher in NSTEACS than STEMI patients. Univariate analysis in NSTEACS patients showed older age (p<0.001), higher CCS (p = 0.001), history of congestive cardiac failure (p<0.01) and cerebrovascular disease (<0.05) to be adverse prognostic factors for 6-month survival; whereas TnT level or severity of ACS risk score were not significant (P = NS). NSTEACS patients who were considered suitable for coronary angiography had a lower 6-month total mortality (2% v 36%; p<0.001) than those not. Of the 150 NSTEACS patients, 37 (25%) were considered suitable for coronary angiography, 63 (42%) were documented as not being suitable because of concurrent illness(es) and/or co-morbidity. These 37 patients were younger (66 (13) v 78 (10); p<0.001), had a lower CCS (0/1/2 v 1/2/3.5; p<0.001) and their ACS risk score were higher (7.8 (2.9) v 6.1 (3.1); p<0.01) than the 113 patients who were not considered suitable for coronary angiography. Stepwise logistic regression showed older age (p<0.001), not considered suitable for coronary angiography (p = 0.002) and higher CCS (p = 0.029) to be independent adverse predictors for 6-month survival in all ACS patients with elevated TnT.
Conclusions: Patients with NSTEACS had a significantly higher 6-month total mortality than those with STEMI. Age and comorbidity predicted 6-month survival better than TnT level or ACS risk score. Clinical outcome was better in those NSTEACS patients who were considered suitable for coronary angiography despite having a high ACS risk score.
Non-ST segment elevation acute coronary syndromes; Elevated troponin T; prognostic factors
112 UNDERUSE OF THROMBOLYTIC THERAPY IN ACUTE MYOCARDIAL INFARCTION AND LEFT BUNDLE BRANCH BLOCK: A CONSEQUENCE OF INACCURATE EARLY DIAGNOSIS
R. Archbold1, K. Ranjadayalan2, A. Suliman2, C. Knight1, A. Deaner3, A. Timmis1.1London Chest Hospital, London, UK; 2Newham University Hospital NHS Trust, London, UK; 3King George Hospital, Ilford, UK
Introduction: Randomised trials have shown that patients with chest pain and left bundle branch block (LBBB) benefit from thrombolytic therapy, but only if cardiac enzymes confirm acute myocardial infarction (AMI). Enzymatic data, however, are rarely available when treatment decisions are made posing a clinical dilemma to which the decision of whether or not to administer thrombolysis is central. The aim of this study was to determine rates of thrombolytic therapy administration and clinical characteristics predicting AMI in patients with LBBB.
Methods: Cross sectional cohort study of 3890 patients with chest pain requiring CCU admission. A CK-based definition of AMI ((CK) >400 iu/l) was used to conform with the evidence base for thrombolytic therapy in LBBB.
Results: 241 (6.2%) patients had LBBB with serial serum (CK) measurements available in 239 (99%). The 55 (23%) patients diagnosed with AMI had substantially higher rates of LVF (62% v 24%; p<0.0005) and hospital death (13% v 1%; p<0.0005) than patients without AMI. However, only 16 (29%) of the LBBB patients with AMI received thrombolytic therapy compared with 583 (78%) of the 747 patients with ST elevation AMI (p<0.0005). A further 19 (10%) patients without AMI also received thrombolysis. Rates of thrombolytic therapy in troponin positive and troponin negative LBBB were 8.6% and 9.0%, respectively. Fewer than half (46%) of the 35 patients with LBBB who were given thrombolysis had a discharge diagnosis of AMI. Logistic regression analysis showed that the only variable independently associated with AMI among patients with LBBB was in-hospital LVF, which carried an odds ratio for AMI of 4.32 (95% CI 1.95 to 9.57; p<0.0005).
Conclusion: Our data highlight the difficulty in making an accurate early diagnosis of AMI in patients with LBBB. This ensured that the majority of those patients with AMI failed to receive thrombolytic therapy while others without AMI were treated inappropriately. Until clinically useful markers of early myocardial infarction are available for this high risk group, we believe that the pragmatic management of patients with acute coronary syndromes and LBBB should include urgent coronary angiography with a view to the percutaneous treatment of critical coronary stenoses.
thrombolytic therapy; acute myocardial infarction; left bundle branch block
113 INTERVENTION IN ACUTE CORONARY SYNDROME IN SCOTLAND: IMPACT ON READMISSION AND MORTALITY
J. Bishop1, K. Oldroyd2, J. Craig3, I. Findlay4.1Information and Statistics Division, Scottish Executive, Edinburgh, UK; 2Western Infirmary, Glasgow, UK; 3NHSQIS, Glasgow, UK; 4Royal Alexandra Hospital, Paisley, UK
Scotland has a well developed and validated ability to track admissions to hospital and subsequent outcomes. We used data provided by the Information and Statistics Division of the Scottish Health Service to look at outcomes for 22 441 patients with a first-ever-recorded admission diagnosis of angina/acute myocardial infarction for the period 2002 to 2004. The analysis was restricted to those hospitals with more than 500 such discharges. 13.2% underwent angiography on the index admission, 9.5% underwent PCI, 2.0% CABG. 30-day mortality was 9.1% and 1-year mortality 16.3%. There were 5614 admissions to hospitals equipped to do angiography and CABG/PCI; 1498 to hospitals equipped to do angiography and PCI, 4342 to angiography-equipped only and 10 987 to the remainder “transfer hospitals”. Data were age/sex/deprivation standardised. The percentage undergoing angiography during the index admission was CABG/PCI = 23.6%, angiography + PCI = 19.5%, angiography only 8.9% and transfer hospitals 8.4%. The figures for those undergoing PCI on that admission were 15.8%, 20.9%, 4.8%, 6.4%, respectively. Subsequently, 4.8%, 8.3%, 5.7%, 7.4% were readmitted for PCI. The median time to intervention PCI was 3, 3, 8 and 13 days, respectively. The percentage undergoing CABG on the index admission was 3.9%, 1.3%, 1.7%, 1.2%, respectively with a subsequent 5.4%, 5.0%, 6.0%, 5.2% readmitted for CABG. The percentage of patients readmitted with a diagnosis of angina/AMI within 30 days was 2.5%, 2.7%, 4.9%, 4.1% and by 1 year it was 8.7%, 10.5%, 15.1%, 13.5%, respectively. The percenatge of patients readmitted and specifically coded as an emergency readmission to their index hospital at 1 year was 4.1%, 3.0%, 5.9%, 5.5% respectively. The 30-day mortality was 8.5%, 8.9%, 9.5%, 9.4%, respectively and 1 year mortality was 15.6%, 15.8%, 16.6%, 16.6%, respectively. There are clear differences in rates of investigation and outcome with the main outcome benefit being a reduced incidence of readmission with angina/AMI with higher rates of intervention. One year mortality suggests that higher intervention rates in this unselected population results in only modest benefit.
intervention; outcome; Scotland
114 INTERMITTENT LIMB ISCHEMIA DURING CORONARY ISCHAEMIA REDUCES MYOCARDIAL INFARCTION THROUGH A K-ATP DEPENDENT MECHANISM: DEMONSTRATION OF REMOTE ISCHEMIC PRECONDITIONING
M. Schmidt1, K. Sorensen2, A. Redington3, R. Kharbanda4.1Aarhus University Hospital, Aarhus, Denmark; 2Aarhus University Hospital, Skejby, Aarhus, Denmark; 3Hospital for Sick Children, Toronto, Canada; 4Papworth Hospital, Cambridge, UK
Background: Previous studies have shown that “remote preconditioning” induced by brief periods of renal, mesenteric, brain or limb ischaemia prior to prolonged myocardial ischaemia reduces myocardial infarction. One unique feature to remote or distant ischaemia stimulus is the option to administer it during the period of established coronary ischaemia and prior to reperfusion. If this concept were proved then there would be important implications for treating clinical syndromes where patients present after the onset of ischaemia.
Aim: We tested the hypotheses that cardiac protection induced by an intermittent limb ischaemia stimulus administered during coronary ischaemia (remote preconditioning, PreC): firstly, reduces infarct size; secondly, improves cardiac function, and thirdly is mediated through the K-ATP channel.
Methods: To test hypotheses one and two, 20–15 kg pigs were randomised (10 in each group) to a 40 min period of left anterior descending artery occlusion with 120 min reperfusion. PreC was four 5 min cycles of lower limb ischemia by tourniquet, during LAD occlusion. Left ventricular function was assessed using a conductance catheter and extent of infarction by tetrazolium staining. The third hypothesis was tested in a randomised study into PreC as above (n = 4) or PreC with pre-treatment by glibenclamide 0.5 mg/kg (n = 6).
Results: The extent of myocardial infarction was significantly reduced by PreC compared to control (38.3 (SD 15.4%) v 60.4 (14.3%) p = 0.004). At 120 min reperfusion there was a 3 (5)% reduction in preload recruitable stroke work in the PreC group v 38 (6)% in control (p = 0.001). The force-frequency relationship was significantly depressed at 120 min reperfusion in both groups, but the optimal heart rate was significantly lower in the control group (p = 0.04). Furthermore, there were fewer malignant arrhythmias with PreC during reperfusion (p = 0.02). The protective effects of PreC were abolished by glibenclamide (fig 1).
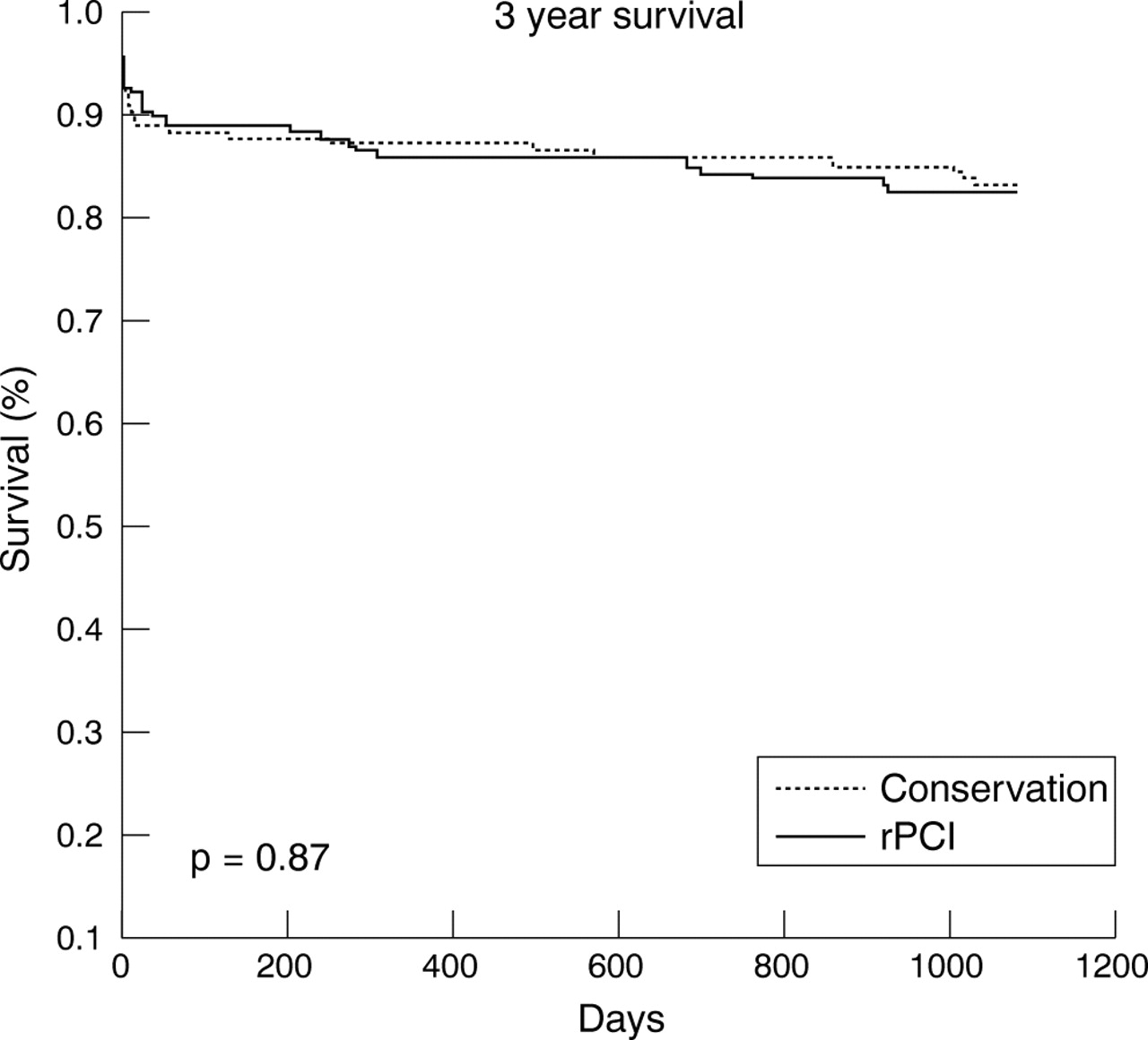
Abstract 114
Conclusion: We show that intermittent limb ischemia during myocardial ischemia reduces myocardial infarction, preserves global systolic and diastolic function, and protects against arrhythmia during the reperfusion phase through a K-ATP dependent mechanism. Understanding this process may have important therapeutic implications for a range of ischaemia-reperfusion syndromes.
ischaemia-reperfusion; remote ischaemic preconditioning; perconditioning
115 TROPONIN AND H-FABP IN THE LONG-TERM PROGNOSIS OF PATIENTS WITH ACUTE CORONARY SYNDROME
N. Kilcullen1, K. Viswanathan1, N. Artis1, K. Bailey1, C. Morrell1, R. Das1, J. Barth2, A. Hall1.1University of Leeds, Leeds, UK; 2Leeds General Infirmary, Leeds, UK
Objective: To assess the value of troponin and H-FABP as predictors of 30-day as compared with long-term all-cause mortality in patients with acute coronary syndrome (ACS).
Design: Prospective observational registry.
Setting: 11 adjacent hospitals in the West Yorkshire region.
Methods: The EMMACE-2 study included 2461 consenting patients validated to have ACS during a 6-month period (28 April 2003 to 28 October 2003). Heart-Fatty Acid Binding Protein (H-FABP), a marker of myocyte necrosis, was measured in 1449 of these patients. All had troponin measured using a single Accu TnI assay. 1165 patients with H-FABP and TnI results and all-cause mortality data were included in the analysis. Median long-term follow-up was 786 days. Patients were divided into quartiles based on the H-FABP and troponin values. Cut-offs for quartiles of H-FABP in µg/l were 6.4,12.1 and 34.1. Cut-offs for quartiles of troponin in µg/l were 0.14, 1.3 and 9.6.
Results: 30-day mortality: Troponin was a significant predictor of 30-day all-cause mortality (Quartile 4 v Quartile 1) while H-FABP was a significant predictor of 30-day mortality across all quartiles. Hazard ratios (HR) and significance with reference to quartile1 (Q1) were:
-
Troponin:Q2 HR 1.27 p = 0.43 (ns), Q3 HR 1.58 p = 0.11 (ns), Q4 HR 2.94 p<0.001
-
H-FABP: Q2 HR 5.10 p = 0.003, Q3 HR 9.50 p<0.001, Q4 HR 20.25 p<0.001
After adjusting for confounding factors using a multivariate Cox proportional hazards model (age, systolic BP, heart rate, admission glucose, admission creatinine, heart failure on admission), both troponin and H-FABP remained significant predictors of mortality [Troponin Q4 v Q1 p <0.001, H-FABP Q4 v Q1 p<0.001].
Long-term mortality: H-FABP was a significant predictor of long-term all-cause mortality across all quartiles. Troponin did not predict long-term mortality significantly (fig 1).

Abstract 115
Hazard ratios (HR) and significance (p) with reference to quartile1 (Q1) were:
-
Troponin: Q2 HR 1.02 p = 0.89 (ns), Q3 HR 1.25 p = 0.17 (ns), Q4 HR 1.33 p = 0.07
-
H-FABP: Q2 HR 3.51 p<0.001, Q3 HR 5.43 p<0.001, Q4 HR 7.01 p<0.001
After adjusting for confounding factors (age, systolic BP, heart rate, admission creatinine, heart failure on admission, gender, previous MI, previous diabetes), H-FABP remained an independent predictor of long-term all-cause mortality across all quartiles (Q2 v Q1 p = 0.003, Q3 v Q1 p<0.001, Q4 v Q1 p<0.001). H-FABP was also a significant predictor of mortality across all categories of ACS by BCS definition (ACS with unstable angina, ACS with myocyte necrosis, ACS with clinical MI).
Conclusions: H-FABP was an independent predictor of long-term mortality among all patients with acute coronary syndrome. Although troponin was valuable as a predictor of 30-day mortality following ACS, it was a poor predictor of long-term all-cause mortality.
acute coronary syndrome; mortality; heart fatty acid binding protein
116 USE OF N-TERMINAL PR0-BRAIN NATRIURETIC PEPTIDE AS A DIAGNOSTIC AND PROGNOSTIC MARKER FOR ISCHAEMIC HEART DISEASE IN PATIENTS PRESENTING TO A RAPID ACCESS CHEST PAIN CLINIC
A. Muir1, J. Neill1, K. Darragh1, J. Dougan1, C. Patterson2, A. Adgey1.1Royal Victoria Hospital, Belfast, UK; 2Queen’s University, Belfast, UK
N-terminal pro-Brain Natriuretic Peptide (NT-proBNP) is a proven diagnostic marker of congestive heart failure and predictor of recurrent ischaemic events and mortality in both stable and unstable ischaemic heart disease (IHD). Its role in diagnosing IHD and predicting outcome in patients with chest pain suggestive of IHD is yet to be established.
We hypothesised that NT-proBNP may be a useful diagnostic and prognostic marker for IHD in patients presenting with previously undiagnosed chest pain to a rapid access chest pain clinic.
Methods: NT-proBNP was measured in patients presenting to a rapid access chest pain clinic for investigation of ischaemic heart disease. NT-proBNP was compared with standard risk stratification methods combined with exercise stress testing (EST).
Results: From November 2004 to January 2005, 447 consecutive patients were studied. Seventy-three patients (16.3%) had a positive diagnosis of IHD defined as positive myocardial perfusion imaging or cardiac catheterisation on subsequent investigation. NT-proBNP (median) was significantly higher among those diagnosed with IHD v non-IHD (139 ng/l (interquartile range 69 to 311) v 45 ng/l (interquartile range 24 to 82) p<0.0001). Patients in the highest NT-proBNP quartile were older, had lower creatinine clearance and more cardiovascular risk factors than those in the lowest quartile. Patients in the highest NT-proBNP quartile were more likely to have IHD diagnosed on further investigation (p<0.0001).
Following logistic regression analysis, NT-proBNP in the highest quartile was a significant predictor of IHD, independent of risk factors, renal function, troponin I and EST (hazard ratio for the fourth quartile compared with the first was 6.6 (95% CI, 1.2 to 36.4); p = 0.019).
Patients were followed up for a mean of 9.6 (0.9) months. Fifty one (11.4%) reached a composite endpoint of death, myocardial infarction (MI) or revascularisation. NT-proBNP was significantly higher in those who met an endpoint v those who did not (166 ng/l (interquartile range 63 to 314) v 49 ng/l (interquartile range 25 to 91) p<0.0001). Kaplan-Meir curves show an increasing event rate with increasing NT-proBNP quartile (p<0.0001) (fig 1).

Abstract 116
In a multivariate Cox regression model, NT-proBNP added prognostic information beyond that of the patient’s sex, age, risk factors, electrocardiogram and biochemistry (hazard ratio for the composite endpoint for the fourth quartile compared to the first was 20.3 ((95% CI, 2.6 to 159); p = 0.002). However when EST was included in the regression model, no quartile was a significant predictor of outcome (p = 0.224).
Conclusion: In the setting of a Rapid Access Chest Pain Clinic, NT-proBNP quartile is a significant independent predictor of IHD. It is associated with the composite endpoint of death, MI and revascularisation, but does not provide better prognostic information than an EST.
N-Terminal Pro-BNP; diagnosis; ischaemic heart disease
117 N-TERMINAL B TYPE NATRIURETIC PEPTIDE IS BETTER AT PREDICTING DEATH FOLLOWING ACUTE MYOCARDIAL INFARCTION THAN THROMBOLYSIS IN MYOCARDIAL INFARCTION RISK SCORE
S. Khan, D. Kelly, P. Quinn, L. Ng.1University of Leicester, Leicester, UK
Background: The thrombolysis in myocardial infarction (TIMI) risk score is a well validated scoring system to predict mortality in patients following an ST segment elevation myocardial infarction (STEMI). N terminal B type natriuretic peptide (NT-BNP) has also been found to be useful in predicting mortality following a STEMI. We sought to investigate the utility of TIMI score and NT-BNP levels at predicting risk of death in acute myocardial infarction (AMI) patients.
Methods: We studied 308 patients (225 men, mean age 64.1 (SD 12.0) years) with AMI. Blood was drawn within the first 24 hours following the onset of chest pain and the plasma concentration of NT-BNP was determined using an in-house non-competitive immunoassay. Patients were TIMI risk scored and stratified into low (0 to 2), intermediate (3 to 7) and high risk (>8) groups.
Results: Mortality was 10.1% and was related to higher TIMI risk scores (p = 0.024 for trend). Higher NT-BNP levels were also related to increased mortality (median (range) fmol/ml, survivors 708.0 (1.2–11481.5) v dead 5754.4 (1.4–10715.2), (p<0.005). In a multivariate binary logistic regression model, the only independent predictor of mortality was NT-BNP levels in the first 24 hours (HR = 5.1, 95% CI: 0.69–0.88, p<0.0001). The receiver-operating curve for NT-BNP in the first 24 h yielded an area under the curve (AUC) of 0.79 (95% CI: 0.69–0.88, p<0.001), for TIMI risk score the AUC was 0.64 (95% CI: 0.55–0.73, p = 0.011).
Conclusion: In the first 24 hours following an AMI, NT-BNP is superior than TIMI risk scoring at predicting mortality. A simple NT-BNP blood test is more easily applicable and is more accurate than a clinical risk score.
NT-BNP; myocardial infarction; TIMI score
118 MYOTROPHIN PREDICTS RISK OF MAJOR ADVERSE CARDIAC EVENTS FOLLOWING ACUTE CORONARY SYNDROMES
S. Khan, D. Kelly, P. Quinn, L. Ng.University of Leicester, Leicester, UK
Background: Myotrophin is a 12 kD protein initially isolated from hypertrophied hearts of spontaneously hypertensive rats and acts by modulating NFkB activity. We have reported the presence of myotrophin in patients with human systolic heart failure. However its role as a predictor of major adverse cardiac events (MACE) in patients with acute coronary syndrome (ACS) is unclear. We sought to investigate this and compared it to N terminal B type natriuretic peptide (NT-BNP), a marker of MACE.
Methods: We studied 269 ACS patients (209 men, mean age 63.5 (SD 13.0) years, 75.5% STEMI, 24.5% NSTEMI). Blood measurement was made at 25–48 h after the onset of chest pain. The plasma concentration of myotrophin and NT-BNP was determined using in-house non-competitive immunoassays. Patients were followed up for the combined endpoint of death, MI or need for urgent revascularisation.
Results: Over the median follow-up period of 203 days (range 0–645) there were 26 deaths, 19 non-fatal MI and 47 patients required urgent revascularisation. Myotrophin was raised in patients with MACE compared with survivors (median (range) fmol/ml, 440.1 (116.0–7445.5) v 330.0 (51.8–6990.0), p<0.001). Using a multivariate binary logistic model myotrophin (OR 2.54, 95% CI: 1.26–5.12, p = 0.009) was the only independent predictor of MACE. This was also confirmed on the Cox proportional hazards model (HR 1.94, 95% CI: 1.17–3.20, p = 0.01). The Kaplan-Meier survival curve revealed a significantly better clinical outcome in patients with myotrophin below the median compared with those with myotrophin above the median (log rank 7.65, p = 0.006).
Conclusion: After an ACS, levels of myotrophin are more informative at predicting MACE than NT-BNP and may be useful to risk stratify patients.
Myotrophin; NT-BNP; acute coronary syndrome
119 SOLUBLE ICAM-1 AT HOSPITAL DISCHARGE AND RISK OF RECURRENT EVENTS IN ACS PATIENTS: RESULTS FROM PROVE IT-TIMI 22
K. Ray1, D. Morrow1, S. Murphy2, C. Cannon1, E. Braunwald1.1Harvard Medical School, Boston, United States; 2Brigham and Women’s Hospital, Boston, United States
Background and Aims: Higher levels of soluble ICAM-1 (sICAM-1) (a marker of endothelial activation) are associated with increased risk of cardiac events in patients with stable CAD. We assessed the relationship between sICAM-1 and acute cardiac events in the PROVE IT-TIMI 22 trial.
Methods: PROVE IT-TIMI 22 enrolled 4162 patients on average 7 days after ACS and randomised them to atorvastatin 80 mg v pravastatin 40 mg. We assessed sICAM-1 levels at study entry in 583 patients who subsequently experienced a death, myocardial infarction or recurrent ACS requiring hospitalisation (cases) and 581 matched controls who remained free of events over 2 years (matched for age, gender, history of hypertension, diabetes or smoking, presenting ACS, use for PCI for the index event and BMI) .
Results: Soluble ICAM-1 tended to be higher in cases than in controls (median and IQR), 271 ng/ml (322–235) v 264 ng/ml (312–229) p = 0.06. In a conditional logistic regression analysis using quartiles of sICAM-1, each quartile was associated with increased risk of events v quartile 1 (fig 1), with the greatest risk observed in quartile 4 (HR 1.53, 95% CI 1.05–2.22, p = 0.03). Further adjustment for statin regimen appeared to abrogate the risk associated with higher quartiles of ICAM-1, among those patients randomized to atorvastatin 80 mg. (fig 2).

Abstract 119
Conclusions: Evidence of endothelial activation approximately 7 days after ACS is associated with a high risk of recurrent cardiac events over 2 years. Intensive statin therapy appeared to diminish the risk associated with higher levels of sICAM-1.
adhesion molecules; ACS; statins
120 THE EFFECT OF ETHNICITY ON BNP LEVELS IN HYPERTENSION – AN ASCOT SUB-STUDY
A. Sharp1, J. Mayet1, D. Francis1, A. Hughes1, A. Stanton2, P. Kyd1, A. Zambanini1, N. Poulter1, P. Sever1, S. Thom1.1International Centre for Circulatory Health, St Mary’s Hospital and Imperial College, London, UK; 2Department of Clinical Pharmacology, Royal College of Surgeons of Ireland, Dublin, Ireland
Background: Measurement of B-natriuretic peptide (BNP) is rapidly becoming incorporated into the diagnostic and management algorithms for heart failure and other cardiac conditions. However, relatively little information is available on the effects of South Asian and African-Caribbean ethnicity on BNP levels, even though these groups are at elevated risk of heart failure and other cardiovascular disorders.
Methods: We measured BNP in 562 hypertensive subjects without heart failure who were part of the Hypertension Associated Cardiovascular Disease (HACVD) substudy of the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT). All subjects were recruited from a single centre and comprised 53 African-Caribbean, 42 South Asian, 28 mixed origin and 439 white subjects. Ethnic origin was confirmed with the participant, using both self assignment and country of birth of both parents.
Results: African-Caribbean subjects had significantly lower BNP levels (16.5 pg/ml) than either whites (28.5 pg/ml, p<0.0001) or South Asians (24.6 pg/ml, p = 0.02). BNP did not differ significantly by sex, presence of diabetes or smoking, and there was no correlation between BNP and ejection fraction or body surface area. However, BNP was related to age, serum creatinine and left ventricular mass index. Ethnic differences in BNP remained significant (p = 0.001) after adjustment for all of the above factors.
Conclusion: BNP differs between ethnic groups. BNP is highest in white hypertensives and lowest in hypertensives of African-Caribbean origin. These observations may have important implications for the clinical interpretation of BNP levels in hypertension.
ethnicity; natriuretic peptide; hypertension

Abstract 120
121 EVIDENCE FOR ATRIAL PRODUCTION OF B-TYPE NATRIURETIC PEPTIDE IN ATRIAL FIBRILLATION
A. Hemmings1, J. Scott2, J. Walker1, C. Sheridan1, J. Overfield3, A. Robins1, R. Egdell1.1Macclesfield District General Hospital, Macclesfield, UK; 2Macclesfield District General Hospital, Macclesfield, UK; 3University of Manchester, Manchester, UK
Background: Patients in atrial fibrillation have higher plasma levels of B-type natriuretic peptide (BNP) than matched controls, even in the absence of apparent ventricular dysfunction. Direct current cardioversion (DCC) has been shown to lead to a reduction in BNP levels, but it is unclear whether this is the result of improved ventricular function or reduced atrial production of BNP. We have investigated this further by measuring BNP before and after DCC and correlating this with echocardiographic measures of ventricular and atrial function.
Methods: Seventeen patients referred for DCC underwent BNP measurement and echocardiography before and six weeks after DCC. Heart rate was recorded. Atrial dimensions and volumes, and left ventricular ejection fraction were recorded from two dimensional echocardiography. Pulmonary capillary wedge pressure was estimated from tissue Doppler imaging. Correlation coefficients were sought between echocardiographic variables and BNP and between changes in these variables and changes in BNP levels before and after DCC.
Results: Plasma BNP fell from 167.8 (23.5) (pg/mL, mean ± SEM) to 116.2 (18.0) (p<0.05), comprising a reduction from 167.5 (31.6) to 89.9 (18.4) in those who had maintained sinus rhythm at six weeks (n = 10, p<0.05) and no significant change in those who had reverted to atrial fibrillation (168.2 (37.8) to 153.6 (31.2); n = 7, p = 0.30). Heart rate, right atrial volume and length, and left atrial length correlated significantly with BNP (r = 0.31, 0.44, 0.59 and 0.31, respectively; p<0.05, <0.01, <0.001 and <0.05, respectively). However, only heart rate, right atrial volume and ejection fraction were significantly altered by successful DCC (HR reduced from 83.2 (6.2) to 59.8 (1.6) beats per minute, p<0.01, right atrial volume from 73.3 (5.5) to 57.1 (7.1) ml, p<0.05, ejection fraction increased from 45.2 (3.7)% to 57.6 (2.8)%, p<0.01). The correlation of percentage change in a variable with percentage change in BNP was significant for right atrial volume (r = 0.61, p<0.05) but was the opposite of that expected for heart rate and ejection fraction (heart rate: r = −0.49, p = 0.08, ejection fraction: r = 0.77, p<0.01), i.e. the greater the reduction in HR the less the reduction in BNP, and the greater the increase in ejection fraction the less the reduction in BNP.
Conclusion: These data support the theory that fibrillating atria produce BNP directly rather than via impairment of ventricular performance.
B-type natriuretic peptide; atrial fibrillation; echocardiography
122 N-TERMINAL PRO-B-TYPE NATRIURETIC PEPTIDE LEVELS PREDICT MORTALITY AND CARDIAC DISEASE IN PATIENTS WITH END STAGE RENAL DISEASE.
R. Sharma1, D. Gaze1, D. Pellerin2, P. Collinson1, H. Gregson1, R. Mehta3, S. Brecker1.1St Georges Hospital, London, UK; 2The Heart Hospital, London, UK; 3Southampton General, Southampton, UK
Background: Elevated natriuretic peptide levels occur in a proportion of patients with end stage renal disease (ESRD). The aim of this study was to identify the prognostic significance and baseline characteristics of ESRD patients with raised N-Terminal Pro – B – Type Natriuretic Peptide (NT-proBNP).
Methods: 140 consecutive renal transplant candidates (mean age 52 (SD 12) years, 90 male, 79 on dialysis) were prospectively studied. All had coronary angiography, echocardiography and baseline biochemical markers.
Results: There were 21 deaths over a follow-up period of 2.2 (0.7) years. From Receiver Operator Characteristic curve analysis, NT-proBNP was predictive of mortality (AUC = 0.78, 95% CI 0.53, 0.95, p = 0.04). A cut point NT-proBNP concentration >350 pg/mL predicted mortality with sensitivity 74%, specificity 80%. Using this cut off value, patients with elevated NT-proBNP levels (n = 66) had significantly impaired left ventricular fractional shortening (31 (10)% v 41 (9)%, p = 0.04), lower peak mitral annular systolic velocity (0.06 (0.02) m/sec v 0.09 (0.02) m/sec, p = 0.01) higher left ventricular end diastolic diameter (5.1 (0.9) cm v 4.4 (0.8) cm, p = 0.04), higher left ventricular end systolic diameter (3.1 (0.8) cm v 2.5 (0.7) cm, p = 0.008), higher estimated left ventricular filling pressure (E/Ea 14 (7) v 11 (4), p = 0.03), and higher left ventricular mass index (186 (92) g/m2v 140 (48) g/m2, p = 0.03) compared with those with NT-proBNP levels <350 pg/mL. Age (55 (10) years v 49 (13) years, p = 0.02), the proportion on dialysis (64% v 48%, p = 0.004,) diabetic (60% v 27%, p = 0.09,) with severe coronary artery disease (CAD, 43% v 15%, p = 0.001) was significantly higher in those with elevated NT-proBNP. There was a significant positive correlation with cardiac troponin T concentration (r = 0.74, p = <0.001). Stepwise logistic regression analysis identified LVEDD (odds ratio 9.6, 95% CI 2.6, 21.3 p = 0.001) and left ventricular peak mitral annular systolic velocity (odds ratio −5.9, 95% CI −9.8, −2.1 p = 0.004) to be independently associated with elevated NT-proBNP.
Conclusions: NT-proBNP predicts mortality in ESRD. This is at least partly explained by those with elevated levels having reduced left ventricular systolic function, larger left ventricular cavity size, a greater proportion with diabetes and severe CAD.
natriuretic peptides; mortality; end stage renal disease
123 RANTES G–403A GENE POLYMORPHISM AND ITS IMPLICATION IN THE DEVELOPMENT OF PREMATURE CORONARY ARTERY DISEASE IN A FAMILY-BASED STUDY IN NORTHERN IRELAND
M. Kamaruddin1, P. Horan1, P. McGlinchey2, M. Spence2, G. Murphy2, T. Jardine2, C. Belton3, C. Patterson3, D. Fogarty3, P. McKeown1.1Royal Victoria Hospital/Queen’s University, Belfast, UK; 2Royal Victoria Hospital, Belfast, UK; 3Queen’s University, Belfast, UK
Purpose: The development of premature coronary artery disease (PCAD) results from accelerated atherosclerosis which has a strong inflammatory component. The C–C chemokine Regulated upon Activation, Normal T–cell Expressed and Secreted (RANTES) is a potent chemo-attractant for inflammatory cells and has been implicated in atherogenesis. Previous studies have demonstrated the association of RANTES A–403 with coronary artery disease. We investigated the influence of functional gene variants in the development of PCAD in our population.
Methods: A total of 1487 individuals were recruited (577 families: 798 discordant sib pairs and 67 parent/affected offspring trios) between August 1999 and August 2004. All subjects were white and whose parents and grandparents were born in Ireland. Probands were defined as having PCAD with disease onset ⩽55 years for males and ⩽60 years for females.
Each family was required to have at least one member affected with proven ischaemic heart disease (IHD) and at least one surviving older unaffected sibling and/or both parents surviving. IHD was defined as having one or more of the following features: a history of myocardial infarction; a history of unstable angina (typical chest pain, dynamic ECG changes and minor elevation of cardiac markers); angiographic evidence of coronary artery disease ⩾50% stenosis. Unaffected siblings were at least 3 years older than the proband, no symptoms of angina or possible myocardial infarction using the standardised “Rose questionnaire”, no history of IHD and no evidence of ischaemia on 12–lead electrocardiogram using the “Minnesota code”.
Genotyping of RANTES G–403A was performed by restriction fragment length polymorphism (RFLP) PCR. Linkage disequilibrium between the polymorphism and PCAD was tested using the pedigree disequilibrium test (PDT). 204 families were informative (295 discordant sib pairs and 42 trios).
Results: The PDT analyses of discordant sib pairs showed less occurrence of the A allele in affected sibs and marginally more transmission of the A allele to affected offsprings. The combined analyses of discordant sib pairs and trios showed a PDT sum test of Zsum = 0.90 (p = 0.37, two tailed).
Conclusion: These data suggest that RANTES A–403 polymorphism does not influence the development of PCAD in our family cohort.
RANTES; premature; coronary
124 UK NATIONAL GUIDELINES FOR DRUG ELUTING STENTS – “NICE” AT THE TIME, BUT DUE FOR AN UPDATE?
M. Cunnington, B. Kunadian, A. Thornley, A. Sutton, D. Muir, R. Wright, J. Hall, M. de Belder.James Cook University Hospital, Middlesbrough, UK
Background: National Institute for Clinical Excellence (NICE) guidance on coronary stents published in 2003 recommends drug eluting stents (DES) for lesions >15 mm long or vessel calibre <3 mm, excluding patients with acute myocardial infarction or intracoronary thrombus. NICE estimated that 1 of 3 stents used would be DES. Evidence now supports DES use in other groups at high risk of restenosis including diabetics, multi-vessel disease, in-stent restenosis (ISR), and chronic total occlusions (CTO). Our unit recommends DES for these lesions as well as proximal LAD lesions and bifurcations, with PCI for acute MI or presence of thrombus not precluding DES use.
Aim: To compare our current DES use with NICE guidance and our own criteria.
Methods: Retrospective analysis of 1000 consecutive patients undergoing PCI in our unit from 1 September 2004 to 25 July 2005.
Results: 1000 patients with 1441 lesions and 1801 stents (1255 DES) were studied (age 61.6 (10.5), 717 male, stable angina 399, acute myocardial infarction 94, other ACS 507, diabetic 145). Lesion length was 16.9 (12.2) mm (547 of 1441 >15 mm). Target artery reference diameter was 3.0 (0.6) mm (709 of 1441 <3 mm). 220 patients had proximal LAD lesions, 28 CTO, 31 ISR, 260 bifurcation lesions and 255 underwent multivessel procedures. 647/ of 1000 (65%) patients fulfilled NICE criteria for DES. Of these, 520 of 647 (80%) received DES but only 423 of 647 (65%) followed NICE guidance for all lesions (37 patients receiving bare metal stents (BMS) for some NICE lesions and 60 receiving some DES for non-NICE lesions). 127 of 647 (20%) patients with NICE criteria for DES did not receive one, with reason stated for 50 of 127. Thus only 77 of 647 (12%) with NICE criteria for DES did not get one without a clear reason. 353 of 1000 (35%) patients had no NICE indication for DES. 176 of these received DES (139 of which met local criteria for DES, and 17 had other reasons for using DES). Overall compliance with NICE guidelines occurred in 600 of 1000 (60%). 879 of 1000 (88%) patients met local criteria for DES, of which 657 of 879 (75%) received DES and 573 of 879 (65%) followed local criteria for all lesions (78 patients inappropriately given BMS, 6 inappropriately given DES). 222 of 879 (25%) patients eligible for DES by local criteria were not given any DES, with reasons for 63 of 222. Thus 159 of 879 (18%) patients with local criteria for DES did not receive one without reason. 121/ of 1000 (12%) had no local criteria for DES, of whom 81 of 121 received only BMS appropriately, but 40 of 121 received DES. Overall compliance with local criteria occurred in 654 of 1000 (65%).
Conclusions: Requirements for DES by NICE criteria exceed their 1 of 3 initial estimate, with 65% patients eligible for DES. Extending DES indications to other patients at high risk of restenosis makes 88% of patients eligible for DES. Current rates of DES use exceed NICE guidance, but are not yet extended to all patients with increased restenosis risk. Due to the high cost of DES, health-economic implications need to be considered.
drug eluting stents; NICE guidelines; audit
125 ENHANCED EXTERNAL COUNTERPULSATION (EECP) THERAPY — INITIAL EXPERIENCE FROM A DISTRICT GENERAL HOSPITAL
A. Morton1, J. Darby2, C. Bradfield2, W. Rhoden2.1Cardiovascular Research Unit, Clinical Sciences Centre, Northern General Hospital, Sheffield, UK; 2Barnsley District General Hospital, Gawber Road, Barnsley, South Yorkshire, UK
Background: Enhanced external counterpulsation (EECP) has been shown by many to reduce angina and to improve myocardial ischaemia in patients with refractory angina in whom there is no potential for revascularisation. Prospective clinical studies from large American centres have shown that a course of EECP therapy is associated with improved symptoms, reduced hospital admissions and enhanced exercise tolerance and quality of life.
Methods: 35 patients were recruited over a 24-month period. Each patient underwent a 35 session course of EECP, consisting of 1 hour of EECP therapy for 35 consecutive working days. Exercise tolerance tests, CCS class determination and quality of life questionnaires were performed at baseline and follow up (immediately after treatment, at 1, 3 and 6 months). All patients were given the opportunity to attend a cardiac rehabilitation course following their treatment, based on individually tailored exercise regime. The number of hospital admissions with angina was recorded.
Results: Three patients were unable to complete the treatment course and were withdrawn from the programme. One patient died 1 month after completion of EECP. There was a significant increase in the METS of exercise performed post EECP (p<0.01). All patients showed an improvement in CCS Class (fig 1). The mean number of hospital admissions prior to EECP therapy was 1 with an average length of stay of 3 days. Post EECP therapy, no patients were admitted to hospital. All patients reported an improvement in physical and mental health based on the SF-36 quality of life score.

Abstract 125
Conclusion: EECP is an effective therapy for angina in patients who have no option for revascularisation. It results in fewer hospital admissions, reduced CCS Class and improved exercise tolerance.
enhanced external counterpulsation; exercise tolerance; CCS score
126 THE APPROPRIATENESS OF REFERRAL AND INVESTIGATION IN ANGINA (ARIA) TRIAL: RANDOMISED CONTROLLED TRIAL OF PATIENT-SPECIFIC DECISION SUPPORT V CONVENTIONAL AHA/ESC GUIDELINES
C. Junghans1, G. Feder2, A. Timmis3, S. Eldridge2, N. Sekhri2, N. Black4, P. Shekelle5, H. Hemingway1.1University College London Medical School, London, UK; 2Queen Mary’s School of Medicine and Dentistry, London, UK; 3Barts and the London NHS Trust, London, UK; 4London School of Hygiene and Tropical Medicine, London, UK; 5RAND organisation, California, United States
Background: Cardiologists and GPs are highly variable in their test ordering behaviour for stable angina and it is not known whether conventional guidelines or patient specific decision support might alter their investigation decisions.
Objectives: To determine the effect of patient-specific decision support v conventional guidelines on appropriate investigation decisions for exercise electrocardiography (ECGs) and coronary angiography.
Design: Randomised controlled trial. 145 doctors were randomised to patient-specific decision support and 147 to conventional guidelines (AHA, ESC). Doctors made recommendations on 12 web-based patient vignettes before and 12 vignettes after these interventions.
Setting: Nine regions in England, Ireland and Scotland.
Participants: Cardiologists (n = 103) and GPs (n = 194).
Main outcome measures: Appropriate investigation decisions defined by two independent expert panels rating in agreement.
Methods: Analysis was conducted blind to the intervention. We used random effects logistic regression to allow for clustering by clinician. We fitted formal interaction terms to the models to test for pre-defined specific subgroup effects (clinician specialty, age, sex and ethnicity).
Results: Doctors in either arm did not differ by demographic or practice characteristics. Before the intervention, there was no difference between the arms in appropriate decisions for Exercise ECG (AR 619 of 1475; 49%, GL 633 of 1484; 51%, p = 0.71) and for angiography (AR 1018 of 1557; 50%, GL 1015 of 1563; 50%, p = 0.42). Patient-specific decision support increased appropriate decisions for exercise ECG (OR 1.57; 95% CI 1.36, 1.82) and for angiography (2.24; 1.90, 2.62) compared with conventional guidelines (figure). This effect was equally strong in cardiologists and GPs and was similar in all pre-specified patient groups. In contrast, conventional guidelines had no effect on decision making, even when appropriate investigation was defined by the guidelines themselves.
Conclusions: Patient-specific decision support changed cardiologist and general practitioner investigation decisions, but current AHA/ESC guidelines were ineffective. Patient-specific decision support is a promising intervention for reducing practice heterogeneity unexplained by clinical need and for improving appropriate use of investigation. It now requires evaluation for its impact on patient prognosis.
angina; interventions; guidelines

Abstract 126
127 WIDESPREAD VARIATION IN THE PRACTICE OF CARDIAC CATHETERISATION IN PATIENTS WITH VALVULAR HEART DISEASE: A TIME FOR UPDATED GUIDELINES?
J. de Bono1, L. Hudsmith1, E. Orchard2, C. McKenna3, W. Orr3.1Department of Cardiology, The Royal Berkshire Hospital, Reading, UK; 2Department of Cardiology, Gloucestershire Royal Hospital, Gloucester, UK; 3Department Of Cardiovascular Medicine, The John Radcliffe Hospital, Oxford, UK
Introduction: Despite major advances in non-invasive imaging, cardiac catheterisation remains an integral part of the investigation and assessment of valvular heart disease, though it is not without risk and can result in stroke, myocardial ischaemia, arrhythmia and bleeding complications. Obtaining optimal information to guide surgical decision-making with an acceptable minimal risk to all patients is vitally important, but up-to-date guidelines as to how this is best achieved are lacking. We carried out a large questionnaire-based study to assess practice in both routine and complex cases within district general hospitals and teaching hospitals.
Method and Results: Anonymous questionnaires were sent to Cardiology Consultants and Trainees within two Deaneries. 67 (41 Consultant, 26 SpR) completed questionnaires were suitable for analysis. 45% (30) Cardiologists worked in teaching hospitals and 55% (37) in district general hospitals. There was huge variation in the practice of cardiac catheterisation amongst cardiologists, particularly between those who work in a district general hospital setting and those in a surgical centre. In direct contrast to the only currently available guidelines (AHA/ACC 1998 Guidelines on Valvular Disease), and despite the proven high risk of cerebral emboli, a quarter (17) of Cardiologists were still routinely crossing the valve in the assessment of aortic stenosis. This was more common in the district general hospital setting (p<0.05 compared with teaching hospitals), particularly among trainees (p <0.005 compared with teaching hospital colleagues). Over half of cardiologists (61%) still perform at least one Right Heart Catheter (RHC) a month, most commonly in the investigation of valvular heart disease (78%, particularly Mitral Valve disease), congenital heart disease (43%) and pulmonary hypertension (42%). Nearly a quarter (24%) of consultants from district general hospitals perform RHC on a weekly basis compared with only a single consultant from a teaching hospital (6%). There was no consensus as to the peri-procedural management of anticoagulation in patients with prosthetic valves. With mechanical mitral prostheses, 24% stop Warfarin alone, 39% admit for heparinisation, whilst 34% continue Warfarin and use a vessel closure-device or arm approach.
Conclusion: There is huge variation among cardiologists in the practice and extent of cardiac catheterisation in patients with valvular heart disease. This is in the context of major advances in non-invasive imaging and a greater proportion of diagnostic catheterisation being done away from surgical centres. In this survey, consultants in district general hospitals were more likely to adopt an invasive approach. This may reflect specialist interest, or different levels of experience, training and availability of local, reliable non-invasive assessment. There is an urgent need for the setting of national guidelines to ensure optimal and uniform information is obtained and patients are not exposed to unnecessary risk, particularly when assessing aortic stenosis or undergoing invasive procedures with prosthetic valve.
aortic stenosis; cardiac catheterisation; valvular heart disease
128 PACEMAKER-ASSOCIATED INFECTION – TIME FOR SOME NICE FRESH AIR?
H. Lashin, R. Anantharaman, R. Cowell, R. Trent.Wrexham Maelor Hospital, Wrexham, UK
Background: To investigate the incidence of infection following permanent pacemaker implantation and determine modifiable contributory factors following the final appraisal determination from the National Institute for Clinical Excellence (October 2004) for dual chamber pacing.
Method: A retrospective evaluation of all implants from January 2002 to 2003 was performed by review of case notes. Demographics, medical history, pacemaker prescription and complications were noted. Radiographic screening time was used as a surrogate marker of procedure time. The use of antibiotic prophylaxis and pre-operative antiseptic skin preparation were documented. Follow up data was collected from pacemaker clinic records with a mean of 32 months.
Setting: A 680-bed UK District General Hospital.
Patients: A total of 170 patients underwent procedures, mean age 76.3 (42–98), of whom 136 received new implants and 34 had generator replacements.
Results: 94 of 170 (55%) of implants were performed unassisted by one of three experienced operators (>100 cases each) with a further 76 (45%) procedures performed by two operators (Consultant + SpR). In all, 23 of 170 (13.5%) patients developed superficial wound infections during a mean follow-up period of 27 months after diagnosis of infection. Most of these presented relatively late after implant, 5 of 23 of these episodes occurred in hospital, 11 of 23 within 6 weeks and 20 of 23 within 6 months. 20 of 23 (87.0%) of these infections were treated successfully on an outpatient basis with oral antibiotics with no sequelae. Late complications occurred in 3 of 170 (2.3% total) patients however, of whom 3 of 170 (1.8%) subsequently required device explantation for deep pocket infection at 5 months, 2.5 years and 2.6 years, respectively. Procedural length (p<.001), device complexity (dual chamber v single chamber) (p = .02) and operator inexperience (p = 0.0006) were all associated with an increased infection rate, although preoperative antiseptic skin preparation (p = NS) and use of antibiotics (n = 145 of 170; 85%) did not reduce infection (p = NS). The presence of a temporary pacing wire did not affect the infection rate (p = NS). Procedural length was significantly shorter for single chamber systems (p = 0.001) and for experienced operators (p = 0.001).
Conclusions: The rate of (late) superficial wound infection is unacceptably high in this series, although the incidence of deep pocket infection is comparable to existing literature. Procedural length, device complexity and operator inexperience were the main determinants of increased risk. Operative techniques and pacing theatre environment should be examined; it is notable that laminar airflow theatres are considered a prerequisite for implantation of orthopaedic bioprostheses. Hopefully this area will be addressed in the forthcoming NICE guidelines.
pacemaker; infection; dual chamber
129 TAKING THE DOCTOR OUT OF THE LOOP; THE IMPACT OF A TECHNICIAN-LED FOLLOW-UP CLINIC FOR HEART VALVE DISEASE
W. Taggu, A. Topham, L. Hart, J. Silberbauer, A. Sulke, N. Patel, G. Lloyd.Eastbourne District General Hospital, Eastbourne, UK
Background: Despite clear guidelines, follow up of heart valve disease (HVD) is often poorly standardised and devolved to junior clinicians. We therefore established a service whereby patients requiring follow up only for their valve condition were assessed by senior echocardiography technicians working under protocol. Clinical support was provided only when required as judged by the technician.
Methods: Patient care was compared for the two years before and after the initiation of the valve clinic.
Results: 382 patients were enrolled (197 male, mean age 51 (range 17–94) years). The valve diagnoses (non-exclusive) were; mitral stenosis 15, mitral regurgitation 121, aortic stenosis 92, aortic regurgitation 169, mechanical prosthesis 103, bioprosthesis 44, previous MV repair 14 and valvuloplasty 2. Following valve clinic attendance, the median yearly echocardiogram rate was reduced from 2 (range 1–10) to 1 (range 1–5) (p<0.01) 807 echo visits were performed before the clinic compared with 550 after the clinic. The total number of outpatient visits dropped from 998 to 31 after the clinic. The median number of outpatient visits dropped from 3 (range 1-6) to 0 (0-3) (p<0.01). The number of patients following AHA guidelines rose from 157 (41%) to 354 (92%) (p<0.01). 12 (3%) patients were referred back to outpatients because of a change in clinical condition or requiring surgical intervention. Documented evidence of endocarditis prophylaxis advice given rose to 373 (97%) from 338 (88%) after the clinic.
Conclusion: Protocol-based, technician-led, follow-up clinics for HVD patients significantly improved the quality of care and decreased the burden on the cardiology clinic and reduced the total number of echocardiograms performed, without compromising safety. This may be highly cost effective way of improving patient care.
heart valve disease; technician led clinic; guidelines
130 SEX DISCRIMINATION IN THE PROVISION OF PRIMARY PREVENTION ICDS – EVIDENCE FROM A SINGLE UK CENTRE
H. Lindsay, R. Snowdon, D. Wright, J. Waktare, D. Todd.The Cardiothoracic Centre NHS Trust, Liverpool, UK
Objective: Women have been under-represented in recent major cardiovascular studies. They represented only 8% of patients in MADIT 1 and 16% of patients in MADIT 2, but were better represented with 32% of patients in COMPANION and 23% of patients in SCD HeFT. There has been recent focus on cardiovascular death in women, which is now the leading cause of death. We sought to determine whether women were receiving equitable care in terms of provision of primary prevention ICDs in our region.
Methods: We reviewed all primary prevention ICD implants over a 1-year-period, from October 2003 to October 2004. Case notes were reviewed to determine indication for implantation, and 1-year-follow-up data. We also reviewed 300 new patient referrals to consultants responsible for ICD implantation in the preceding 6-month period.
Results: A total of 66 patients had a primary prevention ICD implanted during the 1-year period. Of these only 7 (11%) were female (F). A small number of implants were performed for long QT syndrome (2 F), hypertrophic cardiomyopathy (1 male (M), 1 F), and arrhythmogenic right ventricular cardiomyopathy (2 M). Of the remaining 60 patients receiving ICDs on the basis of the MADIT 1 and 2, COMPANION and SCD HeFT studies only 4 (6.7%) were female. The indications in the 4 women were MADIT 2 (n = 3, 1 broad QRS) and SCD HeFT (n = 1). Overall patients had implantation on the basis of MADIT 1 (n = 4), MADIT 2 (n = 44, broad QRS n = 31), COMPANION (n = 7), and SCD HeFT (n = 5) studies. The mean age for men was 65 (12) years and for women was 74 (2) years. Left ventricular function and medications were well matched between males and females. During follow-up anti-tachycardia pacing or shock therapy rates were similar in both groups (1 of 4 (25%) women and 15 of 56 (26%) men). Analysis of the new patient referrals showed that during this period no female patients were declined ICD.
Conclusions: Women are vastly under represented in the clinical practice of primary prevention ICDs in our region. The data obtained from the new patient referrals suggests the cause of the discrepancy is due to referral bias. We hope by highlighting this issue to improve awareness and subsequently referral of women for primary prevention ICD.
ICD; women; primary
131 PERFORMING A COMPREHENSIVE ECHOCARDIOGRAM STUDY
L. Tilling, J. de Bono, H. Becher.John Radcliffe Hospital, Oxford, UK
Introduction: Echocardiography plays a major role in the investigation of heart disease. The British Society of Echocardiography (BSE) Education Committee published a Minimum Dataset for performing a standard adult transthoracic echocardiogram in 2005. We audited the performance of echocardiographers within our institution with the intention of establishing how closely practice adhered to these guidelines.
Methods: We performed an audit of consecutive transthoracic echocardiogram studies generated from a computerised database within the department of Cardiology at the John Radcliffe Hospital, a tertiary referral hospital in Oxford, from 1 June 2005 to 25 August 2005. We analysed each sequence of images to determine which of the 24 views recommended by the BSE had been obtained. Data were collected retrospectively for the period 1 June 2005 to 18 July 2005 (n = 961); the seven echocardiographers were then informed of the audit, and completed a programme of education to familiarise them with the requirements of the Minimum Dataset. Following this intervention prospective data collection occurred between 19 July 2005 to 25 August 2005 (n = 832).
Results: The results showed seventeen views were consistently obtained in over 78% of patients, irrespective of audit period. Seven views were obtained in less than 50% of patients; these were parasternal short axis (PSAX) colour flow Doppler (CFD) mapping for the pulmonary valve; PSAX CFD mapping for the aortic valve; apical 4 chamber (A4C) CFD mapping for the tricuspid valve; apical 5 chamber (A5C) 2D; A5C CFD over the aortic valve; A4C continuous wave Doppler across the tricuspid valve, and subcostal. Of this list, the first five views were performed significantly more frequently after intervention (p<0.001; see graph). The latter 2 views were both performed in less than 45% of patients in the retrospective audit. This did not increase after intervention; the subcostal view was actually obtained in significantly fewer patients (p<0.05) during reaudit.
Discussion: This audit showed incomplete studies were being performed within our own hospital with 7 particular views being consistently omitted. Following intervention, there was a significant increase in acquisition of five of these views. Two views were performed with a low frequency in both audits; this may indicate that the echocardiographers regard these views as unnecessary, or may encounter difficulty obtaining them. The least acquired views were predominantly colour Doppler mapping for valves. It is suggested that all echocardiographers are made aware of the importance of adherence to the Minimum Dataset, and the reason for acquiring each view. Ensuring awareness of the required views will facilitate comprehensive echocardiographic studies.
audit; echocardiography; dataset

Abstract 131
132 THE OUTCOME OF VENTRICULAR ARRHYTHMIAS AND CARDIAC ARREST DURING MYOCARDIAL INFARCTION IN THE 21ST CENTURY
S. Kesavan, B. Nuta, S. Burtchaell, M. James.Taunton and Somerset NHS Trust, Taunton, UK
Introduction: Mortality rates for ishaemic heart disease have dropped steadily over the past decades due to continuing refinement of medical therapy and the availability of new anti-tachycardia devices to treat life threatening arrhythmias. Along with the overall reduction in mortality, there may be a reduction in the incidence of ventricular fibrillation and cardiac arrest during an acute myocardial infarction.
Aim: Evidence indicates that the diminished threshold to ventricular fibrillation and the incidence of malignant ventricular arrhythmias associated with myocardial infarction are affected by the extent of underlying infarction. The purpose of the current observational study was to elucidate the incidence of life threatening arrhythmias and their influence on mortality.
Methods: We recorded the incidence and outcome of ventricular arrhythmias and cardiac arrest in 500 consecutive patients with myocardial infarction who survived to reach hospital. The follow-up period ranged from 2–4.6 years (mean 3.3 years). We have made no attempt to identify the number of victims of arrest prior to arrival in hospital. Myocardial infarction was defined as the following: chest pain or symptoms suggestive of myocardial infarction, ECG changes compatible with myocardial infarction (Qwaves, ST elevation or depression, T-wave changes, new Left Bundle Branch Block), cardiac enzyme rise more than twice the normal range and an elevated troponin value. Cardiac arrest was defined as any syncopy of cardiac origin – ventricular fibrillation, ventricular tachycardia, asystole and pulseless electrical activity. Ventricular tachycardia was defined as a broad complex tachycardia (which was not typical of aberrantly conducted supra ventricular tachycardia) which lasted greater than 5 beats.
Results: Mortality rates
Abstract 132
Conclusion: The incidence of cardiac arrest and ventricular fibrillation is decreasing in myocardial infarction victims in line with the overall reduction in mortality that has been observed in ischaemic heart disease. Whilst immediate survival for these patients is good, the long-term survival remains poor. Mortality is highest for the cardiac arrest group which includes asystole and pulseless electrical activity. In the modern era of well-trained paramedical personnel, early access to thrombolysis and standardised postinfarct therapy with ACE inhibitors, statins, aspirin and beta blockade among myocardial infarction victims who survive to reach hospital, the current incidence of cardiac arrest is 12%, ventricular fibrillation is 8% and ventricular tachycardia is 18%. Although the incidence of these arrhythmias is decreasing, their overall prognosis remains poor. Survival curves after major cardiovascular events, which identify populations at high risk usually demonstrate that the most rapid rate of attrition occurs during the first 6 to 18 months. Thus, there is a time-dependence of risk which focuses the opportunity for effective intervention to the early period after a conditioning event. Hence invasive/non-invasive intervention is of paramount importance in these high risk groups at an early stage of the disease to alter outcome.
cardiac arrest; ventricular fibrillation; ventricular tachycardia
133 THE EFFECTS OF ANXIETY AND DEPRESSION ON FUNCTIONAL CAPACITY AND QUALITY OF LIFE IN CHRONIC HEART FAILURE
S. Gupta1, N. Gandhi1, L. Burgess1, P. Wathall2, N. Brooks1.1Wythenshawe Hospital, Manchester, UK; 2York District General Hospital, York, UK
Background: Anxiety and depression are common in patients with chronic heart failure. The presence of psychological distress can worsen symptoms, reduce functional capacity and diminish quality of life for these patients. The aim of this study was to establish the correlation between anxiety and depression in heart failure with functional capacity and quality of life parameters.
Method: We conducted a retrospective study of patients with heart failure who had been referred for physiotherapy to our unit. Prior to physiotherapy, all patients were asked to complete the Hospital Anxiety and Depression Scale (HADS). The majority of patients also completed a Minnesota quality of life (QOL) questionnaire and a 6-minute walk test. We compared the patients who scored highly (score > = 11) for anxiety or depression with patients with the rest of the group in terms of their QOL scores and the distance they achieved on the walk test.
Results: 379 patients with a confirmed diagnosis of heart failure were referred. 288 were male and 91 female. Mean age was 66.7 years (27–89 years). The most common cause of heart failure was ischaemic heart disease (n = 262) followed by idiopathic dilated cardiomyopathy (n = 55). The majority of patients were either in NYHA class 2 (n = 197) or NYHA class 3 (n = 140). Average left ventricular ejection fraction was 31.6%. 172 patients completed a six minute walk test and 347 patients completed a QOL questionnaire. 81 (21.4%) patients scored highly for anxiety and 53 (14%) scored highly for depression. Patients who were clinically anxious were younger than patients who did not score as highly for anxiety (average age 63.7 v 67.6 years). There was no significant difference in the left ventricular ejection fraction of these two groups. The clinically anxious patients on average did not walk as far as the patients who were not anxious (284.7 v 338.8 metres; p<0.05). Anxious patients also scored significantly worse than their less anxious counterparts on the QOL questionnaire (58.9 points v 36.1 points; p<0.0001). Patients who were clinically depressed were also younger than their less depressed counterparts (average age 63.7 v 67.2 years). These patients also did not walk as far as the rest of the group (average distance 255.9 v 336.5 metres; p <0.05). Quality of life scores were also significantly worse in the depressed patients compared with the rest of the group (61.5 v 37.7 points; p<0.0001).
Conclusion: Anxiety and depression are common in chronic heart failure and their presence correlates with significant reduction in functional capacity as well as quality of life for these patients.
anxiety; depression; heart failure
134 THE FUNCTIONAL ASSESSMENT OF CHRONIC HEART FAILURE CAN BE RELIABLY ACHIEVED USING THE INCREMENTAL SHUTTLE WALK TEST (ISWT)
R. Evans, S. Singh, M. Morgan.University Hospitals of Leicester NHS Trust, Leicester, UK
Background: The incremental shuttle walk test (ISWT) is an important outcome measure for Cardiac Rehabilitation. It is a safe, valid measure of functional capacity, which independently predicts peak VO2 in patients with Chronic Heart Failure (CHF).1 However, the reliability of the ISWT in a general clinic population of individuals with CHF is unknown. We have evaluated the reliability of the test in a rehabilitation setting.
Methods: 38 patients with CHF who were unaware of the ISWT, were recruited as part of a larger training trial; 25 male, mean age 71.8 (9.4) years, NYHA class II-IV. All patients had a clinician diagnosis of CHF, an echocardiogram demonstrating at least mild systolic ventricular impairment and were on optimal medical treatment. Patients performed two ISWTs on the same day with a 30-minute rest in between. The third test was performed 10 to 14 days later at the same time of day. Standardised instructions were given on how to complete the test. Heart rate and oxygen saturation were monitored continuously and blood pressure measured before and immediately upon completion. Telemetry was not employed as all patients had completed a cardiopulmonary exercise test on a cycle ergometer, which excluded any significant arrhythmias or ischaemia.
Statistical analysis: The mean differences between any of the three tests were analysed using repeated measures and post hoc analysis with the least square difference. The formula used for the standard error of the measurement (SEM) was SEM = SD √1-ICC where SD is the standard deviation of the difference of means and ICC is the intraclass correlation. The formula used for the minimal detectable change for 95% CI was MDC = SEM × 1.96 × √2
Results: 36 patients completed all three tests with no adverse events. The mean of the three tests were 195 (123)m, 221 (127)m and 220 (123)m, respectively. There was a significant mean difference of 26 (33)m between tests 1 and 2 p = 0.0004. There was no significant difference in peak heart rate or peak oxygen saturation for any of the tests. There was no mean change in distance walked between tests 2 and 3; 1.4 (32)m p = 0.795 and the ICC between test 2 and 3 was high, 0.968. However, 12 patients had >15% variability between tests 2 and 3. The MDC for 95% CI is 16m (7% of the mean distance), indicating that a meaningful improvement after an intervention would need to exceed this value.
Conclusion: In Chronic Heart Failure, the Incremental Shuttle Walk Test is a reliable measure of functional capacity after familiarisation. A change from an intervention would only need to be above 16m (2 shuttles) to be meaningful.
1
chronic heart failure; incremental shuttle walk test; rehabilitation
135 EUROACTION: A DEMONSTRATION PROJECT OF A NURSE-LED HOSPITAL-BASED CARDIOVASCULAR PREVENTION AND REHABILITATION PROGRAMME
S. Connolly1, K. Kotseva1, C. Jennings1, A. Mead1, J. Jones1, A. Holden1, D. De Bacquer2, G. De Backer2, D. Wood1.1Charing Cross Hospital, London, UK; 2Ghent University, Ghent, Belgium
Introduction: EuroAction is a cluster randomised controlled trial of a nurse-led, multidisciplinary, family-based programme for coronary patients, their partners and first degree-relatives of patients presenting with premature disease in general hospitals in six European countries. The aim of the programme is to manage patients and their families to the European lifestyle, risk factor and therapeutic targets for cardiovascular disease prevention.
Methods: One pair of matched hospitals in each country was randomised to receive the EuroAction programme or usual care. Consecutive patients with a first presentation of coronary disease (myocardial infarction, unstable or stable angina) were actively recruited by the EuroAction nurse. All patients and partners were invited to attend a 16-week programme addressing lifestyle and risk factor management.
Results: 67% (n = 1060) of all eligible coronary patients (mean age 60 years) attended the baseline assessment. Of these, 48% had a recruiting diagnosis of a myocardial infarction, 17% unstable angina and 35% stable angina. 77% (n = 637) of all partners of coronary patients also attended the programme. 83% (n = 713) of patients completed the programme. At the end of the programme, 58% of patients who were smoking prior to their event were not smoking, 16% had relapsed and 26% continued to smoke. 67% of patients had a blood pressure below target (<140/90) at baseline and this significantly increased to 72% of patients at rescreening (p = 0.002). Similarly, 72% of patients had a total cholesterol below target (<5.0 mmol/l) at baseline, which significantly increased to 78% of patients at rescreening. There was also a small but significant increase in HDL cholesterol levels (+0.07 mmol/l, p<0.0001). The use of statin drugs increased significantly from 78% of all patients at baseline to 86% at rescreening (p<0.0001). Newly diagnosed diabetes was detected in 8% and 16% had impaired fasting glycemia. In those with known diabetes (17%) or diabetes diagnosed at baseline (8%), there was no significant change in their fasting glucose (-0.5, p = 0.06). For the partners, 14% were smoking and there was no change in the prevalence of smoking during the programme. However, there were substantial changes in BP with 40% of partners having an elevated blood pressure ⩾140/90 at baseline, which decreased significantly to 27% at 16 weeks (p<0.0001). Although there were no significant changes in mean lipid values there was a significant increase in the use of statins from 14 to 21% (p = 0.008).
Conclusions: This nurse led, multi-disciplinary, family based preventive cardiology programme successfully recruited a large majority of coronary patients and their families and most completed the programme. These families made healthy changes by stopping smoking, modifying their diets and increasing physical activity levels, as well as controlling other risk factors, which will reduce their risk of further cardiovascular disease.
EuroAction; nurse-led programme; cardiac prevention and rehabilitation
136 A RANDOMISED CONTROLLED TRIAL TO EXPLORE THE HARMS AND EFFECTS OF COMPONENTS OF A SELF-HELP INTERVENTION TO PROMOTE EXERCISE AND PSYCHOLOGICAL ADJUSTMENT IN HOME-BASED REHABILITATION PATIENTS WITH STABLE ANGINA (THE SHERPA TRIAL)
P. Wathall1, J. Miles2, J. Sutcliffe1, C. Jones1, K. Griffith1, D. Thompson3.1York Hospital, York, UK; 2University of York, York, UK; 3Chinese University of Hong Kong, Shatin, Hong Kong
Background: The Angina Plan is a home-based, self-help intervention for stable angina patients. The package is nurse administered and includes cardiac misconception correcting advice, relaxation and stress management techniques and goal-setting and pacing. Although widely used, there is no evidence that goal-setting and pacing is either safe or effective in this context. While in its entirety the Angina Plan has been shown to be beneficial, it remains unclear which parts are useful and which are not. If this were known it may be possible to improve the effectiveness of the intervention and to establish which components may be gainfully employed in future CR programmes.
Objectives: To determine the unique contribution of discrete components of the Angina Plan and to see whether goal-setting and pacing is safe for angina patients. Design: A randomised trial (2×2 factorial) exploring the effects of two treatment factors relaxation and stress management techniques and goal-setting and pacing, and their interaction relative to usual care.
Main outcome measures: Seattle Angina Questionnaire (SAQ), Hospital Anxiety and Depression scale, NYHA and Canadian angina class, York Angina Beliefs Questionnaire. 12 month survival of revascularisation or cardiac admissions. Serious and non serious adverse events.
Methods: 108 patients (age 63 (SD 9) 69% male) were randomised to either goal-setting and pacing (n = 29), relaxation and stress management (n = 27), the Angina Plan (27) or control (25) and all received telephone follow up with a nurse for 12 weeks.
Results: All data were analysed on an intention to treat basis. At baseline each of the treatment groups was equally well matched. At factorial ANCOVAs showed a statistically significant interaction effect for relaxation and stress management × goal-setting and pacing (Angina Plan) in relation to SAQ functional limitations (F (8,99) = 4.68, p = 0.03) and angina frequency and perception (F (6,98) = 4.13: p = 0.04). On both subscales scores were clinically significantly lower among patients treated with relaxation and stress management or goal-setting and pacing alone relative to the controls (suggesting harm). There were no significant differences on any of the psychological outcomes although each intervention produced statistically significantly better outcomes on the combined survival endpoint relative to controls. Harms analyses revealed no increase in adverse events among any of the treatment groups although ordinal regression showed treatment with either relaxation and stress management (β 2.62, p = 0.02) or goal-setting and pacing (β 2.82, p = 0.017) alone increased the likelihood of higher NYHA class scores at follow up.
Conclusion: The Angina Plan was statistically, but not clinically significantly better than usual care at reducing functional limitations and anginal frequency at follow up. It did not improve outcome in terms of cardiac misconceptions or psychological morbidity but increased survival on a combined endpoint including revascularisation and chest pain admissions (warrants further investigation). The study suggests that partial administration of the Angina Plan is ill-advised and that goal setting is safe when relaxation and stress management is given concomitently.
goal-setting and pacing; Angina Plan; stable angina
137 REHABILITATION OF SPOUSES OF PATIENTS WITH MYOCARDIAL INFARCTION: A RANDOMISED CONTROLLED TRIAL
D. Jones, R. West.University of Wales College of Medicine, Cardiff, UK
Background: Spouses (or partners) of patients admitted to hospital for acute myocardial infarction experience distress, anxiety and depression. Including spouses in cardiac rehabilitation programmes could help relieve this morbidity.
Objective: To assess the impact of a structured programme of rehabilitation on the psychological health of spouses of patients with myocardial infarction.
Design: A multicentre randomised controlled trial of psychological rehabilitation of spouses of patients with myocardial infarction.
Methods: Baseline measures of spouse health were obtained by structured interview at home shortly after patient discharge, using standard previously validated scales. Outcome measures were obtained at home with the same scales at 6 months. Patients were randomised to rehabilitation or “usual care”. Spouses of those randomised to rehabilitation were invited to attend three of seven sessions, which included sessions designed solely for spouses and opportunities for individual counselling.
Results: 1771 spouses (1394 women and 377 men) were randomised: 888 to rehabilitation and 883 to control. The prevalence of clinical anxiety (30%), clinical depression 1(4%) and severe distress (18%) shortly after patient discharge were all significantly higher than in general populations of comparable age. At 6 months there was significant improvement only in distress and no significant differences between rehabilitation and control groups: anxiety 29% v 32%, depression 12% v 13% and distress 8% v 8%. Rather fewer spouses referred to rehabilitation had consulted GPs for their own health in the preceding 4 weeks, 32% v 37%, but this difference was not statistically significant.
Conclusion: The study found significant clinical sequelae among spouses of patients with myocardial infarction that showed little resolution after 6 months, and the trial found little effect of a programme of psychological rehabilitation, although it was much appreciated. The needs of spouses or informal carers should be considered along with those of the patients themselves and further work is indicated to find more effective ways of helping these people.
randomised controlled trial; rehabilitation; spouses of patients
138 DIETARY IMPROVEMENTS AND IMPACT ON WEIGHT REDUCTION IN PATIENTS ATTENDING A CARDIAC PREVENTION AND REHABILITATION PROGRAMME: A LONGITUDINAL STUDY
A. Mead, A. Van Goor, H. Keightley, K. Fox, G. Frost.Hammersmith Hospitals NHS Trust, London, UK
Introduction: There is substantial scientific evidence showing that lifestyle interventions, including diet and risk factor modification can reduce cardiovascular morbidity and mortality. We hypothesised that providing three simple dietary messages to all patients would help compliance to a cardioprotective diet in the long term.
Methods: Within a set catchment area, all newly diagnosed patients with coronary heart disease were invited to a multi-professional cardiac prevention and rehabilitation (CPRP) 12-week programme which included three individual dietetic standardised assessments (outpatients, re-screening and 1-year follow-up). Data were collected from July 2000 to January 2005. Patients who attended both outpatients and re-screening dietary assessments were included in this study. Dietary advice was based on three evidence-based messages: an increase in omega 3 fats, a reduction in saturated fats with total or partial replacement by unsaturated fats, and Mediterranean dietary advice. Weight loss advice was also provided where appropriate.
Statistics: McNemar’s test was used to test change in percentage achieving dietary targets. Paired t-test was used to test change in weight and waist circumference over time.
Results: 425 patients had dietary assessments at outpatients and re-screening. 241 (57%) patients were seen at one year. There was significant improvement in the percentage of patients achieving the dietary goals from outpatients to re-screening which was maintained at one year (p<0.00001) (table 3). There is a significant mean drop in weight between outpatients and re-screening of 0.9 kg (95% CI 0.4, 1.4) p = 0.0009, but this difference is attenuated at one year to 0.5 kg (95% CI -0.4, 1.5) p = 0.3. In men there was a significant reduction in waist circumference between outpatients and re-screening of 2.3 cm (95% CI –3.0,1.6, p<0.0001) but this reduction is attenuated at one year to 0.8 cm (95% CI –2.0,0.5. p = 0.2). There was no significant change in the waist circumference of women from outpatient to re-sreening (mean change –0.9 cm 95% CI –2.2, 0.3, p = 0.15) or from outpatients to one year (mean change 0.9 cm 95% CI –1.5, 3.3, p = 0.44).
Conclusion: The patients attending the CPRP made dietary changes and maintained these changes at one year. Although patients had regained some weight at one year they did not return to their baseline weight. This is a direct contrast to the national trend of increasing obesity. Further work needs to be done to establish how we can help them improve their weight and waist circumference reduction at 1 year.
Abstract 138
diet; secondary prevention; weight loss
139 THE EFFECT OF A GENERIC PHASE 3 CARDIAC REHABILITATION PROGRAMME ON PATIENTS WITH AN IMPLANTABLE CARDIOVERTER-DEFIBRILLATOR
S. Armstrong, S. Singh.UHL NHS Trust, Glenfield Hospital, Leicester, UK
Cardiac rehabilitation is not routinely offered to patients after implantation of an implantable cardioverter-defibrillator (ICD). It is widely reported that patients with an ICD express anxiety about the device functions and lifestyle adaptation and are reluctant to carry out daily activities including exercise. Despite this, provision and effectiveness of rehabilitation in this patient group immediately after implantation has not been established. There has been no randomised control of rehab in patients with ICDs at equal time points to when rehab might feasibly be offered.
The aim of this study is to establish the effectiveness of a generic cardiac rehabilitation programme for patients 4 weeks after implant of an ICD device. 44 patients were recruited on a convenience basis and were randomised to attend the cardiac rehabilitation programme or to receive usual care using a minimisation technique by an independent researcher. The following criteria of classification of implant i.e. primary or secondary prevention, age, and gender were used. We studied a cohort of 22 patients who received cardiac rehabilitation (20 male, mean age 66.09 (SD 10.56) years) and 22 ICD patients who received usual care (20 male, mean age 65.77 (12.51) years). Patients were excluded from the study if they had been diagnosed with myocardial infarction or had CABG surgery during their admission or had received cardiac rehabilitation in the last 2 years.
All patients were assessed prior to rehabilitation 4 weeks after implant. Patients were enrolled onto the 6-week programme. The table below set out the mean (SD) change in scores for each group using appropriate parametric and non-parametric tests.
Abstract 139
Within the rehabilitation group there was a significant mean change in the incremental shuttle walk test result (p = 0.002) this was not observed in the usual care group. However between groups there was no significant difference (p = 0.97). There was a trend for anxiety levels to reduce more in the rehabilitation group compared with the usual care group. The Macnew scores did not demonstrate a significant change in any of the domains in either within or between groups.
This study demonstrates that a generic cardiac rehabilitation programme for patients with an ICD immediately after implant to improve patients’ physical function. Although there was not a significant change in any of the QOL measures when compared with the usual care group suggesting that the education/psychological component of a generic cardiac rehabilitation programme does not meet the specific needs of patients with ICDs. Therefore, it is proposed that access to a specific education programme and support mechanisms may be important to adjust to living with an ICD.
ICD; cardiac; rehabilitation
140 A PROSPECTIVE AUDIT TO IDENTIFY PATIENT CHARACTERISTICS ASSOCIATED WITH NON-ATTENDANCE AT FORMAL CARDIAC REHABILITATION
R. Allen1, A. Nijjar1, P. McIver1, S. Williams1, V. Badger1, T. Kitto1, A. Suliman2, K. Ranjadayalan2.1Newham PCT, London, UK; 2Newham University Hospital, London, UK
Introduction: The efficacy of formal cardiac rehabilitation has been established (Lau et al. 1992; O’Connor et al.1989; Oldridge et al 1991) however, not all eligible patients attend (Ades et al., 1996, Turner et al., 2002). Non attendance has been linked with socio-demographic factors including social deprivation (Melville, et al. 1999) and age (King et al., 2001), medical factors such as type of heart event (Cooper et al., 1999) and psychological variables including mood and illness beliefs (Cooper et al. 1999). The London Borough of Newham has a diverse population; 40% white, 29% South Asian, 20% Black African/Caribbean, and is one of the more economically deprived in the UK, with 16% unemployed/permanently sick (Census 2001). At Newham University Hospital the cardiac rehabilitation attendance rate is 55% per invited group. In aiming to increase access to cardiac rehabilitation and expand the generic cardiac rehabilitation service a prospective audit was conducted to ascertain which patient groups were not attending.
Method: 354 patients admitted to Newham University Hospital with diagnoses of acute myocardial infarction (AMI), acute coronary syndrome (ACS) or unstable angina were sequentially recruited to the audit from January 2004 to January 2005. Patients were followed up for 12 months with assessments at coronary care admission, 1, 3, 6 and 12 months. Follow up will be complete in January 2006. At each assessment, medical and socio-demographic details were recorded, and patients completed questionnaires assessing anxiety and depression (Hospital Anxiety and Depression Scale), anger (State Trait Anger Expression Inventory) and illness beliefs (Illness Perception Questionnaire).
Results: This abstract presents initial trends in the audit data. Statistical analysis will be completed in February 2006, at the end of the 12-month follow up, and will be presented in addition to the trends described below. Analysis will include differences between patients who attend cardiac rehabilitation and those who do not, and multiple regression analyses with attendance as the dependent variable. Of the 354 patients, 63% (n = 223) were eligible to be invited to formal cardiac rehabilitation. The attendance rate was 57%. Non-attenders were likely to be younger (mean age 55) than attenders (mean age 60). Attenders (57%) were more likely to be born in the UK than non-attenders (43%) and have English as their preferred language (65% as opposed to 57%). 40% of non attenders described their ethnicity as Indian, Pakistani or Bangladeshi compared with 34% of attenders. Non-attenders were less likely to have had an AMI (61%) than attenders (73%). Mean anxiety and depression scores at coronary care admission were higher in patients who did not subsequently attend cardiac rehabilitation.
Conclusions: The audit is innovative because of its prospective design. On the basis of patient characteristics, it is planned to develop a range of cardiac rehabilitation interventions targeted to specific groups, such as those who have returned to work, and Asian men and women.
audit; ethnicity; compliance
141 CARDIAC REHABILITATION STAFFING LEVELS FAIL TO MEET NATIONAL SERVICE FRAMEWORK AND SIGN GUIDELINES
D. Brodie1, H. Bethell2, S. Breen1.1Buckinghamshire Chilterns University College, Chalfont St Giles, UK; 2Basingstoke and Alton Cardiac Rehabilitation Centre, Alton, UK
Introduction: The Scottish Intercollegiate Guideline Network recommend 6.2 whole time equivalent staff per 500 patients for each cardiac rehabilitation programme. The purpose of this study was to establish whether or not this standard was being met in England.
Methods: One cardiac rehabilitation programme was randomly selected for each strategic health authority (n = 28) in England. Questionnaires and interviews with each cardiac rehabilitation coordinator established both the staffing levels and the mix of health professionals involved.
Results: The recommended SIGN guideline level of 6.2 was only achieved in 21% of the programmes surveyed. The shortfall was particularly in the profession of dietician (by 98%), pharmacist (by 80%), physiotherapist (by 79%) and psychologist (by 69%). The coordinators considered that their needs would best be met by increased participation from psychologist (half the centres), from physiotherapists (43%) and from counsellors (36%).
Conclusion: Cardiac rehabilitation has been demonstrated by meta-analysis to be beneficial and cost-effective. Funding for cardiac rehabilitation in England is inadequate to meet NHS recommended levels. This results in constraints being placed on the range of patients being offered cardiac rehabilitation with very few programmes (30%) able to provide a service to all those eligible. A governmental strategy is required to bring staffing levels up to the recommended standard and thus provide a service to meet the secondary prevention needs of those most likely to benefit.
Acknowledgement: This research was supported by the Coronary Prevention Group.
cardiac rehabilitation; SIGN Guidelines; staffing
142 THE IMPEDANCE CARDIOGRAM RECORDED THROUGH THE NOVEL CONFIGURATION OF TWO DEFIBRILLATOR/ELECTROCARDIOGRAM PADS PROVIDES A POWERFUL DETERMINANT OF CARDIAC ARREST
N. Cromie1, J. Allen2, J. Anderson3, A. Adgey1.1Royal Victoria Hospital, Belfast, UK; 2Physiology, Queens University, Belfast, UK; 3University of Ulster, Belfast, UK
Introduction: First responders are poor at emergency pulse checks. As such guidelines recommend that they should not be performed, creating the potential for suboptimal management of cardiac arrest. The impedance cardiogram (ICG; dZ/dt) is used to measure stroke volume. Can the impedance cardiogram recorded through two defibrillation/ECG pads placed in the standard position be used as a marker of cardiac arrest?
Methods: Experimentally, cardiac arrests were induced in 20 pigs (2 sets, 10 training and 10 validation). 40 epochs of sinus rhythm (20 prior to ventricular fibrillation and 20 after successful defibrillation), 40 during ventricular fibrillation, 20 during pulseless electrical activity and 20 during asystole were recorded in each set. Each epoch lasted 5 seconds. The Fast Fourier Transform (FFT) of dZ/dt was assessed to identify changes in the frequency spectrum with the onset of cardiac arrest.
Clinically, 53 “cardiac arrests” and 47 controls were studied in patients. 4-second epochs for dZ/dt were analysed in triplicate by way of a selective filter technique. Similar results in 2 of the 3 consecutive windows confirm the diagnosis of circulatory arrest.
Results: Experimentally, a peak FFT amplitude of ⩽4 dB.ohms.rms indicated cardiac arrest with sensitivities and specificities of 94% and 98% (Training) and 86% and 90% (Validation). Clinically - a sensitivity and specificity of 89.69% and 99.4% was found.
Conclusions: The FFT of the ICG waveform is a powerful clinical marker of circulatory collapse.
cardiac arrest; impedance cardiography; pulse check
143 DEFIBRILLATORS, DRIVING AND THE DRIVERS AND VEHICLES LICENSING AUTHORITY: ARE THE RULES RATIONAL?
B. Gordon, K. Lyons, E. Chew.Belfast City Hospital, Belfast, UK
Background: Current Drivers and Vehicles Licensing Authority (DVLA) regulations following an implantable cardioverter defibrillator (ICD) depend on the indication for implant. Patients are obliged to refrain from driving for one month if it is deemed a prophylactic implant or six months in other cases. For many, the inability to drive for 6 months is a major issue of quality of life. We sought to determine if the current rules are rational by assessing the frequency and timing of ICD therapy relative to implant date in our ICD population.
Methods: Patients who had an ICD between May 1999 and April 2005 and who are still alive were reviewed by telephone contact and examination of pacemaker clinic records. Indication for implant, details of therapy delivered and impact on driving were assessed.
Results: 123 of 141 patients were reviewed. 28 were non-drivers. 65 of 95 (68%) have had no ICD therapy since implant. 30 of 95 (32%) have had at least one ICD shock. Indication for implant in this group was 7 of 30 prophylactic and 23 of 30 non-prophylactic. Time to first shock was less than 1 month in 1 of 7 and 3 of 23, between 1 and 6 months in 1 of 7 and 4 of 23 and greater than 6 months in 4 of 7 (57%) and 16 of 23 (70%). Only 2 of 30 patients received a further shock in the 6 months after their first therapy. No patients experienced significant incapacity just before or due to device therapy.
Conclusions: The majority of ICD patients will not receive any device related therapy. Of those that do, 2 of 3 experience their first shock at least 6 months after the device has been implanted. In other words, most patients will have device therapy when they have been allowed to return to driving and not during the initial ban. This suggests that there is poor rationale for the current driving regulations regarding ICD devices. We suggest the rules should be reviewed as this could significantly improve quality of life for these patients.
implantable defibrillator; driving; quality of life
144 CARDIOLOGIST MEDIATED IMPLANTATION OF BIVENTRICULAR INTERNAL CARDIOVERTER DEFIBRILLATORS AND INTERNAL CARDIOVERTER DEFIBRILLATORS USING CONSCIOUS SEDATION: SAFE AND EFFECTIVE
D. Fox1, N. Davidson2, M. Royle1, R. D’Sa2, D. Bennett2, B. Clarke1, C. Garratt1, S. Williams2, A. Zaidi1, K. Patterson1, S. Petkar1, A. Fitzpatrick1.1Manchester Heart Centre, Manchester Royal Infirmary, Manchester, UK; 2North West Regional Cardiac Centre, Wythenshawe Hospital, Manchester, UK
Introduction: Implantation and testing of biventricular internal cardioverter defibrillators (Bi-ICDs) and implantable cardioverter defibrillators (ICDs) using local anaesthetic and conscious sedation is widely practised, but contentious with some centres using general anaesthesia. Selected patients with severe heart failure require Bi-ICDs, often with longer procedure times. We assessed safety and acceptability for both groups.
Methods: The records of 475 implanted devices at two regional UK centres from January 1996 to December 2004 were reviewed. Procedure time, left ventricular ejection fraction (LVEF), sedative dosage (midazolam), analgesic dosage (diamorphine or fentanyl), requirement for anxiolytic reversal and the need for respiratory support were recorded. Patient acceptability and the willingness to undergo a repeat procedure if required, was assessed by questionnaire.
Results: From the 475 new implants there were 387 ICDs and 88 Bi-ICDs. Patients with Bi-ICDs had significantly longer mean SD procedure times (129.7 (SD 7.6) mins v 63.3 (32.3) mins; p<0.0001) and lower LVEF (24.4 (8.4)% v 35.7 (15.4)%;p<0.0001). There were no differences between the doses of midazolam (8.9 (3.5) v 8.0 (3.1); p = NS) (mg), diamorphine (4.3 (2.0) v 3.8 (1.7), p = NS) (mg) or fentanyl (94.5 (53.7) v 92.2 (48.6), p = NS) (mcg) between the two groups. There were no deaths, intubations or need for formal ventilatory support in either group. There was only one respiratory complication, which occurred in the ICD group (apnoea post ventricular fibrillation induction responding to flumazenil reversal and transient manual ventilation). Patients with Bi-ICDs were less likely to require anxiolytic reversal 2 of 88 (2.3%) v 36 of 387 (9.3%); p<0.0001. Patient acceptability was available for 373 of 500 (75%) patients (49 dead, 78 unobtainable). 58 of 373 (16%) had some recollection of the implant or ventricular fibrillation defibrillation with 41 of 373 (11%) describing ‘pain’ but only 14 of 373 (3.8%) would decline a second procedure under local anaesthetic and conscious sedation.
Conclusion: In a large series of Bi-ICDs and ICDs implanted via cardiologist mediated local anaesthetic and conscious sedation, implantation was safe and acceptable. Although Bi-ICD patients have significantly longer procedure times and a lower LVEF, they seemed to tolerate the procedure as well as the ICD group. General anaesthesia is not routinely required for safe and effective implantation of Bi-ICD and ICD devices.
defibrillator implantation; conscious sedation; biventricular defibrillator
145 REGIONALISATION OF STEEP RESTITTUTION SLOPES AND VENTRICULAR TACHYCARDIA CIRCUITS
N. Sunni, A. Yue, K. Michael, S. Allen, P. Roberts, J. Morgan.Southampton University Hospitals, Southampton, UK
Introduction: Electrical instability and arrhythmogenesis have been linked to the steepness of the action potential duration restitution curve slope in experimental and animal models. Inducibility of re-entry ventricular tachycardia may be associated with the steepness of the restitution slopes but this is yet to be established in pathological human hearts.
Methods: Global activation recovery interval (ARI) restitution curves were constructed from virtual unipolar electrograms from 16 sites in the right or left ventricle of 7 patients (age 49 (21) years, 4 male) with ischaemic (2), nonischaemic (2) cardiomyopathies and fascicular ventricular tachycardia (3) and a mean ejection fraction of 48% (22)%. All patients had inducible sustained monomorphic ventricular tachycardia and underwent ventricular tachycardia ablation with the Ensite 3000 noncontact mapping (NCM) system. Standard S1-S2 restitution curves were constructed from pacing at the right ventricular apex. Maximum slopes (Smax) for the ARI restitution curves were formulated using the overlapping linear segments method. Dispersion of Smax was defined by the standard deviation.
Results: 1680 beats were analysed; mean ARI at steady state was 213 (SD 33) ms and at shortest coupling interval 183 (32) ms, mean overall Smax was 0.89 (0.25). The Smax was >1 at 20% of the sites. Dispersion of Smax 0.35 (0.14). However, the distribution of Smax was not uniform and appeared regionalised. In 6 of the 7 patients; ventricular segments at which ablation was successful in terminating the VT demonstrated the steepest ARI restitution slopes. The mean Smax for ventricular segments with the ablated sites was 1.64 (0.5). The mean distance between sites where Smax were determined and successful ablation sites was 19 (13) mm.
Conclusion: Steep ARI restitution slopes are regionalised in pathological hearts. Regional differences in electrical restitution may be masked by global analysis. There may be an association between critical pathways of ventricular tachycardia circuits and steep ARI restitution slopes.
cardiac mapping; ventricular arrhythmia; restitution
146 RISK STRATIFICATION OF VENTRICULAR ARRHYTHMIAS IN THE TROPONIN ERA: SHOULD PATIENTS WITH A POSITIVE TROPONIN FOLLOWING PRESENTATION WITH VENTRICULAR TACHYCARDIA/VENTRICULAR FIBRILLATION RECEIVE AN IMPLANTABLE CARDIOVERTER DEFIBRILLATOR?
R. Snowdon, H. Lindsay, L. Boodhoo, D. Wright, J. Waktare, D. Todd.The Cardiothoracic Centre NHS Trust, Liverpool, UK
Background: Implantation of an implantable cardioverter defibrillator (ICD) is recommended by National Institute for Health and Clinical Excellence (NICE) for patients presenting with sustained ventricular tachycardia/ventricular fibrillation associated with either: cardiac arrest, significant haemodynamic compromise or an ejection fraction <35%, in the absence of a treatable cause. The reclassification of myocardial infarction by the European Society of Cardiology/American College of Cardiology to include troponin positive events has resulted in an increase in diagnosis of myocardial infarction. There is a lack of clear consensus as to whether patients presenting with ventricular tachycardia/ventricular fibrillation in the setting of an elevated troponin, but without ST elevation or new left bundle branch block (LBBB), can be classified as having a non-ST elevation myocardial infarction and therefore a treatable cause as a basis for their ventricular arrhythmia. This may result in patients presenting with ventricular tachycardia/ventricular fibrillation being more frequently diagnosed with myocardial infarction and therefore being less likely to receive an ICD. In addition, arrhythmias alone can cause elevated troponin levels, which could result in an inappropriate diagnosis of myocardial infarction in such patients.
Methods: We reviewed all secondary prevention ICD implants over a 1-year period (October 2003 to October 2004) at our centre. Data on presenting arrhythmia, troponin level and coronary artery disease were collated with subsequent device therapy over a mean follow up period of 1.3 years.
Results: A total of 52 patients receiving secondary prevention ICDs were studied. All patients met current NICE criteria for secondary prevention ICD. The patients were divided into two groups according to troponin at presentation: Troponin positive, troponin T >0.2 µg/L or troponin I>2 µg/L (>99th percentile of the reference control group i.e. compatible with myocardial infarction); and Troponin positive, troponin T<0.2 µg/L or troponin I<2 µg/L. Trop+ve (n = 30, 57%) and Trop-ve (n = 22, 43%) groups were well matched for age, sex, antiplatelet drugs, beta blocker use, coronary artery disease, left ventricular function and previous revascularisation (all p>0.05). Presentation was with ventricular tachycardia in 18 patients in the Troponin positive group and 23 patients in the Troponin negative group. During 1.3 (0.6) years of follow up appropriate shock or anti-tachycardia pacing therapy was delivered to 32% of patients in Troponin positive and 67% of patients in Troponin negative groups (p = 0.025). Six patients had normal coronary arteries on angiography and 2 of these had troponin levels >0.2 µg/l at presentation.
Conclusion: Implantation of an ICD is indicated in patients with a positive troponin, without ST elevation or new LBBB, at the time of presentation with ventricular tachycardia/ventricular fibrillation. Although the positive troponin predicts a lower likelihood of subsequent appropriate ICD therapy, the rate of therapy is significantly higher than that reported in primary prevention studies such as the MADIT 2 trial (40% over 4 years). Patients with a positive troponin at the time of presentation with ventricular tachycardia/ventricular fibrillation should be referred for ICD.
ICD; troponin; myocardial infarction
147 A ZERO FLUOROSCOPY APPROACH FOR ELECTROPHYSIOLOGY STUDIES AND CATHETER ABLATION FOR COMMON SUPRAVENTRICULAR TACHYCARDIAS
N. Grubb, E. Petzer, C. Lang, A. Colthart, O. ElHag.Royal Infirmary of Edinburgh, Edinburgh, UK
Background: Radiation exposure during electrophysiology procedures carries risk for patients and operators. Non-fluoroscopic mapping systems help reduce exposure but have not been systematically evaluated as a means of eliminating fluoroscopy altogether.
Objective: To determine the feasibility of performing electrophysiology studies and radiofrequency ablation without fluoroscopy in patients with common supraventricular tachycardias using a non-fluoroscopic navigation system.
Methods: 76 patients underwent an electriophysiology study and ablation, using a zero or minimal fluoroscopy (ZMF) technique, for atrioventricular nodal re-entrant tachycardia (AVNRT) or atrioventricular re-entrant tachycardia mediated via left (L-AVRT) or right (R-AVRT) sided accessory pathways. An Endocardial Solutions/St Jude NavX system was used to guide catheters from the femoral veins to target positions in the heart for EPS, and to guide ablation. (Data from 38 consecutive standard fluoroscopic cases are shown for comparison). All patients had structurally normal hearts.
Results: Tachycardia substrates were AVNRT (n = 41, including 3 atypical variants), L-AVRT (n = 22, 24 pathways comprising 8 manifest and 16 concealed pathways) and R-AVRT (n = 13, 13 pathways comprising 9 manifest, 1 Mahaim, 1 middle cardiac vein and 2 concealed pathways). Using the ZMF group fluoroscopy was totally eliminated in 51 cases (76%) with no significant increase in procedure time or number of radiofrequency applications. Fluoroscopy was eliminated in 39 of 41 (95%) of AVNRTs, 10 of 13 (76%) of R-AVRTs and 2 of 22 (9%) of L-AVRTs. Median radiation dose was only 1692 cGy cm-2 for L-AVRTs. There were no significant complications.
Abstract 147
Conclusions: Non fluoroscopic navigation systems may safely completely eliminate radiation exposure for simpler EP procedures with minimal impact on procedure time.
radiation; catheter ablation; supraventricular tachycardia
148 MEASURING SUCCESS OF CATHETER ABLATION PROCEDURES FOR SUPRAVENTRICULAR TACHYCARDIA IN THE REAL WORLD: DO WE ENCOURAGE UNREALISTIC PATIENT EXPECTATIONS?
R. Showkathali, D. Gupta, M. Alzetani, M. Earley, P. Kistler, S. Harris, S. Sporton, A. Nathan, R. Schilling.St. Bartholomew Hospital, London, UK
Introduction: Catheter ablation is the treatment of choice for most patients with supraventricular tachycardia (SVT). The purpose of this study was to investigate whether the ‘real world’ clinical results are as good as success rates quoted to patients.
Methods: We analysed prospectively the acute and follow-up results of all cases of catheter ablation performed for SVT (excluding atrial fibrillation and left atrial flutter) at our institution over a 2-year period. Patients were assessed at 6-8 weeks follow up and evaluated for symptoms, arrhythmia recurrence and complications. We defined successful ablation as freedom from recurrence of the index arrhythmia at first follow up and compared our results with the success rates of 90–98% for catheter ablation for SVT quoted to patients on the websites of three major cardiovascular societies (American Heart Association, Heart Rhythm Society, British Cardiac Society).
Results: We performed a total of 547 ablations at our institution in the past 2 years of which 389 (71.1%) were for common SVT. Follow-up data were available for 367 (94.3%) of these. The success rates at follow up varied between 73.4% and 91.3% depending upon the SVT type as shown in the table (overall 83.9%). In addition, 75 (20.4%) patients continued to experience palpitations although they had no documented arrhythmia recurrence. The follow-up success rates were lower for revision procedures (46 of 65, 70.6%) as compared with de novo procedures (264 of 302, 87.4%), p<0.001.
Abstract 148
Conclusion: While physicians and cardiology association websites frequently quote success rates of greater than 90% for catheter ablation for SVT, in our experience “real world” results are considerably less impressive, particularly for accessory pathways and especially when early recurrence is taken into account. In addition, a significant proportion of patients may continue to experience palpitations without documented SVT recurrence. We feel it is important for institutions to audit their own success rates to guide patient counselling and decision making more accurately.
catheter ablation; supraventricular tachycardia; results
149 CATHETER CRYOABLATION FOR ATRIOVENTRICULAR NODAL RE-ENTRANT TACHYCARDIA: ARE THE RESULTS IN NORMAL PRACTICE AS GOOD AS IN PUBLISHED TRIALS?
D. Gupta, R. Al-lamee, M. Earley, S. Harris, S. Sporton, R. Schilling, A. Nathan.St. Bartholomew Hospital, London, UK
Background: Published trials indicate that cryoablation is as effective as radiofrequency ablation for the treatment of atrioventricular nodal re-entrant tachycardia (AVNRT). This coupled with the absence of the complication of atrioventricular nodal damage has led to cryoblation being considered the modality of first choice for AVNRT in many institutions. However, it is unclear whether the trial results with cryoblation are duplicated in the “real world” setting.
Methods and Results: We sought to compare the efficacy of cryoblation and radiofrequency for the AVNRT cases at our institution using a retrospective matched case control study design. The acute and follow-up results of 71 consecutive cryoblation AVNRT cases (Group A, 55 female, 52 (SD 16) years, median number of lesions 3, (range 1–19)) were compared with those of 71 matched AVNRT patients in whom radiofrequency was used (Group B, 55 female, 52 (15) years, median number of lesions 2, range 1–25). 4 mm tip cryoblation catheters were used in 61 cases and larger 6 mm tip catheters used in the other ten. Primary failure of cryoblation (thus necessitating radiofrequency at the same sitting) was seen in 11 (15.4%) cases in Group A while there was 1 (1.4%) primary failure with radiofrequency in Group B (p<0.01). The procedure time, screening time and radiation dose were not significantly different among the two groups and no complications were seen in either group. On follow up (66 (12) days), 15 (21.1%) patients in Group A had documented recurrence of AVNRT compared with 3 (4.7%) patients in Group B (p<0.01). Thus primary and/or secondary failure was seen in 26 (36.9%) patients when cryoblation was used as the initial ablation modality and in only 4 (5.6%) patients when radiofrequency was used (p<0.001). There were four cases of primary failure in the 10 cases where 6 mm tip cryoblation catheters were used.
Conclusions: We have observed a much higher primary failure and recurrence rate with cryoblation as compared with RFA for AVNRT, especially using 4-mm tip catheters. Whether the larger 6-mm tip catheters would have greater efficacy while preserving the inherent safety of this technique remains to be seen.
cryoablation; atrioventricular nodal reentrant tachycardia; radiofrequency ablation
150 AUDIT OF TEMPORARY CARDIAC PACEMAKER THERAPY IN EAST LANCASHIRE NHS TRUST
P. McCann, S. Singh.East Lancashire NHS Trust, Burnley, UK
Introduction: This retrospective audit of temporary cardiac pacemaker therapy was carried out to determine whether or not the American College of Cardiology and American Heart Association guidelines are followed. In addition, local guidelines state that transfer to a tertiary centre for permanent pacemaker insertion should be within 48 hours of temporary pacemaker insertion.
Methods: The audit was located in East Lancashire NHS Trust. Patients admitted and had a temporary pacemaker inserted were identified from a pacemaker register. All temporary pacings between 2002 and 2004 were identified. 73 patients were identified in total, and 56 were identified for audit. 17 were excluded because their case notes could not be located in the allotted audit time. From those 56, 41 were analysed in detail. 15 were excluded because insufficient detail was recorded in the notes to allow sufficient audit. The Audit Form primary objectives were firstly, to determine demographics of patients receiving temporary wires, secondly, to check whether the guidelines had been followed, thirdly, to determine the complication rates of wire insertion and also too analyse how long transfer to a tertiary centre took.
Results: Demography—The average age of the patients was 78 years (range 54–90 years). The male/female split was 55%/45%. Most patients came from the accident and emergency department (A&E). Falls and dizziness were the main symptoms. SpRs inserted 37 temporary wires and it was unusual for a consultant to be present at the time of insertion. Four wires were placed by SHOs. Insertion of Temporary Pacemakers—Nearly half of the patients were asymptomatic at the time of wire insertion. Often wires were put in against the advice of the guidelines. 76% of wires were inserted through the right internal jugular vein. 18% were inserted through the right subclavian vein. 6% were inserted through the femoral vein. 15 temporary wires were not successfully placed and 8 patients developed septicaemia. This led to very long delays transferring to the tertiary centre. Overall, 1 month mortality was 25%. 24 patients were referred to a tertiary centre but only 2 were transferred within 48 hours (range 1–37 days, mean 12 days).
Conclusions: In 3 years just 73 patients were identified. It is unlikely that much improvement in doctors’ skills will be achievable (because practice is so scarce) but limiting the number of wires to only those necessary will reduce the complications suffered. We propose advertisement of the guidelines widely (e.g. in A&E, Corinary Care Unit, the cardiac pacing room). Telephone advice must be sought from the tertiary centre if there is any doubt as to whether or not a wire should be inserted. In addition, an on-call rota of experienced doctors who can put wires in competently should be considered. Emphasis has to be put into reducing the rates of infection as transfer time to the tertiary centre was far greater than 48 hours. Sometimes this was due to septicaemia, but often the reason for delay was not obvious. This will need addressing in the future by liaison between the hospitals and the tertiary centre.
temporary wires; complications; audit
151 IMPACT OF INTRODUCING NATRIURETIC PEPTIDE ASSAY FOR PATIENTS PRESENTING ACUTELY TO SECONDARY CARE
A. Lokare, J. Johnston, W. Smellie, A. Fuat, J. Murphy, S. Mani.Darlington Memorial Hospital, Darlington, UK
Introduction: N-terminal pro B-type natriuretic peptide (NT proBNP) has been widely studied in primary care as a triage strategy to exclude left ventricular systolic dysfunction (LVSD). In contrast, experience in secondary care of patients presenting with acute breathlessness is limited. A level below 300 pg/dl could be used to exclude LVSD and reduce the need for echocardiography. A high level (adjusted for age) may identify patients with a high probability of LVSD and help with case finding. This paper describes the impact of introducing an NT proBNP assay on requests for echocardiography and number of patients discharged from an acute hospital with a primary diagnosis of heart failure. Cost/benefit is explored.
Method: The assay was provided in just one of three acute hospitals that form a single county-wide trust. NT proBNP was measured in patients presenting with acute breathlessness and/or oedema if the differential diagnosis included heart failure. Those previously investigated with proven LVSD were excluded. The laboratory report recommended echocardiography if the result exceeded 300 pg/ml. We studied referrals for echocardiography and discharge data (ICD 10, codes 150.0–150.9) for all three sites during the 7 months before (control period) and during the trial.
Results: During the 7 months 332 assays were performed of which just 49 (15%) were below 300 pg/ml and 21 of these underwent echocardiography for other reasons. Of the remaining 283 patients, all but 78 (27%) had echocardiograms. Requests for in-patients echoes increased from 368 in the 7 months before to 444 during the study (21% rise). During the control period, there were 223 coded discharges/deaths from heart failure compared with 185 during the study period (17% fewer). The comparable figures at the other hospital sites were 500 and 475 (5% fewer). Allowing for quality control the basic cost of each assay was estimated at £50, so over the seven months the service cost £16 600.
Conclusion: In patients presenting to a district hospital with unexplained breathlessness or oedema, only 15% had an NT proBNP <300 pg/ml so introducing this service did not significantly reduce referrals for echocardiography. Furthermore many had another indication so in practice just 8% of the cohort avoided echoes. During the period of study we saw a 21% increase in in-patient echocardiograms but a 17% reduction in the number of patients diagnosed with heart failure compared to a 5% fall in neighbouring hospitals. Introducing the service did not reduce the pressure for echocardiography or obviously increase the number of diagnoses of heart failure.
heart failure; natriuretic peptide; acute
152 MATRIX METALLOPROTEINASE -2 AND -9 IN THE PATHOGENESIS OF LEFT VENTRICULAR REMODELLING POST ACUTE MYOCARDIAL INFARCTION IN HUMANS
D. Kelly1, S. Khan2, N. Samani1, M. Thompson3, L. Ng1, I. Squire1.1University Hospitals Leicester, Leicester, UK; 2University Hospitals Leicester, Leicester, UK; 3St Georges Hospital, London, UK
Introduction: Matrix metalloproteinases (MMP) are implicated in the pathogenesis of adverse ventricular remodelling. We investigated the temporal profile of the gelatinases MMP-2 &-9, their relationship to left ventricular remodelling following acute myocardial infarction and compared with NT-BNP as a predictor of clinical events.
Methods: We studied 91 patients with confirmed acute myocardial infarction (AMI) (85% ST elevation myocardial infarction (STEMI),15% Non-ST elevation myocardial infarction (NSTEMI), 72.5% male, mean age 63.4 years). Serial blood samples were taken at 0–12, 12–24 and 24 h after symptom onset for measurement of MMP-2 and -9 and NT-BNP. Echocardiographic assessment of left ventricular end systolic (LVESV), end diastolic volume (LVEDV) and the change in volume (Δ, % of original) was performed pre-discharge and at a mean of 179 (SD 25.5) days. NT-BNP was measured as a surrogate marker of left ventricular function. Our primary end point was a composite of death or readmission with heart failure.
Results: MMP-2 was similar at all times with lower levels in inferior AMI (p = 0.007–0.019).Within the first 12 h MMP-2 was lower in smokers (p = 0.018)and males (p = 0.013). There was a univariate, but no multivariate, negative correlation between MMP-2 at 12–24 h and ΔEDV. MMP-9 peaked within 12 hours after AMI followed by a fall at 12–24 h to a plateau(0–12 hrs cf. 12–24 h p = 0.03). MMP-9 within the first 12 hours was higher in smokers (p = 0.029). There was a direct correlation between peak MMP-9 and ΔEDV (r = 0.324, p = 0.017) (fig 1), which remained on multi-variant analysis(r = −0.406, p = 0.011). Paradoxically. there was a negative correlation between trough MMP-9 and ΔEDV and ΔESV (r = −0.29, p = 0.034 and r = −0.454, p<0.001, respectively), maintained in our multi-variant model (r = −0.314, p = 0.04 and r = −495, p = 0.002). Univariant (r = −0.383, p = 0.002) and multivariate (r = −0.454, p<0.001) negative correlations were noted between trough MMP-9 and NT-BNP at follow up. No differences in MMP levels were seen in those who did (n = 10) or did not experience our end point. In comparison NT-BNP was significantly elevated at all time points from 24–96 h (p<0.001) in those who reached endpoint.

Abstract 152
Discussion: Individual temporal profiles of plasma MMP occur after AMI and are influenced by external factors. Correlation of peak MMP-9 with increasing left ventricular volumes implicates this enzyme in remodelling. Paradoxically, the negative correlations seen with trough levels suggest that some degree of MMP-9 release may be required to maintain left ventricular integrity. Our data does not support the use of plasma MMPs in prognostication.
metalloproteinase; NT-BNP; LV volumes
153 CARDIOTROPHIN-1 PREDICTS RISK OF DEATH OR HEART FAILURE FOLLOWING ACUTE MYOCARDIAL INFARCTION
S. Khan, D. Kelly, P. Quinn, L. Ng.University of Leicester, Leicester, UK
Background: Cardiotrophin-1 (CT-1) is an important inflammatory cytokine, its presence has been documented in patients following unstable angina and acute myocardial infarction (AMI). However its role as a predictor of death or heart failure in patients with AMI is unclear. We sought to investigate this and compared it to N-terminal B type natriuretic peptide (NT-BNP), a marker of death and heart failure.
Methods: We studied 291 post AMI patients (227 men, mean age 64.8 (SD 12.5) years, 80% ST elevation myocardial infarction (STEMI), 20% Non-ST elevation myocardial infarction (NSTEMI)). Blood measurement was made at 25–48 h after the onset of chest pain. The plasma concentration of CT-1 and NT-BNP was determined using in-house non-competitive immunoassays. Patients were followed-up for the combined endpoint of death or heart failure.
Results: Over the median follow-up period of 336 days (range 0–645) there were 27 deaths and 19 readmissions with heart failure. CT-1 was raised in patients with death or heart failure compared with survivors (median (range) fmol/ml, 0.9(0.1–392.2) v 0.7(0–453.3), p = 0.019). Using a multivariate binary logistic model CT-1 (OR 1.8, 95% CI: 1.1–3.2, p = 0.031) and NT-BNP (OR 2.4, 95% CI: 1.1–5.2, p = 0.026) independently predicted death or heart failure. This was also confirmed on the Cox proportional hazards model with the independent predictors of death or heart failure being CT-1 (HR 1.5, 95% CI: 1.1–2.0, p = 0.034) and NT-BNP (HR 2.1, 95% CI: 1.0–4.3, p = 0.05). The Kaplan-Meier survival curve revealed a significantly better clinical outcome in patients with CT-1 below the median compared with those with CT-1 above the median (log rank 5.79, p = 0.016). The receiver-operating curve for CT-1 yielded an area under the curve (AUC) of 0.62 (95% CI: 0.53–0.70, p = 0.017) for NT-BNP the AUC was 0.77 (95% CI: 0.69–0.86, p<0.001); the logistic model combining the 2 markers yielded an AUC of 0.84 (95% CI: 0.78–0.91, p<0.001).
Conclusion: After an AMI, combined levels of CT-1 and NT-BNP are more informative at predicting death or heart failure than either marker alone.
cardiotrophin-1; heart failure; NT-BNP
154 MATRIX METALLOPROTEINASE -2 AND -9 IN THE PATHOGENESIS OF VENTRICULAR DYSFUNCTION POST ACUTE MYOCARDIAL INFARCTION IN HUMANS
D. Kelly, S. Khan, L. Ng, I. Squire.University Hospitals Leicester, Leicester, UK
Introduction: Matrix metalloproteinases (MMPs) are involved in the degradation of extra-cellular matrix and have been implicated in the pathogenesis of ventricular dysfunction following acute myocardial infarction (AMI). We sought to investigate the temporal profile of the gelatinases MMP-2 and -9, post AMI, the relationship between their levels and ventricular dysfunction, and to compare with N-terminal B type natriuretic peptide (NT-BNP) as a predictor of such a process.
Method: We studied 91 patients (mean age 63.4 (11.4) years, male 72.5%, ST elevation myocardial infarction (STEMI) 85%, Non-ST elevation myocardial infarction (NSTEMI) 15%) with AMI. Serial blood samples were taken at 0–24, 25–48, 49–72 and 73–96 h after onset of chest pain. MMP-2 and -9 and NT-BNP were measured using a validated in-house assay. Echocardiography was performed pre-discharge and ejection fraction (LVEF) calculated via the biplane rule of discs method.
Results: MMP-2 remained constant at all time periods. Levels differed between anterior and inferior infarcts with lower levels seen in inferior infarctions. MMP-2 was lower within the first 12 hours post infarct in smokers v non-smokers (mean 20.0 v 25.2 ng/ml p = 0.018) and males v females (mean 21.2 v 28.5 ng/ml p = 0.013). MMP-9 levels displayed a peak within the first 12 hours post infarct followed by a fall at 12–24 h to a plateau (0–12 h cf. 12–24 h p = 0.03). MMP-9 was significantly higher in smokers within the first 12 hours (mean 149.1 v 94.0 ng/ml p = 0.029).
On univariant analysis both elevated levels of NT-BNP (24–96 h) and suppressed levels of MMP-2 (24–48 and 72–96 h) were associated with a risk of LVEF <40% the strongest predictor being NT-BNP at 48–72 h (p = 0.002).
Using a binary logistic regression model, after adjusting for confounding factors suppressed levels of MMP-2 was an independent predictor of EF<40% at 24–96 h, the strongest being at 72–96 h (p = 0.004). NT-BNP was most predictive at 24–48 h (OR p = 0.039) however to a lesser extent. MMP-9 was not found to be a significant predictor.
Conclusion: Levels of the gelatinases MMP-2 and -9 follow an individual temporal pattern post acute myocardial infarction. Suppressed levels of MMP-2 are associated with adverse ventricular function post AMI, possibly suggesting a protective role in this pathological process. The observation of differing levels between smokers v non-smokers is novel and warrants further investigation
matric metalloproteinase; BNP; MI
155 COST EFFECTIVENESS OF B TYPE NATRIURETIC PEPTIDE, ELECTROCARDIOGRAPHY AND PORTABLE ECHOCARDIOGRAPHY FOR THE ASSESSMENT OF SUSPECTED HEART FAILURE PATIENTS FROM THE COMMUNITY
T. Lim1, P. Collinson2, E. Celik2, D. Gaze2, R. Senior1.1Northwick Park Hospital, Harrow, UK; 2St George’s Hospital, London, UK
Objective: To analyse the cost efficiency of guidelines proposed by the European Society of Cardiology for investigation of suspected heart failure which recommend the electrocardiography (ECG) and/or measurement of N-terminal pro B type natriuretic peptide (NTproBNP) prior to referral for ECG. Portable echocardiography is a new but validated technique for the evaluation of heart failure.
Methods: Accordingly, 137 symptomatic patients (68 male, 69 female) mean age 71 (13) years were referred from primary care for portable echocardiology to confirm or exclude the diagnosis of cardiac abnormalities (left ventricular systolic dysfunction (LVSD), isolated left ventricular diastolic dysfunction (LVDD), significant valvular heart disease(VHD) and right ventricular dysfunction (RVD)) underwent prior ECG and NTproBNP estimation. A value of NTproBNP>20 pmol/l was considered as abnormal. Significant LVSD and LVDD were defined as left ventricular ejection fraction (LVEF)<45% and left atrial volume index>26 ml/m2 with LVEF> = 45% in absence of atrial fibrillation or significant mitral valve disease, respectively. The cost effectiveness of the 5 strategies to detect cardiac abnormalities was compared. The total costs of each strategy for detecting per case of cardiac abnormality were calculated from the total cost of initial tests and follow up portable echocardiology divided by the number of patients with respective cardiac abnormality. Indicative costs used were ECG Euros(€)16.20, NTproBNP measurement €22.50 and portable echocardiology € 41.
Results: Of the 137 patients referred, 19 (13.9%) demonstrated LVSD, 12 (8.8%) had isolated LVDD, 1 (0.7%) suffered from isolated RVD and 4(2.9%) had evidence of significant VHD. Sensitivity of ECG for the detection of LVSD, LVDD and VHD/RVD were 95%, 50% and 80%, respectively. Sensitivity of NTproBNP for the detection of LVSD, LVDD and VHD/RVD were 100%, 75%, and 100%, respectively. All strategies had excellent negative predictive values. The costs for each aforementioned cardiac abnormalities detected by the 5 strategies are shown in the table.
Conclusion: Whilst a strategy where initial NTproBNP estimation is cost-effective in detecting any causes of heart failure, portable echocardiography remains the most cost effective strategy to assess patients from the community with suspected heart failure.
Abstract 155
portable echocardiography; cost effectiveness; natriuretic peptide
156 THE PROTODIASTOLIC EXPANSION WAVE: A COMPENSATORY MECHANISM FOR THE REDUCTION IN LONGITUDINAL RELAXATION VELOCITY WITH AGEING?
C. Manisty, J. Davies, D. Francis, A. Zambanini, S. Thom, A. Hughes, J. Mayet.International Centre for Circulatory Health, Imperial College and St Mary’s Hospital, London, UK
Introduction: Diastolic filling is initiated by a left ventricular suction wave during protodiastole - the period between peak ventricular contraction and closure of aortic valve. When active myocardial shortening stops in protodiastole, aortic blood flow continues under its own momentum and left ventricular pressure declines giving rise to a “sucking” wave that decelerates flow (expansion wave; fig 1). The deceleration of flow contributes to aortic valve closure and transmitral left ventricular filling.
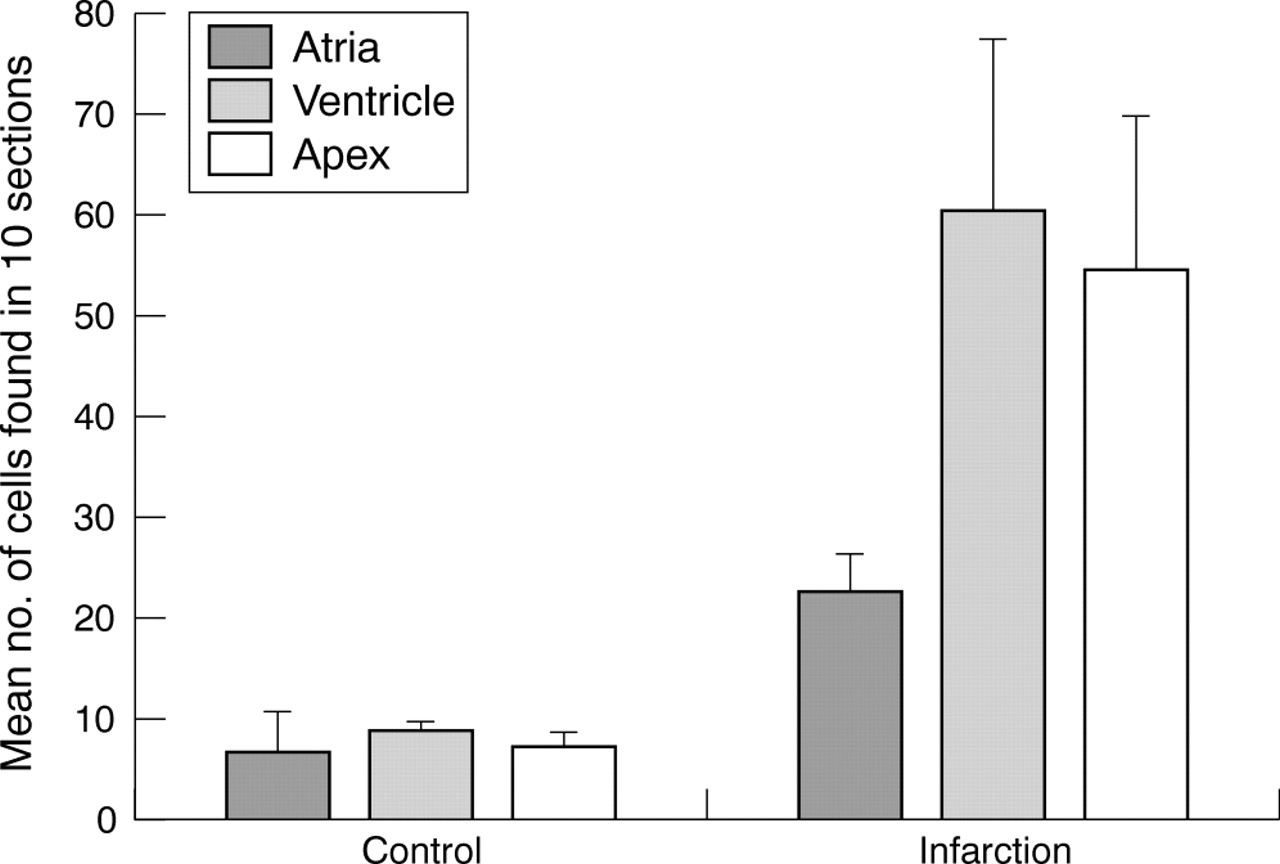
Abstract 156
Active relaxation declines with advancing age. This is easily detected on echocardiography by studying transmitral blood flow and long axis function. Little is known however, about the effects of age and hypertension on protodiastole—a passive process that is likely to depend not only on the systolic properties of the heart, but also on myocardial and vascular compliance.
Methods: We used wave intensity analysis to quantify the expansion wave during protodiastole in the carotid artery of 270 subjects (mean age 64 years, range 39 years). Our study group consisted of normal subjects and subjects with controlled hypertension who were participating in the Anglo-Scandinavian cardiac Outcomes Trial (ASCOT).
Wave intensity analysis identifies unambiguously differentiates the direction, amplitude and timing of the individual waves that amalgamate to form the carotid pressure waveform. In addition, we assessed diastolic function using echocardiography (tissue Doppler and pulsed wave Doppler).
Results: With age there was a fall in longitudinal relaxation velocity (E′) (r = −0.32, p = <0.0001), as expected. In contrast, both the systolic compression wave (r = 0.21, p = 0.0006) and the protodiastolic expansion wave intensity increased with age (r = 0.39, p<0.0001) – fig 1.
In multivariant analysis the wave intensity of the expansion wave was related to age and preload (as measured by E/E′ on echocardiography) – Table 1.
Abstract 156
Conclusions: Protodiastole can be considered the earliest stage of diastole but the extent of its contribution to left ventricular filling has not been established.
Our non-invasive wave intensity analysis shows that with advancing age the expansion wave increases significantly, in contrast to other markers of diastolic function.
As the ventricle becomes less compliant with age, at end systole the fall in myocardial contraction velocity will be more rapid. This means that there will be a greater pressure and velocity difference between the contracting ventricle and aortic blood flow, leading to a larger expansion wave in protodiastole.
The expansion wave was also independently correlated to preload due to the greater systolic contraction force, producing an increased expansion wave.
The expansion wave in protodiastole may play a larger role in passive left ventricular filling with advancing age, thereby helping to counterbalance the fall in longitudinal relaxation velocity.
protodiastole; wave intensity; ageing
157 THE EXTENT OF MYOCARDIAL SCAR IDENTIFIES PATIENTS WITH LEFT VENTRICULAR SYSTOLIC DYSFUNCTION WHO HAVE PERSISTENT ADVERSE VENTRICULAR REMODELING: A CARDIAC MAGNETIC RESONANCE STUDY WITH DELAYED ENHANCEMENT
N. Nikitin, P. Loh, R. de Silva, E. Lukaschuk, D. Ettles, M. Alamgir, A. Clark, J. Cleland.University of Hull, Hull, UK
In chronic heart failure (CHF), beta-blockers and angiotensin converting enzyme (ACE) inhibitors improve left ventricular systolic function but not all patients respond. We sought to establish whether scar extent, assessed by cardiac magnetic resonance (CMR) with delayed enhancement, can determine the risk of persistent adverse left ventricular remodelling despite standard pharmacological treatment.
Methods and results: Thirty-eight patients with CHF because of left ventricular systolic dysfunction and already receiving treatment with ACE inhibitors/angiotensin receptor antagonists and beta-blockers underwent CMR with delayed enhancement which was repeated after 12 months. Delayed enhancement on CMR (interpreted as scar tissue) was present in 24 patients. The scar mass was 24 (SD 9) g (range 9–43 g) and scar extent (percentage of left ventricular mass) was 17 (7)% (range 6–31%). At baseline, there were no differences in clinical or CMR-derived indices between patients showing delayed enhancement (+ group) and no delayed enhancement (delayed enhancement - group). After 12 months, left ventricular volumes and ejection fraction were unchanged in the delayed enhancement+ group. In the delayed enhancement- group, left ventricular end-diastolic and end-systolic volumes fell (231 (83) to 196 (71) ml, p = 0.018 and 161 (74) to 120 (68) ml, p = 0.007, respectively) and ejection fraction increased (32 (11) to 41 (11)%, p = 0.003). No delayed enhancement- patients showed deterioration in ejection fraction of ⩾5%. Eight delayed enhancement+ patients who demonstrated deterioration in ejection fraction had higher scar extent than 17 delayed enhancement+ patients with no deterioration (22 (8) v 14 (3)%, p = 0.03). There was a strong negative correlation between scar extent and change in ejection fraction (p<0.001, r = −0.77).
Conclusions: In patients with LV systolic dysfunction, scar extent can predict the risk of persistent adverse left ventricular remodelling.
heart failure; ventricular remodelling; magnetic resonance imaging
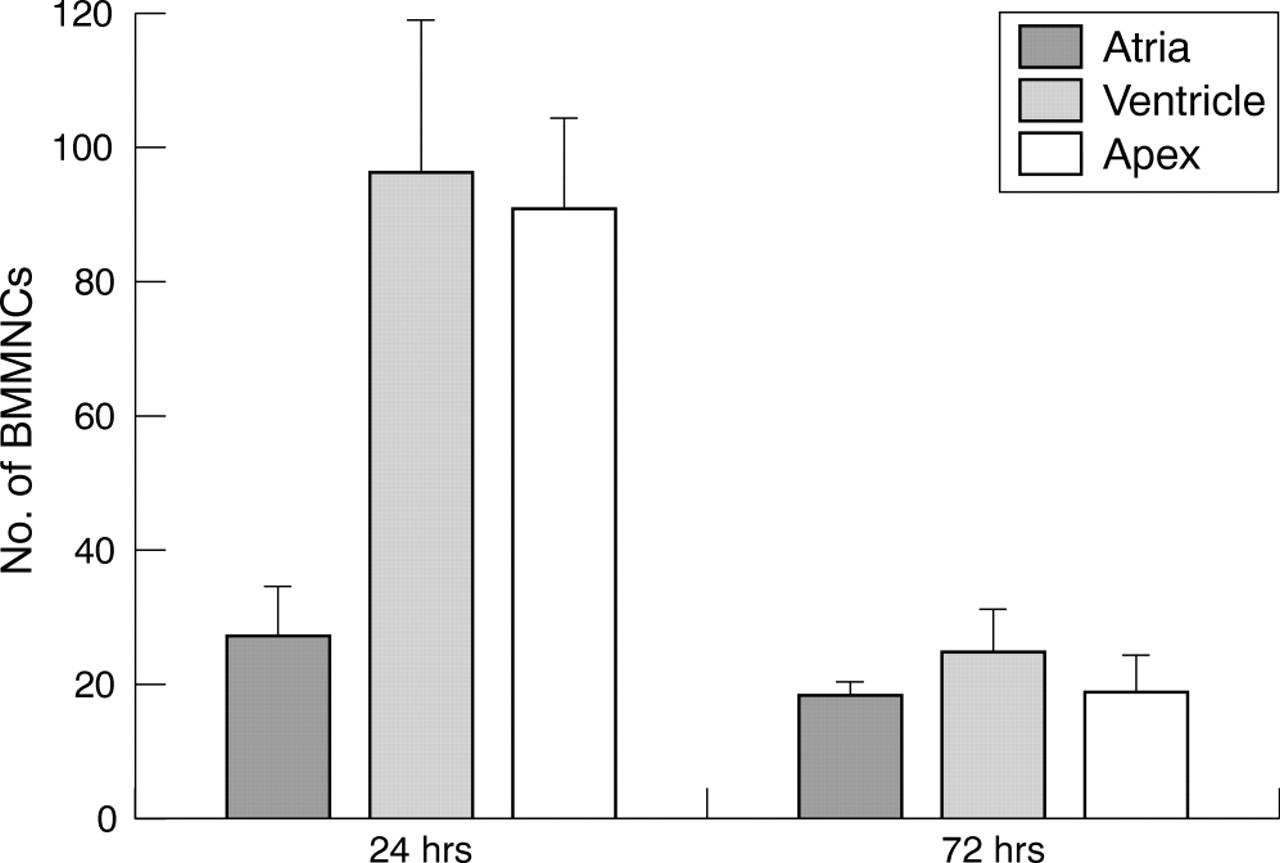
Abstract 157
158 PREVALENCE OF VIABLE BUT DYSFUNCTIONAL MYOCARDIUM IN PATIENTS WITH HEART FAILURE OF ISCHEMIC ORIGIN AS ASSESSED BY CARDIAC MRI WITH DELAYED CONTRAST ENHANCEMENT
N. Nikitin, P. Loh, R. de Silva, E. Lukaschuk, D. Ettles, M. Alamgir, A. Clark, J. Cleland.University of Hull, Hull, UK
Accurate assessment of the myocardial pathology leading to chronic heart failure (CHF) of ischemic origin may help select appropriate therapy. Cardiac magnetic resonance (CMR) with delayed enhancement can differentiate between viable and non-viable myocardium and provide unique data on the transmural extent of scar/viability.
Methods and results: We studied 134 patients with CHF of ischemic etiology using delayed enhancement CMR. Myocardial contractility and extent of delayed enhancement were assessed blindly in a 17-segment model. At least one dysfunctional but viable (defined as delayed enhancement affecting ⩽50% of wall thickness) myocardial segment was present in 128 patients (96%) and 63 patients (47%) had >5 affected segments. If only segments with no delayed enhancement were deemed viable, 53 patients (40%) had at least one such segment and 27 patients (20%) had >5 such segments. Of 2278 segments assessed, 1222 were dysfunctional of which 30% showed no delayed enhancement (entirely viable), 35% had delayed enhancement of ⩽50% (partly viable) and 35% had >50% of wall thickness associated with delayed enhancment (deemed non-viable). Patients with significant myocardial viability (>5 segments) had larger left ventricular end-diastolic and end-systolic volumes (256 (85) v 220 (110) ml, p = 0.034 and 184 (74) v 144 (109) ml, p = 0.012, respectively) and a lower left ventricular ejection fraction (29 (9) v 40 (14)%, p<0.001) than patients with <5 dysfunctional but viable segments.
Conclusions: Nearly half of patients with CHF of ischemic origin have a substantial volume of myocardium that is viable but dysfunctional on delayed enhacnement CMR. About a third of all dysfunctional segments are partly viable with ⩽50% scar extent.
heart failure; Hibernation; magnetic resonance imaging
159 INFARCT SIZE AND PROGRESSIVE LEFT VENTRICULAR SYSTOLIC DYSFUNCTION AND REMODELING POST MYOCARDIAL INFARCTION: A CONTRAST-ENHANCED MRI STUDY
Y. Zhang1, A. Chan1, G. Yip1, M. Wang1, W. Lam1, N. So1, C. Yu1, J. Sanderson2.1The Chinese University of Hong Kong, Shatin, Hong Kong; 2Keele University Medical School and University Hospital of North Staffordshire, Stoke-on-Trent, UK
Background: Contrast enhanced cardiac MRI can accurately measure infarct size. However, there is little data on the impact of infarct size and location by ce-MRI on ventricular remodelling post myocardial infarction.
Methods: Short-axis contrast-enhanced MRI was performed in 47 consecutive patients (59.9 (11.5) years) with a first documented myocardial infarction at day 2–5, and after 3 months and 1 year. Infarct size was determined as a percentage of left ventricular volume, as the sum of hyperenhanced areas from each of all the short-axis images divided by the total area of pixels within the myocardium. Standard 2D-echocardiographic recordings and measurements were also done.
Results: Patients were classified into two groups according to changes of end-systolic volume (ESV) at baseline and at 1 year: a non-remodelling group (n = 31) with unchanged (<10% increase) or reduced ESV and a remodelling group (n = 16) with percentage increase of ESV >10%. Patients with left ventricular remodelling had significantly greater infarct size and more anterior infarction at baseline compared with those without remodelling. Infarcts diminished in the non-remodelling group but showed no regression in the remodelling group. A multivariate logistic regression analysis showed that baseline infarct size was the most powerful independent predictor of left ventricular remodelling in the subsequent year after adjustment for anterior location, ESV and infarct transmurality (Odds Ratio: 1.64, p = 0.004), and it added incremental predictive value to standard clinical and echocardiographic measurements. Furthermore, an infarct size ⩾15% for the anterior myocardial infarction and ⩾20% for the inferior had a high sensitivity and specificity for the prediction of left ventricular remodelling.
Conclusion: A contrast-enhanced MRI determined infarct size ⩾15% for the anterior myocardial infarction and ⩾20% for the inferior predicts subsequent remodeling in the following year after an acute infarction.
MRI; infarction; remodelling

Abstract 159
160 ATRIAL NAD(P)H OXIDASE ACTIVITY PREDICTS THE DEVELOPMENT OF ATRIAL FIBRILLATION AFTER CORONARY ARTERY BYPASS GRAFT SURGERY
Y. Kim1, H. Kattach2, C. Ratnatunga2, R. Pillai2, K. Channon1, B. Casadei1.1University of Oxford, Oxford, UK; 2John Radcliffe Hospital, Oxford, UK
Atrial fibrillation is a common complication of cardiac surgery leading to increased morbidity and prolonged hospitalisation. Emerging evidence indicates that treatment with antioxidants may prevent post-operative atrial fibrillation, however, it is not clear whether treatment should be targeted to reducing the systemic oxidant response to cardiac surgery or to inhibiting the synthesis of reactive oxygen species (ROS) in the atrial myocardium.
To address this issue, we prospectively measured NAD(P)H oxidase activity (by lucigenin-enhanced chemiluminescence) in right atrial appendage (RAA) tissue obtained in 170 consecutive patients undergoing first-time elective coronary artery bypass (CABG) surgery. We have recently demonstrated that a phagocytic-type NAD(P)H oxidase is the main source of reactive oxygen species (ROS) in the human atrial myocardium. Plasma markers of lipid (TBARS) and protein (carbonyls) oxidation were measured in blood samples drawn from a central line immediately after the induction of anaesthesia and 10 minutes after the administration of protamine.
Seventy-one patients (42%) developed atrial fibrillation within 5 days of CABG surgery. No significant differences between groups were found with respect to treatment, cardiovascular risk factors, duration of cardiopulmonary bypass or aortic cross-clamp, and number of grafted vessels. However, patients who developed post-operative atrial fibrillation were older and had a significantly higher atrial NADPH-stimulated superoxide production than those who remained in sinus rhythm (4.77 (0.17) v 3.54 (0.11) RLU/sec/ug protein, p<0.001) Plasma markers of lipid and protein oxidation increased significantly after reperfusion (p<0.05 for both) reflecting the increase in oxidant stress associated with cardiac surgery. However, neither preoperative nor postoperative plasma levels of TBARS or protein carbonyls differed between patients who developed atrial fibrillation and those who remained in sinus rhythm after surgery. Multivariate analysis identified myocardial NAD(P)H oxidase activity as an independent predictor of postoperative atrial fibrillation in our patients (OR: 2.58; 95% CI: 1.67–3.98, p<0.001).
These findings indicate that atrial NAD(P)H oxidase activity, but not plasma markers of oxidant stress, is a independent predictor of post-operative atrial fibrillation in patients undergoing CABG surgery and suggest that the tissue-specific capacity to generate ROS may be a more accurate predictor of myocardial perioperative oxidant injury than conventional plasma markers of lipid or protein oxidation and as such, it may provide a more accurate risk stratification tool and better target for pharmacological interventions.
oxidant stress; atrial fibrillation; human
161 EXERCISE REHABILITATION ENCHANCES THE BENEFITS OF CARDIAC RESYNCHRONISATION THERAPY
A. Patwala1, P. Woods2, D. Barker3, S. Williams1, D. Goldspink2, L. Tan3, D. Wright1.1The Cariothoracic Centre, Liverpool, UK; 2RISES, Liverpool John Moores University, Liverpool, UK; 3Academic Unit of Molecular Vascular Medicine, University of Leeds, Leeds General Infirmary, Leeds, UK
Background: Cardiac Resynchronisation Therapy (CRT) has been shown to improve mortality and morbidity in patients with severe heart failure and evidence of electromechanical dyssynchrony. It has previously been shown that heart failure patients also suffer from chronic skeletal muscle deconditioning the reversal of which may be assisted by exercise rehabilitation. We therefore performed a randomised controlled trial to assess whether exercise rehabilitation increased the benefits of CRT.
Methods: 28 patients referred to our centre for CRT were recruited. Patients were tested pre-, 3 months post and 6 months post CRT. At each visit triplicate resting cardiac output measurements were made using the equilibrium method of Collier. A modified Bruce protocol treadmill was then carried out to assess peak VO2 and peak cardiac output was measured using the exponential method of Defares. After 30 minutes rest peak skeletal muscle torque was measured in extension and flexion at both knees with a Biodex isokinetic dynamometer using a 60-degree/sec protocol. Peak and Resting Cardiac Power Output (CPO) were calculated using the formulae: CPO = CO x mean arterial pressure × 2.22×10-3. Cardiac reserve was calculated by subtracting Rest CPO from Peak CPO. After the 3 months’ test the patients were randomised into either an exercise group or a control group. The exercise group underwent a programme of supervised exercise rehabilitation programme consisting of three visits per week. Each visit was made up of 20 minutes of treadmill walking and 10 minutes cycling. After 3 months of the exercise programme the patients were tested at the 6-month stage along with the control group. Paired t-tests were used to look for statistically significant differences.
Results: There were no significant differences between the groups at baseline. By 3 months there was a significant improvement in NYHA class, Exercise Duration, Peak VO2, Peak CPO and cardiac reserve in both the control group and the exercise group. In both groups there was no change in skeletal muscle function at this point. After the period of randomisation to exercise rehabilitation the exercise group showed further significant improvement in the exercise haemodynamic measures and also showed significant improvements in peak skeletal muscle torque. The control group showed no significant changes over this period in any measure (see table 1 results shown as mean (SE))
Conclusion: Exercise Rehabilitation leads to an improvement in both exercise haemodynamic measures and peak skeletal muscle torque in addition to the improvement seen after CRT. By the end of the study the group undergoing exercise rehabilitation have a much larger functional capacity. Therefore exercise rehabilitation allows maximal benefit to be attainted after CRT. In our opinion exercise rehabilitation should be considered for all patients following CRT.
Abstract 161
exercise rehabilitation; cardiac resynchronisation therapy; cardiac power output
162 METFORMIN AT REPERFUSION: A NEW INDICATION THAT THE FIRST LINE ORAL HYPOGLYCAEMIC THERAPY MAY PROTECT THE DIABETIC MYOCARDIUM FROM ISCHAEMIA - REPERFUSION INJURY
G. Bhamra, S. Davidson, M. Mocanu, D. Yellon.The Hatter Cardiovascular Institute, UCL Division of Medicine, Royal Free and University College Medical School, UCL, London, UK
Background: The only current clinical use of metformin is in combination therapy with sulphonylureas, insulin and thiazolidinediones, to achieve more effective glycaemic control, as evident by the United Kingdom Prospective Diabetes Study (UKPDS). Interestingly, UKPDS also demonstrated that metformin was associated with a reduced level of myocardial infarction and stroke, independent of glycaemic control, suggesting pleiotropic cardiovascular protective effects. At a more basic level, metformin has recently been shown to inhibit the opening of the mitochondrial permeability transition pore (MPTP) in cancer cells. With regard to the myocardium, we have demonstrated that inhibition of the MPTP is associated with protection against myocardial ischaemia-reperfusion injury, with this protection being linked to the up-regulation of survival signalling kinases. The aim of this study was to investigate whether metformin could reduce myocardial infarction, and if this involves inhibition of the MPTP and the recruitment of the survival kinases PI3-Kinase/Akt and Erk1/2 MAP kinase.
Methods and results: a) Isolated perfused Wistar rat hearts were subjected to 30 min ischemia and 120 min reperfusion. 50 µM metformin, and/or 15 µM LY 294002 (PI3-K inhibitor) or 10 µM UO126 (Erk1/2 inhibitor), were given at reperfusion. Infarct size (expressed as a percentage of myocardium at risk, I/R%) and Akt, Erk1/2 and AMP kinase phosphorylation were measured. Metformin significantly reduced myocardial infarction (35% (2.68) v 62% (3.0) in control, p<0.03). This protection was abolished by LY 294002 (61% (6.7), p = NS), but not U0126 (42% (5.0), p<0.05). Akt and Erk1/2 phosphorylation were also increased in metformin-treated hearts. b) Isolated adult cardiomyocytes were subjected to a reactive oxygen species-induced cell model of reperfusion injury. By using confocal microscopy we found that metformin increased the time to MPTP opening from 217 (20) sec to 343 (29) sec (p<0.03) and rigor contracture from 558 (38)s to 871(40)s (p<0.05), compared with control, therefore delaying the cell death. This effect was abolished by prior incubation with LY 294002 (188 (20)s; 687 (70)s; p = NS), but not with U0126 (442 (41)s; 1131 (97)s; p<0.03) again indicating a role for the PI3K, but not the Erk1/2 pathway.
Conclusions: This is the first study to demonstrate that metformin has direct protective properties against ischaemia-reperfusion injury, and appears to act via inhibiting MPTP opening, linked to the PI3-Kinase/Akt dependent pathway. This finding may account for some of the beneficial effects observed in the UKPDS study, and suggests a new indication as first line oral therapy of type 2 diabetics.
reperfusion injury; metformin; PI3 Kinase/Akt pathway
163 INCIDENCE AND PROGNOSIS OF VENTRICULAR ARRHYTHMIAS
D. Chase1, P. Roderick1, R. Milne1, J. Morgan2.1University of Southampton, Southampton, UK; 2Southampton University Hospitals, Southampton, UK
Objectives: To estimate the incidence rate of diagnosed symptomatic ventricular arrhythmia and assess prognosis.
Methods: A prospective population based cohort study. Cases were consecutive adults with newly diagnosed sustained ventricular tachycardia, inducible ventricular tachycardia, non-sustained ventricular tachycardia and survivors of out of hospital cardiac arrest with ventricular tachycardia as presenting rhythm. Patients were prospectively identified at Southampton NHS Trust Hospitals and the Royal Hampshire County Hospital over 11 months and followed up for 12 months. Multiple sources were used to identify cases including use of diagnostic test results, Emergency and Coronary Care Unit admissions. Postcode analysis was used to link patients to a defined catchment population. Participants were sent a brief questionnaire about themselves and two standardised quality of life questionnaires (SF-36 and the syncope functional status questionnaire). Medical notes were reviewed for information on previous medical history, presentation and health care management during follow up. Results: 84 cases were identified over 11 months in a population of 450 959 adults; with an annual incidence rate of 202 per million population (pmp) (95% CIs, 164, 248). For males, the incidence rate was 273 pmp (95% CIs, 210, 356) and 137 pmp (95% CIs, 95, 197) for females. There was a steep increase in incidence with age (p<0.0001). The incidence of life threatening ventricular arrhythmias was 62 pmp (95% CI 43, 90) and 140 pmp (109, 179) for non-sustained ventricular tachycardia. 71% of patients with life threatening ventricular arrhythmias had an Implantable Cardioverter Defibillator implanted. 88% of cases survived for 12 months. A statistically significant improvement in the SF-36 mental health sub-scale was reported.
Conclusions: This is the first UK study of the epidemiology of ventricular arrhythmias. About one third of cases were life threatening. However, there were fairly wide confidence intervals around estimates due to the small number of cases. The survival experience was good and quality of life showed improvement.
incidence; prognosis; ventricular arrhythmias
164 LEPTIN, THE OBESITY-ASSOCIATED HORMONE, EXHIBITS DIRECT CARDIOPROTECTIVE EFFECTS
C. Smith, M. Mocanu, S. Davidson, A. Wynne, J. Simpkin, D. Yellon.The Hatter Cardiovascular Institute, University College London, London, UK
Introduction: Protection against ischaemia-reperfusion injury has been linked to activation of the PI3K-AKT and p44/42 signalling cascades, collectively termed the Reperfusion Injury Salvage Kinase (RISK) pathway. Leptin, an adipocytokine that regulates appetite and energy balance, also promotes myocyte proliferation via PI3K-AKT and p44/42 activation. We hypothesised, therefore, that leptin may exhibit direct cardioprotective activity through the RISK pathway and employed two experimental models to test this theory.
Methods: Firstly, the influence of leptin (10 nM), administered at reperfusion following global ischaemia, was examined in a mouse Langendorff perfused heart model, infarct size being assessed by tetrazolium staining and signalling protein phosphorylation by Western blot analysis. Secondly, the actions of leptin on mitochondrial permeability transition pore (MPTP) opening, a possible determining factor in cardioprotection, were studied in rat cardiomyocytes utilising a model of oxidative stress in which cells are preloaded with tetra-methyl rhodamine methyl ester (TMRM) and then subjected to laser stimulation resulting in reactive oxygen species (ROS) generation and leading to MPTP opening and cardiomyocyte contracture.
Results: Leptin reduced infarct size significantly (26.4 (2.62)% v 50.9 (3.2)% for control, p<0.01). Experiments with the kinase inhibitors LY294002 and UO126 indicated that the actions of leptin were mediated via activation of PI3K-AKT and p44/42, i.e. protection was blocked by either LY294002 (51.6 (4.9)% v 50.9 (3.2)% for control) or UO126 (55.0 (2.64)% v 50.9 (3.2)% for control). Western blot analysis confirmed that leptin stimulated AKT (+33.1%, NS) and p44/42 (p44/42, +29.8%, p<0.05 ; p42, +42.9%, p<0.02) phosphorylation and that this was also blocked by LY294002 and UO126, respectively. In rat cardiomyocytes, under control conditions, the time until MPTP opening was 243 (16)s and the time until contracture 682 (74)s. Leptin delayed these times significantly, values for MPTP opening and cardiomyocyte contracture of 337 (13)s (p<0.05) and 829 (110)s (p<0.05), respectively, being obtained. Again the PI3K inhibitor LY294002 and MEK inhibitor 1, an upstream inhibitor of p44/42, blocked these actions.
Conclusions: Our data indicate for the first time that leptin, the obesity-associated hormone, has direct cardioprotective properties that involve the RISK pathway.
leptin; cardioprotection; cell signalling
165 CARDIAC REHABILITATION IMPROVES LONG-TERM SURVIVAL AFTER ACUTE CORONARY SYNDROME
K. Viswanathan1, N. Artis1, K. Bailey1, C. Morrell1, R. Das1, N. Kilcullen1, J. Barth2, A. Hall1.1University Of Leeds, Leeds, UK; 2Leeds General Infirmary, Leeds, UK
Objective: To assess the impact of cardiac rehabilitation on the long-term mortality of patients with acute coronary syndrome (ACS) and across each of the British Cardiac Society (BCS) categories of ACS.
Design: Prospective observational registry.
Setting: 11 adjacent hospitals in the West Yorkshire region.
Methods: The EMMACE-2 study included 2461 consecutive consenting patients validated to have acute coronary syndrome during a 6-month period (28 April 2003 to 28 October 2003). Demographic, clinical and treatment variables were collected on all patients and their mortality was monitored through the Office of National Statistics. 2067 patients, who were discharged alive from hospital and on whom data on referral for cardiac rehabilitation was available, were included in the analysis. Patients were also analysed in each of the 4 categories based on the BCS working group definition: Unstable angina, Troponin positive ACS (evidence of myocyte necrosis), Non-ST elevation myocardial infarction (NSTEMI) and ST elevation myocardial infarction (STEMI). Median follow-up was 786 days.
Results: Referral for cardiac rehabilitation was an independent predictor of long-term all-cause mortality among patients discharged alive from hospital (hazard ratio (HR) 1.665 (1.372 to 2.02), p <0.001). After multivariate analysis (using a Cox proportional hazards model) with correction for age, heart rate and systolic blood pressure (BP), cardiac rehabilitation remained a significant predictor of long-term mortality (HR 1.26 (1.03 to 1.53), p = 0.02).
Patients referred for rehabilitation are less likely to die across all BCS categories of ACS (fig 1; table 1). Figure 1 shows the mortality (in percentage) of patients referred for and not referred for cardiac rehabilitation across the various BCS categories of ACS. Table 1 shows the significance and hazard ratios in each of the categories on univariate analysis.
Abstract 165
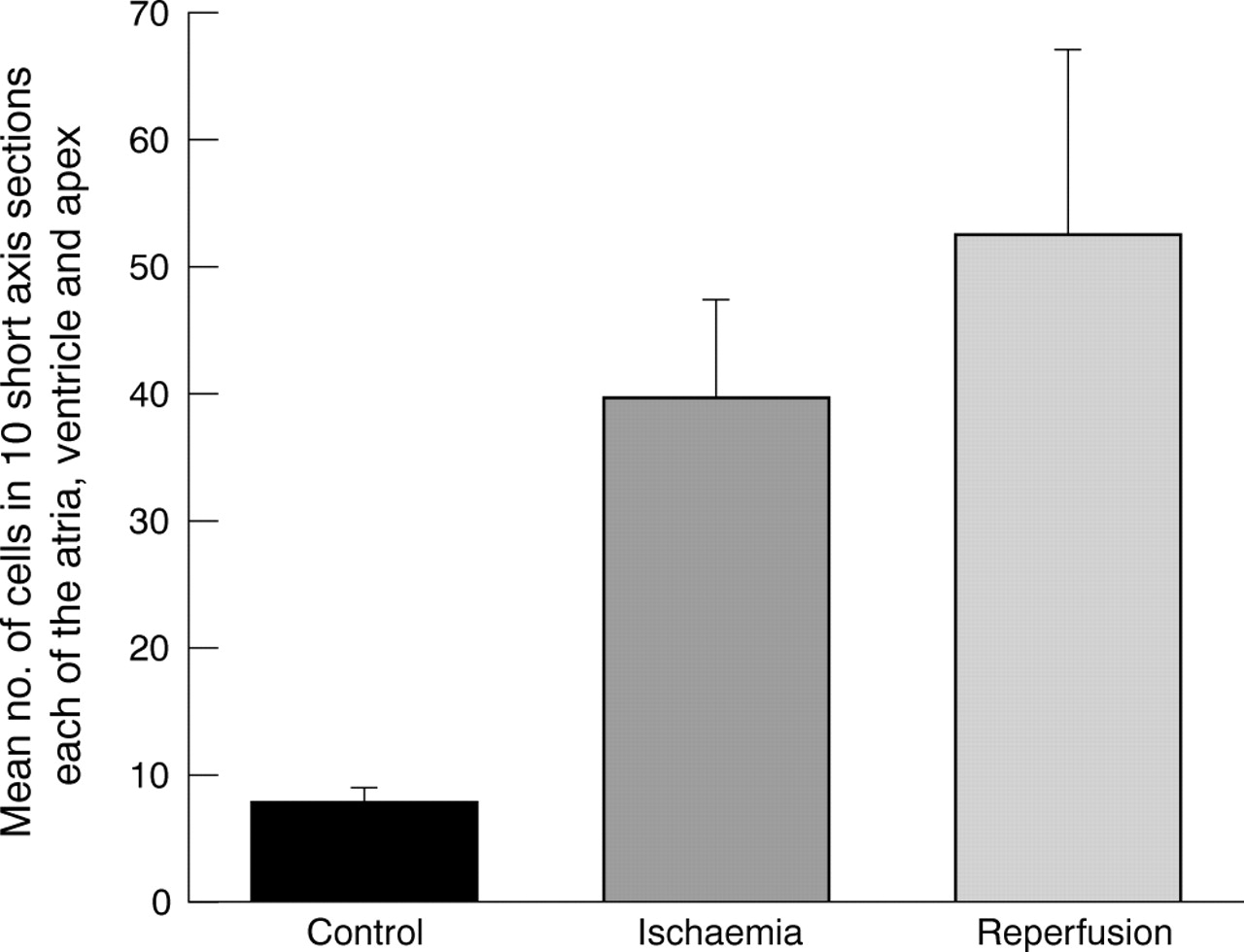
Abstract 165
Only 34% patients diagnosed with troponin positive ACS (153 of 452) had been referred for cardiac rehabilitation as compared with 69% of those diagnosed as NSTEMI (527 of 765). This is notable given the fact that the long-term mortality following discharge from hospital in patients with troponin positive ACS is comparable with that of patients diagnosed with NSTEMI (22.6% v 21.8%)
Conclusion: Cardiac rehabilitation improves long-term survival in patients with acute coronary syndrome and should be offered to all patients with evidence of myocyte necrosis or myocardial infarction.
acute coronary syndrome; rehabilitation; mortality
166 OPTIMISING DOOR-TO-BALLOON TIMES IN PRIMARY PERCUTANEOUS CORONARY INTERVENTION: UK EXPERIENCE
M. Dorsch, C. Priestley, J. Blaxill, J. McLenachan, A. Mackintosh, U. Sivananthan, J. Greenwood, D. Blackman.Yorkshire Heart Centre, Leeds, UK
Introduction: Primary percutaneous coronary intervention (PCI) is a superior treatment strategy to thrombolysis for ST-segment elevation myocardial infarction (STEMI), but must be provided promptly. American College of Cardiology/American Heart Association and European Society of Cardiology guidelines recommend a target of 90 minutes from initial medical contact to balloon inflation. We evaluated door-to-balloon times for the first 8 months after institution of 24/7 primary PCI in a large UK tertiary centre.
Methods: After a brief local roll-in, all patients presenting with STEMI in Leeds (population 800 000) from 1 April 2005, both to the tertiary centre (TC) with on-site PCI, and to the other city hospital requiring transfer (DGH), were referred for primary PCI as part of the National Infarct Angioplasty Pilot. Door-to-balloon, door-to-referral, referral-to-catheter laboratory and lab-to-balloon times were recorded for each individual patient. Times were compared according to presenting hospital, working hours (09:00–17:00) v out-of-hours, and weekdays v weekend. Results were reviewed on a monthly basis, identifiable sources of delay addressed, and systems changed to enhance speed of PCI delivery. All times quoted are medians.
Results: 136 patients (62 (12) years, 67% male) were treated over an 8-month period, 76 (56%) from TC and 60 (44%) from DGH. Door-to-balloon times improved progressively from 112 mins in the first 2 months to 91 mins in the final 2 months (p<0.05), entirely as a result of a reduction in referral-to-laboratory time (fig 1). Door-to-balloon times were longer in patients presenting to DGH v TC (107 v 98, p = 0.09) weekday out-of-hours v in-hours (107 v 84, p<0.01) and weekend v weekday (106 v 98, p = 0.54).

Abstract 166
Conclusions: Door-to-balloon times progressively improved to achieve target level of 90 minutes via a reduction in time from accident and emergency department (A&E) referral to arrival in the catheter laboratory. Required improvements in door-to-balloon times for DGH and out-of-hours patients may be attained by planned introduction of direct ambulance referral to the tertiary centre and on-site staff on-call. We believe that prompt, effective 24/7 primary PCI is deliverable in a UK setting.
primary percutaneous coronary intervention; acute myocardial infarction; angioplasty
167 CAN EXISTENT NHS SERVICES BE MODIFIED TO DELIVER AN EFFICIENT PRIMARY ANGIOPLSTY SERVICE? PRELIMINARY RESULTS FROM A PRIMARY ANGIOPLASTY MODEL IN SOUTH LONDON
J. Byrne, N. Melikian, S. Basavarajaiah, M. Thomas, R. Wainwright, J. Hill, A. Shah, P. MacCarthy.Cardiology Department, King’s College Hospital, London, UK
Introduction: Primary percutaneous coronary intervention (PCI) as a treatment for ST-segment elevation myocardial infarction (STEMI) has been shown to be safe and superior to thrombolysis. However, the healthcare system in the UK has been slow to adopt this strategy as first line management for STEMI. Absence of an existing efficient working model and cost implications of providing a 24-hour, seven-days-a week primary PCI service within the existent NHS framework have been two major deterrents for provision of such a service. We report on our experience of providing a 24/7 primary PCI service over a 25-month period using a ‘Hub’ (cardiothoracic centre) and ‘Spoke’ (feeding district general hospitals) model in an urban (central London) setting.
Methods and results: From September 2003 STEMI patients presenting to King’s College Hospital (KCH – ‘Hub Hospital’) were treated with primary PCI. From April 2005 this service was sequentially extended to include all STEMI patients presenting to Lewisham (UHL) and Princess Royal (PRUH) University Hospitals (‘Spoke Hospitals’ – transferred via ambulance to KCH cardiac catheter laboratory) and patients suspected/diagnosed (ECG based) by paramedical ambulance crew of having STEMI who were transferred directly from home to the cardiac catheter laboratory (DIRECT).
234 patients presented to the service (KCH 158, UHL 37, PRUH 10, DIRECT 29). Median age of patients was 63 years (35–95) and 70% were male. 25% of patients presented at weekends or on a bank holiday. Distribution of presentation times were: 00:00–04:00: 3%, 00:40–08:00: 9%, 08:00–12:00: 18%, 12:00–16:00: 30%, 16:00–20:00: 17% and 20:00–24:00: 13%. Mean time from onset of pain to arrival in A&E and/or of paramedic team (direct transfers) was 199 (299) minutes (median 120 minutes). Angiography was performed in 224 (95%) patients (reason for not undergoing angiography: 3 thrombolysed, 2 deaths and 2 strokes before angiogram, 1 patient refusal, 2 non cardiac cases) and primary PCI was performed in 196 (84%) patients (reason for not having primary PCI: 3 pericarditis, 15 unobstructed coronary arteries, 6 PCI technically not possible, 4 underwent/recommended to have CABG). Median transfer times between KCH/UHL/PRUH A&E and direct transfer from home to the cardiac catheter laboratory were within accepted guidelines of <90 minutes (table 1).
Significantly, primary PCI resulted in a dramatic fall in mean inpatient length of stay for KCH (3.4 days), UHL (3.2 days) and PRUH (2.2 days) patients in comparison with length of stay for patients undergoing thrombolysis for STEMI in the 6-month period leading to the start of the primary PCI service at KCH (10.2 days).
Conclusion: Our pilot data show that a “real world” primary PCI service can be delivered safely and according to recommended guidelines by modifying existent NHS services. Furthermore, primary PCI significantly reduces inpatient hospital stay with direct reductions in cost.
Abstract 167
primary angioplasty; length of stay; NHS
168 PRIMARY ANGIOPLASTY PERFORMED “OUT-OF-HOURS” HAS THE SAME OUTCOMES AS FOR PATIENTS “IN-HOURS”
B. Kunadian, K. Vijayalakshmi, J. Dunning, A. Thornley, A. Sutton, D. Muir, R. Wright, J. Hall, M. deBelder.The James Cook University Hospital, Middlesbrough, UK
Background: Given the benefits of primary percutaneous coronary intervention (PPCI), many hospitals in the UK have started a PPCI service for patients presenting with AMI. Some centres have adopted a policy of PPCI during standard working hours and thrombolysis out-of-hours because of logistic constraints. Some centres have reported worse outcomes for patients treated out-of-hours. This might relate to inherent delays in activating an on-call team. We performed this study to compare the characteristics of patients and their outcomes depending on the time of treatment.
Methods: We studied 299 patients undergoing PPCI or facilitated PCI within 24 hours of symptom onset for documented ST elevation myocardial infarction from August 2003 to October 2005.
Results: A total of 116 (39%) patients presented in-hours (group 1) and 183 (61%) presented out-of-hours (group 2). There were no differences in baseline characteristics (age, previous AMI, DM, HT, admission cholesterol, smoking status, cardiogenic shock) except there were more women (group 2: 32% v group 1: 21%; p = 0.04) in group 2. Target vessels and patients with multivessel disease were similar in both groups. TIMI 3 flow pre- and post-PCI was similar (see table 1). PCI success and complication rates were similar in both groups. Treatment delays were similar for both groups. The 30-day mortality for patients treated out-of-hours was no different to outcomes for group 1, regardless of whether they were in shock or not. In multivariate analysis by logistic regression, age (odds ratio (OR) 1.08, 95% confidence interval (CI) 1.01 to 1.17, p = 0.4), diabetes (OR 19.9, 95% CI 3.5 to 114), hypercholesterolemia (OR 4.2, 95% CI 1.08 to 16.4), shock (OR 59.7, 95% CI 11.9 to 300), LAD territory infarct (OR 4.9, 95% CI 1.2 to 20.4) were independent predictors of 30-day mortality but out-of-hours PCI was not an independent predictor of 30-day mortality. Group 2 patients had a significantly longer length of stay during the index hospitalisation (8 (13) days v 5.7 (4) days for group 1, p = 0.04).
Conclusions: Patients treated out of working hours tend to stay longer during the index hospitalisation but treatment success and mortality rates were similar to those for patients treated in-hours. Patients presenting out-of-hours at experienced centers should be routinely offered PPCI.
Abstract 168
STEMI; primary angioplasty; out-of-hours
169 CIRCUMSTANCES AND MODE OF IN-HOSPITAL DEATH IN 9914 CONSECUTIVE PATIENTS UNDERGOING PERCUTANEOUS CORONARY INTERVENTIONS IN THE NORTHWEST OF ENGLAND: IN STENT ERA
S. Rathore1, S. Sastry2, P. T. Gray3, R. Beynon4, D. A. Grayson1, M. Jackson1, A. R. Perry1.1The Cardiothoracic Centre, Liverpool, UK; 2Blackpool Victoria Hospital, Blackpool, UK; 3Manchester Royal Infirmary, Manchester, UK; 4South Manchester University Hospital, Manchester, UK
Background: Some deaths after percutaneous coronary interventions (PCI) occur in high-risk situations e.g. shock, whereas others are unexpected and related to procedural complications. Several studies available have been mainly focused on the issue of unsupported or primary angioplasty and predates high stent usage. To better describe the epidemiological causes of death after PCI in present era, we undertook a systematic review of all in-hospital deaths following PCI in northwest of England from 2001 to 2004.
Methods: Sixty-two deaths were identified from 9914 consecutive PCI undertaken during the study period. The medical records of four patients were missing and, leaving 58 patients to be reviewed with a standardised data extraction tool to determine the circumstance of death e.g. death resulting from procedural complication, pre-existing cardiac disease and non cardiac disease and a mode of death (e.g. low output failure, arrhythmia, renal failure,stroke, respiratory failure and others). Medical records were reviewed at each centre and cases were discussed at regional consensus meetings. All the collected data were validated by random crosschecking of data by exchange site visits. Multivariate logistic regression was used to identify risk factors for deaths related to procedural complications.
Results: Overall in-hospital mortality was 0.6%. The circumstance of death was a procedural complication in 35 patients (60.3%), and pre-existing acute and chronic cardiac disease and non cardiac disease in 23 patients (39.7%). Low output failure was the most common mode of death occurring in 42 patients (72.4%). Other modes of deaths included ventricular arrhythmias (13.8%), renal failure (5.2%), stroke (1.7%), respiratory failure (1.7%), ventricular rupture (1.7%), and other (3.5%). Significant predictors of death from procedural complication were treatment of left main stem disease (OR 10.3, 95% CI 3.4–30.8, p<0.001), treatment of bypass graft disease (OR 4.9, 95% CI 1.8–13.3, p<0.001), ejection fraction <50% (OR 5.0, 95% CI 2.5–9.8, p<0.001), and female sex (OR 3.4, 95% CI 1.7–6.7, p<0.001).
Results: Procedural complications account for over half of all post PCI in-hospital deaths. Other deaths are directly ralated to patient acuity or non cardiac, co-morbid conditions. We have identified several risk factors for in-hospital mortality following PCI in present stent era which may help reduce number of deaths realted to procedural complications.
PCI; in-hospital death; procedural complications
170 LONG TERM ALL CAUSE MORTALITY IN CONTEMPORARY ACUTE CORONARY SYNDROME PATIENTS (ST ELEVATION MYOCARDIAL infarction V BUNDLE BRANCH BLOCK MYOCARDIAL INFARCTION)
N. Artis1, K. Bailey1, K. Viswanathan1, C. Morrell1, J. Barth2, R. Das1, N. Kilcullen1, C. Pepper2, A. Hall1.1University of Leeds, Leeds, UK; 2Leeds General Infirmary, Leeds, UK
Objective: To assess the impact of admission ECG on long-term mortality.
Design: Prospective observational registry.
Setting: 11 adjacent hospitals in the West Yorkshire region.
Patients: 2461 consecutive patients with confirmed acute coronary syndrome (ACS) were identified during a 6-month period (28 April 2003 to 28 October 2003). Demographic, clinical and treatment variables were collected on all patients and their all cause mortality was monitored through the Office of National Statistics. 2251 patients had the required data available and were included in the analysis. Patients were divided into: Marker negative ACS, Marker positive ACS, percutaneous coronary intervention, non-ST elevation myocardial infarction (NSTEMI), ST elevation myocardial infarction (STEMI), BBB-ACS and BBB-MI. We now have mortality data extending to 2 years.
Results: Figure 1 shows the all cause mortality of the separate groups with number of deaths/number in group. The age, heart rate and blood pressure adjusted hazard ratios (confidence intervals) and p values for the separate groups in relation to marker negative ACS are: STEMI 1.21 (0.86–1.69) p = 0.26(ns), Marker positive ACS 1.19 (0.87–1.64) p = 0.25(ns), NSTEMI 1.35 (1.01–1.81) p<0.05, BBBMI 1.66 (1.12–2.47) p = 0.01, BBBACS 1.85 (1.17–2.91) p = 0.008.
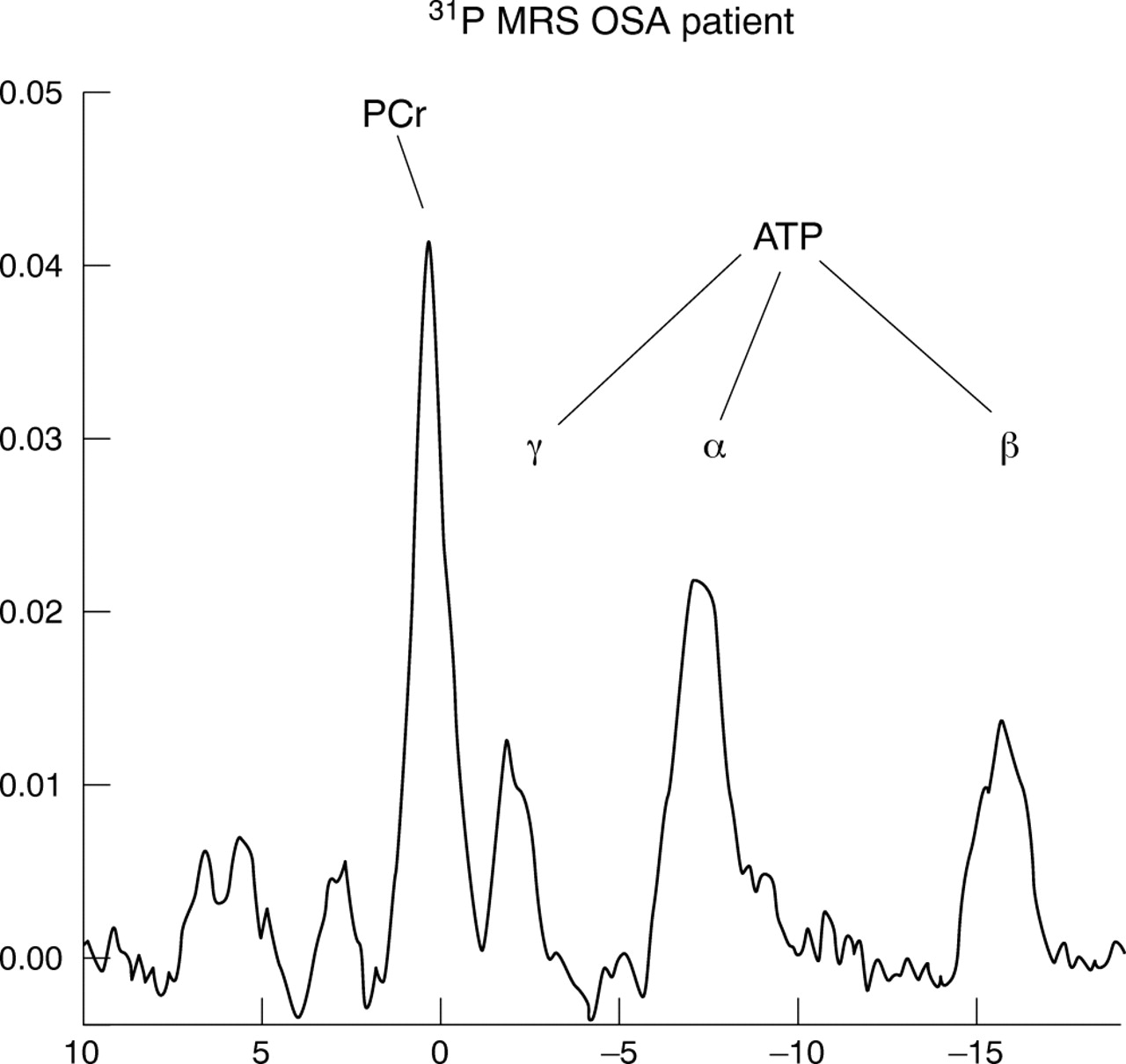
Abstract 170
Conclusions: The worst mortality is seen among those who present with LBBB on their admission ECG. The most favourable outcome if markers are elevated is within the STEMI group. Interestingly the marker negative ACS group have a 2-year mortality approaching that of STEMI. Often the prime focus of rehabilitation and secondary prevention is the STEMI group of patients. It may be this focus of resources that improves the prognosis and perhaps we should be doing more to promote health in the BBB group.
acute coronary syndrome; bundle branch block; mortality
171 HOSPITAL VOLUME OF THROUGHPUT AND PERI-PROCEDURAL AND MEDIUM TERM OUTCOMES FOLLOWING PCI: PROSPECTIVE COHORT STUDY OF ALL 17 417 PROCEDURES UNDERTAKEN IN SCOTLAND BETWEEN 1997 AND 2003
K. Burton1, R. Slack2, K. Oldroyd3, A. Pell4, A. Flapan5, I. Starkey6, H. Eteiba7, K. Jennings8, R. Northcote9, S. Hillis3, J. Pell10.1University of Calgary, Calgary, Canada; 2Greater Glasgow NHS Board, Glasgow, UK; 3Western Infirmary, Glasgow, UK; 4Monklands Hospital, Airdrie, UK; 5Royal Infirmary, Edinburgh, UK; 6Western General Hospital, Edinburgh, UK; 7Glasgow Royal Infirmary, Glasgow, UK; 8Aberdeen Royal Infirmary, Aberdeen, UK; 9Victoria Infirmary, Glasgow, UK; 10University of Glasgow, Glasgow, UK
Introduction: More hospitals now offer percutaneous coronary intervention (PCI). Undertaking sufficient to maintain expertise must be balanced against equalities in access. Studies disagree on whether periprocedural complications vary by hospital volume, and medium-term outcomes have not been studied.
Methods: We examined all PCIs in Scotland between 1997 and 2003. Linkage to administrative databases identified events over two years follow up. We compared the risk of events by hospital volume at 30 days and 2 years using logistic regression and Cox proportional hazards models.
Results: Of the 17 417 PCIs, 4900 (28%) were in low volume hospitals and 3242 (19%) in high volume. Following adjustment for case-mix, there were no significant differences in risk of death or myocardial infarction. Patients treated in high volume hospitals were less likely to require emergency surgery (adjusted OR 0.18, 95% CI 0.07–0.54, p = 0.002). Over two years, patients in high volume hospitals were less likely to undergo surgery (adjusted hazard ratio 0.52, 95% CI 0.35–0.75, p = 0.001), but this was offset by an increased likelihood of further PCI. There was no net difference in coronary revascularisation, or overall events.
Conclusions: Death and myocardial infarction are infrequent complications of PCI and did not differ significantly by volume. Emergency surgery for acute occlusion or dissection was less common in high volume hospitals. Over two years, patients treated in high volume centres were as likely to undergo some form of revascularisation, but less likely to undergo surgery.
health services research; percutaneous coronary intervention; volume of throughput
172 ANGIOPLASTY FOR UNSTABLE ANGINA AND NON ST ELEVATION MYOCARDIAL INFARCTION IN THE OVER 75S: DIFFERENT FEATURES, DIFFERENT MANAGEMENT, DIFFERENT OUTCOMES
A. Thornley, B. Kunadian, M. Cunnington, R. Wright, D. Muir, A. Sutton, J. Hall, M. de Belder.James Cook University Hospital, Middlesbrough, UK
Background and Aims: The elderly have been under-represented in studies showing a benefit in favour of early revascularisation in patients presenting with Non ST Elevation Myocardial Infarction (NSTEMI) or unstable angina and represent a higher risk cohort. This study compared the clinical characteristics and procedural results of three age groups of patients undergoing PCI in this setting.
Methods: A retrospective analysis of all patients undergoing PCI for NSTEMI or unstable angina over 36 months from 1 September 2002. Patients were divided in to three age groups: group A - under 65; group B - 65–75 years; group C - over 75.
Results: During this period 1810 PCIs were performed in patients with NSTEMI or unstable angina (group A = 1035, group B = 604, group C = 171). Group C had more women (240 (23.2%) group A v 207 (34.3%) group B v 71 (41.5%) group C, p<0.001) and fewer current smokers (524 (50.6%) v 123 (20.4%) v 8 (4.7%), p<0.001). Group C patients were more likely to have had a previous myocardial infarction (242 (23.4%) group A v 188 (31.1%) group B v 75 (43.9%) group C, p<0.001); have peripheral vascular disease (65 (6.3%) v 74 (12.3%) v 32 (18.7%), p<0.001); cerebrovascular disease (43 (4.2%) v 54 (8.9%) v 18 (10.5%), p<0.001) or to be hypertensive (447 (43.2%) v 352 (58.3%) v 118 (69.0%), p<0.001). Group A patients were less likely to have had previous CABG (56 (5.4%) group A v 61(10.1%) group B v 15 (8.8%) group C, p = 0.001) or diabetes mellitus (133 (12.9%) v 112 (18.5%) v 31 (18.1%), p = 0.005). Admission cholesterol levels of groups B and C were higher than for group A patients (5.02 group A v 4.58 group B (p<0.001 v group A) v 4.35 group C (p<0.001 v group A)). There was a longer delay between symptom onset and PCI in the elderly (226.5 hours group A v 259.5 group B (p = 0.003 v group A) v 270.9 group C (p = 0.008 v Gp A)). Culprit vessels were similar but other angiographic and procedural variables differed (table 1): a GP IIb/IIIa inhibitor was used less frequently and an intra aortic balloon pump used more frequently in the elderly. Older patients were more likely to undergo balloon angioplasty alone but were just as likely to be treated with drug eluting stents. Procedural success was lower and hospital stay was longer in group C (1.85 days group A v 2.69 days group B (p<0.001 v group A) v 4.46 days group C (p<0.001 v group A, p = 0.005 v group B)). Mortality rates were higher in the older group both in hospital and at 30 days.
Conclusions: Older patients undergoing PCI with NSTEMI or unstable angina have different admission characteristics to younger patients. There is a longer delay between symptom onset and treatment and they have significantly worse outcomes. In relation to informed consent quoted mortality rates should be varied depending on patient age.
Abstract 172
acute coronary syndromes; angioplasty; elderly patients
173 IN-PATIENT ANGIOPLASTY IMPROVES LONG-TERM SURVIVAL IN ACUTE CORONARY SYNDROME
K. Viswanathan1, K. Bailey1, N. Artis1, C. Morrell1, R. Das1, N. Kilcullen1, J. Barth2, J. McLenachan2, A. Hall1 On behalf of the EMMACE-2 Investigators1University of Leeds, Leeds, UK; 2Leeds General Infirmary, Leeds, UK
Objective: To assess the impact of inpatient angioplasty on long-term mortality.
Design: Prospective observational registry.
Setting: 11 adjacent hospitals in the West Yorkshire region.
Methods: The EMMACE-2 study included 2484 consecutive patients confirmed to have acute coronary syndrome (ACS) during a 6-month period (28 April 2003 to 28 October 2003). Out of these, 2154 patients who were discharged alive were included in the analysis. Demographic, clinical and treatment variables were collected on all patients and their mortality was monitored through the Office of National Statistics. Median long-term follow-up was 786 days at the time of analysis.
Results: Out of 2154 patients discharged alive, 248 had inpatient coronary angioplasty and 59 had inpatient CABG. We found that inpatient angioplasty was a significant predictor of long-term all cause mortality among patients discharged alive (hazard ratio (HR) 0.20 (0.11 to 0.35), p<0.001). When the analysis was extended to include patients who had inpatient CABG (inpatient revascularisation vs. no inpatient revascularisation) the effects remained highly significant (HR 0.18 (0.11 to 0.31), p<0.001).
Even after correcting for confounding factors (age, heart rate, systolic blood pressure) in a multivariate Cox proportional Hazards model, the effect remained highly significant. Inpatient angioplasty v No inpatient angioplasty (HR = 0.42 (0.24 to 0.76), p = 0.004); Inpatient revascularisation v No inpatient revascularisation (HR = 0.36 (0.21 to 0.61), p<0.001).
Similar results were noted when the analysis included the patients who had died in hospital. Further analyses across various categories of ACS by BCS definition showed that the effects were significant across each of the three categories: STEMI, NSTEMI and ACS with myocyte necrosis (all p<0.001) but not in those with unstable angina without evidence of myocyte necrosis (p = 0.739).
Conclusion: Inpatient angioplasty appears to improve long-term survival in all patients with ACS with evidence of myocyte necrosis including those with clinical myocardial infarction.
acute coronary syndrome; angioplasty; mortality

Abstract 173
174 ANGINA AND GENDER: INCIDENCE AND PROGNOSIS IN 118 523 CASES IN AMBULATORY CARE
H. Hemingway1, A. McCallum2, M. Shipley1, K. Manderbacka2, P. Martikainen3, I. Keskimaki2.1University College London Medical School, London, UK; 2National Research and Development Centre for Welfare and Health (STAKES), Helsinki, Finland; 3University of Helsinki, Helsinki, Finland
Introduction: Angina in women has often been considered a “soft” diagnosis, with “real” coronary disease predominantly affecting men, but large scale population studies have been lacking.
Objective: To determine gender differences in the incidence and prognosis of angina.
Design: Prospective cohort study using linked national registries, with median 4-year follow up.
Setting: All primary care providers in Finland.
Participants: Among patients aged 45–89 years who had no previous history of coronary disease, we defined new cases of angina based on nitrate prescription (56 441 women, 34 885 men) or abnormal invasive or non-invasive test result (11 391 women and 15 806 men).
Main Outcome Measures: Fatal and nonfatal myocardial infarction.
Results: The age standardised annual incidence per 100 population of all cases of angina was 2.03 in men and 1.89 in women with a sex ratio 1.07 (95% CI 1.06–1.09). Among angina cases, absolute rates of outcome tended to be lower among women, but this gender difference was diminished or absent among patients with diabetes, higher doses of nitrates, or at least two co-morbid non-cardiovascular conditions. Among diabetics with test positive angina, age standardised coronary event rates were 9.9 per 100 person years in women v 9.3 in men (p = 0.69). At every age, nitrate angina in women and men was associated with a similar increase in risk of coronary mortality relative to the general population. Women with test positive angina aged <75 years had higher coronary standardised mortality ratios than men; among those aged 55–64 it was 4.69 (95% CI 3.60–6.11) in women, compared with 2.40 (95% CI 2.11–2.73) in men, p for interaction <0.0001.
Conclusion: Angina in women has a similarly high incidence to that in men, is associated with increased coronary mortality relative to women in the general population and, among easily identifiable clinical subgroups, has similarly high absolute rates of prognostic outcomes compared with men.
angina pectoris; gender; prognosis
175 SELECTED HUMAN ADULT BONE-MARROW AND UMBELICAL CORD-BLOOD DERIVED CD133+ CELLS EXPRESS MYOCARDIAL PROTEINS FOLLOWING IN VITRO DIFFERENTIATION
S. Meyrick1, P. Denning-Kendall2, R. Ascione1.1Bristol Heart Institute, University of Bristol, Bristol, UK; 2University of Bristol, Bristol, UK
Objective: To investigate the potential for in vitro differentiation of selected human bone marrow and cord blood derived CD133+ cell into cells expressing cardiac proteins.
Methods: Bone marrow (10 donors) and cord blood (16 donors) derived CD133+ cells were immunomagnetically isolated, with the use of Miltenyi Biotec MiniMACS kits (Milteny Biotec, Germany) from mononuclear cell preparations. Bone marrow and cord blood derived CD133+ cells were cultured for 4 days in fibronectin-coated chamber slides at a concentration of 5×105 cells/well in DMEM media containing 10% FBS, 1× endothelial cell growth supplement, 20 nmol/L retinoic acid, 1 mol/L dexamethasone, 0.14 mol/L prostaglandin-E2, 0.6 nmol/L interleukin-2, 3.3 nmol/L FGF4, and 1.9 nmol/L BMP4. Prior and after culture, isolated CD133 fractions were immunophenotyped. The antibody panel used included the haemopoietic marker CD133 and the cardiac markers Troponin I and actinin.
Results: Following isolation, a purity of 82% and 92.8% was achieved for bone marrow and cord blood derived cells, respectively. Immunophenotyping prior culture demonstrated the expression of CD133+ marker (71% and 79% for bone marrow and cord blood derived cells respectively) and undetectable expression of cardiac markers. Immunophenotyping after culture demonstrated undetectable expression of the CD133+ marker, while 11.6% of CB and 6.2% of bone marrow derived CD133+ cells expressed the cardiac protein Troponin I (p<0.05). Furthermore, 5.1% of cord blood and 2.3% of bone marrow derived cells expressed the cardiac protein actinin (NS).
Conclusion: Selected human adult bone-marrow and umbilical cord-blood derived CD133+ cells express cardiac proteins following in vitro differentiation in an appropriate medium. Cord-blood derived cells are more effective than bone-marrow derived cells in expressing cardiac proteins.
adult stem cell; myocardial repair; in vitro differentiation
176 LOCALISATION OF BONE MARROW MONONUCLEAR CELLS ADMINISTERED DURING ACUTE MYOCARDIAL INFARCTION; THE EFFECTS OF TIME IN CULTURE
M. Lovell1, M. McDonald2, A. Sivarajah2, N. Wright3, C. Thiemermann2, A. Mathur1.1Barts and The London/Clinical Pharmacology/William Harvey Research Institute, London, UK; 2Centre for Experimental Medicine/William Harvey Research Institute, London, UK; 3Barts and The London/Histopathology Department, London, UK
Introduction: Bone marrow mononuclear cells (BMMNCs) improve left ventricular function when administered following myocardial infarction. Opinions vary as to the mechanism of action of these cells and even how these cells reach the damaged myocardium. Several published reports suggest that the cells home towards signals released in response to ischaemia and hence that the cells should be administered as soon as possible after infarction. While other articles comment that the injected cells ability to home, engraft and survive may be impaired by the hypoxic and inflammatory environment in acute infarction. Thus suggesting cells should be given some days after infarction. We sort to clarify the exact parts of the heart these cells home to following infarction. If there was a tendency towards ischaemic or non-ischaemic segments this would help clarify the current situation. In addition, injecting cells sometime after infarction necessitates maintaining cells in tissue culture. We also aimed to analyse the effects of time spent in culture on the ability of BMMNCS to home to the myocardium in acute infarction.
Hypothesis: 1) BMMNCs will home to the site of injury when administered in myocardial infarction. 2) Prolonged culture will allow the development of a mature phenotype that improves homing and engraftment.
Methods: Rat BMMNCs were collected using a percoll density gradient and fluorescently labelled with a cell tracker dye. Myocardial infarction was induced in Wistar rats by ligation of the left anterior descending artery for 30 mins; this was followed by 6 hours of reperfusion. Animals received the cells via the jugular vein and were injected either following 24 h or 72 h of tissue culture. Sham operated animals injected with BMMNCs acted as controls. All tissues were fixed in formalin and paraffin embedded. Homed cells were detected in myocardial tissue with fluorescent microscopy and subsequently quantified by region. Ten sections of the atria, ventricle and apex were quantified for each animal.
Results: There was a significant increase in cells homing to all segments of the infarcted hearts compared to the sham operated hearts (p<0.05), (fig 1). In addition there was a significant increase in cells found in the infarcted hearts ventricle segments over the atrial segments, (fig 1) (p<0.05). Cells cultured for only 24 h homed to the heart significantly more than those cultured for 72 h (p<0.05). (Fig 2)

Abstract 176
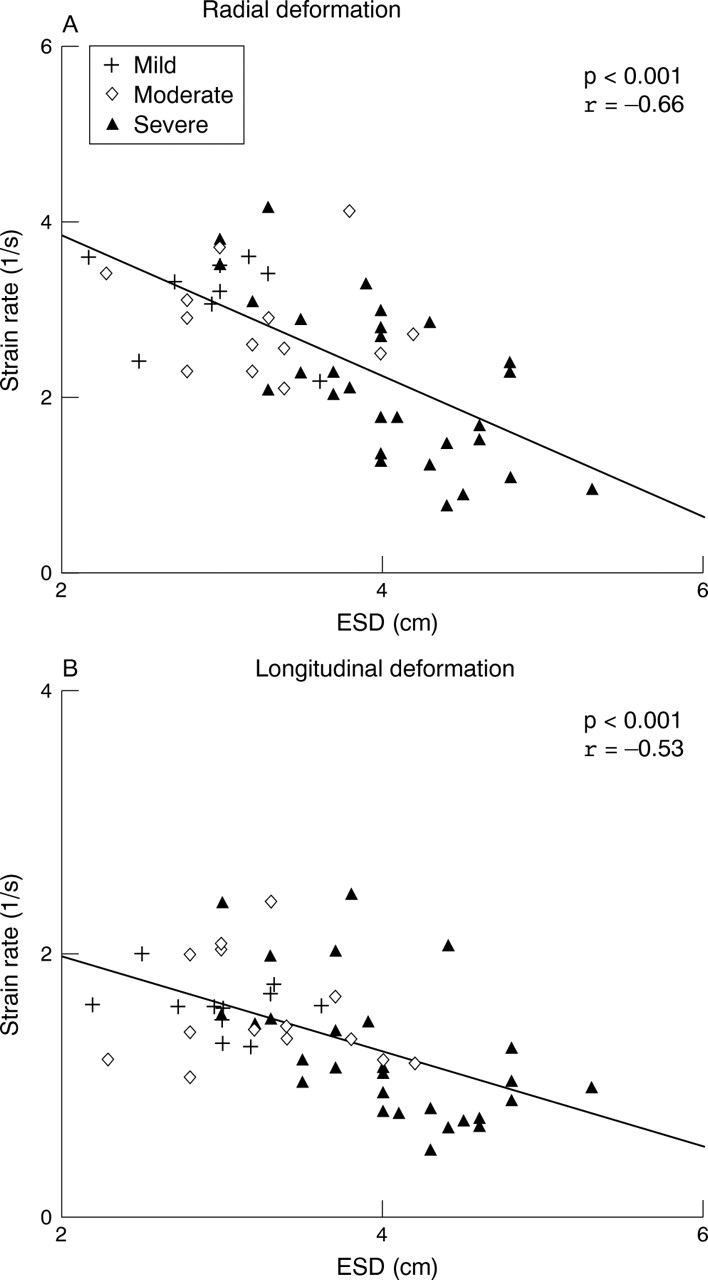
Abstract 176
Conclusions: Ischaemia is a stimulus for the homing of BMMNCs to the myocardium. This homing effect is maximal in the ischaemiac segments rather than a organ level phenomenon. Our future studies aim to identify the homing signals found in the ischaemic myocardium.
The ability of cells to home to infarcted myocardium is significantly reduced by time spent in culture. This finding suggests that optimisation of culture conditions could enhance outcome in cellular therapies.
stem cells; myocardial infarction; tissue culture
177 BONE MARROW MONONUCLEAR CELLS HOME TO THE HEART IN THE ACUTE SETTING OF MYOCARDIAL INFARCTION WITH NO ADVERSE EFFECTS ON CARDIAC FUNCTION
M. Lovell1, M. McDonald2, A. Sivarajah2, D. Harrington3, S. Ferguson3, N. Wright4, C. Thiemermann2, A. Mathur1.1Barts and The London/Clinical Pharmacology/William Harvey Research Institute, London, UK; 2Centre for Experimental Medicine/William Harvey Research Institute, London, UK; 3The London Chest Hospital/Echocardiography Department, London, UK; 4Barts and The London/Histopathology Department, London, UK
Introduction: Bone marrow mononuclear cells (BMMNCs) have been shown to improve left ventricular function when given after myocardial infarction. However it has been suggested that if given acutely the ischaemic conditions could prevent BMMNCs homing, engraftment and survival. Furthermore, it has been proposed that acute injection of BMMNCs may adversely affect left ventricular function in the short term, given their inflammatory phenotype. We sort to establish if there were detrimental effects of acute administration of BMMNCs.
Hypothesis: 1) Injected BMMNCs home to the heart and survive in the acute phase of myocardial infarction. 2) BMMNCS will not impair left ventricular function when given at the time of myocardial infarction. 3) There is no difference in homing survival and engraftment of BMMNCS whether administered in the ischaemic or reperfusion phase of myocardial infarction.
Methods: Rat BMMNCs were collected using a percoll density gradient and fluorescently labelled with a cell tracker dye. Myocardial infarction was induced in Wistar rats by ligation of the left anterior descending artery for 30 min; this was followed by 6 hours of reperfusion. Animals received the cells via the jugular vein either during ischaemia or following reperfusion. Sham operated animals injected with BMMNCs and infarcted rats not receiving cells acted as controls. Left ventricular function was assessed with 2D and M-mode echocardiography and haemodynamic measures were monitored. Blood was taken for analysis. All tissues were fixed in formalin and paraffin embedded. Homed cells were detected in myocardial tissue with fluorescent microscopy and subsequently quantified by region. 10 sections of the atria, ventricle and apex were quantifed for each animal.
Results: No adverse effects on left ventricular function, haemodynamics, biological markers of inflammation or cardiac necrosis were seen following acute administration of BMMNCS compared to controls (fig 1 and table 1). The number of labelled cells was significantly higher in the infarcted hearts compared to sham operated animals in spite of the ischaemic conditions (fig 2). There were no significant changes in the quantity of cells that had homed to the heart whether given during the ischaemic or reperfusion phase (figs 3).
Abstract 177
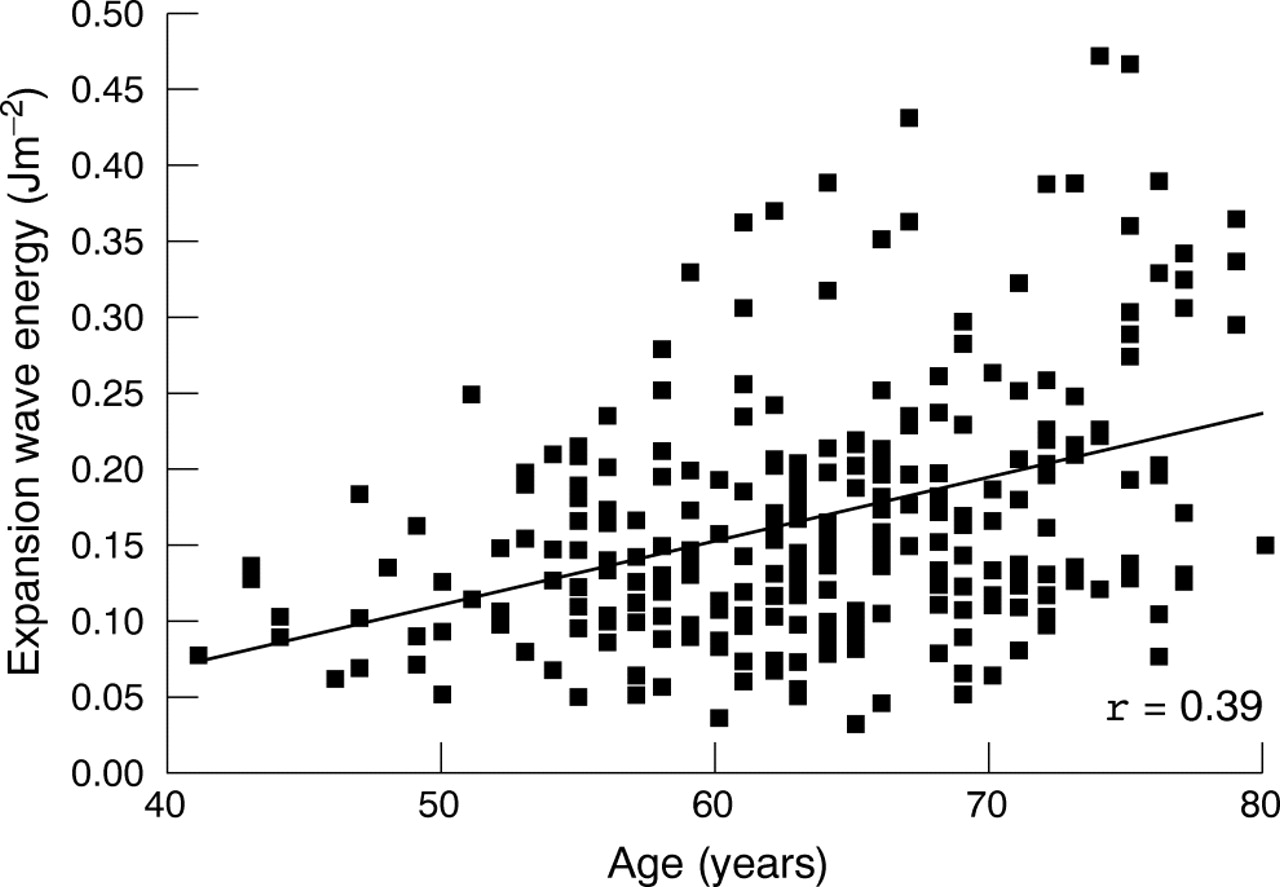
Abstract 177

Abstract 177
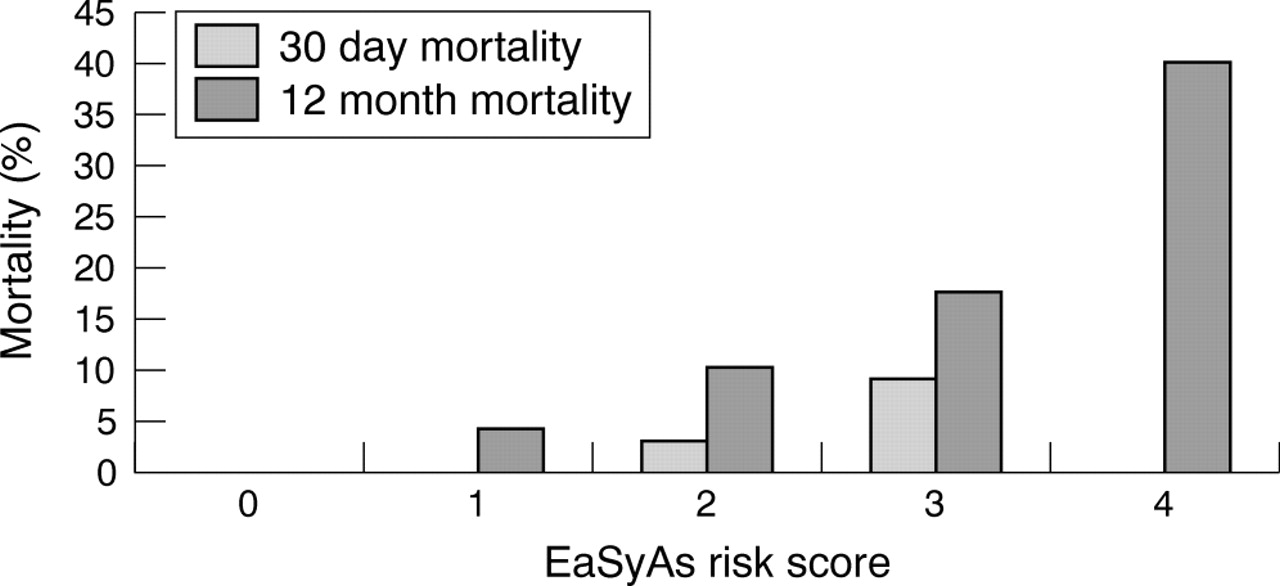
Abstract 177
Conclusions: The ischaemic environment at the time of acute myocardial infarction is not detrimental to the homing, engraftment or survival of BMMNCs in a rat model of myocardial infarction. Furthermore, injection of these cells which have an inflammatory phenotype does not have an adverse effect on left ventricular function measured acutely. The timing of injection i.e. whether the cells are injected during ischaemia or reperfusion does not influence the number of cells engrafting. These findings have implications for cellular therapy, and will be further investigated in a chronic rat model.
stem cells; myocardial infarction; cardiac regeneration
178 MAST CELL DEFICIENT MICE PRODUCE LESS CIRCULATING IL-6 AND EXHIBIT LESS CARDIAC TISSUE DAMAGE THAN THEIR LITTERMATES FOLLOWING MYOCARDIAL ISCHEMIA REPERFUSION INJURY
K. Bhattacharya1, K. Farewell2, M. Huang2, D. Kempuraj2, J. Donelan2, T. Theoharides2.1Western Infirmary, Glasgow, UK; 2Tufts University, Boston, United States
Objectives: Myocardial ischemia reperfusion injury complicates all forms of coronary artery revascularisation. Circulating interleukin-6 (IL-6) has been implicated in cell death following a variety of stimuli. To date macrophages, platelets, neutrophils and the endothelium have been shown to release IL-6 after ischemia reperfusion injury. Cardiac mast cells have been implicated in ischemia reperfusion; however, their involvement has never been quantified. In this randomised prospective study, we compared cardiac tissue susceptibility and serum IL-6 changes between the mast cell deficient (W/Wv) mice and their normal littermates (+/+).
Methods: Twenty-four male W/Wv mice and their +/+ littermates were anaesthetised with 2.5% isofluorane. The left coronary artery (LCA) was ligated for 30 min or a sham procedure was performed. After 6 hours of reperfusion, the animals were killed. The muscle viability was assessed on fresh whole-mount slices by the nitroblue tetrazolium (NBT) histochemical assay and serum IL-6 concentrations measured with ELISA.
Results: Cardiac muscle viability was significantly higher in W/Wv than the +/+ mice. Serum IL-6 levels were higher in the +/+ sham mice (163 (11) pg/ml, n = 6) than the W/Wv mice (65 (11) pg/ml, n = 6), p<0.001. The IL-6 levels increased significantly after reperfusion only in the +/+ mice (245 (14) pg/ml, n = 6, p = 0.001), while it remained similar in the W/Wv mice (71 (17) pg/ml, n = 6, p = 0.783).
Conclusions: These results show that the absence of mast cells reduces the myocardial damage associated with ischemia reperfusion injury. Furthermore, there is an attenuation is the inflammatory response, as measured by serum IL-6 levels, following this local insult. This finding entertains the prospect of developing prophylactic therapy - targeting selective inhibition of cardiac mast cell activation, in clinical situations involving medical or surgical myocardial revascularisation.
mast cell; Interleukin 6; inflammation
179 THE EFFECTS OF CHRONIC TNF-α ADMINISTRATION IN C57/BL6 MICE
M. Faircloth, J. Clark, K. Dighe, M. Marber.King’s College London and St Thomas’ Hospital, London, UK
Introduction: Tumour necrosis factor-α (TNF) is a pro-inflammatory cytokine that is elevated in conditions of depressed cardiac contractility such as myocardial infarction and congestive heart failure. A causative rather than associative role is indicated by the contractile depression and remodelling that accompanies in vitro exposure to TNF-α in which exposure of isolated hearts and cardiac myocytes to TNF causes almost immediate contractile depression in most studies. In mice, cardiac restricted TNF expression leads to chamber dilatation but it is not known whether TNF infusion results in a similar phenotype.
Methods: Osmotic infusion pumps were implanted in 16 mice, of which six received recombinant murine TNF-α and the others received vehicle only. TNF-α was administered at a rate of 1.65 or 3.31 µg/kg/min for seven days; doses similar to those administered in a similar study in rats. After 7 days, a 1.4F Millar conductance catheter was inserted into the left ventricle to obtain real time measures of left ventricular volume and pressure. We thus generated pressure-volume loops and were able to calculate parameters of contractility. Serum TNF-α levels were measured by enzyme immune assay. The hearts were arrested in diastole and set in 5% formaldehyde, before being sliced to measure chamber and muscle volumes.
Results: The TNF-α level was higher in the treated group (556.7 (2.40) pg/ml) than in the control group (340.9 (53.47) pg/ml) (p<0.05). There were similar rates of weight gain in the control group and a non-treated group – of approximately 1 g in one week; significantly higher than in the TNF group, in which there was a mean weight loss of 1.5 g (p<0.05). A trend towards left ventricular cavity dilatation was seen when measured by planimetry (cavity volume in the TNF-α group 5.58 (0.73) mm3v control group 4.08 (0.65) mm3, p = 0.14). In addition, the stroke volume was significantly higher in the TNF treated group (table 1). The heart rates were similar in the two groups and thus the cardiac output was higher in the TNF group. The minimum rate of change of pressure (dP/dtmin) was significantly lower in the TNF group whilst a trend to a lower dP/dtmax was also seen in this group. Arterial elastance was higher in the TNF group, though stroke work was higher.
Conclusions: This first in vivo mouse study of the effects of prolonged TNF infusion suggests combined left ventricular dysfunction and systemic vasodilatation. Dysfunction is indicated by abnormal relaxation whilst vasodilatation by lower arterial elastance and systemic pressure despite higher stroke volumes. This implies that there are compensatory mechanisms ameliorating the direct cardiac effects of TNF. These findings may help to explain the lack of benefit of anti-TNF therapy in the treatment of heart failure.
Abstract 179
TNF; heart failure; conductance catheter
180 NEW INSIGHTS INTO THE CREATINE KINASE-PHOSPHOCREATINE ENERGY BUFFER AND TRANSPORT SYSTEM USING MOUSE MODELS OF ALTERED CREATINE CONTENT
C. Lygate, J. Wallis, M. ten Hove, S. Neubauer.University of Oxford, Oxford, UK
Background: The creatine kinase (CK)/phosphocreatine (PCr) system acts as a transport and buffering system for high energy phosphate groups, and is down regulated in heart failure. To determine whether this contributes to dysfunction, we created two mouse models.
Method: In the first, we knocked out the enzyme GAMT, which catalyses the final step in creatine biosynthesis, resulting in a creatine deficient mouse. We hypothesised that this would result in cardiac dysfunction due to a primary abnormality of reduced creatine and PCr.
Results: As expected, GAMT KO mice had normal CK activity, undetectable levels of PCr and creatine, and an accumulation of the precursor (phospho-) guanidinoacetate (P-GA). GAMT KO mice did not develop cardiac hypertrophy, and indices of resting in vivo systolic and diastolic cardiac function were similar to wildtype mice (eg dP/dtmax, dP/dtmin, PRSW, LVEDP, and EF). However, during inotropic stimulation, contractile reserve was severely impaired in GAMT KO hearts. 31P-MR spectroscopy in isolated hearts showed that GAMT KO utilised P-GA during inotropic stimulation, to a similar extent that WT hearts utilised PCr. When subjected to acute global ischemia (10 min) and reperfusion (20 min), GAMT hearts showed markedly impaired recovery of systolic and diastolic function. We conclude that the ability of GAMT KO mice to utilise P-GA in the creatine kinase reaction, enables normal cardiac function at low workload, however, under stress conditions a fully functional CK/PCr system is required. The second model is of elevated creatine in the heart, to test the hypothesis that increasing myocardial high energy phosphate stores is a potential strategy for treatment of heart failure. We created a transgenic mouse line overexpressing the myocardial creatine transporter (CrT-OE). Compared with wildtype controls, total creatine was increased in CrT-OE hearts (66 (SD 6) nmol/mg protein in wildtype; 133 (52) in CrT-OE); while phosphocreatine levels were increased to a lesser extent. Surprisingly, CrT-OE mice developed significant LV hypertrophy, dilatation and substantial LV dysfunction, that was closely correlated with myocardial creatine content eg EF (r = −0.74, p = 0.0002). Furthermore, the total creatine content correlated inversely with the phosphorylated fraction of creatine (PCr/total creatine; r = −0.61, p = 0.001), indicating that the heart is incapable of keeping the augmented creatine pool adequately phosphorylated. The result is an increase in free ADP concentrations, and a reduction in the free energy available from ATP hydrolysis, which could contribute to the heart failure phenotype.
Conclusion: In conclusion, myocardial energetics is tightly controlled in the normal mouse heart, and any disturbance of the system has the potential to lead to myocardial dysfunction. While this implies caution in the application of therapeutic interventions to this system, it also strongly supports the hypothesis that energetic imbalance is a causal factor in the development of heart failure.
creatine; metabolism; heart failure
181 SLEEP APNOEA IS ASSOCIATED WITH IMPAIRED CARDIAC HIGH-ENERGY PHOSPHATE METABOLISM AND ABNORMAL DIASTOLIC FUNCTION
M. Scheuermann-Freestone1, S. West2, G. Watson3, D. Tyler3, J. Francis1, J. Stradling2, S. Neubauer1, K. Clarke3.1OCMR, John Radcliffe Hospital, Oxford, UK; 2Churchill Hospital, Oxford, UK; 3Department of Physiology, Oxford, UK
Introduction: Obstructive sleep apnoea (OSA) is associated with increased cardiovascular morbidity and mortality. We have found that abnormal cardiac function and energy metabolism correlate with free fatty acid levels in patients with heart failure, but it is unknown whether cardiac energetics or function are altered in patients with OSA.
Methods: We measured fasting circulating metabolites and cardiac high-energy phosphate metabolism (phosphocreatine PCr/ATP ratios) and function using magnetic resonance spectroscopy (MRS) and imaging, respectively, in 19 patients with OSA, and compared them with 15 age-, sex- and body mass-index matched control subjects.
Results: Fasting plasma concentrations of free fatty acids (FFA) were significantly increased from 0.37 (0.04) mmol/l in healthy control subjects to 0.51 (0.06) mmol/l in patients with OSA (p<0.05), without any changes in fasting plasma glucose or insulin concentrations. Cardiac PCr/ATP was significantly reduced, from 2.11 (0.10) to 1.77 (0.07), in patients with OSA compared with healthy control subjects (p = 0.01), and correlated negatively with circulating concentrations of FFA (r = −0.38, p<0.05). Left ventricular systolic function was preserved, but diastolic function was impaired in patients with OSA compared with control subjects.
Conclusion: Obstructive sleep apnoea is associated with increased plasma FFA concentrations, reduced cardiac high-energy phosphate metabolism and diastolic dysfunction. These results suggest that the increased morbidity and mortality in OSA may be due to alterations in myocardial energetics caused by metabolic abnormalities.
cardiac energy metabolism; free fatty acids; obstructive sleep apnoea

Abstract 181
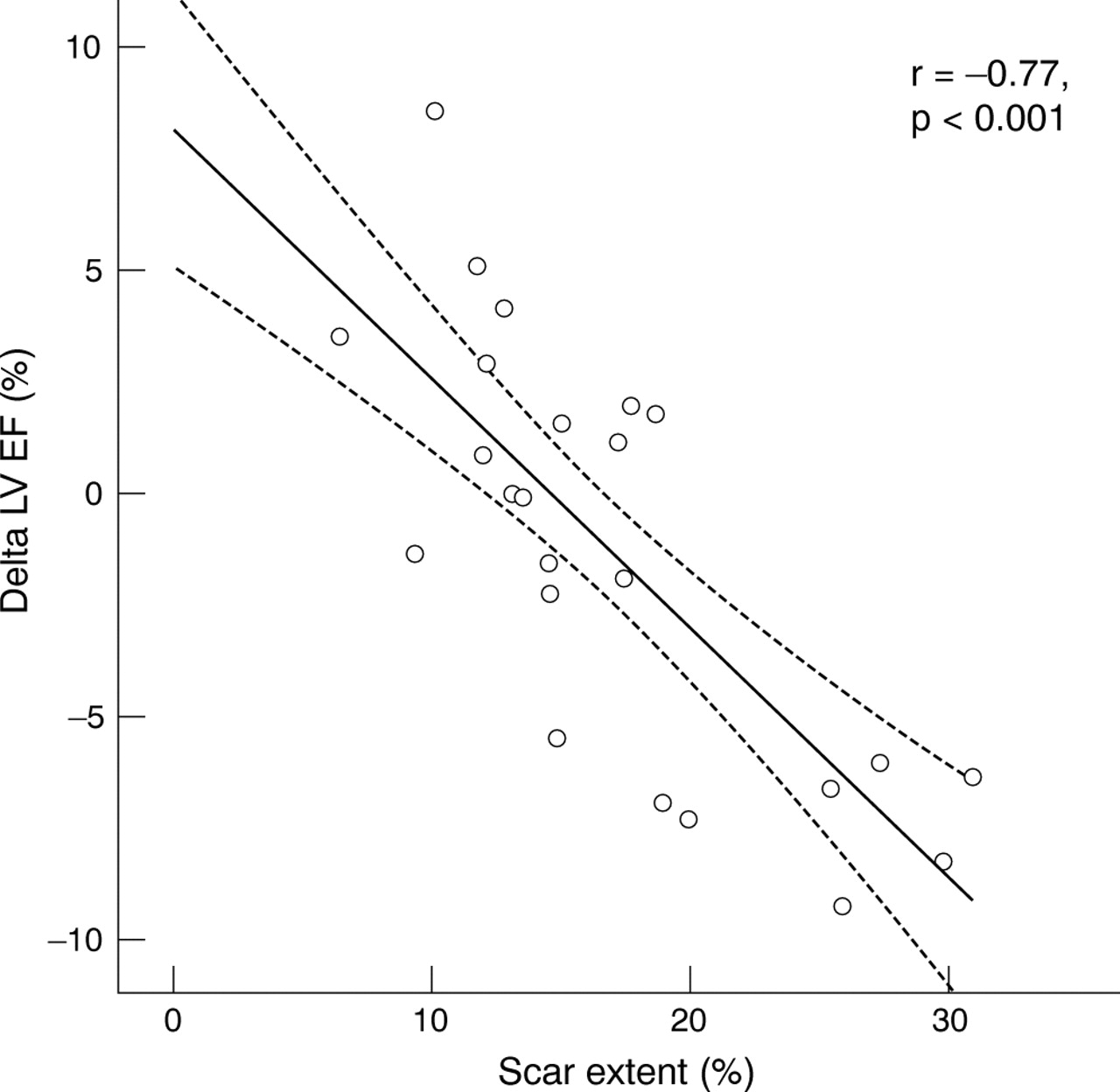
Abstract 181
182 DEVELOPMENT OF A RISK MODEL TO PREDICT EARLY DEATHS DUE TO PRIMARY GRAFT DYSFUNCTION IN ADULT HEART TRANSPLANTATION
J. Ganesh, C. Rogers, J. Meulen, N. Banner, R. Bonser.1On Behalf of the Steering Group, UK Cardiothoracic Transplant Audit, The Royal College of Surgeons, London, UK
Introduction: Primary graft dysfunction (PGD) following adult heart transplantation (HTx) may directly or indirectly lead to early death via cardiogenic shock or multi-organ failure. We have previously reported that PGD causes 65.5% of early deaths after HTx. We sought to identify risk factors and develop a risk model to predict death from PGD (dPGD).
Methods: Univariate logistic regression analysis was performed for dPGD in adults undergoing Htx in the UK between April 1995 and December 2002. Factors with univariate significance (p¡Ü0.05) and other clinically relevant variables were entered into a multivariate analysis. A backward stepwise selection process was used with a significance level of 20% and applied to 200 bootstrap samples. Variables selected in >45% of samples were then internally cross-validated to derive the final risk model.
Results: Of 229 of 1388 (16.5%) early deaths, 150 of 229 (65%) were because of PGD. Significant univariate recipient risk factors included a diagnosis other than dilated cardiomyopathy, previous open heart surgery, higher creatinine, preoperative ventilation, peripheral vascular disease (PVD), transpulmonary gradient (TPG) >12 mmHg and anti-arrhythmic treatment. Significant donor factors were older age, combination of female donor and male recipient with donor: recipient height or weight ratio<1 (FDMRHWM), non-traumatic cause of death, female donor on inotropic support (FINO) and ischaemia time. These risk factors along with recipient age, diabetes, previous resuscitation episode, PA systolic >45 mmHg, preoperative inotropes, mechanical support and donor smoking status, donor hypotensive episode (systolic blood pressure <60 mmHg for ¡Ý20min), donor cardiac arrest episode and donor noradrenaline support were considered for inclusion in the multivariate model. Following validation, the final model included: RECIPIENT: anti-arrhythmia treatment (OR 1.48 95%CI 1.01 to 2.07), TPG >12 mmHg (OR1.90 95%CI 1.17 to 3.07), preoperative ventilation (OR 2.81 95%CI 1.25 to 6.33), diagnosis other than dilated cardiomyopathy (OR 1.63 95%CI 1.11 to 2.40), peripheral vascular disease (OR 3.09 95%CI 1.10 to 8.65), higher creatinine (OR 1.29 95%CI 1.01 to 1.66 if 120–150¦Ìmol.L-1; OR 1.292 = 1.66 if >150¦Ìmol.L-1), DONOR: increasing ischaemia time (OR 1.33 95%CI 1.09 to 1.63 if 120–180 min; OR 1.332 = 1.77 if 181–240 min; OR 1.333 = 2.35 if >240 min), FDMRHWM (OR 2.03 95%CI 1.26 to 3.28), FINO (OR 1.66 95%CI 0.94 to 2.93), D hypotension (OR 1.45 95%CI 0.97 to 2.16) and non-traumatic cause of death (OR 1.45 95%CI 0.95 to 2.20). The area under the ROC curve was 0.71 (fig 1) and Hosmer-Lemeshow goodness of fit was p = 0.8.

Abstract 182
Conclusion: Risk factors for dPGD have allowed development of a risk model which may assist donor-selection and donor-recipient matching. There is now an opportunity to validate this model in a separate cohort.
primary graft dysfunction; heart transplantation; risk model
183 SURVIVAL BEFORE AND AFTER HEART TRANSPLANTATION: ANALYSIS OF A COHORT OF 610 PATIENTS AT TWO UK CENTRES
N. Banner1, C. Rogers2, J. Ganesh3, K. Ranganathan1, S. Jayakumar4, R. Bonser4.1Royal Brompton and Harefield NHS Trust, Harefield, UK; 2Bristol Heart Institute, University of Bristol, Bristol, UK; 3Royal College of Surgeons, London, UK; 4Queen Elizabeth Hospital, Birmingham, UK
Evidence-based criteria for listing patients for cardiac transplantation (HTx) have been difficult to establish because ethical concerns and limited organ availability have precluded the use of randomised trials. Consequently, in ambulatory heart failure, listing based on risk-stratification and scoring systems such as the Heart Failure Survival Score (HFSS) have been proposed. However, one study conducted in Germany (COCPIT) cast doubt on the survival benefit from HTx even after risk stratification. We examined survival before and after HTx in non-ambulatory heart failure and ambulatory heart failure (with the latter divided into low, moderate and high risk HFSS groups) 610 adult patients listed for a first HTx between April 1996 and December 2003 at two UK centres were followed to September 2004. The HFSS was not used to prospectively select or prioritize ambulatory patients. Patients were grouped at listing as non-ambulatory (123, 20%), high risk (164, 27%), moderate risk (181, 30%) low risk (142, 23%). The mean age was 47 (SD 11) years, with 83% male, the commonest diagnoses were ischaemic heart disease (44%) and dilated cardiomyopathy (43%). In ambulatory patients, peak VO2 was 12 (4) ml/Kg/min. Most non-ambulatory patients were on inotropic support (79%) and/or an IABP (33%). Outcome after listing comprised one of: HTx, death or removal from list; the probability of each was calculated using competing risks. Survival after HTx was estimated using the Kaplan-Meier method. A time-dependent non-proportional hazards model was used to compare the relative-risk of death (RRD) for HTx patients with those on the waiting list. Almost 80% of non-ambulatory patients had a HTx within a year of listing, compared with approx. 2 of 3 of ambulatory patients; the median waiting time in the non-ambulatory and ambulatory groups was: 20 v 116 days. The probability of dying within 12 months while awaiting transplantation was greatest for the non-ambulatory patients (16%) and lowest for the low risk HFSS patients (6%). Survival after transplantation did not differ significantly between the four groups. The RRD fell below the risk on the waiting list in all groups:, the benefit was seen after 52 days (95%CI 0–144) in the high risk HFSS group, compared with 93 days (95%CI 35–151) for the non-ambulatory group, 127 days (95%CI 76–177) for moderate-risk and 116 days (95%CI 75–157) for low-risk. Non-ambulatory status and the HFSS in ambulatory patients predicted mortality while awaiting transplant but did not influence mortality after transplantation. Transplantation was followed by a reduction in the RRD in all groups.
heart failure; transplantation; survival
184 SIROLIMUS IN CARDIAC TRANSPLANTATION: ROLE AS A PRIMARY IMMUNOSUPPRESSANT IN CALCINEURIN-INHIBITOR INDUCED NEPHROTOXICITY
S. Kushwaha, Z. Khalpey, R. Frantz, R. Rodeheffer, A. Clavell, B. Edwards.Mayo Clinic, Rochester, Minnesota, United States
Introduction: Calcineurin inhibitor (CNI) immunosuppressants are a major cause of renal dysfunction in cardiac transplant recipients leading to increased morbidity and mortality. The feasability of complete CNI withdrawal and replacement with mTOR inhibitors, such as Sirolimus, remains ill-defined. This study evaluates the efficacy and safety of CNI withdrawal and substitution with Sirolimus as the primary immunosuppressant, as well as assesses the effect on renal function in cardiac transplant recipients with CNI induced renal impairment.
Methods: We evaluated the safety of a stepwise CNI withdrawal and substitution with Sirolimus in 58 cardiac transplant recipients (group A) of whom 39 had CNI induced renal impairment (Glomerular Filtration Rate (GFR) <50 ml/min with no other cause of renal failure). A further 24 patients (group B), were retrospective controls maintained on CNI, who also met criteria for CNI induced renal impairment. GFR baselines were measured using iothalamate clearances before starting Sirolimus and within 4 to 12 months following complete CNI withdrawal. Secondary immunosuppressants (azathioprine or mycophenolate mofetil, prednisone) were left unchanged.
Results: GFR significantly improved (baseline 42.7 (16.7) to 54.6 (23.7) ml/min, p<0.001, following CNI withdrawal) without exacerbating rejection or compromising cardiac function. Furthermore we noted a fall in serum creatinine (baseline 1.97 (0.49) to 1.74 (0.52) mg/dl, p<0.05). In contrast, in control group B, the GFR declined from 40.04 (1.86) to 34.63 (1.6) ml/min over the course of one year (p<0.01). ISHLT grades of rejection in both groups were unchanged during the trial.
Conclusions: Substitution of CNIs with Sirolimus in cardiac transplant recipients is safe, effective and leads to an improvement in renal function, without compromise in cardiac function and rejection.
sirolimus; renal dysfunction; cardiac transplantation
185 PHARMACOLOGICAL TREATMENT OF VEIN GRAFT DISEASE: EARLY INHIBITION OF PATHOLOGICAL CHANGES FOLLOWING RAPAMYCIN PRE-TREATMENT ARE NO LONGER EVIDENT IN LONG-TERM PORCINE SAPHENOUS VEIN BYPASS GRAFTS IN VIVO
S. Rizvi, G. Murphy, J. Johnson, S. George, G. Angelini, A. Newby.Bristol Heart Institute, Bristol, UK
Objective: The aim of this study was to evaluate the effects of short-term exposure to rapamycin on vein graft disease in porcine saphenous vein bypass grafts in vivo.
Methods: Porcine saphenous vein to carotid interposition grafts immersed in rapamycin (0.01 mg/ml, 0.1 mg/ml, 0.5 mg/ml) for 30 min prior to implantation were compared with contralateral, paired, controls immersed in vehicle only at 7, 28 and 90 days. Data were expressed as median, (interquartile range). Paired values were compared using the Wilcoxon signed ranks test.
Results: Rapamycin 0.01 mg/ml had no effect on vein graft disease. Rapamycin 0.5 mg/ml induced thrombosis in 42% of grafts at 28 days. This was attributed to possible adventitial precipitation of the relatively insoluble rapamycin at this high concentration. Rapamycin 0.1 mg/ml significantly inhibited vessel remodelling at 7 days; plaque ratio (wall area/total vessel area) 0.18, (0.12–0.23) rapa v 0.34, (0.20–0.55) control, p = 0.028. This was associated with a significant reduction in the Proliferating Cell Nuclear Antigen (PCNA) Index, (ratio of PCNA positive to total number of vessel wall cells) 0.31 (0.30–0.33) rapa v 0.61 (0.50–0.65) control, p = 0.028. The attenuation of wall thickening was still evident at 28 days; neointimal area, (2392 µm2, (0–15056 µm2) rapa v 16095 µm2, (7296–24720 µm2) control, p = 0.028); plaque ratio 0.20, (0.14–0.25) rapa v 0.34, (0.22–0.37) control, p = 0.028. Luminal area was increased in the rapamycin 0.1 mg/ml group at 28 days, (223300 µm2 (189182–277939 µm2) rapa v 184723 µm2 (154721–209975 µm2) control, p = 0.046) with similar total vessel areas in both groups. These effects were not sustained in the long-term however with only a marginal difference evident in long-term grafts (90 days); plaque ratio 0.24, (0.22–0.36) rapa v 0.33, (0.25–0.40) control, p = 0.091.
Conclusions: This data suggests that local rapamycin treatment effectively attenuates early pathological changes in vein bypass grafts in a large animal model. A catch-up phenomenon occurs however with no attenuation of vein graft disease evident in the long term.
rapamycin; saphenous vein graft disease; neointimal hyperplasia
186 MECHANICAL VALVES IN SEPTUAGENARIANS: A HAZARDOUS CHOICE?
R. Ascione, C. Rogers, L. Culliford, G. Angelini.Bristol Heart Institute, Bristol, UK
Objective: To assess the safety and efficacy of a third generation bileaflet mechanical valve in elderly patients.
Methods: Prospectively collected data for a consecutive series of 567 patients undergoing Sorin Bileaflet mechanical valve replacement between April 1996 and November 2001 were extracted from a database. Patients were grouped by age: <70 years, and ⩾70 years, and their in-hospital and mid-term valve-related outcome analysed.
Results: Six hundred and sixteen Sorin Bileaflet valves were implanted in 567 patients (437 patients <70 years, median age 61 years, and 130 patients ⩾70 years, median age 72). Elderly patients were more likely to present with coronary disease, and to undergo concomitant coronary surgery (both p<0.01). In-hospital mortality was 2.8% and 2.3% (p = 0.79) and neurological complications 1.4% v 3.8% (p = 0.026) in the younger and older age groups respectively. The older group tended to stay longer in ITU and hospital post-operatively, (p = 0.051 and 0.0037 respectively), but no other significant differences in in-hospital outcomes were observed between groups. Two-year valve-related mortality was 1.6% (95% CI 0.6% to 3.3%) and 4.1% (95% CI 1.5% to 8.7%), cumulative 3-year incidence of thromboembolic and major haemorrhagic event was 10.2% (95% CI 7.3% to 14.2%) and 7.1% (95% CI 3.4% to14.4%) in the younger and older age group, respectively.
Conclusions: The use of Sorin Bicarbon bileaflet in over 70-year-old patients is safe and effective with no increased risk of mid-term valve-related mortality, bleeding or thromboembolism when compared with a younger cohort.
prosthatic valve; elderly; valvular surgery
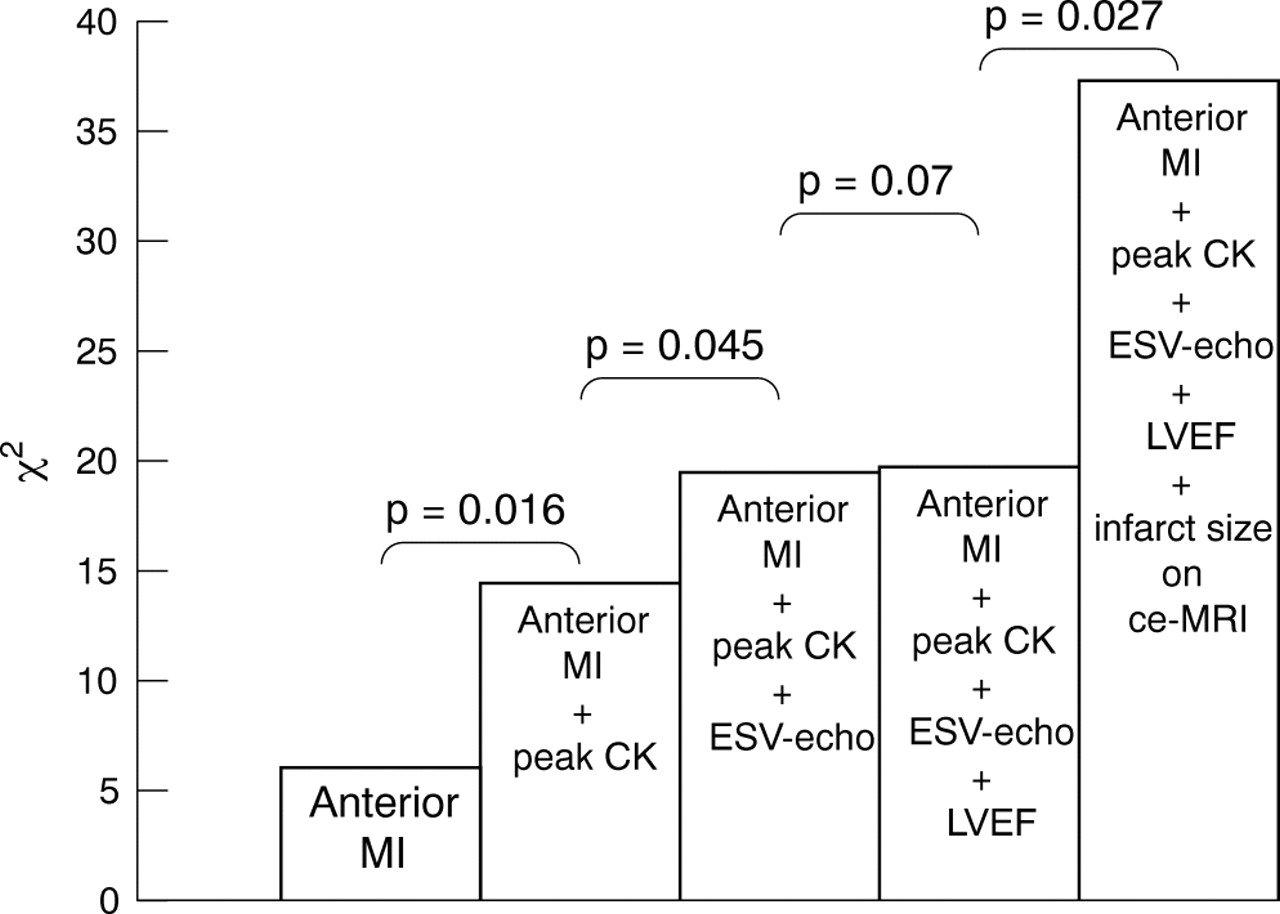
Abstract 186
187 STRAIN RATE IMAGING DETECTS EARLY CHANGES IN LEFT VENTRICULAR DEFORMATION IN PATIENTS WITH ASYMPTOMATIC MITRAL REGURGITATION
A. Marciniak, G. Sutherland, M. Marciniak, B. Bijnens, T. Karu, A. Baltabaeva, E. Merli, E. Wilton, M. Jahangiri.St. George’s Hospital, London, UK
Background: Valvular heart disease with poor ventricular function is recognized as an important cause of morbidity and mortality. To date, there is no specific and widely used diagnostic method to detect subclinical changes in systolic function before irreversible left ventricular dysfunction occurs in mitral regurgitation. Strain rate imaging ultrasound is a newly developed technique which is very sensitive in detecting regional systolic abnormalities and would allow to diagnose subclinical changes of systolic left ventricular function.
Aims: To assess the changes in regional left ventricular function by strain rate imaging in patients with mitral regurgitation before development of clinical features and detection by conventional echocardiography.
Methods: 77 individuals were studied: 54 consecutive asymptomatic patients with mitral regurgitation isolated (age 58 (12)) divided into three groups: mild, moderate, severe mitral regurgitation according to regurgitant volume and 23 age-matched healthy subjects. All patients underwent a standard echocardiographic examination extended with a tissue Doppler imaging study. For left ventricular radial deformation, the posterior wall (LVPW) was examined. To assess left ventricular longitudinal deformation, strain rate data were acquired from the septum and left ventricular lateral wall. Patients were excluded if they had ischemic heart disease.
Results: Radial peak systolic strain rate in the LVPW was significantly decreased in patients with severe mitral regurgitation compared with healthy subjects (2.2 (0.7)s−1v 3.0 (0.5)s−1, p<0.001), In addition strain rate was inversely correlated with left ventricular end systolic diameter (ESD), (fig 1) and end diastolic diameter (EDD), (p = 0.001, r = −0.42). Longitudinal strain rate was significantly reduced for mid segment of septum in the severe mitral regurgitation group compared with control subjects (1.1 (0.5)s−1v 1.5 (0.3)s−1) as well as for left ventricular lateral wall compared to controls (1.1 (0.4)s−1v 1.6 (0.2)s−1). Longitudinal strain rate was inversely correlated with ESD (fig 1) and EDD (p = 0.006, r = −0.36). There was no significant difference in radial or longitudinal peak systolic strain rate in the groups with mild and moderate mitral regurgitation compared with the healthy subjects.

Abstract 187
Conclusions: Strain rate imaging is a sensitive tool in detecting subclinical changes in left ventricular function in asymptomatic patients with severe mitral regurgitation. It could be an useful tool in predicting left ventricular function before the ventricle starts to fail irreversibly.
mitral regurgitation; echocardiography; strain rate imaging
188 REAL TIME THREE DIMENSIONAL TRANSTHORACIC ECHOCARDIOGRAPHY FOR PLANNING MITRAL RECONSTRUCTIVE SURGERY: A COMPARISON WITH TWO DIMENSIONAL TRANSOESOPHAGEAL ECHOCARDIOGRAPHY
R. Sharma1, J. Mann1, L. Drummond2, S. Livesey1, I. Simpson1.1Southampton General Hospital, Southampton, UK; 2Southampton General Hopsital, Southampton, UK
Background: Transoesphageal echocardiography (TOE) is considered the gold standard imaging technique for mitral valve assessment prior to surgery. We compared the accuracy of 2 – Dimensional TOE with Real Time 3 – Dimensional transthoracic echocardiography (RT-3DE) for the pre-operative functional assessment of patients with mitral valve prolapse.
Methods: In 39 patients with severe mitral regurgitation due to type 2 valve dysfunction, TOE and RT-3DE were performed 24 hours prior to surgery and analysed by two separate observers. TOE and RT-3DE images were acquired digitally on the Phillips IE33 ultrasound machine and stored for off – line analysis. The RT-3DE datasets were analysed with Phillips Qlab software (version 4.0). Leaflet segments and commissures were displayed in short axis en-face and long axis views. Echocardiographic results were validated intraoperatively.
Results: Five patients did not have image quality suitable for analysis with RT-3DE and were excluded from analysis. This was due to atrial fibrillation in 4 and motion artefact in one patient. This left a sample size of 34 patients (mean age 52 (11) years, 19 male). Twenty–five patients had mitral valve repair and 9 mitral valve replacement. In total, 47 out of 304 analysed mitral valve segments were diseased. Prolapse of a single mitral valve segment was present in 22 patients. 12 patients had complex disease involving 2 or more segments. Sensitivity, specificity and accuracy for TOE in identification of diseased segments were 94%, 100% and 96% respectively. The same values for RT-3DE were 91%, 100%, 94%. The differences were not statistically significant. Accuracies were not significantly different according to segment location. Ruptured chordae was confirmed at surgery in 20 patients. Sensitivity for the diagnosis of ruptured chordae was 90% for TOE and 44% for RT-3DE (p = 0.01). Specificity was comparable by both techniques (88% TOE v 82% RT-3DE). Interobserver agreement was 92% for TOE and 86% for RT-3DE (non significant).
Conclusions: RT-3DE is feasible with comparative accuracy to TOE for precise anatomical localisation of prolapsing mitral valve segments. However, the technique is limited by poor image quality in a small proportion of patients. TOE remains superior for diagnosis and localisation of chordal rupture.
mitral valve prolapse; real time 3 Dimensional echocardiography; transoesophageal echocardiography
189 THE -1171 5A/6A POLYMORPHISM OF MATRIX METALLOPROTEINASE 3 GENE PREDICTS REGURGITATION AND LEFT VENTRICULAR REMODELLING IN MITRAL VALVE PROLAPSE PATIENTS
D. Oceandy1, R. Yusoff2, L. Neyses1, S. Ray2.1Division of Cardiology, University of Manchester, Manchester, UK; 2Department of Cardiology, Wythenshawe Hospital, Manchester, UK
Mitral valve prolapse (MVP) is common and highly variable in its natural course, but the determinants of severity are unclear. We hypothesised that polymorphic variations in genes whose products determine contractility and remodelling of the heart may be predictors of the haemodynamic severity of MVP. We therefore investigated 12 polymorphisms in 10 genes including the α and β adrenergic receptors, matrix metalloproteinases (MMP), elastin, tumor necrosis factor, aldosterone synthase and angiotensin converting enzyme. A total of 70 MVP patients with severe mitral regurgitation (Regurgitant Fraction >40%), diagnosed by echocardiography, have been studied.
Of 12 polymorphisms studied, we found that the -1171 5A/6A polymorphism of MMP3 gene have associations with the severity of regurgitation and left ventricular remodelling in MVP patients. Patients homozygous for -1171 5A allele in the MMP3 gene (n = 16) had a larger end-diastolic dimension (p<0.05), left ventricular mass (p<0.05), left atrial volume (p<0.05), mitral annulus (p<0.01), and higher regurgitation volume (p<0.05) than patients with 6A/6A (n = 18) or 5A/6A (n = 34) alleles.
We also found that in a cellular assay system the 6A polymorphic allele was associated with higher activity of the MMP3 gene promoter. Thus, the presence of 6A allele predicts higher expression of the MMP3 gene and hence may reduce the development of left ventricular remodelling.
In conclusion, our data identifies the -1171 5A/6A MMP3 polymorphism as a possible novel marker of an adverse disease course in MVP and most importantly, these are the first data to identify genetic determinant for the severity of MVP.
mitral valve prolapse; polymorphism; matrix metalloproteinase
190 SURVIVAL AFTER AORTIC VALVE REPLACEMENT IN PATIENTS WITH SEVERE AORTIC STENOSIS AND IMPAIRED LEFT VENTRICULAR FUNCTION
W. Ding, A. Duncan, R. Chung, J. Pepper, M. Henein.The Royal Brompton Hospital, London, UK
Background: The long-term outcome of patients with severe aortic stenosis and impaired left ventricular systolic function after aortic valve replacement (AVR) remains unclear. We aimed to determine the surgical risk, survival, and factors influencing mortality in patients with end-stage aortic stenosis.
Methods: Between 1998 and 2003, 86 patients with impaired left ventricular function (fractional shortening <25%) and severe aortic stenosis (transvalvular mean gradient <30 mmHg) underwent AVR. An echo-Doppler study performed 1 month prior to AVR recorded FS, peak aortic valve pressure gradient (AVPG), and E:A ratio. Peak systolic pulmonary artery pressure (PSPAP) was estimated from tricuspid regurgitant velocity and right-atrial pressure.
Results: The operative (30-day) mortality was 10%. FS (15 (1)% v 20 (1)%, p<0.001) and AVPG (47 (4) mmHg vs. 64 (3) mmHg, p = 0.024) were significantly lower, E:A ratio (4.8 (0.4) v 2.5 (0.2), p<0.001) and PSPAP (52 (3) mmHg v 24 (2) mmHg, p = 0.0003) were significantly higher, and the prevalence of NYHA class III/IV (100% v 35%, p = 0.05) or emergency surgery (78% v 35%, p = 0.026) were greater in 9 of 86 non-survivors than 77 of 86 survivors. In multivariate analysis, the only independent predictors of operative mortality were FS (odds ratio (CI) 0.77 (0.62–0.94), p = 0.011) and PSPAP (1.05 (1.00–1.09, p = 0.032).
Median time to follow up (IQR) was 46 (27) months. Overall survival at 4 years was 71 (83%). There were no differences in age, gender, incidence of hypertension/diabetes/atrial fibrillation, QRS duration, haemoglobin, valve size, or LV mass index in non-survivors compared with survivors. FS and peak AVPG were lower (15 (1)% v 21 (2)%, 47 (3) mmHg v 66 (3) mmHg), and E:A ratio and PSPAP were greater (4.8 (0.3) v 2.3 (0.3), 53 (4) mmHg v 22 (2) mmHg, all p<0.001) in non-survivors. The incidence of NYHA class III-IV (94% v 63%, p = 0.017) and coronary artery disease (CAD: 81% v 53%, p = 0.049) were greater in patients who died, as was bypass time (138 (11) min v 115 (5) min, p = 0.036). Independent predictors of mortality were valve type (stentless v stented) (odds ratio 0.26 (CI: 0.12–0.56, p = 0.0005) and NYHA class (OR 0.43 (0.25–0.73, p = 0.002).
Conclusion: The surgical risk of AVR in patients with severe aortic stenosis and impaired left ventricular function is acceptable. Predictors of operative mortality are those that reflect underlying ventricular dysfunction. Moreover, dysfunctional ventricles are vulnerable to outflow tract resistance, and thus long-term survival is enhanced with the insertion of stentless aortic valve replacements.
severe aortic stenosis; left ventricular impairment; aortic valve replacement
191 BASELINE PREDICTORS OF OUTCOME FOR PATIENTS WITH SYNCOPE: THE EASYAS SYNCOPE RISK SCORE
R. Veasey1, D. Farwell2, J. Silberbauer1, A. Sulke1.1Eastbourne District General Hospital, Eastbourne, UK; 2Leeds General Infirmary, Leeds, UK
Aims: To develop a simple risk classification for patients presenting with syncope.
Methods: A group of consecutive patients presenting with unexplained syncope over a twelve month period to the Eastbourne District General Hospital were followed up for one year to form a derivation cohort. Data from the baseline clinical history, physical examination and electrocardiogram were used to identify independent predictors of mortality at 30 days and 12 months. The syncope risk score was then prospectively applied to a second cohort of patients, presenting from July 2003 to June 2004, to validate the risk score.
Results: A group of 376 patients (195 females, median age 76) were followed for 1 year in the derivation cohort. 10 deaths occurred after 30 days and 37 deaths after one year. Multivariate analysis allowed recognition of the following predictors of 30 day mortality: (1) male gender, (2) age 75 or older and (3) first presentation with syncope. Multivariate analysis allowed recognition of the following predictors of 12 month mortality: (1) male gender, (2) age 75 or older, (3) first presentation with syncope and (4) a diagnosis of neurological syncope. Linear ascending score effectively predicted increased mortality risk. The 30-day mortality in the derivation cohort was 0.0% for a score of 0; 0.0% for 1 point; 4.1% for 2 points; 12.2% for 3 points (p<0.0001 for trend), (see figure 1). The 12 month mortality in the derivation cohort was 1.0% for a score of 0; 6.8% for 1 point; 17.1% for 2 points; 25% for 3 points; 36.4% for 4 points (p<0.0001 for trend), (fig 1).

Abstract 191
When prospectively applied to a validation cohort of all syncope admissions from July 2003–June 2004 similar patterns of increasing mortality with increasing score where seen (226 consecutive patients, 115 females, median age 78) (fig 2).

Abstract 191
Conclusion: A simple risk score has been derived and validated which may be applied upon admission to patients with unexplained syncope to predict mortality. The EaSyAs risk score may allow high risk patients to be easily identified and targeted for a more intense management strategy.
Syncope; risk stratification; mortality
192 “ABC FOR LIFE” – A REGIONAL PROGRAMME TO TRAIN SCHOOL CHILDREN IN CARDIOPULMONARY RESUSCITATION
M. Connolly1, P. Toner1, D. Connolly2, D. McCluskey2.1Queen’s University, Belfast, UK; 2Royal Victoria Hospital, Belfast, UK
Introduction: Widespread cardiopulmonary resuscitation (CPR) skills would be beneficial to a population. The European Resuscitation Council has recommended CPR training for school children. We describe the design of the “ABC for life” programme and the change and retention of children’s CPR knowledge following training within the programme.
Methods: Medical students were taught to train CPR skills to lay people. Using a “peer-training” model, medical students train teachers, who in turn train children in CPR. Training consists of a two hour teaching session based on video, small group teaching and manikin practice. A standard checklist ensures acceptable performance of CPR. Schools are provided with teaching material and a manikin to promote retraining.
A 22 point multiple choice questionnaire was developed with emphasis on the main teaching points and performance of CPR. Year 8 children (aged 11–13 years) were trained by medical students (maximum ratio of 1:5), completing the questionnaire anonymously, before and immediately after training, and at six months. A Year 9 group received no training and completed the questionnaire at baseline and 6 months.
Results: 79 children were included (46 CPR group, 33 controls). All completed the questionnaire at baseline with 93.7% (43 CPR, 31 controls) completing at 6 months. Baseline knowledge was similar in the CPR and control groups. Baseline CPR knowledge was higher in those with a family history of heart problems (51.8% v 47.3%, p<0.05) but not affected by sex or previous CPR training. Mean age was significantly higher in the control group (12.7 v 11.8 years, p<0.05). Scores changed significantly following training (fig 1) with a mean increase from 46.8% to 82.7% (t-test, p<0.001). After 6 months, although scores decreased significantly they remained higher than baseline and control group scores (61.8% v 46.8/52.4% respectively, p<0.001).
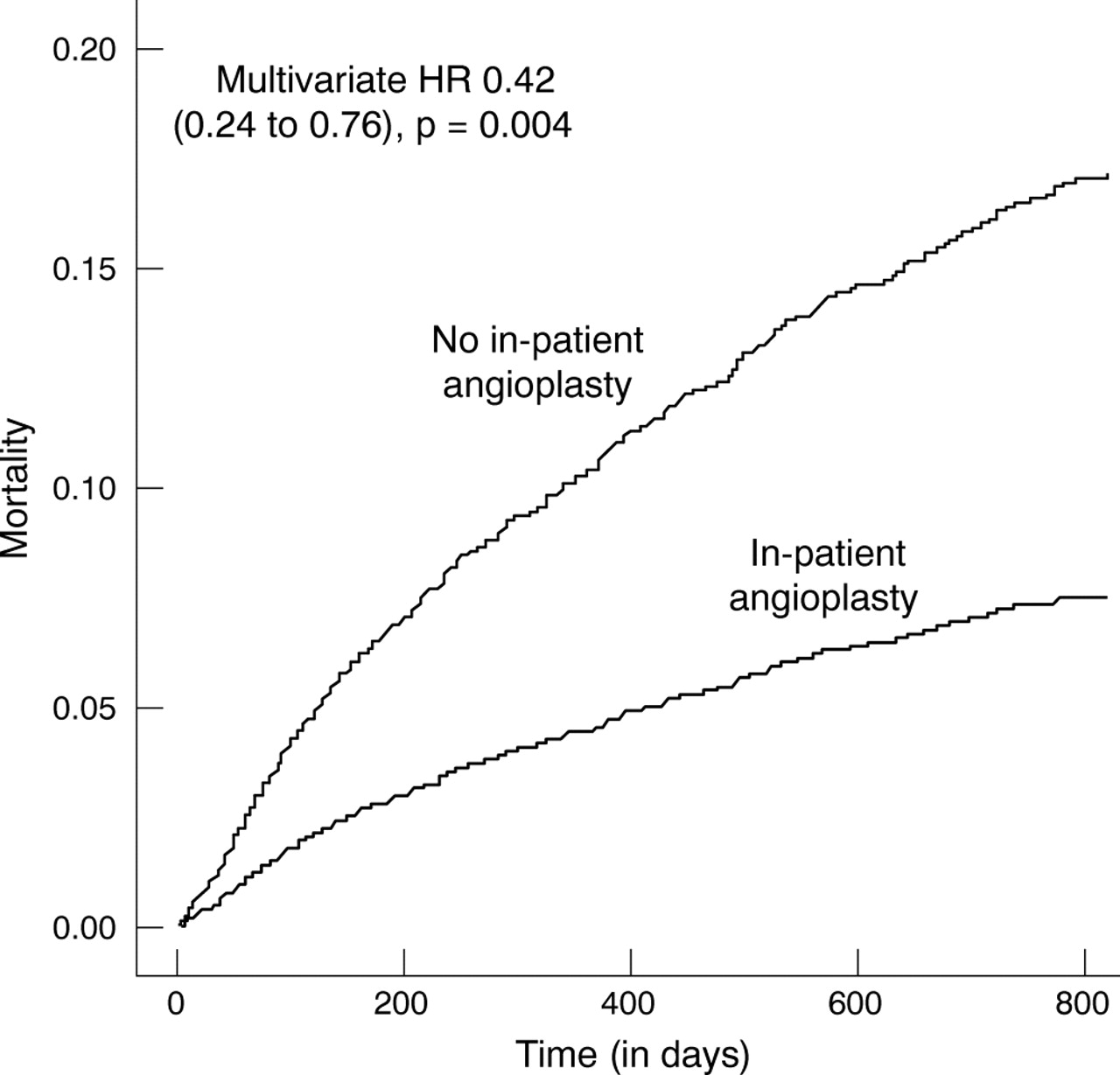
Abstract 192
Conclusion: Children can learn CPR skills through the “ABC for life” programme. Using a “peer-training” model, large numbers of children could successfully be trained each year. This would be the most efficient and cost effective method of increasing the proportion of the population capable of administering CPR and may have a major impact on survival figures for sudden cardiac events. As knowledge retention at 6 months is poor, provision needs to be made for future retraining.
CPR; training; children
193 SHOULD INTRAVENOUS AMIODARONE BE A FIRST-LINE TREATMENT FOR PHARMACOLOGICAL CARDIOVERSION OF HAEMODYNAMICALLY-TOLERATED SUSTAINED VENTRICULAR TACHYCARDIA?
D. Tomlinson, P. Cherian, T. Betts, Y. Bashir.John Radcliffe Hospital, Oxford, UK
Background: Current American Heart Association (AHA) and Resuscitation Council (UK) guidelines recommend intravenous amiodarone as a first choice treatment for haemodynamically-tolerated, sustained ventricular tachycardia. However, this advice is based on extrapolation of data from trials of intravenous amiodarone in shock-resistant ventricular fibrillation or to suppress recurrent haemodynamically-destabilising ventricular fibrillation. The efficacy and safety of standard (non-aqueous) intravenous amiodarone for termination of ventricular tachycardia in haemodynamically-stable patients has not been reported.
Methods: Retrospective analysis of 32 consecutive patients with sustained monomorphic ventricular tachycardia who received bolus intravenous amiodarone 150–300 mg. Primary end-points were: ventricular tachycardia termination within 15 and 60 mins, and incidence of hypotension and/or need for emergency DC cardioversion. The data were compared with historical controls from two randomised trials of intravenous lignocaine v sotalol or procainamide in the identical clinical setting (Ho et al 19941, Gorgels et al 19962).
Results: Baseline characteristics of the study population were: 25M:7F, mean (SD) age 68(13) years, left ventricular ejection fraction 0.32(0.12), Ischaemic heart disease (28/32), systolic blood pressure 109(23) mmHg and ventricular tachycardia cycle length 363(25) ms. Median ventricular tachycardia duration 54 mins (range 20 mins to 72 h). These did not differ significantly from the historical control groups.
Conclusions: Intravenous amiodarone was less effective than procainamide or sotalol for acute cardioversion of haemodynamically-tolerated, sustained ventricular tachycardia, with a slower onset of action and higher incidence of hypotension. These findings suggest the need for a prospective randomised trial to clarify the optimum agent for pharmacological termination of sustained monomorphic ventricular tachycardia in the emergency setting.
Abstract 193
amiodarone; ventricular tachycardia; guidelines
194 HOW USEFUL IS HOLTER MONITORING IN PATIENTS WITH PALPITATIONS OR ALTERED CONSCIOUSNESS? ANALYSIS OF 9729 RECORDINGS IN 8052 CONSECUTIVE PATIENTS
S. Sulfi1, N. Sekhri1, D. Balami1, K. Ranjadayalan1, A. Suliman1, A. Archbold2, A. Kapur2, A. Timmis2.1Newham University Hospital, London, UK; 2Barts and the London NHS Trust, London, UK
Background: 24-hour Holter monitoring is one of the most widely used non-invasive tests for diagnosis of palpitation and altered consciousness (dizziness, presyncope, syncope). Yet the diagnostic usefulness of Holter monitoring has not been systematically evaluated.
Method: We have prospectively recorded data in 8052 consecutive patients who underwent 9729 Holter recordings over a 13-year period. Data included demographics, indications for Holter monitoring and electrocardiographic analysis of the recording.
Result: Palpitation was the indication in 3066 patients who underwent 3537 Holter recordings. Diagnostic tachy-arrhythmias were recorded in 20.4% of all patients on the first recording, rising to 30.8% and 38.4% on second and third recordings (p<0.0001). Age was a major determinant of a diagnostic recording, rates rising from 8.2% in patients aged <30 years to 39.5% in patients aged >70 years (p<0.0001).
Altered consciousness was the indication in 3299 patients who underwent 3987 Holter recordings. Diagnostic tachy- or brady-arrhythmias were recorded in 13.7% of all patients on the first recording, rising to 17.9% and 15.2% on second and third recordings (p = 0.03). Age was a major determinant of a diagnostic recording, rates rising from 7.3% in patients aged <30 years to 16.9% in patients aged >70 years (p<0.0001).
Conclusion: The diagnostic usefulness of Holter monitoring in patients with palpitation or altered consciousness is age dependent, with pick-up rates for arrhythmias of less than 10% in younger patients but considerably higher in patients aged >70 years. Pick-up rates increase with repeat recordings but the data suggest that thresholds for Holter monitoring should be set at a high level in younger patients.
holter; palpitation; syncope
195 CASE SERIES OF SUDDEN CARDIAC DEATH
D. Chase1, P. Roderick1, P. Gallagher2, H. Burnley2, P. Roberts2, J. Morgan2.1University of Southampton, Southampton, UK; 2Southampton University Hospitals, Southampton, UK
Objective: The objective of this study was to establish whether Sudden Cardiac Death (SCD) victims could have been identified prior to their event and potentially considered for an implantable cardioverter defibrillator (ICD) on the basis of previous cardiac history recorded within healthcare records.
Methods: A case series of SCD in the UK (Southampton). Consecutive cases of adult SCDs presumed to be primarily caused by a ventricular arrhythmia as determined by an experienced pathologist with special interest in heart disease were identified over a 12-month period. SCD cases with clear evidence of acute myocardial infarction or coronary thrombosis were excluded from this study. Data were extracted from pathology and police reports. Hospital and GP notes provided information on previous symptoms, investigations and cardiac disease history. Two experts (Consultant Cardiologists, Electrophysiologists) judged the appropriateness of each case against pre-defined criteria.
Results: 975 Coroner’s post-mortems were undertaken, 366 of these cases were SCDs (38%). There was no clinical/pathological evidence of an acute myocardial infarction or thrombus in 232 of these cases (63% of all SCDs). Two hundred and fifteen of these cases lived within the catchment area and were included in this study. Sixty-four percent of cases were male and median age was 75 years. Thirty-seven percent of events were witnessed. Agreement between experts on appropriateness for an ICD was very good (kappa score of 0.64). One case (<1%) was considered appropriate for an ICD. Forty-one percent of cases had no evidence of confirmed or suspected heart disease. Fifty-eight percent of cases were considered to have required further cardiac investigations to determine appropriateness.
Conclusion: Two fifths of SCD victims had no recorded health service contact in relation to cardiac abnormalities or possible arrhythmia symptoms within their lifetime. A large number of patients suffered previous cardiac events or symptoms suggestive of a ventricular arrhythmia but were not referred for further investigations.
sudden cardiac death; implantable cardioverter defibrillators; case series
196 LONG QT PEAK MEASURED FROM A SINGLE ECG LEAD PREDICTS CARDIAC DEATH AND ALL-CAUSE MORTALITY
K. Wong1, R. MacWalter2, D. Douglas2, H. Fraser2, S. Ogston3, A. Struthers2.1Cardiothoracic Centre, Liverpool NHS Trust, Liverpool, UK; 2Tayside Institute of Cardiovascular Research, Ninewells Hospital and Medical School, Dundee, UK; 3Department of Epidemiology and Public Health, Ninewells Hospital and Medical School, Dundee, UK
Introduction: Stroke survivors are at high risk of cardiac death. Hidden but potentially treatable lethal cardiac abnormalities are common and often co-exist in stroke survivors.[1] QT peak prolongation is a novel marker of left ventricular hypertrophy and also appears to predict myocardial ischaemia. We have therefore tested the hypothesis that QT peak prolongation predicts cardiac death in stroke survivors.
Methods: ECGs were recorded from 296 stroke patients (152 male), mean age 67.2 (SD 11.6) approximately 1 year after the event. QT peak measurements were made in lead I and were heart rate corrected using Bazett’s formula (QTpc = QTp/RR1/2). The ECGs were digitised by a single observer who was blinded to patient outcome. The patients were followed up for a median of 3.3 years. The primary endpoint was cardiac death. Death from any cause was the secondary endpoint. Cox regression was carried out, comparing the cohort with QT peak in the upper tertile (346 ms or more) with the remainder to calculate relative risks of cardiac death and all-cause mortality. A Kaplan-Meier survival analysis was also carried out.
Results: A prolonged QT peak was associated with a 3.2 fold increased relative risk of cardiac death (RR = 3.2, 95% CI 1.2–8.2, p = 0.017). After adjustment for conventional risk factors of atherosclerosis (age, sex, pulse pressure, glucose, cholesterol, known ischaemic heart disease), QT peak prolongation was still associated with a 3-fold increased risk of cardiac death. (adjusted relative risk 3.0 (95% CI 1.1–8.5), p = 0.037). The Kaplan-Meier survival curves showed patients with long QT peak were at higher risk of cardiac death (log rank p = 0.012). With regards to the secondary endpoint, long QT peak was associated with a 3.2-fold increased risk of all-cause mortality (p = 0.017).
Conclusion: QT peak prolongation predicts cardiac death and all-cause mortality following stroke. Future research should test the hypothesis that reversal of QT peak prolongation might reduce the risk of cardiac death in this high risk population.
1
cardiac death; QT peak; all-cause mortality
197 DO RESTING AND EXERCISE ELECTROCARDIOGRAMS CONTRIBUTE INCREMENTALLY TO THE PROGNOSTIC ASSESSMENT OF PATIENTS WITH UNDIFFERENTIATED CHEST PAIN?
N. Sekhri1, C. Junghans2, G. Feder3, H. Hemingway2, A. Umaipalan3, R. Madhu3, A. Timmis3.1Newham University Hospital, London, UK; 2University College London, London, UK; 3Barts and The London, London, UK
Background: The rapid assessment of undifferentiated chest pain has been given high priority by policy makers but clinical factors and electrocardiogram (ECG) findings predictive of adverse outcomes in this patient population have not been defined.
Objectives: To measure the incremental value of the resting (r’ECG) and exercise (ETT) ECG in predicting adverse outcomes (CHD death, non-fatal acute coronary syndromes) in patients presenting to rapid access chest pain clinics (RACPCs).
Methods: We studied 1672 patients with undifferentiated, recent onset chest pain and no previous cardiac history who had resting and exercise ECGs as part of their clinical assessment, with a median follow up of 2.26 (IQR 1.51–5.11) years. We developed 3 iterative prognostic indices from clinical factors, clinical + r’ECG factors, and clinical + r’ECG + ETT factors. All significant covariates from each iterative model were used to calculate a prognostic index and c-statistic (ROC). Finally we refitted the model and applied it to 329 patients with follow up for from another chest pain clinic for external validation.
Results: The table shows covariates retained in the final prognostic models and the relevant c statistic for the main cohort and for the external validation sample.
Abstract 197
Conclusion: In patients with undifferentiated chest pain presenting to RACPCs, simple assessment of age, gender and typicality of symptoms embraces most of the prognostic information provided by the r’ECG and ETT. However these widely applied tests remain useful in this setting by providing incremental prognostic data that contribute to identification of patients at greatest risk of CHD death and non-fatal acute coronary syndromes.
exercise stress test; incremental value; prognosis
198 LEFT VENTRICULAR HYPERTROPHY IS A COMMONLY IGNORED BUT STRONG RISK FACTOR IN NORMOTENSIVE ANGINA PATIENTS
D. Ang, J. Davies, S. Pringle, A. Struthers.Ninewells Hospital/University of Dundee, Dundee, UK
Aims/hypothesis: Patients with coronary artery disease (CAD) are common and have a variable prognosis depending on various factors. A potentially reversible factor leading to cardiac death in CAD patients is left ventricular hypertrophy (LVH). However, cardiologists seldom pay attention to LVH because of the misconception that LVH is only a problem in hypertension. This is despite good data that LVH regression is an effective method of reducing morbidity and mortality. We took the first step to address this problem by assessing the prevalence of echocardiographic LVH in patients diagnosed with CAD in the UK.
Methods: 351 consecutive patients with the diagnosis of angiographically positive coronary artery disease were recruited into this study. M-mode measurement of left ventricular mass was carried out in each patient. In addition, 24 hour ambulatory blood pressure monitoring was carried out to see if this method is better at predicitng LVH than clinic blood pressure.
Results: Of the 286 patients in whom left ventricular mass could me successfully assessed, 149 (52%) had LVH (indexed to body surface area). The mean 24-hour ambulatory blood pressure reading was systolic 124 (16) mmHg and diasotlic 68 (8) mmHg in the group of patients with LVH. 63% of the patients in the LVH group had a normal 24 hour blood pressure reading. Conclusions: We conclude that echo LVH is remarkably common (52%) in patients with coronary artery disease. In additon, normotensive LVH (based on 24-hour blood pressure reading) is very frequent. This finding contradicts the long held assumption that only patients with hypertension are at risk of developing LVH. As LVH regression has been proven to be a favourable prognostic indicator, more attention should be paid towards detecting and treating this condition in patients with CAD.
echocardiographic left ventricular hypertrophy; coronary artery disease; prevalence
199 USE OF TROPONIN T MEASUREMENT IN PREDICTING MORTALITY AMONG HOSPITALISED PATIENTS
A. Khan, S. Murray, A. Ramsewak, A. Dhanasekeran, A. Robinson, U. Velupandian, G. Viswanathan, E. Rodrigues, P. Wong.University Hospital Aintree, Liverpool, UK
Introduction: Troponin T (TnT) measurement is widely used to assess patients with suspected acute coronary syndromes (ACS). These patients can be further categorised into 4 groups: (1) ACS with elevated TnT, (2) ACS with normal TnT, (3) non-ACS conditions with elevated TnT, and (4) non-ACS conditions with normal TnT. We investigated the in-hospital mortality and TnT in predicting death among patients admitted to hospital where TnT measurement was performed as part of their clinical assessment.
Methods: All patients admitted to a large university hospital over an 8-week period (5 January 2004 to 29 February 2004) who had TnT blood test were included. TnT level was routinely taken at 12 hours after symptom onset in accordance with a hospital wide policy. An elevated TnT level was defined as >or = 0.01 μg/l. Medical records were reviewed to ascertain the diagnostic category and hospital mortality.
Results: Of 1021 hospitalised patients where TnT level was measured, 313 (31%) had elevated TnT, and 708 (69%) had normal TnT. Patients with elevated TnT were older than those with normal TnT (mean age 74 (SD 12) v 66 (17); p<0.001), and there was no sex difference (female 48% v 51%; p = NS) between the two groups. Among these 1021 patients, there were 195 (19%) ACS with elevated TnT, 80 (8%) ACS with normal TnT, 118 (12%) non-ACS with elevated TnT, and 628 (61%) non-ACS with normal TnT respectively. Their in-hospital mortality was as follows.
Abstract 199
In-hospital total mortality was highest in patients who had non-ACS conditions with elevated TnT, and this was significantly higher than the other three groups (36% v 18% in TnT positive ACS; p<0.001). Cardiac mortality as a result of the primary condition accounted for 94% of all deaths in ACS patients with elevated TnT, comparing with 8% in those having non-ACS conditions with elevated TnT (p<0.001). No patient with a normal TnT had a primary cardiac death. Sensitivity and negative predictive value of a positive TnT in predicting cardiac death were 100% and 100%, and death of any cause were 79% and 97%, respectively.
Conclusions: Patients with non-ACS conditions and elevated TnT had the highest in-hospital mortality among our hospitalised patients where TnT measurement was performed. A normal TnT level was a good predictor for survival irrespective of the primary diagnosis.
Troponin T; mortality; hospitalised patients
200 LOWER CIRCULATING ENDOTHELIAL PROGENITOR CELL NUMBERS AND VASCULAR DYSFUNCTION IN HEALTHY YOUNG SOUTH ASIAN MEN
C. Murphy1, G. Kanaganayagam2, P. Chowienczyk2, A. Shah1, M. Marber2, M. Kearney1.1Denmark Hill Campus, King’s College London, London, UK; 2St Thomas’ Campus, King’s College London, London, UK
Introduction: South Asians in westernised countries have a higher incidence of coronary artery disease (CAD) than do white people. Potential determinants of this excess risk were examined.
Methods: 24 South Asian (25 (SD 5) years) and 25 age-matched white (26 (7) years) healthy non-smoking men without conventional risk factors for CAD were studied. Conduit vessel function was assessed by endothelium-dependent flow mediated dilatation (FMD) and endothelium-independent glyceryl trinitrate dilatation of the brachial artery. Resistance vessel function was assessed by forearm blood flow (FBF) responses to brachial artery infusion of the endothelium-dependent dilator acetylcholine (ACh) and the nitric oxide synthase inhibitor L-NMMA (to estimate basal NO production). Endothelial progenitor cells (EPCs) were quantified by flow cytometry as CD34, CD133 and KDR triple antigen positive cells.
Results: Body mass index, waist hip ratio, blood pressure, hsCRP and fasting glucose and lipids were similar in the 2 groups. South Asian men had significantly higher fasting insulin levels (6.01 v 3.62 uU/ml; p = 0.02). FMD (6.9 v 8.5%; p = 0.003), L-NMMA response (0.8 v 1.3 ml/min/100 ml; p = 0.03) and EPC count (0.046 (SD 0.005)% v 0.085 (0.009)%; p<0.001) were significantly lower in South Asian compared with white men. On multivariate regression, among various risk factors, EPC count was the strongest independent predictor of FMD and ethnicity was the strongest independent predictor of EPC count.
Conclusion: Young healthy South Asian men are more insulin resistant, have reduced endothelium-dependent vasomotor function and lower numbers of circulating EPCs. These abnormalities may contribute to their increased cardiovascular risk.
endothelial progenitor cells; vascular function; south asians
201 THE EFFECTS OF PERCUTANEOUS CORONARY INTERVENTION ON CIRCULATING ENDOTHELIAL PROGENITOR CELLS
N. Mills1, O. Tura2, C. Millar3, N. Lang1, D. Stirling3, C. Ludlam3, M. Turner2, G. Barclay2, D. Newby1.1Edinburgh University, Edinburgh, UK; 2Scottish National Blood Transfusion Service, Edinburgh, UK; 3Department of Haematology, Edinburgh, UK
Background: Endothelial progenitor cells (EPCs) are circulating mononuclear cells with the capacity to mature into endothelial cells, and to contribute to the process of vascular repair. We assess the effect of local vascular injury during percutaneous coronary intervention (PCI) on circulating levels of EPCs in patients with stable coronary disease.
Methods: Forty patients were recruited; 20 underwent diagnostic angiography alone and 20 received percutaneous intervention with balloon angioplasty and stenting. Peripheral blood samples were drawn before femoral artery catheterisation, immediately after, 6 hours after and 24 hours after angiography. Endothelial progenitor cells were quantified in whole blood by flow cytometry (CD34+KDR+) and by real-time PCR of leucocyte mRNA sequences, with functional EPC quantified using a colony forming unit (CFU) assay. Markers of inflammation and myocardial necrosis were assessed before and 24 hours after the procedure.
Results: Diagnostic angiography did not induce systemic inflammation or myocyte necrosis, nor affect the number of circulating CD34+KDR+ cells or CFU. Coronary intervention resulted in an increase in whole blood neutrophil count (mean 1.31(SD 0.35)×106 cells, p<0.001) at 24-hours, in the absence of significant myocardial necrosis (Troponin I, 0.04 (0.01) mg/dl). The number of functional EPC increased following PCI (baseline v 24 hours; 0.06 (0.02) v 0.23 (0.09)×104 CFU, p = 0.05), however, the number of circulating CD34+KDR+ cells (0.083 (0.011) v 0.083 (0.010)% of MNC, p = 0.75) and levels of leucocyte CD34 mRNA (2.26 (0.48) v 2.10 (0.42) RQ, p = 0.21) were unchanged. There was no correlation between the number of functional EPC and CD34+KDR+ cells at any time point. The number of circulating monocytes and levels of leucocyte CD14 mRNA fell transiently following catheterisation, but levels increased significantly 24 hours following PCI (2.5 (0.5) v 4.5 (1.0), p<0.05).
Conclusions: Local vascular injury following PCI results in a systemic inflammatory response and increases the number of functional EPCs. This increase was not associated with a mobilisation of CD34+KDR+ cells, suggesting these cells are not the primary source of circulating endothelial progenitors, and that they are not involved in the early response to vascular injury.
angioplasty; vascular injury; endothelial progenitor cells
202 MOBILISATION OF HAEMOPOIETIC STEM CELLS INTO PERIPHERAL BLOOD DOES NOT OCCUR IN ALL PATIENTS AFTER MYOCARDIAL ISCHAEMIA
V. Suresh1, E. Jaworska2, C. Pritchard3, A. Buckle4, S. Ray1, R. Chopra5.1Wythenshawe Hospital, Manchester, UK; 2Paterson Institute, Christie Hospital, Manchester, UK; 3Royal Cornwall Hospital, Truro, Cornwall, UK; 4UMIST, Manchester, UK; 5UCL, London, UK
Introduction: Preliminary preclinical and phase 1 studies in humans have suggested that mobilised haemopoietic stem cells (HSC) may contribute to the repair of ischaemic myocardial tissue. This has prompted us to hypothesise that after myocardial infarction (MI) there may be a de novo increase in circulating HSC. The kinetics of HSC circulation after MI is not well defined and the mechanism of their contribution of HSC to myocardial tissue repair is unclear. HSC may be attracted to the site of myocardial injury via cytokine/chemokine gradient, resulting in either neovascularisation and/or myocardial cell regeneration.
Objective: We aimed to establish whether and over what time course HSC are released in the peripheral circulation after myocardial infarction (MI) in humans. We investigated the expression of CD34+ and novel stem cell marker CD133+ on peripheral blood stem cell and also the time course of their release after ischaemic insult. We also investigated the stem cell expression of various endothelial markers like CD31+ and CD144+. We also measured various growth factors, chemokines and cytokines to ascertain whether they increased in the peripheral circulation and if so, whether there was any correlation with HSC release.
Material and methods: We recruited 5 patients with acute ST segment elevation MI, 5 patients with non-cardiac chest pain and 5 healthy controls. 20 ml of peripheral blood was obtained after informed consent on days 1–7 on patients with MI and non-cardiac chest pain and days 1, 4 and 7 on healthy controls. Stem cells were identified from the mononuclear cells (MNC) after fluorescent antibody staining and by using flow cytometry. Platelet poor plasma was used for measuring growth factors, chemokines and cytokines using ELISA technique.
Results: There was no significant increase in the HSC in the MI group when compared to the control. Furthermore, these HSC did not show an increased expression of endothelial markers CD31+ and CD144+. Vascular endothelial growth factor (VEGF), granulocyte colony stimulating factor (G-CSF), Interleukin-6 (IL-6) were significantly elevated in the MI group when compared to healthy controls. The VEGF peaked at day 4 after MI. Other chemo-attractants like monocyte chemo-attractant protein (MCP-1), stromal derived factor (SDF1-á), Interleukin-8 (IL-8) were not elevated. The results are shown in the table below.
Abstract 202
Conclusions: Preliminary results in a small number of patients’ reveals that HSC are not mobilised in peripheral circulation after myocardial ischaemia. Furthermore these HSC also failed to show increased expression of endothelial markers. These data highlight that HSC mobilisation does not occur in all patients with myocardial ischaemia and that de novo release of stem cells from the bone marrow is unlikely to be an important mechanism for myocardial repair.
myocardial infarction; stem cells; peripheral circulation
203 PROINFLAMMATORY AND WOUND-HEALING MACROPHAGES OCCUPY DISTINCT MICROENVIRONMENTS WITHIN THE VULNERABLE ATHEROSCLEROTIC PLAQUE
J. Boyle1, D. Horncastle2, P. Philippidis1, D. Haskard1, R. Landis1.1Imperial College Hammersmith Hospital, London, UK; 2Hammersmith Hospital, London, UK
Background: Intraplaque haemorrhage is a major contributor to atherosclerotic plaque growth and instability. This may be due in part to the pro-oxidant properties of ferrous haem released upon hemolysis. In vitro, haemoglobin is sequestered within macrophages via the haemoglobin-haptoglobin scavenger receptor CD163, expressed by cells that have differentiated in response to Th2 cytokines (IL-4, IL-10) into a putative alternatively-activated wound-healing phenotype. In contrast, classically-activated proinflammatory macrophages driven by Th1 cytokines (eg IFNγ) express HLA-DR. Although the concept of classical and alternative macrophage activation is well established, the relevance to atherosclerosis is less clear.
Methods and Results: We assessed macrophage phenotype in postmortem coronary artery ruptured plaques from fatal acute coronary syndrome (n = 8 cases). Sections were dual-stained by double immunohistochemistry for CD163 and HLA-DR using an immunoperoxidase-immunoalkaline phosphatase combination. This demonstrated compartmentalisation of CD163 and HLA-DR staining into distinct areas of the plaque. Out of a total of 6211 CD68+ (pan-macrophage marker) cells, 4577 (73.7%) stained positively for HLADR but not CD163, 1566 stained positively for CD163 but not HLADR (25.2%) and only 68 macrophages (1.1%) were HLA-DR/CD163 dual-positive (p<0.0001 for the inverse relationship between CD163 and HLA-DR by Chi square analysis). CD163+ macrophages were within 1 mm of CD34+ microvessels and colocalised with erythrocyte membranes (glycophorin staining). CD163+ macrophages were IL-10+ and contained intracellular iron (Perl’s stain). In contrast, HLADR+ macrophages were localised to the vicinity of the necrotic (lipid) core (within 1 mm) and expressed myeloperoxidase and matrix metalloproteinase-1 in parallel sections.
Conclusion: This is the first study showing distinct segregation of macrophages in plaques into reciprocal CD163+HLADR- and CD163-HLADR+ subpopulations. The balance between these subpopulations may differentially regulate inflammatory activity and healing within the vulnerable plaque.
vulnerable plaque; macrophage; oxidation
204 STIMULATED ENDOTHELIAL TISSUE PLASMINOGEN ACTIVATOR RELEASE PREDICTS FUTURE CARDIOVASCULAR EVENTS IN PATIENTS WITH CORONARY HEART DISEASE
S. Robinson1, D. Markie1, C. Ludlam2, N. Boon2, D. Newby1.1University of Edinburgh, Edinburgh, UK; 2Royal Infirmary of Edinburgh, Edinburgh, UK
Background: To date, most clinical studies have focussed on the assessment of endothelium-dependent vasomotion as a surrogate measure of endothelial function. However, the resolution of thrombus following atheromatous plaque rupture is critically dependent on the efficacy on endogenous thrombolysis. We assessed the relationship between acute stimulated tissue plasminogen activator (t-PA) release and future athero-thrombotic events in patients with stable coronary heart disease.
Methods: Forearm blood flow was measured using venous occlusion plethysmography in 100 patients with proven coronary heart disease (stable anginal symptoms for ⩾3 months) during intra-brachial infusion of substance P (2–8 pmol/min) and sodium nitroprusside (2–8 µg/min). Plasma concentrations of t-PA antigen, plasminogen activator inhibitor (PAI-1) and estimated net release of t-PA were determined during substance P infusion. Cardiovascular events, including death from cardiovascular causes, myocardial infarction (MI), ischaemic stroke (CVA), and hospitalisation for cardiac ischaemia were determined through the Information and Statistics Division of the NHS in Scotland and the General Register Office in Scotland.
Results: Patients had a typical cardiovascular risk factor profile and most were prescribed secondary preventative medications. Patients experiencing cardiovascular events (n = 21; median follow-up, 34 months) had similar baseline characteristics and vasodilator responses to substance P (p = 0.86) and sodium nitroprusside (p = 0.90). Net release of t-PA during substance P infusion was reduced by 91% in those subjects suffering death/MI/CVA, and 43% for those with Death/MI/CVA/hospitalisation for cardiac ischaemia (p = 0.02, ANOVA for both).
Conclusion: Acute endothelial t-PA release predicts the risk of future cardiovascular events in patients with stable coronary heart disease. In vivo assessment of endogenous fibrinolysis may be a more sensitive marker of endothelial dysfunction than impaired endothelium-dependent vasodilatation alone. Therapeutic interventions that augment acute t-PA release may represent a novel approach to the prevention of future cardiovascular events.
coronary heart disease; tissue plasminogen activator; prognosis

Abstract 204

Abstract 204
205 IMPAIRED SYSTEMIC MICROVASCULAR ENDOTHELIAL FUNCTION WITH CORONARY ARTERY DISEASE CAN BE DETECTED NON-INVASIVELY USING NOVEL LASER DOPPLER TECHNIQUES
S. Agarwal, J. Allen, A. Murray, I. Purcell.Freeman Hospital, Newcastle upon Tyne, UK
Introduction: Endothelial dysfunction (ED) is a diffuse process resulting in abnormal regulation of blood vessel tone and the loss of endothelial athero-protection. ED precedes overt cardiovascular disease therefore early detection may be of value in disease prevention. Since ED is generalised through the vascular bed, measurement of peripheral endothelium dependent vasodilatation (EDV) can possibly give information on ED in regions such as coronary circulation. Cutaneous laser Doppler (LDF) is a novel method which allows non-invasive measurement of microvascular EDV in response to provocative stimuli including acetylcholine (ACh) and local hyperthermia. However there is limited data involving this method in patients with coronary artery disease (CAD).
Aim: To assess endothelial function using laser Doppler flowmetry in patients with CAD compared with age and sex matched control subjects.
Methods: Cutaneous microvascular endothelial function was assessed by laser Doppler flowmetry. Twenty two healthy controls were compared with 32 patients with CAD. Endothelium dependent vasodilatory response was measured in response to local hyperthermia (controlled, localised heating of skin to 41 degree Celsius) and transcutaneous 1% acetylcholine, on the volar surface of the arm in a temperature controlled room at mean 23 (SD1) degree Celsius. Peak vasodilatation from the baseline was assessed and is expressed in arbitrary flux units (AFU).
Results: Subject characteristics are shown in table 1. All the patients with CAD were receiving statins. Body mass index (BMI) was higher in patients (29+4 kg/m2) compared with controls (26+3 kg/m2), p = 0.001. Eight patients had diabetes, 7 had hypertension. One control had hypertension. The peak vasodilatation stimulated by ACh was significantly higher in the control group (median 270, inter-quartile range 198–316 AFU) compared with the CAD group, (median 182, inter-quartile range 132–242 AFU), p = 0.004. Peak vasodilatation by hyperthermia was also significantly higher in the control group (median 95, inter-quartile range 75–137 AFU) compared to the patient group (median 56, inter-quartile range 41–68 AFU), p<0.001.
Conclusion: Using a novel laser based method we have demonstrated generalised microvascular endothelial dysfunction in patients with CAD. This simple non-invasive technique has great potential as a measure of endothelial function in clinical practise including response to therapeutic interventions.
Abstract 205
endothelial dysfunction; laser doppler; CAD
206 INHIBITION OF NEOINTIMA FORMATION IN HUMAN SAPHENOUS VEIN ORGAN CULTURE BY ADENOVIRUS-MEDIATED OVEREXPRESSION OF FIBROMODULIN
P. Ranjzad, H. Salem, P. Kingston.University of Manchester, Manchester, UK
Introduction: The success of coronary artery bypass grafting (CABG) is limited by poor long-term graft patency. Saphenous vein (SV) is the most commonly used conduit for CABG with a high failure rate due to intimal thickening and superimposed atherosclerosis. In the absence of any effective pharmacological therapies, late vein graft failure has been identified as a putative target for gene therapy. Two small leucine-rich proteoglycans, decorin and fibromodulin, possess TGF-β1-antagonist activity in vitro and in vivo. Local overexpression of decorin reduces neointima formation in response to arterial injury in animal models. However fibromodulin is a more effective competitor for TGF-β1 binding than decorin. The purpose of this study was to evaluate the ability of adenoviral-mediated gene transfer of bovine fibromodulin to inhibit neointima formation in an ex vivo model of vascular injury.
Methods: Excess surgically prepared SV segments from patients undergoing CABG were cannulated and the luminal surface was exposed to PBS or 108iu of 1 of 2 adenoviruses for 1 hour: Ad5-lacZ (expressing β-galactosidase) or Ad5-FMOD (expressing bovine fibromodulin). The vein segments were incised longitudinally and cultured luminal surface uppermost. Segments cultured for 14 days were fixed and paraffin-embedded. Sections stained for elastic tissues underwent morphometric assessment and the area of neointima and maximum neointimal thickness and I/M ratio were measured in each segment.
Results: (See table) Mean neointimal area (mm2) in vein segments exposed to Ad5-FMOD was significantly less than in PBS or lacZ groups (p = 0.0003 by ANOVA). I/M ratio and maximum neointimal thickness (µm) were also significantly reduced in veins exposed to Ad5-FMOD compared to controls (p = 0.008 & 0.018 respectively). Post-hoc analysis revealed that maximum neointimal thickness and I/M ratio did not differ significantly between PBS and lacZ groups, although neointimal area in lacZ vessels was significantly smaller than that in the PBS group (p<0.05). All parameters were significantly reduced in the Ad5-FMOD group compared with both control groups (all p<0.05).
Abstract 206
Conclusions: Fibromodulin overexpression significantly reduces neointima formation in an ex vivo model of vein graft intimal hyperplasia. Fibromodulin gene transfer thereby offers potential therapeutic benefit to reduce neointima formation associated with late vein graft failure.
gene therapy; vein graft disease; extracellular matrix
207 TARGETED MAGNETIC RESONANCE IMAGING OF TNF-ALPHA INDUCED ENDOTHELIAL VCAM-1 EXPRESSION IN VITRO USING MONOCLONAL ANTIBODY CONJUGATED MICROPARTICLES OF IRON OXIDE
M. McAteer, J. Schneider, N. Warrick, K. Channon, S. Neubauer, R. Choudhury.Department of Cardiovascular Medicine, University of Oxford, Oxford, UK
Introduction: Intracellular superparamagnetic microparticles of iron oxide (MPIO) have been shown to be useful for murine cell tracking using magnetic resonance imaging (MRI). Conjugation of MPIOs to specific antibodies may allow targeted molecular MR imaging of extracellular epitopes, such as VCAM-1, a marker of endothelial inflammation. Therefore the aims of this study were to investigate whether covalent conjugation of primary rat anti-mouse VCAM-1 antibody to MPIO (4.5 µm diameter) can specifically detect and quantify TNF-alpha induced VCAM-1 expression in cultured mouse endothelial (sEND) cells using high resolution MRI.
Methods: Mouse sEND cells (8×105) were stimulated in vitro for 20 hr with TNF-alpha (0.1, 1, 10 or 50 ng/ml) to induce endothelial VCAM-1 expression. The cells were then incubated in duplicate with either anti-VCAM-1-MPIO complexes or isotype anti-IgG-1-MPIO negative controls (1.2×106) for 30 min. Unbound beads were removed by extensive washing with phosphate buffered saline. The cells were examined for MPIO binding using light microscopy and the number of MPIO bound to sEND cell surfaces in 4 fields of view were quantified for each dose of TNF-alpha using ImagePro plus. The cells were then embedded in 2% agarose and MRI of cell phantoms was performed using an 11.7 T vertical magnet and a 40 mm probe with a home built sample holder allowing for imaging of up to 10 samples simultaneously. A 3D gradient echo sequence was used (TR/TE = 4/90 ms, field of view 30×30×30 mm, matrix size (512)3, two averages, imaging time∼13 h overnight) with a final isotropic resolution of 29.3 µm3 (after image reconstruction). The area of signal voids corresponding to MPIO in individual 2D images was quantified (8 images per sample selected at slice intervals of 293 µm) using a semi-automated histogram based approach.
Results: Using light microscopy, anti-VCAM-1-MPIO bound specifically to TNF-alpha stimulated sEND cells. No binding of anti-IgG-MPIO was observed. The number of anti-VCAM-1-MPIO binding to sEND cell surfaces increased significantly in response to increasing doses of TNF-alpha stimulation (r2 = 0.94, p = 0.03). By MRI, the area of anti-VCAM-1-MPIO in cell phantoms was also observed to significantly increase in a linear fashion in response to increasing dose of TNF-alpha stimulation (fig 1. r2 = 0.98, p = 0.01).

Abstract 207
Conclusions/implications: Anti-VCAM-1 antibody conjugated MPIO bind specifically and in a TNF-alpha dose-dependent manner to sEND cells in vitro as quantitatively assessed by light microscopy and MRI. The conjugation of VCAM-1 monoclonal antibody to MPIO may therefore be a useful strategy for targeted MRI investigation of VCAM-1 expression in mice in vivo.
VCAM-1; magnetic resonance imaging; iron oxide microparticles
208 AUTOANTIBODIES AGAINST HSP60 INDUCE ATHEROSCLEROSIS IN APO-E KNOCK OUT MICE VIA ENDOTHELAIL DAMAGE
K. Mandal, G. Foteinos, A. Afzal, M. Jahangiri, Q. Xu.St George’s Hospital Medical School, London, UK
Objectives: Accumulating evidence supports a positive association between anti-heat shock protein 60 (HSP60) autoantibodies and the presence of atherosclerosis in humans. However, whether these autoantibodies play a causal role in its development is still unknown.
Methods: Anti-HSP60 autoantibodies from blood of patients with coronary heart disease, scheduled for CABG, were isolated by affinity chromatography. These antibodies were injected in Apo-E deficient mice (with appropriate controls). Immuno-histochemical analysis of atheromatous tissues, obtained after killing them, was carried out.
Results: Mouse aortic sinus from hyperlipidemic apoE-deficient mice and wild-type controls were sectioned, stained with antibodies isolated from human sera, mentioned above. Positively stained cells appeared only in the atheromas. Injecting these autoantibodies into tail vein of apoE-deficient mice, resulted in significant increase (p<0.05) in atherosclerotic lesions in aortas, 8 weeks after injection (figure). Administration of a specific mouse monoclonal antibody (II-13) recognising amino acid residues 288 to 366 of HSP60 also effectively induced atherosclerotic lesions in apoE−/− mice. II-13 injection resulted in endothelial cell damage followed by increased leukocyte attachment, and accumulation of macrophages and smooth muscle cells in lesions. Interestingly, II-13-induced atherosclerosis was blocked by pretreatment of animals with F(ab)2 segments derived from the antibody, not mouse IgG F(ab)2.
Conclusions: Purified human anti-HSP60 autoantibodies recognise murine atheromatous cells. Monoclonal antibody, recognising amino acid residues 288 to 366 of HSP60, mimics the action of purified human antibodies. The pro-atherogenic effects are possibly mediated via autoimmune reactions to HSP60 expressed on arterial endothelial cells, which can be prevented by F(ab)2 segments derived from these antibodies.
HSP60/65; autoantibody; atherosclerosis

Abstract 208
209 DOES ATRIAL FIBRILLATION BEGET VENTRICULAR FIBRILLATION? AN ANALYSIS IN POST MYOCARDIAL INFARCTION PATIENTS
S. Kesavan, B. Nuta, S. Burtchaell, M. James.Taunton and Somerset NHS Trust, Taunton, Somerset, UK
Introduction: Atrial fibrillation remains an independent predictor of increased in-hospital and long-term mortality in post myocardial infarction patients. But the causes that lead to the increased mortality remains unexplained.
Hypothesis: We proposed that atrial fibrillation (AF) predisposes to ventricular fibrillation (VF) in post infarct patients thereby accounting for increased mortality.
Methods: 500 (358 - male, 142 - female) consecutive patients with a diagnosis of acute myocardial infarction were enrolled between March 2000-March 2002 for the study. Follow up period was between 2–4.6 years, with a mean follow up of 3.3 years. Patients were classified into two groups - AF group (124) and Non -AF group (376). The AF group was further subdivided into AF on admission - includes chronic AF (67) and New onset AF (57).We included a wide range of variables into the database, that might influence or confound the results.
Results: Mortality in patients in the AF group when compared to the non-AF group was 53% v 23%, p<0.001. AF correlated with advanced age, female sex, higher Killip class, previous myocardial infarction, hypertension, diabetes and heart failure. Univariate analysis showed that VF has no significant relation with age (p = 0.47), gender (p = 0.362), hypertension (p = 0.743), smoking (p = 1.000), beta blocker therapy on admission (p = 0.18), diabetes mellitus (p = 1.000), thrombolysis (p = 0.624) and a significant relation with ejection fraction (p = 0.04), infarct size (p = 0.043), peak CPK level (p = 0.01) and AF (P = 0.034). Multi variate analysis showed that only AF was significantly and independently related with VF. The correlation was stronger with AF on admission/chronic AF (p<0.001) than new onset AF. These data suggest that AF in the setting of myocardial infarction is an independent predictor of a worse outcome probably due to the occurence of VF.
Conclusion: AF in the setting of myocardial infarction is associated with an increased risk of VF. The mechanism by which AF triggers VF is not known but there are several possibilities. We believe it is due to the rapid stimulation of the vulnerable ventricle with short - long - short sequences. It could also be due to the beat to beat alteration in the mechano - electrical feedback in the ventricle or it may be an epiphenomenon. Chronic AF may alter ventricular electrophysiology thereby acting as a substrate and the sudden occurrence of acute myocardial ischaemia acts as a trigger for ventricular arrhythmias in the vulnerable period.
atrial fibrillation; ventricular fibrillation; mortality
210 TERMINATION OF CHRONIC ATRIAL FIBRILLATION BY CATHETER ABLATION MAY BE PREDICTED BY BASELINE FIBRILLATORY CYCLE LENGTH
M. O’Neill, Y. Takahashi, A. Jonsson, M. Hocini, P. Sanders, M. Rotter, F. Sacher, T. Rostock, P. Jaïs, J. Clémenty, M. Haïssaguerre.Hôpital Cardiologique du Haut Lévèque, Bordeaux, France
Background: A high rate of termination of chronic atrial fibrillation (AF) can be achieved by catheter ablation. This study evaluates some variables predictive of AF termination in a cohort of 97 consecutive patients.
Methods: Patients (mean 53 (SD 9) years) underwent catheter ablation of persistent or permanent AF (17 (25) months) using an irrigated-tip catheter. Ablation involved isolation of pulmonary veins and coronary sinus, all left atrial (LA) areas showing rapid/heterogeneous activity with the endpoint of local slowing or organisation, and linear lesions at the LA roof and mitral isthmus. Activation mapping and ablation was performed after conversion to atrial tachycardia until sinus rhythm was restored. Variables evaluated in relation to termination of AF included: sex, age, presence of structural heart disease, diagnosis of heart failure, amiodarone use, LA diameter, baseline AF cycle length (AFCL) in the LA appendage by averaging 30 consecutive cycles using automated software, duration of persistent AF, procedure and RF application.
Results: AF terminated in 82 patients (84%): directly to sinus rhythm in 13 (13%) or via ablation of intermediate atrial tachycardias in 69 (71%) patients. AF could not be terminated by ablation in 15 patients (16%). Of the variables evaluated, only baseline AFCL was significantly greater in patients with termination of CAF by ablation (155 (22) v 138 (16), p<0.01). Furthermore, procedure duration was inversely related to baseline cycle length (p<0.01 compared with CL 120–129, see fig).
Conclusions: Termination of persistent and permanent AF can be achieved in 84% of patients by catheter ablation. A short baseline AFCL is a strong predictor of failure of ablation therapy to terminate AF. Pretreatment which prolongs the AFCL may improve the outcome of catheter ablation in chronic AF.
atrial fibrillation; catheter ablation; cycle length

Abstract 210
211 RELATIONSHIP BETWEEN EXTENT OF LEFT ATRIAL ABLATION AND TERMINATION OF CHRONIC ATRIAL FIBRILLATION
M. O’Neill, A. Jonsson, P. Jaïs, P. Sanders, M. Hocini, Y. Takahashi, T. Rostock, M. Rotter, J. Clémenty, M. Haïssaguerre.Hôpital Cardiologique du Haut Lévèque, Bordeaux, France
Background: Termination of chronic atrial fibrillation (AF) by sequential catheter ablation of left atrial structures is accompanied by a progressive increase in cycle length (AFCL) measured at the LA endocardium. Knowledge of the number of steps required for termination of AF might be helpful in informing therapy strategy and potentially prevent futile left atrial ablation. We sought to evaluate if the baseline AFCL could serve as a procedure-specific predictor of ablation outcome.
Methods: Ninety-seven patients (mean 53 (SD 9) years) underwent catheter ablation of persistent or permanent AF (17 (25) months) using an irrigated-tip catheter. The procedure aiming at termination of AF initially involved three stages: pulmonary veins, coronary sinus and left atrial (LA) areas showing rapid/heterogeneous activity. In patients remaining in AF after 3 stages, linear ablation at the LA roof and mitral isthmus was performed (stage 4). Stage 5 addressed any deficiencies noted in the previous steps. Activation mapping and ablation was performed after conversion to atrial tachycardia until sinus rhythm was restored. Baseline AFCL was recorded at the beginning of each procedure in the LA appendage by averaging 30 consecutive cycles using automated monitoring software.
Results: Patients in whom AF terminated had a greater baseline AFCL than those in whom AF persisted. A sigmoidal relationship was observed between the number of ablation steps required and termination of AF.
Conclusion: For each ablation stage performed, there is an incremental benefit in terms of termination of AF however, the relative proportion of patients in whom AF terminates decreases after three ablation steps. A low baseline AFCL together with ongoing AF by stage 4 may be predictive of ultimate procedural failure and could therefore be used to avoid unnecessary RF ablation in the LA.
atrial fibrillation; ablation; cycle length

Abstract 211
212 WAVELET ANALYSIS USING A MODULUS MAXIMA METHOD TO PREDICT RHYTHM STATUS AFTER CARDIOVERSION FOR PERSISTENT ATRIAL FIBRILLATION
A. Shah1, P. Addison2, J. Watson2, N. Uchaipichat2, N. Grubb3.1University of Edinburgh, Edinburgh, UK; 2Cardiodigital, Edinburgh, UK; 3Royal Infirmary of Edinburgh, Edinburgh, UK
Background: Wavelet transforms allow real time analysis of complex signals to provide temporal and spectral information. The aim of this study was to determine whether parameters derived from wavelet analysis of ECG signals can predict medium term outcome from elective DC cardioversion (DCC) with sufficient accuracy to be clinically useful, in patients with atrial fibrillation (AF).
Method: Thirty patients with persistent AF were enrolled. A three lead ECG was obtained from each patient before DCC, via a Datex Ohmeda CardioCap5 Machine onto a laptop computer. Five minutes of continuous electrocardiogram signal was sampled at 300 Hertz. Signals were analysed offline using a modulus maxima algorithm, and outcome of DCC was evaluated in relation to combinations of frequency, amplitude and entropy. ECGs were examined 28 days after DCC to determine rhythm status.
Results: Of 30 patients enrolled, six (20%) failed to cardiovert. At four weeks, 13 (43%) patients were in sinus rhythm and 11 (36%) reverted into AF. Of the wavelet parameters investigated, several predicted outcome at 4 weeks but the combination of peak spectral amplitude and wavelet entropy was the best predictor (see scatter plot). A linear decision boundary can be used to identify patients that sustain sinus rhythm for at least one month after DCC with 100% sensitivity and 76% specificity. These results compare favourably with previous reports utilising smoothing and Fourier analysis for DCC outcome prediction.
Conclusion: Although clinical markers can be used to predict outcome after DCC, these have limited predictive power. Wavelet analysis may provide an insight into the electrical status of atrial tissue during atrial fibrillation, and in this limited study was a good predictor of medium-term outcome. Larger scale clinical outcome studies are planned to determine whether wavelet analysis can be usefully incorporated into a clinical predictive algorithm, and to assess the impact of antiarrhythmic drugs on peak spectral amplitude and wavelet entropy.
wavelet analysis; external DC cardioversion; atrial fibrillation

Abstract 212
213 EFFECT OF ANGIOTENSIN II TYPE 1 RECEPTOR (AT1R) BLOCKADE ON ATRIAL ELECTROGRAM MORPHOLOGY IN A BURST PACED GOAT MODEL OF ATRIAL FIBRILLATION
S. Kirubakaran1, M. Hall1, R. Chowdhury2, N. Peters2, C. Garratt1.1Manchester Heart Centre, Manchester, UK; 2Imperial College, London, UK
Background: It has been postulated that the self-perpetuation of AF is caused in part by localised abnormalities in cell-to-cell conduction (structural remodeling) and that this process may be inhibited by angiotensin II type 1 receptor (AT1R) blockade. We examined this hypothesis in a chronic conscious goat model of AF.
Method: Fifteen goats underwent pacemaker implant. Three goats were kept in sinus rhythm (controls) and the remaining twelve goats underwent atrial burst pacing as per the Allessie protocol for 1 month (3 candesartan, 3 placebo) and 3 months (3 candesartan, 3 placebo). Goats were cardioverted and then atrially paced at 400 ms. Epicardial mapping was performed on the right atrium using a multipolar rectangular array of 70 unipolar electrodes with a 3.57 mm interelectrode separation. Electrograms were acquired using a Cardiomapp system at a sampling rate of 1 kHz. The morphology of the atrial unipolar electrograms were divided into 3 categories: single potentials, double potentials (the amplitude of the smallest being ⩾25% of the amplitude of the largest) and fractionated potentials (exhibiting more than two negative deflections). Atrial conduction velocity was calculated by the method of triangulation.
Results: After 3 months of AF, although overall conduction velocity did not change, atrial electrograms became more prolonged and fractionated (table). There was no difference between placebo and candesartan treated goats at any AF duration.
Abstract 213
Conclusion: Local atrial electrograms increase in duration and are more fractionated after 3 months of AF, with no change in overall conduction velocity. These findings are consistent with localised conduction abnormalities as a contributory cause to the self perpetuation of AF and are unaffected by AT1R blockade.
atrial fibrillation; electrograms; angiotensin
214 POOR OUTCOME OF ATRIAL FIBRILLATION ASSOCIATED WITH HYPERTHYROIDISM
F. Osman, J. Franklyn, M. Sheppard, M. Gammage.Queen Elizabeth Hospital, Birmingham, UK
Background: Atrial fibrillation is common in hyperthyroidism and may account for the excess vascular mortality reported in these patients.
Aim: To evaluate the prevalence and outcome of AF associated hyperthyroidism and predictors of its successful reversion to sinus rhythm.
Methods: 425 consecutive unselected patients with hyperthyroidism recruited (334 females/91 males). All had 12-lead ECG and 24hr Holter monitoring before and after antithyroid therapy.
Results: Thirty-five patients (8.2%) had persistent or paroxysmal AF (PAF) at recruitment (24 females, 11 males), median age 71.0 yrs (IQR 64–77): 25 newly diagnosed (20 persistent AF, 5 PAF) and 10 known AF prior to hyperthyroidism (9 remained in AF after treatment of hyperthyroidism, 1 reverted with sotalol). Of the 20 with newly diagnosed persistent AF 14 remained in AF, 6 reverted to sinus rhythm. Of the 5 with PAF, none had PAF at follow-up; 6 underwent electrical cardioversion once euthyroid, 2 successfully (newly diagnosed AF) and 4 failed (3 newly diagnosed, 1 previously known). Overall, 12 successfully achieved sinus rhythm at follow-up: 5 spontaneously (mean 18.0 (SD 2.9) weeks following recruitment), 5 on drug therapy (19.8 (6.1) weeks following recruitment) and 2 electrically. Electrical cardioversion was declined by 7 and not offered to 8. Multivariate regression revealed increasing age (p<0.0001), known cardiac failure (p<0.0001), diabetes (p<0.02), systolic blood pressure at recruitment >140 mm Hg (p<0.005) and LVH on resting ECG (p<0.02) independently predicted AF at presentation. Those reverting successfully were more likely to have been rendered initially hypothyroid (defined as serum TSH >5.5 mU/l and low serum free T4) compared with those remaining in AF (58% v 13%, p<0.02). Independent predictors of successful reversion were lower systolic blood pressure at presentation (p<0.02) and an initial hypothyroid state (p<0.009).
Conclusions: AF is common at presentation of hyperthyroidism. Those with persistent AF have a poor outcome in terms of restoration of sinus rhythm despite treatment of thyroid dysfunction. Actively inducing an initial hypothyroid state may facilitate reversion to sinus rhythm.
hyperthyroidism; atrial fibrillation; predictors
215 CARDIAC DYSRHYTHMIAS IN HYPERTHYROIDISM BEFORE AND AFTER ANTITHYROID THERAPY
F. Osman, J. Franklyn, M. Sheppard, M. Gammage.Queen Elizabeth Hospital, Birmingham, UK
Background: Overt and subclinical hyperthyroidism are known to induce many cardiovascular effects including dysrhythmias and are associated with significant vascular morbidity and mortality.
Aim: To evaluate dysrhythmia risk in overt hyperthyroidism before and after effective antithyroid therapy.
Methods: 408 consecutive unselected patients with overt hyperthyroidism were recruited with 408 age/sex-matched euthyroid controls for comparisons; all had 24-hour Holter monitoring. Patients were reassessed after antithyroid therapy and comparisons made between those rendered euthyroid and their matched controls.
Results: The median age of both cohorts was 50.0 yrs (IQR 37–65); 320 females and 88 males in each. Cohorts were matched with respect to past and family history of vascular disease (20% v 18% and 68% v 70%, p = ns). Median presentation serum free thyroxine (T4) and tri-iodothyronine (T3) concentrations in patients were 37.5 pmol/L (IQR 27–52) and 11.4 pmol/L (IQR 8–18); serum TSH was undetectable in all. Serum free T4 and TSH were normal in all controls. Persistent and paroxysmal AF was more prevalent in hyperthyroid patients than controls (8% v 1%, p<0.0001) as were atrial salvoes (>3 consecutive atrial ectopics, 24% v 14%, p<0.002). Ventricular salvoes (>3 consecutive ventricular ectopics) and non-sustained VT (>5 consecutive ventricular beats lasting <30 sec) were no different (4% v 1%, p = 0.1 and 2% v 0%, p = 0.3). Significant atrial or ventricular ectopics (>240/24 hr) were also no different (7% v 5%, p = 0.8 and 7% v 8%, p = 0.7). After antithyroid therapy, 219 were rendered biochemically euthyroid (mean follow-up 36.9 (SD 1.6) weeks). AF was still more prevalent in patients than controls (6% v 1%, p<0.0001); all other rhythm disturbances were no longer different.
Conclusions: Hyperthyroidism is associated with a marked prevalence of supraventricular dysrhythmias at presentation, especially AF, which persists even after restoration of euthyroidism. This may account, in part, for our previously reported excess vascular mortality in subjects with treated hyperthyroidism.
hyperthyroidism; atrial fibrillation; dysrhythmias
216 THE PACEMAKER ATRIAL FIBRILLATION STUDY: THE EFFECT OF ANTI-ATRIAL FIBRILLATION PACING ALGORITHMS IN PATIENTS WITH PAROXYSMAL ATRIAL FIBRILLATION
J. Silberbauer1, L. Boodhoo1, A. Arya1, N. Freemantle2, D. Hildick-Smith3, S. O’Nunain3, G. Lloyd1, K. Kamalvand4, P. O’Kane5, N. Patel1, A. Sulke1.1Eastbourne General Hospital, Eastbourne, UK; 2University of Birmingham, Birmingham, UK; 3Royal Sussex County Hospital, Brighton, UK; 4William Harvey Hospital, Ashford, UK; 5Ashford and St Peters Hospital, Chertsey, UK
Introduction: The pacemaker atrial fibrillation study (PAFS) is a randomised, multicentre, investigation of the effects of anti-AF pacing algorithms in patients with paroxysmal atrial fibrillation (PAF). Patients were implanted with DDDRP devices (Vitatron T70 and Selection 9000) with sophisticated holters assessing AF burden, episode no and AF onset mechanisms.
Methods: With at least 3 symptomatic episodes of PAF resistant to at least 2 anti-arrhythmics 182 patients (mean 72 (SD 9) years, 55% male) were enrolled. Holter-derived AF burden of 1–50% was required in the initial 2 month monitoring phase (DDD 50 or DDI 60). 79 patients fulfilled these criteria and were then randomised to 4 phases of 1 month each in a within patient crossover design. The 3 active phases were “Rate Soothing”, “Ventricular Rate Stabilisation” and “All On” which included these 2 algorithms plus Post AF Response. Principal outcomes were analysed using repeated measures analyses in SAS Proc Mixed (v 9.12) and active phases were compared to “All Off” (DDD 60). The majority of atrial leads were sited in the right atrial appendage (RAA).
Results: 42% of patients had no AF throughout the monitoring phase confirming the efficacy of bradycardia dual chamber pacing alone. There was no significant decrease in AF burden or AF episode number with any algorithm (See table). However, the percentage of AF onsets induced by premature atrial contractions (PAC) was significantly reduced by Rate Soothing. The VRS algorithm increased ventricular pacing and the Rate Soothing algorithm increased atrial pacing appropriately. This study was powered to detect a 22% AF burden reduction, in each study phase.
Abstract 216
Conclusion: None of the studied algorithms increased AF burden, pt symptoms or induced any pro-arrhythmia. However, 42% of PAF pts are “cured” with bradycardia pacing alone.
RAA overdrive pacing using the Rate Soothing algorithm reduces PAC-initiated PAF. Despite this there was no overall AF burden or PAF episode reduction with any pacing algorithm.
atrial fibrillation; pacemaker; algorithms
217 QUALITY OF LIFE AND SYMPTOMATOLOGY IN PATIENTS WITH ANTI-AF PACEMAKER IMPLANTED TO TREAT PAROXYSMAL ATRIAL FIBRILLATION
J. Silberbauer1, L. Boodhoo1, A. Arya1, P. O’Kane2, K. Kamalvand3, N. Patel1, A. Sulke1.1Eastbourne General Hospital, Eastbourne, UK; 2Ashford and St Peters Hospital, Chertsey, UK; 3William Harvey Hospital, Ashford, U K
Introduction: The multicentre randomized PAFS trial assessed the effect of pacing algorithms using Vitatron T70 and Selection 9000 DDDRP pacemakers in paroxysmal atrial fibrillation (PAF) patients. The study assessed the effect of atrial overdrive, ventricular rate stabilisation and ERAF suppression algorithms on patient quality of life (QOL) and symptoms.
Methods: Inclusion required ⩾3 documented symptomatic episodes of PAF resistant to ⩾2 anti-arrhythmics. 182 patients (mean72 (SD 9) years, 55% male) were enrolled. Patients completed the Short Form-36 (SF-36), Visual analogue scales (VAS), specific symptom scores (SSS) questionnaires and a symptom diary for each of 4 monthly study phases. The 3 active phases were “Rate Soothing”, “Ventricular Rate Stabilisation” and “All On” which included these 2 algorithms plus Early Recurrence of AF (ERAF) suppression. Questionnaire scores were analysed using a repeated measures analysis in SAS Proc Mixed (v9.12). All active phases were compared to the control phase “All therapies Off (DDD 60)”.
Results: There was no difference in any of the SF-36 subscales (p = ns). VAS was divided into general health, mental health and physical health. There was no significant difference in any of these scales (p = ns). There was no difference in any SSS parameter or total SSS score (p = ns). The rate of specific AF symptoms, non-specific AF symptoms, unrelated symptoms and total AF symptoms did not vary significantly across phases as assessed using the patient symptom diaries.
Abstract 217
Conclusion: QOL and day to day symptoms was not significantly affected by continuous atrial overdrive, ventricular rate stabilisation or ERAF suppression pacing algorithms in drug resistant PAF patients using dual chamber anti-AF pacemakers.
symptom; pacemaker; atrial fibrillation
218 WHAT PROPORTION OF HEART FAILURE PATIENTS IN SOUTH WEST GLASGOW WOULD BE ELIGIBLE FOR CARDIAC RESYNCHRONISATION THERAPY AND WHAT WOULD THE IMPLICATIONS BE?
D. Murdoch, A. Davie, J. Byrne, R. McGeoch.Southern General Hospital, Glasgow, UK
Introduction: The prevalence of heart failure in the general population of Scotland is 7.1 in 1000 increasing to 90.1 in 1000 among those who are 85 or over. Recent trials have shown that cardiac resynchronisation therapy (CRT) in selected heart failure patients improves morbidity and mortality. This treatment is yet to get widespread funding in Scotland. Our aim is to evaluate which proportion of patients in our catchment area would be suitable for CRT and what the financial implications would be.
Methods: We conducted a case note search of the South West Glasgow Heart Failure Liaison Nurse Service database for people satisfying these criteria: 1. New York Heart Association class III or IV 2. QRS duration >120 ms 3. Standard pharmacological therapy 4. Moderate or severe left ventricular dysfunction on echocardiography. The notes of those who met the criteria were scrutinised further with regard to ECG rhythm and co-morbidity.
Results: We looked at the case notes of 126 of the 130 patients in the heart failure liason nurse service. In total, 25 (19.8%) met the above noted criteria. The age range was 60 to 85 with a mean age of 70.4 years. Seventeen (68%) were male and 8 (32%) were female. Ninety two per cent were NYHA class III and 8% were NYHA class IV. Of these 25 patients 10 had to be excluded because of atrial arrythmias. This left 15 (11.9%) of patients eligible. A number of these patients (3) had co-morbidities which would need further evaluation prior to any procedure and other (3) had room for optimisation of drug therapy.
Conclusions: Therefore in our catchment area only 7.1% (9/126) of our heart failure patients would be defined as candidates for CRT. This would result in an initial outlay of 35 100 pounds sterling for our unit. The number is less than our initial estimations and if mirrored throughout Scotland the financial implication would not be prohibitive.
heart failure; cardiac resynchronisation therapy; financial implications
219 PROLONGED QT PEAK IS A GOOD PREDICTOR OF RESPONSE TO CARDIAC RESYNCHRONISATION THERAPY
A. Patwala1, K. Wong1, R. Clements2, P. Woods2, D. Goldspink2, D. Wright1.1The Cardiothoracic Centre, Liverpool, UK; 2RISES, Liverpool John Moores University, Liverpool, UK
Background: Cardiac Resynchronisation therapy (CRT) is now recognised as a treatment for patients with severe heart failure and evidence of electromechanical dyssynchrony. The trials to date have used a prolonged QRS duration as a marker of dyssynchrony. However these trials have shown significant non-responder rates of approximately 20%. The main benefit of using a prolonged QRS duration is the ease of measurement from a 12-lead ECG. QT peak is similarly easy to measure and T peak appears close to the onset of repolarisation. We therefore performed a prospective study to assess if QT peak was any better at predicting CRT response than QRS duration.
Methods: 33 patients referred for CRT were recruited. Pre CRT, a resting 12-lead ECG was taken and patients performed a modified Bruce protocol treadmill test with measurement of peak VO2. Patients were assessed again 3 months post CRT with a further measurement of peak VO2. A responder was defined as a patient who showed an improvement in peak VO2 at 3 months.
The baseline ECG was analysed by one observer who was blinded to the peak VO2 results. QRS duration and QT peak were measured from lead I. The heart rate corrected QT peak was calculated using Bazett’s formula (QT peak/square root of the preceding RR interval). Aortic pre-ejection period, defined as start of QRS to start of aortic inflow, was measured in all patients via transthoracic echocardiography.
Results: There was significant improvement in peak VO2 at 3 months post CRT (baseline 16.06 (SD 0.74) v 3 months 18.52 (0.75), p<0.001). In this study 23 patients were responders and 10 were non-responders. QRS duration did not predict improvement in peak VO2 at 3 months (160 ms (5.9) ms in responders v 163 ms (8.9) ms, p = 0.78). In contrast, QT peak was significantly longer in responders (395 (8.3) v 363 (12.5), p = 0.039) [Fig 1]. The longer the baseline QT peak the greater the benefit in peak VO2-this relationship was continuous (Spearman r = 0.4 2-tailed p = 0.041). A QT peak cut-off value of 390 ms has a sensitivity of 61% and specificity of 70% at predicting improvement in peak VO2. Using a lower cut-off value of 290 ms, no cases that would benefit from CRT would be missed. [Area under the ROC curve was 0.75, SE 0.086, p = 0.027]. QT peak also correlated with the aortic pre-ejection time (Spearman r = 0.36, 2-tailed p = 0.041).
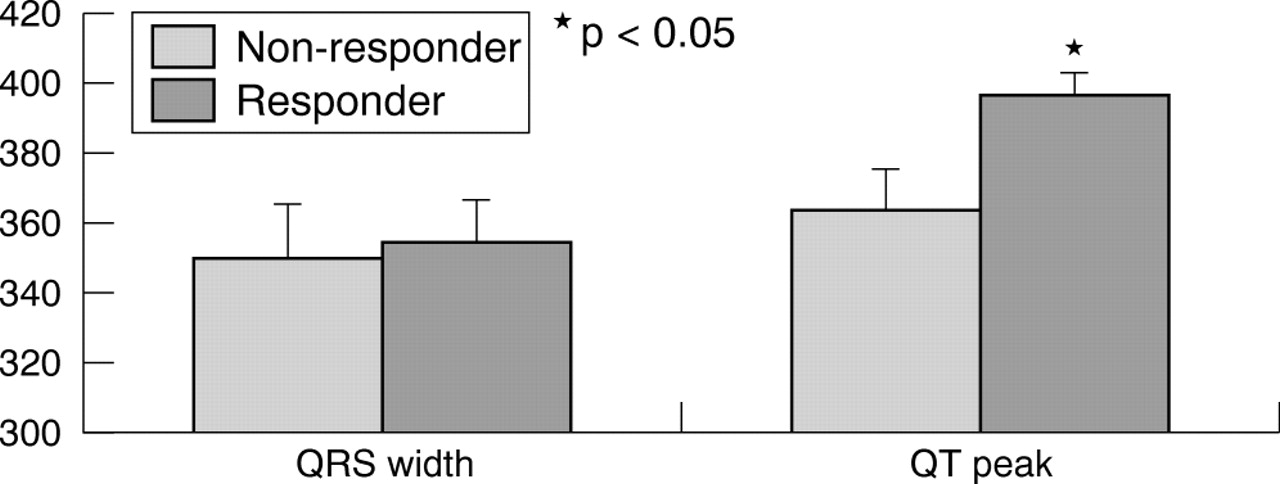
Abstract 219
Conclusions: Prediction of response to CRT is of major interest. As shown in previous clinical trials, a prolonged QRS duration is not a predictor of response. QT peak is a much better predictor of response. The ease of measurement is similar to QRS width and does not require any new equipment or skills. A possible mechanism explaining the ability of QT peak to predict response to CRT is that QT peak correlated with the aortic pre-ejection time, prolongation of which above 140 ms represents echocardiographic evidence of dyssynchrony.
QT peak; cardiac resynchronisation therapy; QRS duration
220 DO PATIENTS WITH ATRIAL FIBRILLATION BENEFIT FROM CARDIAC RESYNCHRONISATION THERAPY?
A. Patwala1, R. Clements2, P. Woods2, S. Williams1, D. Goldspink2, L. Tan3, D. Wright1.1The Cardiothoracic Centre, Liverpool, UK; 2RISES, Liverpool John Moores University, Liverpool, UK; 3Academic Unit of Molecular Vascular Medicine, University of Leeds, LGI, Leeds, UK
Background: The major multi-centre trials to date assessing cardiac resynchronisation therapy (CRT) have focussed on patients in Sinus Rhythm (SR). Currently little clinical outcome data exists to confirm whether similar benefits are seen in those patients with atrial fibrillation. We therefore performed a prospective trial to assess the benefits of CRT in patients with atrial fibrillation (AF) compared to a control group in SR.
Method: 13 patients with AF, symptomatic heart failure despite optimal medical therapy and a QRS width >120 ms were recruited. Patients were assessed pre and 3 months and 6 months post CRT. At each visit triplicate resting cardiac output measurements were made using the equilibrium method of Collier. A modified Bruce protocol treadmill was then carried out to assess peak VO2 and peak cardiac output was measured using the exponential method of Defares. The patients New York Heart Association (NYHA) class was also recorded at each visit. Peak and resting cardiac power output (CPO) were then calculated using the formulae: CPO = cardiac output x mean arterial pressure × 2.22×10−3. Cardiac reserve (CR) was calculated by subtracting Rest CPO from Peak CPO. The results were compared to a control group who were age, sex and peak VO2 matched at baseline and in sinus rhythm. A repeated measures ANOVA was used to look for improvements between the baseline and post tests.
Results: At baseline there was no significant difference in any variables between the control and AF group. By three months there were significant improvements in NYHA class, exercise duration, peak CPO and CR in both groups. Peak VO2 was significantly improved by 3 months post CRT in the control group whilst in the AF group the improvement was significant at 6 months. There were no statistically significant differences between the improvements in the 2 groups (see table 1, results shown as mean (SE)).
Conclusions: In our study patients with AF improved to a similar level when compared to sinus rhythm CRT patients. Peak VO2 improvement was slightly delayed in the AF group, however by 6 months both groups showed very similar improvements. We therefore feel that in appropriate patients with AF, CRT should be considered as past of the management strategy.
atrial fibrillation; cardiac resynchronisation therapy; cardiac power output
221 MULTI-STAGE IMPROVEMENT IN FUNCTIONAL AND HAEMODYNAMIC STATUS FOLLOWING CARDIAC RESYNCHRONISATION THERAPY
A. Patwala1, P. Woods2, R. Clements2, K. Albuoaini1, D. Goldspink2, L. Tan3, D. Wright1.1The Cardiothoracic Centre, Liverpool, UK; 2RISES, Liverpool John Moores University, Liverpool, UK; 3Academic Unit of Molecular Vascular Medicine, University of Leeds, LGI, Leeds, UK
Background: Cardiac resynchronisation therapy (CRT) has been shown to improve functional capacity, quality of life and mortality in suitable patients. The rate at which this improvement occurs, and the underlying physiological changes have not been fully described. We longitudinally evaluated the inter-relationships in physiological variables to better understand the benefits of CRT.
Methods: 50 patients (mean age 64 years [range 38–80]) were assessed pre CRT and 2 weeks, 6 weeks, 3 months and 6 months post CRT. Each test was conducted over 2 days. On the first day triplicate resting cardiac output measurements were made using the equilibrium method of Collier. A modified Bruce protocol treadmill test was then carried out to assess peak VO2 and peak cardiac output was measured at maximal exercise using the exponential method of Defares. On the second day a further peak cardiac output measurement was taken. After 30 minutes rest peak skeletal muscle torque was measured in flexion and extension at both knees with a Biodex isokinetic dynamometer using a 60-degree/sec protocol. Peak and resting cardiac power output (CPO) was calculated using the formulae: CPO = cardiac output x mean arterial pressure × 2.22×10−3. Cardiac reserve (CR) was calculated by subtracting CPORest from CPOPeak. A repeated measures ANOVA was used to look for statistically significant differences between the baseline and post CRT tests.
Results: Post CRT there is a significant improvement in functional class, exercise duration, peak VO2 and exercise haemodynamic measures after only two weeks. This improvement is then followed by further significant improvements until 6 months post CRT. Peak skeletal muscle torque during extension shows a trend towards improvement over the 6 months however this only achieves statistical significance on the left side. Peak torque during flexion is unchanged throughout. Full results are shown in table 1 (as mean (SE)).
Conclusions: CRT significantly improves exercise capacity and functional class, as shown in previous trials. Significant improvements occur within two weeks and therefore it is feasible to check responder status at this stage. Early identification of non-responders would allow further management decisions to be made. The overall improvement described in trials at 6 months is composed of multiple significant improvements especially at the 3 and 6 months stage. However despite these improvements skeletal muscle function is not significantly improved in most cases. This may reflect chronic muscle deconditioning, the reversal of which is delayed beyond an initial improvement in functional capacity. A rehabilitation programme post CRT focussing on improving skeletal muscle strength could potentially lead to a further increase in exercise capacity than CRT alone.
cardiac resynchronisation therapy; cardiac power output; exercise tests
222 CLINICAL AND ECHOCARDIOGRAPHIC RESPONSE IS SUSTAINED BEYOND 4 YEARS OF CARDIAC RESYNCHRONISATION THERAPY
B. Gordon, M. Harbinson, E. Chew.Belfast City Hospital, Belfast, UK
Background: The ultimate responder to cardiac resynchronisation therapy (CRT) could be considered as the patient who has prolonged survival without loss of functional status. No study has involved follow–up of this group beyond four years. It is unclear if these patients have a sustained response or if we are simply delaying heart failure decompensation. The aim of this study was to define clinical and echocardiographic characteristics in these patients to determine prognostic outlook.
Methods: 29 patients had CRT at our centre before September 2001. Survivors were invited for review. Data collected included New York Heart Association (NYHA) functional class, electrocardiogram, renal function, haemoglobin and echocardiographic assessment of left ventricular size and function. These were compared to preimplant values. In addition, pulsed wave tissue Doppler imaging was carried out at follow up to observe the prevalence of intraventricular (difference in time to peak systolic velocity between basal septal and lateral walls- TsLV/LV) and interventricular (maximal difference in time to peak systolic velocity between the left and right ventricular basal walls- TsLV/RV) dyssynchrony.
Results: 20/21 survivors attended for review. Significant improvements between baseline and follow up were seen in NYHA class (3.1 to 2.0), left ventricular size (end diastolic dimension 67.9 to 58.3 mm, end systolic dimension 58.8 to 48.2 mm), left ventricular ejection fraction (21.0 to 30.8%) and grade of mitral regurgitation (2.1 to 0.8). Serum creatinine and haemoglobin remained stable (129.3 to 122.2 µmol/l and 13.5 to 13.4 g/dl respectively). Mean TsLV/LV was 46.3 ms and TsLV/RV was 62.8 ms.
Conclusions: Survival beyond four years of CRT is associated with sustained improvement in clinical status and echocardiographic reverse remodelling. Renal function and haemoglobin do not deteriorate. Significant myocardial dyssynchrony is not highly prevalent, presumably because it has been corrected. These are all excellent prognostic indicators and confirm CRT as a key therapeutic option for select patients with advanced heart failure.
heart failure; cardiac resynchronization therapy; echocardiography
223 THE LONG-TERM COST-EFFECTIVENESS OF CARDIAC RESYNCHRONISATION THERAPY WITH OR WITHOUT AN IMPLANTABLE CARDIOVERTER-DEFIBRILLATOR: MODEL BASED ANALYSES BASED ON RESULTS FROM THE CARDIAC RESYNCHRONISATION IN HEART FAILURE TRIAL
G. Yao1, N. Freemantle1, M. Calvert1, J. Cleland2, S. Bryan1.1University of Birmingham, Birmingham, UK; 2University of Hull, Hull, UK
Background: Cardiac resynchronisation therapy (CRT) is an effective treatment for patients with heart failure and cardiac dyssynchrony when moderate or severe symptoms persist despite pharmacological therapy. Addition of an implantable cardioverter-defibrillator (ICD) function may further reduce the risk of sudden death. We assessed the cost-effectiveness of CRT and CRT-ICD compared to medical therapy on incremental cost per life year and quality adjusted life year (QALY) using data from two contemporary clinical trials.
Methods: A Markov model with Monte Carlo simulation to assess costs, life years and QALYs associated with CRT (±ICD) and medical therapy in patients with heart failure and cardiac dyssynchrony was developed, based on a UK healthcare perspective. Model parameter estimates, including NYHA class distribution and transitions, associated health utilities, rates and cause of hospitalisation and death and were estimated from individual patient data from the CARE-HF trial that enrolled patients between January 2001 and March 2003. Patients who were thought to require an ICD according to the then current evidence were excluded from the study. The additional benefit on survival of an ICD was based on results from SCD-HeFT. The base case analysis was based on 100,000 simulations over 6 years.
Results: The incremental cost-effectiveness of CRT compared with medical therapy was £4604 (95% CI £4335, to £4890) per life year, and £3955 (95% CI £3768 to £4148) per QALY. The incremental cost-effectiveness of CRT-ICD compared with medical therapy was £15 857 (95% CI £15 389 to £16 349) per life year, and £14 270 (95% CI £13 955 to £14 579) per QALY. Data on the incremental cost-effectiveness of adding an ICD to CRT in patients at different risks of sudden death will be presented.
Conclusions: Long-term treatment with CRT or CRT-ICD appears cost-effective compared to medical therapy. Compared to CRT, CRT-ICD may be cost-effective in patients with an increase in the risk of sudden death.
cardiac resynchronisation therapy; cost effectiveness; implantable cardioverter defibrillator
224 ARE BETA BLOCKERS EFFECTIVE IN ELDERLY PATIENTS WITH HEART FAILURE AND PRESERVED EJECTION FRACTION? RESULTS FROM THE RANDOMISED, MULTINATIONAL SENIORS TRIAL
A. Taneja1, D. Van Veldhuisen2, P. Lechat3, M. Shibata4, A. Cohen-Solal5, P. Poole-Wilson6, M. Flather1.1Royal Brompton Hospital and Imperial College of Science Technology and Medicine, London, UK; 2University Hospital, Groningen, Netherlands; 3Hôpital Pitie-Salpetrière, Paris, France; 4University of Alberta, Edmonton, Canada; 5Hôpital Beaujon, Clichy, France; 6National Heart and Lung Institute, Imperial College of Science Technology and Medicine, London, UK
Background: The benefits of beta blockers in patients with heart failure and reduced left vetricular ejection fraction (LVEF) are well established. These benefits also appear to be present in elderly heart failure patients with reduced LVEF, but there is little evidence in elderly patients with preserved EF (Diastolic heart failure). The SENIORS study showed that nebivolol reduced the composite of all cause mortality or cardiovascular hospital admission (HR 0.86; 95% CI 0.74–0.99: p = 0.04) in 2128 patients with HF >70 years with a median EF of 34% (36% with EF>35%) followed for a mean of 21 months. We explored the influence of age and EF on outcomes in the SENIORS population.
Methods: The group was divided by age (<median ( = 75.2 yrs) v Greater or equal to median) and ejection fraction (less or equal 35% v >35%). We explored treatment effects on time to first event in these subgroups for the primary outcome (death/CV hospitalisation), and all cause mortality, separately.
Results: are shown in the table. Tests for interaction between the subgroups were not significant.
Conclusions: These data suggest that nebivolol reduces the risk of cardiovascular hospitalisation in HF patients irrespective of age or EF, and raises the hypothesis that the main reduction in risk of death is in those with reduced EF. Further analyses of existing trials need to be carried out to explore the interaction of age, ejection fraction and effects of beta-blockers in HF.
Abstract 224
heart failure; beta blocker; elderly patients
225 TREATMENT OF HEART FAILURE WITH A NORMAL EJECTION FRACTION: THE EFFECT OF DIURETICS WITH IRBESARTAN OR RAMIPRIL ON QUALITY OF LIFE, EXERCISE AND DOPPLER-ECHOCARDIOGRAPHY PARAMETERS
J. Sanderson1, M. Wang2, T. Wang2, G. Yip2, Y. Zhang2, J. Fung2, C. Lau3, M. Tang3, C. Yu4.1Keele University Medical School and University Hospital of North Staffordshire, Stoke-on-Trent, UK; 2The Chinese University of Hong Kong, Hong Kong; 3Queen Mary Hospital, Hong Kong; 4The Chinese University of Hong Kong
Background: Approximately 40–50% of patients with heart failure have a LV ejection fraction >45%. There are few clinical trials on the effect of treatment on quality of life and exercise capacity in this mainly elderly group of patients. This study addressed this question.
Methods: 150 patients with a clinical history of heart failure and a chest X-ray demonstrating pulmonary congestion, LVEF> 45%, and on therapy with diuretics only for >14 days prior to the screening visit were recruited. Patients were randomly allocated to one of 3 treatments: (1) continue with diuretics alone, (2) diuretics plus irbesartan, or (3) diuretic plus ramipril.
Results: There were no differences at baseline between the 3 groups and the average age was 74 years. At 52 weeks quality of life score significantly improved to the same degree in all 3 groups (46%, 51%, and 50% respectively, all p<0.01), the majority of the improvement taking place by 12 weeks. However, exercise duration increased only slightly (average +3–6%). Peak early diastolic and systolic mitral annular velocities increased significantly more with both irbesartan and ramipril than diuretic alone, and LA dimension and LV mass were significantly reduced by the irbesartan and diuretic combination. There were no changes in LV dimensions or LVEF in any group.
Conclusions: In this typically elderly group of HF patients with normal LVEF, diuretic based therapy significantly improved quality of life. However, all treatments had only a marginal effect on exercise capacity. However, both irbesartan and ramipril in combination with diuretics improved Doppler-echo parameters of diastolic and systolic dysfunction more than diuretics alone.
heart failure; diastolic; treatment
226 THE ADDITION OF SPIRONOLACTONE TO AN ANGIOTENSIN RECEPTOR BLOCKER INDUCES REVERSE LEFT VENTRICULAR REMODELLING IN CHRONIC HEART FAILURE
J. Sanderson1, A. Chan2, T. Wang2, M. Wang2, Y. Zhang2, Y. Lam2, L. Yeung2, W. Lam2, C. Yu2.1Keele University Medical School and University Hospital of North Staffordshire, Stoke-on-Trent, UK; 2The Chinese University of Hong Kong, Shatin, Hong Kong
Background: Additional blockade of aldosterone receptors by spironolactone, in conjunction with standard therapy of angiotensin converting enzyme (ACE) inhibitor, substantially improves clinical outcomes among patients with severe heart failure. Angiotensin receptor blockers (ARB) might offer more ‘complete’ renin-angiotensin-aldosterone inhibition and sustained inhibition of aldosterone has been claimed. However, the incremental value of aldosterone blockade in heart failure patients taking ARB has not been assessed.
Methods: In this double blind placebo-controlled study, we enrolled heart failure patients with left ventricular ejection fraction (LVEF) <40% who were being treated on ACE inhibitors for more than 6 months. The patients were randomly assigned to replace ACE inhibitors with candesartan 8 mg daily alone (C group, n = 25) or candesartan 8 mg daily plus spironolactone 25 mg daily (C+S group, n = 24) in a double blind manner. The primary end points were changes in LV volume index, LVEF, LV mass index measured by cardiac magnetic resonance imaging (CMR). Serial CMRs were performed at baseline, 6, and 12 months after randomisation.
Results: The baseline demographic data were comparable between the two groups. The combination C+S group showed significant improvement in LVEF (28% at baseline vs 37% at 12 months, p<0.01, Table 1), reduction of LV end-diastolic volume index (147 (SD 15) ml/m2 at baseline v 120 (16) ml/m2 at 12 months., p = 0.001) and end-systolic volume index (112 (15) ml/m2 at baseline v 86 (17) ml/m2 at 12 months, p<0.0005) and LV mass index (91 (6) g/m2 at baseline v 80 (7) g/m2 at 12 months, p = 0.002) by serial CMR, despite equivalent reduction in blood pressure among the 2 treatment groups. Significant changes in LVEF and volumes were seen at 6 months. In the C group there were smaller nonsignificant changes between baseline and 12 months.
Conclusion: The addition of spironolactone to an ARB has important beneficial effects on LV remodelling in patients with chronic systolic heart failure.
heart failure; spironolactone; candesartan
227 THE SARCOLEMMAL CALCIUM PUMP MODULATES CALCINEURIN MEDIATED CARDIOMYOCYTE HYPERTROPHY
M. Buch1, A. Maass2, A. Pickard1, S. Gillies1, A. Armesilla1, L. Neyses1.1The University of Manchester, Manchester, UK; 2University of Wuerzburg, Wuerzburg, Germany
Background: The calcineurin/nuclear factor of activated T-cell (NFAT) pathway is a central regulator of pathologic cardiac hypertrophy. Calcineurin is a calcium/calmodulin dependent phosphatase and a number of calcium control hypotheses to explain the regulation of calcineurin activity in cardiac cells have been proposed. Calcium transporters in the cardiac myocyte are recognised for their fundamental role in the excitation-contraction process; however whether they may also subserve the vital role of intracellular calcium in cardiac growth and hypertrophy has not been fully evaluated. The sarcolemmal calcium pump (PMCA: plasma membrane calcium/calmodulin ATPase) is not regarded as being directly involved in the excitation-contraction coupling process. Emerging evidence suggests a role for PMCA as modulator of signal transduction pathways. We have recently published findings demonstrating a novel interaction in mammalian cells between PMCA4b, an isoform known to be expressed in the heart, and calcineurin; with consequent inhibitory effect on calcineurin activity.
Aim: To examine the relevance of the interaction between calcineurin and PMCA in rat neonatal cardiomyocytes (RNCM).
Methods: Interaction between endogenous calcineurin and PMCA was demonstrated by immunoprecipitation and western blot analysis. An adenovirus encoding human PMCA4b was used to over-express PMCA4b, confirmed by immunofluorescence studies and western blot analysis. The functional significance of this interaction was examined by stimulating RNCM with phenylephrine and observing the effect of over-expressed PMCA4b on calcineurin phosphatase activity, protein synthesis and ANP transcriptional activity.
Results: The relevance of this interaction was confirmed by demonstrating the interaction between endogenous calcineurin and PMCA in RNCM. Adenoviral infection was shown to successfully result in over-expression of PMCA4b. In RNCM stimulated with phenylephrine, PMCA4b significantly inhibited calcineurin activity in a dose-dependent manner (p<0.05). Furthermore, phenylephrine mediated cardiomyocyte hypertrophy was markedly attenuated by PMCA4b as evidenced by the significant reduction in protein synthesis (p<0.05) and ANP transcriptional activity (p<0.05).
Conclusion: This study yields an unexpected finding in PMCA as a potential modulator of the calcineurin/NFAT signalling process in cardiomyocyte hypertrophy. Moreover, it generates a novel hypothesis for the calcium control mechanism that regulates calcineurin activity in the heart; and identifies a potentially new therapeutic target of interest in heart failure.
cardiac hypertrophy; signal transduction; calcineurin/NFAT
228 MYOCARDIAL PRODUCTION OF REACTIVE OXYGEN SPECIES AND THE NEGATIVE INOTROPIC EFFECT OF β3-ADRENERGIC RECEPTOR STIMULATION IN NNOS−/− MICE
W. Idigo, Y. Zhang, M. Zhang, B. Casadei.University of Oxford, Oxford, UK
Stimulation of cardiac β3-adrenergic receptors (AR) produces a negative inotropic effect which depends on the production of nitric oxide (NO) by the endothelial isoform of NO synthase (eNOS). Recent evidence suggests that increased superoxide production by xanthine oxidoreductase (XOR) may decrease bioavailability of eNOS-derived NO in the myocardium of mice with selective disruption of the gene encoding for the neuronal isoform of NO synthase (nNOS−/− mice). To test the functional relevance of these findings, we compared the inotropic and [Ca2+]i transient response to β3-AR stimulation (with BRL-37344, 10 uM in conjunction with the β1/β2-AR blocker, nadolol, 10 uM) in LV myocytes from eNOS−/− and nNOS−/− mice and their respective wild type littermates (WT).
β3-AR stimulation caused a significant reduction in cell shortening in WT myocytes (4.8 (SD 0.2)% v 5.3 (0.2)% in basal conditions, p<0.01, n = 34) but not in eNOS−/− myocytes. Interestingly, the negative inotropic effect of β3-AR stimulation was also abolished in nNOS−/− mice (5.9 (0.2)% v. 6.1 (0.2)% in basal conditions, p = 0.12, n = 64), despite a 2-fold increase in β3-AR protein expression and no change in eNOS protein level in the nNOS−/− myocardium (4 hearts/group). Consistent with these results, β3-AR stimulation significantly decreased the amplitude of [Ca2+]i transients in nNOS+/+ myocytes (F365/F380: 0.52 (0.050) v 0.59 (0.037) in basal conditions, p = 0.02, n = 18) but not in nNOS−/− myocytes (0.64 (0.052) v 0.64 (0.046) in basal conditions, P = 0.76, n = 12). Inhibition of XOR by 100ìM oxypurinol restored the negative inotropic effect of β3-AR stimulation in nNOS−/− mice (mean 5.8 (0.4)% v 6.5 (0.4)% in control, p<0.01, n = 11).
Our data suggest that increased superoxide production by XOR in the LV myocardium of nNOS−/− mice abolishes the eNOS-dependent negative inotropic effects of β3-AR stimulation, presumably by scavenging eNOS-derived NO. These findings suggest that aspects of the myocardial functional phenotype of nNOS−/− mice may result from inhibition of eNOS-mediated effects.
beta-adrenergic; nitric oxide; superoxide
229 ERYTHROPOIETIN MEDIATED PROTECTION AGAINST ISCHAEMIA/REPERFUSION INJURY IN THE HUMAN HEART IS VIA PHOSPHATIDYLINOSITOL-3-KINASE ACTIVATION
N. Mudalagiri, D. Yellon.Hatter Institute, University College London, London, UK
Introduction: Erythropoietin (EPO), a cytokine produced by the kidneys, has in many animal studies demonstrated its cardioprotective phenotype. Protection has been linked to activation of phosphatidylinositol-3-kinase (PI3K) in the animal setting. However, to date this has not been shown in human myocardium. We hypothesised that EPO mediated cardioprotection could also be demonstrated in human myocardium and employed an experimental model to delineate the cardioprotective mechanism involved.
Methods: Isolated human atrial trabeculae removed from patients undergoing cardiac bypass surgery were suspended in an organ bath and exposed to 90 minutes of hypoxia followed by 120 minutes of reoxygenation. The influence of EPO (50 ng/ml) administered throughout reperfusion following simulated ischaemia was examined. Cardiac function was assessed by measuring the developed force of contraction which was calculated as a percentage of the baseline force of contraction.
Results: EPO significantly improved developed force of contraction when administered at reperfusion (46.72% (SD 1.74) v 30.22% (2.19) for control, p<0.001). The cardioprotective effects of EPO were abrogated by the use of a PI3K inhibitor LY294002 (29.41% (2.47) v 30.22% (2.19) for control). EPO administration at reperfusion offered a similar degree of protection to that observed with preconditioning (46.72% (1.74) v 51.17% (1.35) for preconditioning).
Conclusions: Our data demonstrate for the first time that EPO administered at reperfusion protects the human myocardium via the PI3K dependant pathway. The protection offered is similar in magnitude to that seen with preconditioning. This data therefore, supports the use of EPO as a novel cardioprotective strategy when used alone or as an adjunct in the clinical setting alongside existing reperfusion therapies.
erythropoietin; phosphatidylinositol-3-kinase; reperfusion
230 CONTRIBUTION OF A NOX2 NADPH OXIDASE TO POST-MYOCARDIAL INFARCTION CARDIAC REMODELLING
Y. Looi, D. Grieve, A. Siva, S. Walker, N. Anilkumar, A. Cave, M. Marber, A. Shah.King’s College London, London, UK
Background: Reactive oxygen species (ROS) are implicated in the processes underlying cardiac remodelling. NADPH oxidases are important ROS sources and both Nox2 and Nox4 oxidase are found in cardiomyocytes. Recent studies showed an important role for Nox2 in cardiac fibrosis. Here, we studied the role of Nox2 in adverse cardiac remodelling after myocardial infarction (MI).
Methods: Adult female mice lacking Nox2 (KO) and wild-type littermates (WT) aged 8–12 weeks underwent coronary artery ligation or sham surgery. 4 weeks later, left ventricular (LV) dimensions were studied by echocardiography and haemodynamics by LV catheterisation with a 1.4F Millar catheter.
Results: Infarct size measured 24h post-MI (triphenyltetrazolium staining) was similar in a cohort of WT and KO mice (45 (SD 2) v 49 (2)%; p = NS). After MI, KO mice had significantly less LV dilatation and better preserved LV function than WT (eg, ejection fraction 41.6 (3.7)% v 32.9 (3.2)%, p<0.05). Similarly, in vivo assessment indicated better preserved LV systolic and diastolic function in KO compared to WT mice after MI (eg, LVdP/dtmax 7969 (385) v 5746 (234), p<0.05). The increase in heart/body weight ratio after MI was significantly greater in WT compared to KO, as was the increase in myocyte cross-sectional area. Histological interstitial fibrosis (picrosirius red staining) was attenuated in KO mice after MI (5.0 (0.4)% to 13.5 (1.0)% in WT compared 5.1 (0.3)% to 8.8 (0.9)% in KO; p<0.05). Atrial natriuretic factor mRNA (real-time RT-PCR) was increased significantly more in WT versus KO MI (1389 (233) v 427 (97)%; p<0.05) as was procollagen IαI mRNA (443 (70)% v 146 (18)%; p<0.05). Myocardial MMP-2 activity (gelatin zymography) was significantly increased after MI in WT but not in KO mice. Myocardial Nox2 mRNA expression was unregulated in WT but was undetected in KO mice. Interestingly, Nox4 mRNA expression was unregulated to a similar extent in both KO and WT mice post-MI. Correspondingly, total myocardial NADPH oxidase activity (lucigenin chemiluminescence) also increased in both KO and WT mice groups post-MI.
Conclusions: These results indicate that a Nox2-containing NADPH oxidase contributes significantly to the processes underlying adverse cardiac remodelling and contractile dysfunction post-MI. These effects are specific for Nox2 since Nox4 oxidase was unregulated to a similar extent in both WT and KO groups after MI.
Supported by the British Heart Foundation
NADPH oxidase; reactive oxygen species; cardiac remodelling
231 DOES DIETING AFFECT CARDIAC HIGH-ENERGY PHOSPHATE METABOLISM AND CARDIAC FUNCTION? EFFECTS OF TWO WEEKS OF A HIGH-FAT, LOW-CARBOHYDRATE DIET IN HEALTHY SUBJECTS
M. Scheuermann-Freestone1, D. Tyler2, J. Francis1, G. Watson2, E. Twerdahl2, P. Robbins2, S. Neubauer1, K. Clarke2.1OCMR, John Radcliffe Hospital, Oxford, UK; 2Department of Physiology, Oxford, UK
Introduction: Reductions in myocardial high-energy phosphate metabolism predict mortality and are associated with increased concentrations of circulating free fatty acids (FFA) in patients with heart failure. We hypothesised that increased FFA concentrations, caused by a high-fat, high-protein, low-carbohydrate (Atkins) diet, may alter cardiac energy metabolism in healthy subjects and may affect cardiac function.
Methods: We assessed fasting circulating metabolites and cardiac high-energy phosphate metabolism (phosphocreatine PCr/ATP ratios) and function using magnetic resonance spectroscopy (MRS) and imaging, respectively, in 19 healthy subjects before and after two weeks on a high-fat, low-carbohydrate diet and two weeks after returning to their normal diet. In addition, circulating metabolites, cardiac PCr/ATP and respiratory quotient (RQ) were measured daily in a subgroup of 6 subjects for the first week of diet.
Results: Two weeks of the diet resulted in 3.2 (SD 0.5) kg (4%) weight loss and a 1.9-fold increase in fasting plasma FFA concentrations from 0.41 (0.04) v 0.77 (0.12) mmol/l (p<0.01). Cardiac PCr/ATP decreased from 2.34 (0.07) v 2.01 (0.20) (p<0.05) after the first day of the diet and remained low throughout the diet. In addition, the reduction in PCr/ATP was accompanied by a significant decrease in RQ and correlated negatively with plasma FFA concentrations (r = −0.33, p<0.05). Left ventricular peak filling rate decreased from 90 (6) v 75 (4) ml/s (p<0.01) after two weeks of diet, indicating diastolic dysfunction, and correlated positively with cardiac PCr/ATP. All metabolic and functional effects reversed after returning to a normal diet for two weeks.
Conclusion: A high-fat, low-carbohydrate diet increased plasma FFA concentrations, impaired cardiac high-energy phosphate metabolism and caused diastolic dysfunction within two weeks, suggesting that such a diet may have long-term detrimental effects on the heart.
cardiac energy metabolism; free fatty acids; diet
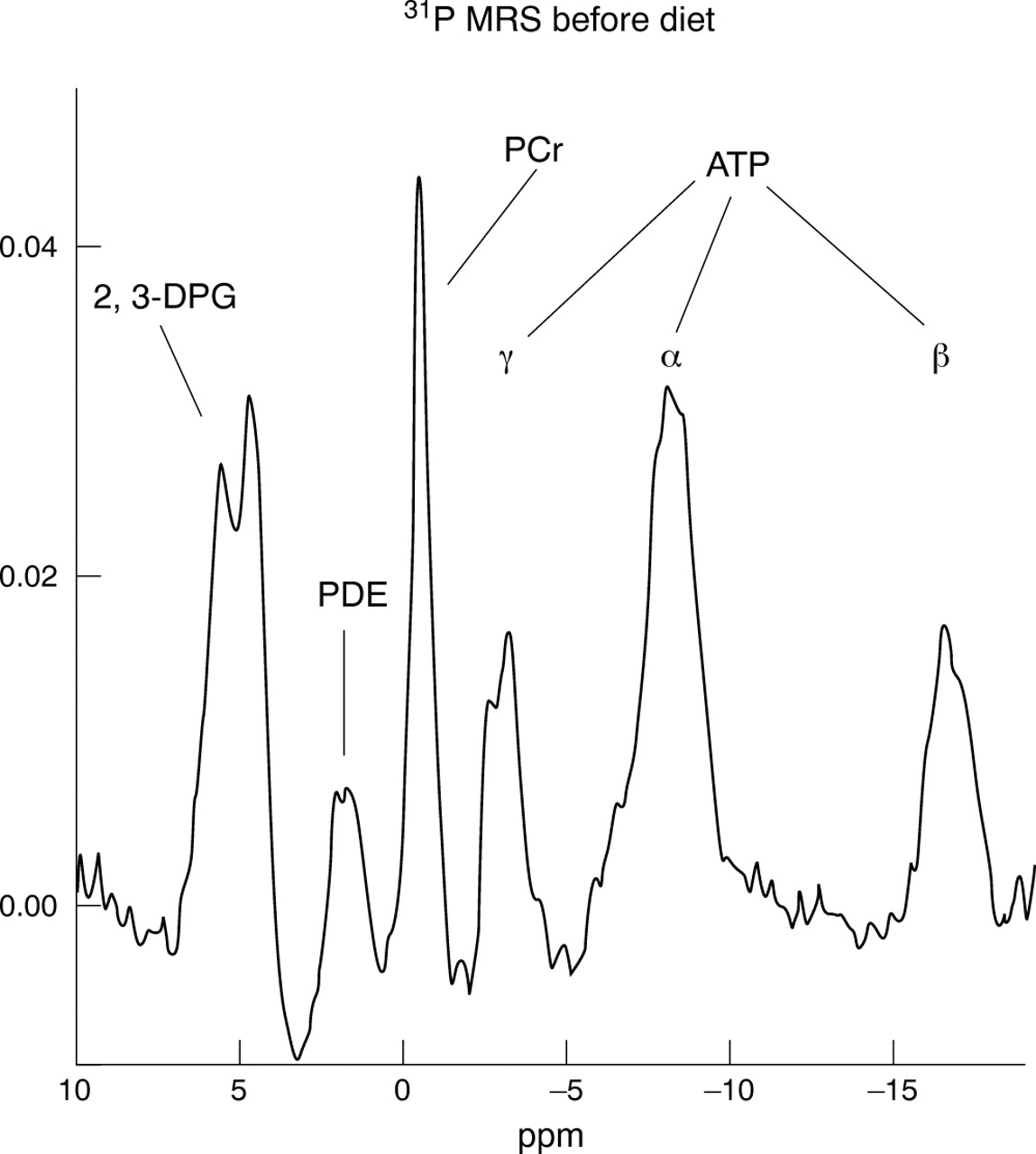
Abstract 231
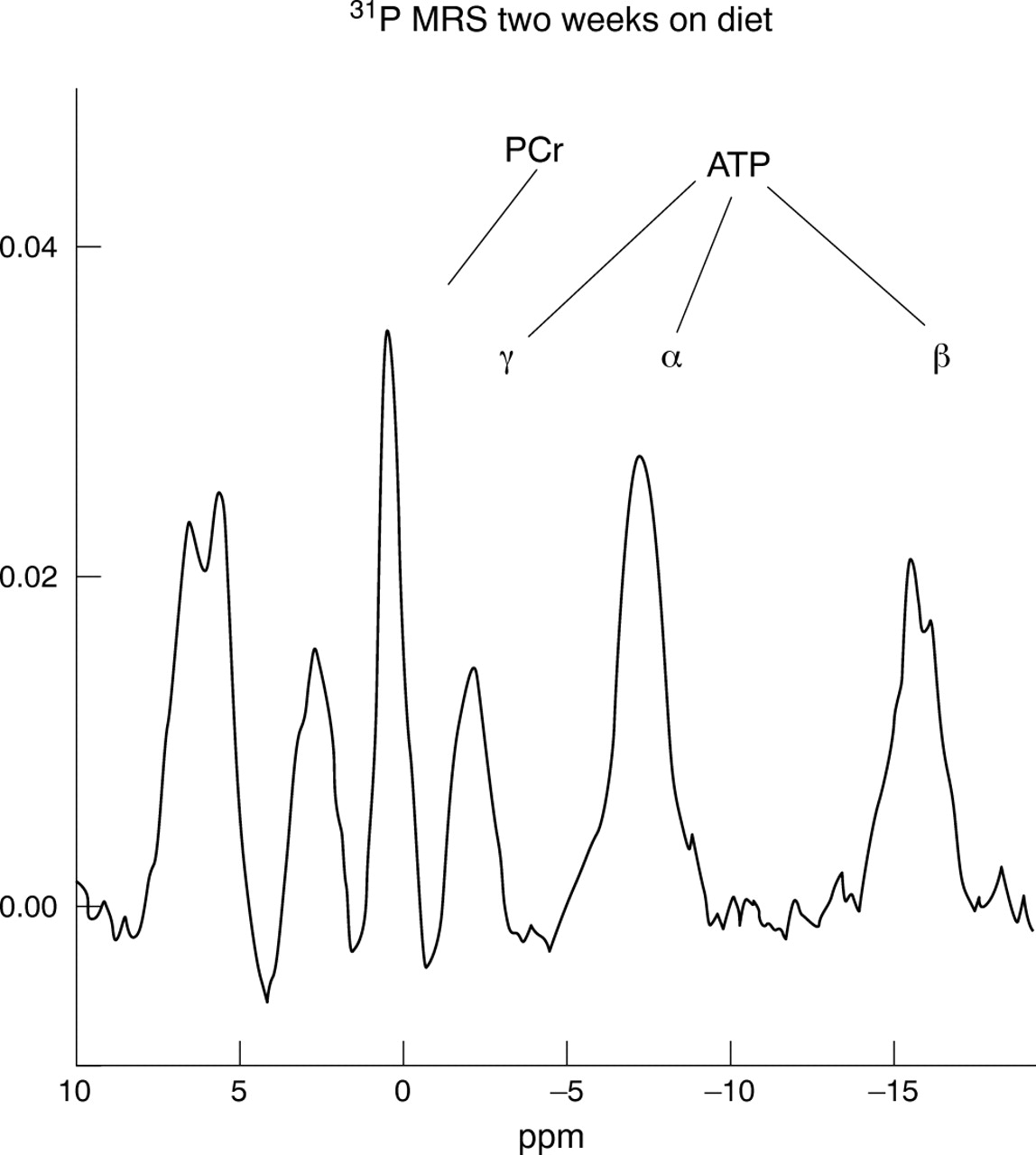
Abstract 231
232 BONE MARROW DERIVED MULTI-POTENT PROGENITOR CELLS AUGMENT PERFUSION OF ISCHAEMIC TISSUES VIA PARACRINE MECHANISMS RATHER THAN BY ENDOTHELIAL DIFFERENTIATION
C. Graham1, S. Hong1, A. Mathur2, M. Boehm1, A. Wragg1.1NHLBI/NIH, Bethesda, US; 2Barts and the London, London, UK
Recent studies have suggested that injection of bone marrow derived cells can improve perfusion and function of ischaemic tissues. Clinical studies are already underway. The optimal cell type and method for processing cells has not yet been established. Rare fractions of bone marrow cells have been identified that may be able to differentiate into cells of all three germ lineages, such as the multi-potent adult progenitor cells (MAPC). These multi-potent progenitor cells may prove useful for the treatment of chronic ischaemic conditions.
We isolated multi-potent progenitor cells (rMPCs) from rat bone marrow. rMPCs were cultured at low density in media previously used for the isolation of MAPC. rMPCs proliferated without obvious senescence for >220 population doublings with a stable phenotype, karyotype and maintained telomere length. rMPC were negative for CD45 and MHC Class II expression and positive for CD44, CD90 and MHC Class I. rMPC did not express Oct4 by PCR. rMPC exhibit a potential for differentiation into cells of all three germ layers in vitro. After endothelial, hepatocyte or neuronal differentiation, tissue specific antigens were up regulated as measured by RT PCR and immuno fluorescence (NSE, nestin and NF200 were induced after neuron, albumin and CK18 after hepatocyte and Dil LDL uptake and RECA1 staining after endothelial differentiation). In addition rMPC secreted multiple cytokines related to inflammation and angiogenesis including MCP1, SDF1, FGFb and VEGF.
We investigated whether perfusion and function of an ischaemic hind limb could be restored by transplantation of rMPC. Syngeneic rMPC were injected into ischaemic hind limbs of rats. rMPC engrafted into the adventitia of arterioles of ischaemic muscles in large numbers although rMPC did not engraft into normally perfused muscles. Engrafted cells did not appear to differentiate into an endothelial or smooth muscle phenotype as assessed by von Willebrand factor and smooth muscle actin staining respectively. However, limb perfusion, measured by fluorescent microspheres did increase after rMPC injection, although there was no improvement in limb muscle atrophy (measured by muscle weight) and limb function assessed by treadmill running distance 4 weeks after cell injection. Cytokine analysis of muscles 5 days after rMPC injection revealed raised levels of cytokines, including the chemokines MCP1 and SDF1, indicating that rMPC continued to be biologically active in vivo after injection.
In summary, although rMPC can express tissue specific antigens from all 3 germ lineages after differentiation in vitro, it appears that the beneficial effects on perfusion are not due to in vivo differentiation and de novo vasculogenesis but are probably due to paracrine mechanisms modulating local inflammatory and angiogenic responses. As rMPC secrete SDF1 in vivo they may increase the homing of resident stem or progenitor cell populations.
multi-potent progenitor cells; ischemia; paracrine
233 DO SIMPLE CLINICAL AND ECHOCARDIOGRAPHIC PARAMETERS PREDICT LONG TERM RESPONSIVENESS TO CARDIAC RESYNCHRONISATION THERAPY? RESULTS FROM THE CARE-HF TRIAL
S. Ghio1, F. Leyva2, N. Freemantle3, A. Serio1, G. Magrinia1, L. Scelsia1, M. Pasottia1, J. Cleland4, L. Tavazzi1.1Division of Cardiology, IRCCS Policlinico S. Matteo, University Hospital, Pavia, Italy; 2Department of Cardiology, Good Hope Hospital, Sutton Coldfield, UK; 3Department of Primary Care and General Practice, University of Birmingham, Birmingham, UK; 4Department of Cardiology, University of Hull, Kingston upon Hull, UK
Background: Refinement of selection criteria for the implantation of biventricular devices is crucial to improve cost-effectiveness of cardiac resynchronisation therapy (CRT). The CARE-HF trial gives the opportunity to verify whether clinical criteria and the interventricular mechanical delay (IVMD), a dyssynchrony parameter easily measurable using conventional Doppler echocardiography, may predict long term responsiveness to CRT.
Methods: Echocardiographic examinations were performed at baseline and at 18 months in 735 patients enrolled in the CARE-HF trial and randomised 1:1 to CRT and control. Echocardiographic recordings were quantitatively analysed in a core laboratory. A long term responder to CRT was defined as a patient who survived and whose end-systolic volume was reduced at the 18 month evaluation by more than twice the standard deviation of inter-observer variability in the core laboratory (40 ml).
Results: According to the above definition, the percentage of long term responders was 49.2% in the CRT group as compared to 18.6% in the control group. In a multivariate model which included age, sex, aetiology of heart failure (ischemic vnon ischemic), systolic blood pressure, end-diastolic and end-systolic volumes, ejection fraction, mitral regurgitation, left ventricular filling pattern, tricuspid annular plane excursion and IVMD, IVMD and etiology were significantly predictive of response (p<0.001). The probability of being a responder increased linearly with the increase in IVMD in both ischemic and non ischemic patients with a fairly smooth slope but it was substantially lower in ischemic patients. For an IVMD of 20, 40 or 60 ms the calculated probability was respectively 52%, 58% and 64% in non ischemic patients and 28%, 33% and 39% in ischemic patients.
Conclusions: In patients with non ischemic aetiology the probability of a positive response to CRT is never zero: low values of IVMD should therefore not be used to negate the benefits of CRT in such patients. In ischemic patients, the probability of being a long term responder is lower and the risk of non response is therefore higher for low values of IVMD.
cardiac resynchronisation; echocardiography; heart failure
234 REPERFUSION IN ACUTE MYOCARDIAL INFARCTION: WHERE ADMINISTERED AND OUTCOME IN 40 000 PATIENTS RR WEST, JS BIRKHEAD, CFM WESTON ON BEHALF OF MINAP STEERING GROUP
R. West1, J. Birkhead2, C. Weston3.1University of Wales College of Medicine, Cardiff, UK; 2Northampton General Hospital, Northampton, UK; 3Singleton Hospital, Swansea, UK
Background: Analysis of pooled data from large randomised trials has shown benefit of early over late thrombolysis in acute myocardial infarction (MI). These findings have led to practical means of reducing time to thrombolysis, initially ‘door to needle’ time and more recently ‘call to needle’ time.
Objective: To compare 30 day outcome of MI patients, according to where thrombolysis was administered.
Method: Analyse data collected by the myocardial infarction national audit project (MINAP) of patients reperfused, where both location of reperfusion and 30 day vital status were known, adjusting for principal potential confounders (age, sex, past medical history).
Results: In 2003–4 MINAP recorded in England and Wales some 40 000 reperfused MI patients, for whom both location of reperfusion (before admission, A and E, CCU direct, CCU indirect and elsewhere in hospital) and 30 day vital status were known. Median times from onset to reperfusion were 98, 157, 157, 288 and 232 minutes respectively. Median times from call to reperfusion were 40, 69, 73, 156 and 103 minutes respectively. Thirty day mortality, 4.6, 9.9, 10.8, 15.8 and 14.4% respectively, was very highly correlated with both time from call to reperfusion (R2 = 0.895) and onset to reperfusion (R2 = 0.936). Multivariate analysis showed that highly significant differences in 30 day mortality between all locations, except ‘CCU indirect’ and ‘elsewhere in hospital’, were maintained after adjustment for age (five year age groups), sex and previous medical history (MI, hypertension, hypercholesterolaemia, angina). Thus, despite case mix differences and in particular conservative inclusion criteria in pre-hospital thrombolysis protocols, early administration appears to be independently associated with improved 30 day outcome.
Conclusion: This large observational study adds further support for the case for early reperfusion and now, since much of the ‘door to needle’ time gain has been achieved with direct admission to CCU or lysis in A and E, for the potential benefits of pre-hospital lysis.
reperfusion; acute myocardial infarction; 30 day mortality
235 ATTAINMENT OF THE OPTIMUM CLINICAL TARGET FOR HYPERTENSION IS MUCH LESS SUCCESSFUL THAN FOR GMS AUDIT TARGETS IN PATIENTS WITH TYPE 2 DIABETES
P. Ambery1, T. McCormack2.1GlaxoSmithKline, Uxbridge, UK; 2Whitby Group Practice, Whitby, UK
Introduction: Studies such as UKPDS, Steno-2 and CARDS have established the benefit of intervention across a range of risk factors in the management of Type 2 diabetes. Here we examine, in a UK wide audit, whether the sentiment of GMS has translated into improved attainment of treatment targets, with specific reference to hypertension.
Methods: Practices were invited to take part in electronic audit of their Type 2 diabetes care. Additional permission was gained for the export of clinical data in anonymised form to an external independent server. Here we present the pooled data for 88 738 Type 2 diabetes patients in England and Wales and 24 242 Scottish patients. Data points are the latest practice data exports between March and October 2005.
Results: 58 316 out of 112 980 patients met the optimum BP target for Type 2 diabetes of 140/80 mm Hg (52%) whereas 77 244 met the audit target of <145/85 (68%). Attainment of optimum target was higher for England and Wales v Scotland (54% v 45%). Cholesterol audit target attainment (total cholesterol<5 mmol/l) was 74%, similar for England and Wales and Scotland. Less than 50% of patients with recorded HbA1c achieved optimum target of <7%, whilst around 55% achieved the audit target of <7.4%.
Conclusion: Although the GMS contract has brought great progress in the management of risk factors associated with Type 2 diabetes, some work is still to be done. The established QMAS data used to measure GMS achievement does not measure success in achieving optimum targets. Our study, which does measure optimum target attainment, suggests that audit targets are being met, yet we still have some way to go to meet established treatment goals. Aggressive treatment to target of multiple risk factors in Type 2 diabetes is essential to reduce the burden of future complications.
diabetes; hypertension; hyperlipidaemia
236 HIGH DOSE ALLOPURINOL DRAMATICALLY IMPROVES ENDOTHELIAL DYSFUNCTION MORE THAN CONVENTIONAL DOSES IN CHRONIC HEART FAILURE
J. George, E. Carr, J. Davies, A. Struthers.1University of Dundee Medical School, Dundee, UK
Introduction: Endothelial dysfunction is known to be abnormal in patients with chronic heart failure (CHF).We have previously shown that 300 mg of Allopurinol, a xanthine oxidase inhibitor, improves endothelial dysfunction in chronic heart failure. This has been the conventional dose utilised in most clinical studies of Allopurinol. However, for various reasons, 300 mg/day may not be the optimal dose and hence we investigated whether higher doses were even better.
Methods and results: We performed a randomised, placebo-controlled, double-blind crossover study on 30 patients with New York Heart Association class II–III stable chronic heart failure. We compared placebo v 300 mg Allopurinol v 600 mg Allopurinol. Each treatment phase was one month with a two week washout period between treatment phases. Endothelial function was assessed by forearm venous occlusion plethysmography with an endothelium dependent vasodilator acetylcholine compared with an endothelium-independent vasodilator, sodium nitroprusside. There was a significant step-wise increase in forearm blood flow from placebo to 300 mg Allopurinol and 600 mg (high dose) Allopurinol (percentage change in blood flow [mean±SEM]: 73.96 (SD 10.29)% v 152.10 (18.21)% v 240.31 (38.19)%; p<0.001). There were no significant differences in the forearm blood flow changes between the treatment groups with regard to sodium nitroprusside (p = 0.817). As expected, plasma urate was significantly reduced with increasing doses of Allopurinol [mean±SD]: Placebo 0.41 (0.11) v 300 mg Allopurinol 0.23 (0.05) v 600 mg Allopurinol 0.16 (0.06).
Conclusions: For the first time, we have shown that high-dose (600 mg/day) Allopurinol is significantly more potent than the conventional 300 mg dose in improving endothelial dysfunction in patients with chronic heart failure. Indeed 600 mg Allopurinol improves endothelial function by a much larger margin (using estimated marginal means–143% increase) than has ever been seen by any other treatment. These results suggests that virtually all of the literature on Allopurinol have used suboptimal doses and future studies on Allopurinol should consider using the 600 mg/day dose so that we can fully harness the therapeutic potential of this treatment.
heart failure; allopurinol; endothelial dysfucntion
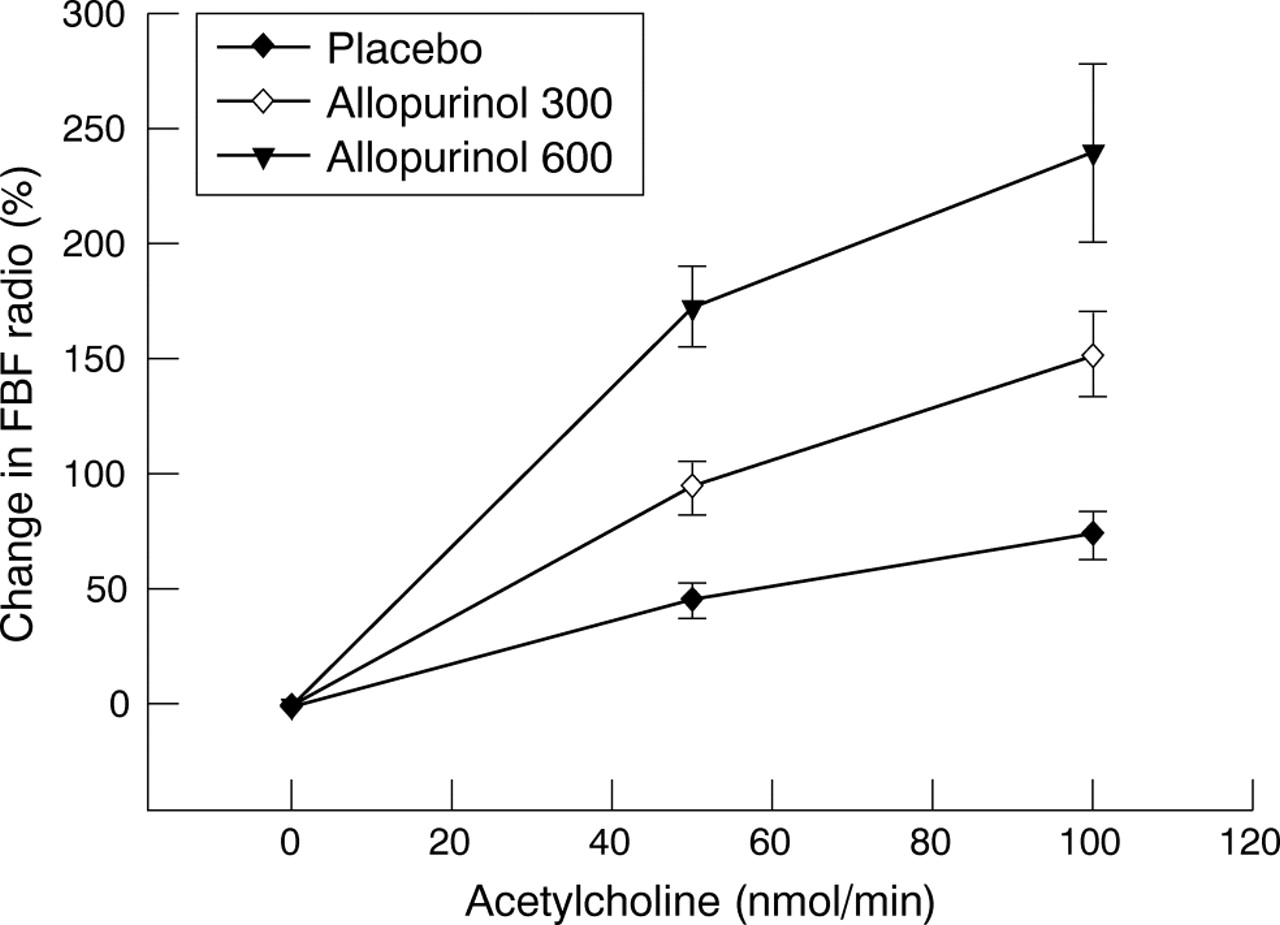
Abstract 236
237 SUPERIOR CLINICAL AND ECONOMIC IMPACT OF STRESS ECHOCARDIOGRAPHY COMPARED TO EXERCISE ELECTROCARDIOGRAPHY IN PATIENTS WITH SUSPECTED ACUTE CORONARY SYNDROME BUT NEGATIVE TROPONIN: A PROSPECTIVE RANDOMISED CONTROLLED STUDY
P. Jeetley1, L. Burden1, B. Stoykova2, R. Senior1.1Northwick Park Hospital, Harrow, UK; 2Health Economics Research Group, Brunel University, Uxbridge, UK
Background: The assessment of patients with coronary risk factors presenting to hospital with cardiac-sounding chest pain, non-diagnostic ECG and negative Troponin is clinically challenging. We hypothesised that stress echocardiography (SE) is more cost-effective and accurate than exercise ECG (ExECG) for the risk stratification of these patients.
Methods: Patients were randomised to either ExECG or SE within 24 hours of admission. Patients with a low post test risk were discharged from hospital. Patients with a high post-test risk were referred to on-call cardiologists. The remaining classified as intermediate post-test risk were managed according to standard hospital protocol. A cost analysis of tests was performed using UK government figures.
Results: Of a total of 433 patients, 215 underwent SE and 218 ExECG. Significantly more patients in the SE group were discharged without further tests compared to ExECG group (77% v 33% p<0.0001) with no difference in cardiac event rates (death, myocardial infarction and revascularisation) at follow-up of 9 (SD 5) months (3% v 5% for ExECG and SE respectively p = ns). SE classified fewer patients as intermediate risk (3% v 39%, p<0.0001) and more patients in the ExECG group v SE required further tests to confirm or refute the diagnosis of CAD (47% v 20% respectively; p<0.001). Patients with high risk studes were more likely to demonstrate normal coronary angiography if they had ExECG as the initial test (39% v 23%). Cardiac events in the SE arm in low, intermediate and high post-test risk groups were 5%, 17% and 51% respectively, compared to 3%, 15% and 29% (p = 0.04 v high risk SE). Cost to investigate for CAD in the SE group was significantly less v ExECG group (£367 v £515 per patient; p<0.0001). The difference was seen in all pre-test TIMI risk groups ie. low (£211 v £446), intermediate (£421 v £511) and high risk (£332 v £690).
Conclusions: In patients presenting to hospital with acute cardiac-sounding chest pain, non-diagnostic ECG and negative troponin, SE resulted in earlier hospital discharge, required fewer further tests and more accurately risk-stratified patients than Ex-ECG which translated into cost-benefit.
cost-effectiveness; echocardiography; coronary artery disease
238 ACHIEVED CRP IS ADDITIVE TO APO B/A I RATIO IN EXPLAINING THE LONG TERM CLINICAL BENEFITS OF HIGH DOSE STATIN THERAPY IN ACS PATIENTS IN THE PROVE IT-TIMI 22 TRIAL
K. Ray1, C. Cannon1, D. Morrow1, R. Cairns2, E. Braunwald1.1Harvard Medical School, Boston, US; 2Nottingham Clinical Research Group, Nottingham, UK
Background and aims: ApoB/AI ratio is believed to be the most sensitive marker of atherogenic dyslipidemia in prospective studies and of statin efficacy in trials using standard doses of statins. We assessed the benefit of reductions in ApoB/AI with pravastatin 40 mg vs atorvastatin 80 mg in ACS patients in PROVE IT-TIMI 22.We postulated that the greater efficacy of intensive therapy on acute events would be explained both by a lower achieved ApoB/AI and CRP.
Methods: Baseline and 4 month ApoB/AI and CRP were available in 3683 and 2998 patients respectively. The acute clinical endpoints of death, myocardial infarction or unstable angina from 4 months to end of study was assessed using the achieved ApoB/AI ratio at 4 months and a cox proportional hazards model that adjusted for known clinical risk predictors.
Results: Baseline apoB/AI (0.84, IQR 0.7–1) fell to 0.67 (IQR 0.6–0.8) with pravastatin 40 mg at 4 months v 0.53 (IQR 0.4–0.6) with atorvastatin 80 mg (p<0.0001). Median CRP at 4 months was also lower with atorvastatin 80 mg 1.3 mg/L v 2.1 pravastatin 40 mg (p<0.0001). The 4 month achieved apoB/AI ratio was an independent predictor of clinical events (HR 1.55, 95% CI 1.04–2.14, p = 0.03). Stratified analysis adjusting for other risk factors (fig 1) suggested that the risk per unit change in apoB/AI differed between statin regimens. The correlation between Apo B/A I and CRP was weak (0.2). After inclusion of CRP in the model Apo B/AI was no longer a significant predictor of clinical events (HR 1.4, 95% CI 0.9–2.18, p = 0.1), but CRP>2 mg/L was significant (HR 1.61, 95% CI 1.22–2.13, p = 0.0008). Irrespective of high or low ApoB/A I ratio, clinical risk could be further discriminated by achieved CRP (Fig 2, adjusted model).
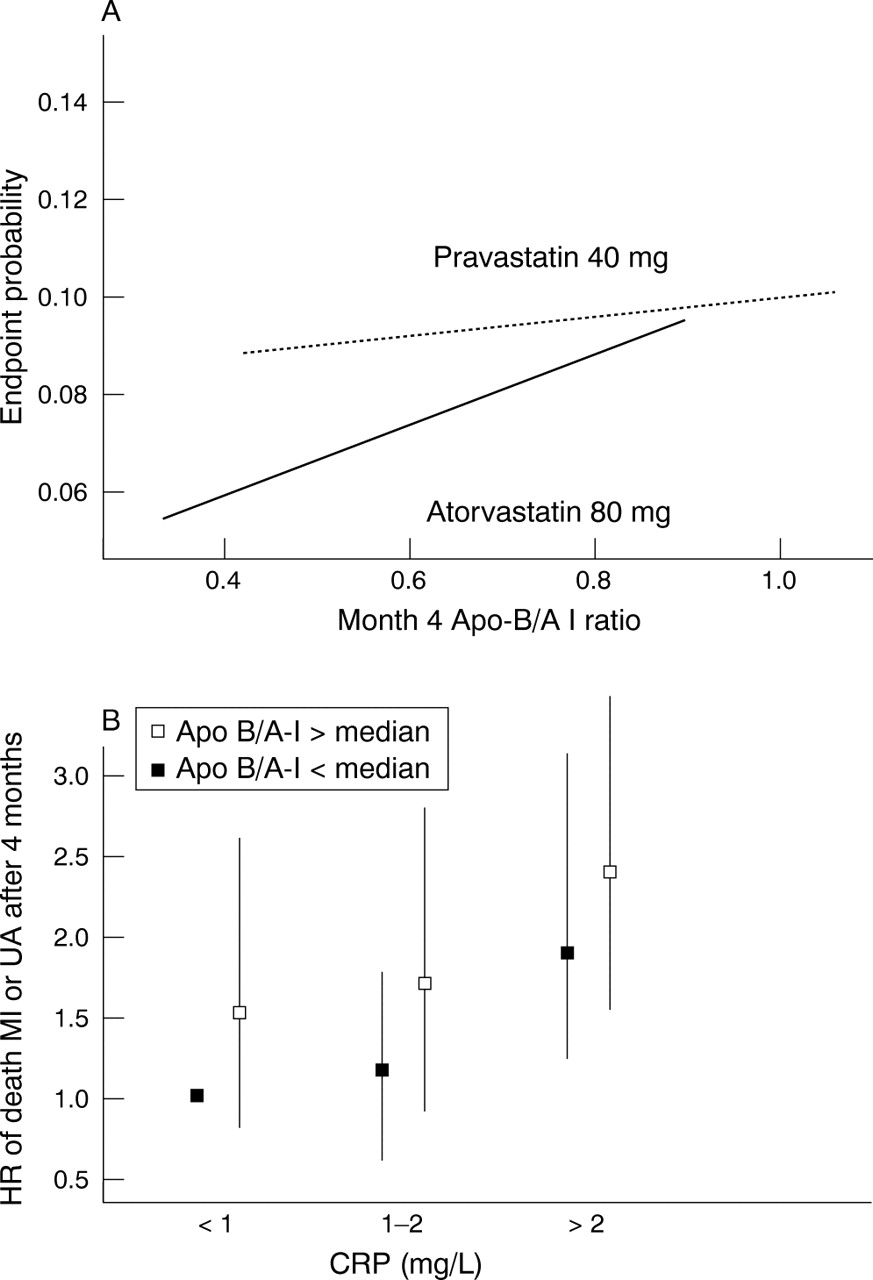
Abstract 238
Conclusion: These data suggest that the long term benefits of intensive statin therapy are not entirely mediated by lipid reduction alone. Reduction in inflammation appears to be at least as important as reduction in lipids in reducing long term events. CRP monitoring in the post ACS patient may be a useful means to further monitor long term risk in ACS patients.
CRP; lipids; statins
239 TRANSTHORACIC CONTRAST ECHOCARDIOGRAPHY IN THE DETECTION OF PATENT FORAMEN OVALE
A. Turley1, J. Thambyrajah1, P. Finn2, A. Griffiths1, M. de Belder1, M. Stewart1.1The James Cook University Hospital, Middlesbrough, UK; 2Teesside University Statistical Department, Middlesbrough, UK
Introduction: A patent foramen ovale (PFO) is a common clinical finding and is becoming increasingly implicated in several important pathophysiological conditions including cryptogenic embolic stroke, migraine with aura, decompression sickness and more rarely acute myocardial infarction. Echocardiographic techniques are the principal means for diagnosis and assessment of a PFO. The development of transthoracic echocardiography (TTE) with harmonic imaging coupled with the use of contrast and provocation testing has potentially enhanced our ability to detect a PFO transthoracically.
Methods: A total of 20 patients with an unexplained embolic event were recruited. We compared four routes of contrast delivery (upper extremity vein in a dependant position, upper extremity vein in an elevated position, right femoral vein and lower extremity vein) with provocation manoeuvres on the detection of PFO using both TTE and transoesohphageal echocardiography (TOE). Route of contrast delivery was performed in a random fashion. Studies were interpreted in real time by an echocardiographer in an unblinded manner as in real-life clinical practice. All studies were digitally recorded and later reviewed independently by a 2nd BSE accredited echocardiographer blinded to the sequence and site of contrast injections.
Results: The mean age of the 20 patients was 24 (SD 10.7) yrs) and 12 (60%) were male. All patients were in sinus rhythm. Six patients (30%) were ex smokers and four (20%) current smokers. Two patients were on treatment for hypertension and five (25%) patients had hyperlipidaemia (Total cholesterol >5 mmol/L). One patient suffered with type 1 diabetes mellitus. The prevalence of PFO detected by the TTE approach combined with a provocation manoeuvre was 50% (10/20). The prevalence in divers was 100% (5/5) and 38% (5/13) in patients with a cryptogenic stroke/TIA. TOE only detected 5/20 (25%) PFO. All PFO detected by TOE were detected by TTE. Valsalva improved the detection rate for all routes of contrast delivery except IV access at the ankle. The highest detection rates were seen with contrast injection in the elevated arm or via the right femoral venous route (10/20). Agreement between reviewers was excellent (p<0.01). All non-agreement observed between TTE and TOE occurred when TTE reported a positive result and TOE a negative. In 9/10 (90%) cases, the clearest image was using TTE with 7/9 (78%) following a provocation manoeuvre. Left ventricular opacification was most marked during femoral vein delivery of contrast agent coupled with valsalva manoeuvre and TTE.
Conclusion: TTE with harmonic imaging and femoral vein delivery of contrast should be regarded as gold standard for the echocardiographic detection of PFO. Maximising contrast lad by use of large ante-cubital vein and arm elevation improves detection if arm injection is used.
PFO; contrast; femoral
240 THE USE AND ABUSE OF TRANSTHORACIC ECHOCARDIOGRAPHY: CAN LESSONS FROM THE ANALOG PAST SHAPE OUR DIGITAL FUTURE?
S. Churchill, D. Colclough, A. Wallis, V. Curnow, E. Rees, A. Ionescu.Morriston NHS Trust, Morriston, UK
Background: Transthoracic echocardiography (TTE) is widely available, portable, versatile, non-invasive, performed by ‘technical’ rather than medical personnel, and thus often perceived as an ‘easy to obtain’ imaging test, with a potential for unnecessary scans being requested. The first step to improve the effectiveness of ECHO is to understand how, by whom, and for what it is used. This information can be used to shape the current transition to a full digital echo lab.
Setting: Echocardiographic laboratory based in regional cardiothoracic centre, and serving also the local multispecialty DGH.
Methods: We analysed TTE scans performed between 31 October 1997–18 May 2005 using our electronic database, and documented user-related parameters to allow us to understand the patterns of use of ECHO, and to plan for the on-going transition to a full digital echo service.
Results: There were 21375 TTE (monthly average 271+72, range 142–475; 55.3% M, age (mean 65.6 (SD 15.0) years). Two thirds of the studies, 8404 (34.6%), were requested by the tertiary cardiologists (CARD), 7302 (30%) by the physicians (MED), 3775 (15.5%) by the secondary cardiology service (S-CARD), 2978 (12.2%) by the cardiac surgeons (CVS), and 1452 (6%) by the general surgeons (SURG); in 412 (1.7%) studies the specialty of the user was not documented. Overall yearly workload doubled between the first and the last full calendar years, with the sharpest increase in requests from SURG. Only 3504 (14.4%) scans were performed outside the department (mainly at the bedside). Six indications accounted for more than 2/3 of the requests: 12946 (53.2%) for the assessment of LV function; 1439 (5.9%) for embolic source, 1336 (5.5%) for aortic stenosis, 1209 (5.0%) for assessment of pericardial pathology, 907 (3.7%) for infective endocarditis, and 822 (3.4%) for mitral regurgitation. The average number of scans per patient was 2.4 (2.3) range 1–24. Assessment of LV function, pericardial effusion and infective endocarditis had the highest proportion of repeated scans. CVS requested on average 3.5 (2.6), S-CARD 2.7 (2.2), CARD 2.6 (2.6), MED 1.7 (1.5), Surg 1.5 (1.2) scans/patient (p<0.05 for all inter-group comparisons).
Conclusions: Devising a strategy to limit the duration of scans performed for the assessment of left ventricular function would substantially increase the throughput of patients in the department. The referral process to echocardiography should be tightened up to avoid ‘routine’ repeat echocardiograms. Reasons for the sharp increase in requests for echo from the general surgeons should be examined.
transthoracic echocardiography; audit; service provision
241 EVALUATION OF CARDIAC FUNCTION AND MORPHOLOGY DURING MYOCARDIAL CONTRAST ECHOCARDIOGRAPHY WITH CARDIOSPHERE IN ANESTHETISED DOGS
J. Goldman, U. del Balzo, T. Ottoboni.POINT Biomedical Corp, San Carlos, US
Background: The purpose of this study was to determine whether electrocardiographic and systemic hemodynamic changes or microvascular damage occur in anesthetised dogs with CARDIOsphere (PB127) administered during myocardial contrast echocardiography (MCE).
Methods: CARDIOsphere was administered intravenously (150 ml/hr) in anesthetised closed-chest dogs (table). Harmonic Power Doppler MCE was performed using the Philips M2424A ultrasound system (triggering in diastole once every 4 beats). Each dog was exposed to ∼1,000 triggers and MCE duration varied (25–45 minutes) depending on basal heart rate. The heart was imaged in a parasternal short axis view using a custom transducer mount to hold the imaging plane. In all groups, one or more MCE settings exaggerated the conditions used in CARDIOsphere Phase 3 clinical trial: dose ∼10X (actual 0.175 mg/kg/hr), power ∼40% higher (actual MI⩽1.0) and exposure ∼5X longer (actual 200 triggers/imaging plane).
Abstract 241
Hemodynamics and ECG (including QT/QTc, conduction disturbances and PVC) were continuously monitored and analysed. Blood samples were collected for clinical chemistry and troponin I/T levels (baseline, 1 and 7 days post dosing). Macroscopic and histopathological evaluation of the lung, liver and heart was performed at 24 hrs (n = 3 in each Group) and 14 days post dosing (n = 2 Group 1 and n = 3 Group 5).
Results: There were no treatment-related changes in cardiovascular and ECG parameters, or troponin levels. There were no clinical pathology findings. None of the dogs had microscopic evidence of inflammation, myocyte loss, necrosis or thrombosis. Mild and reversible morphological changes in the heart were seen only when all MCE settings were exaggerated beyond conditions used in clinical trials (group 5). At 24 hrs post-dosing, areas of minimal red discoloration corresponding to subepicardial and subendocardial red blood cells extravasation were observed that resolved after the 14-day recovery period.
Conclusion: In this model, exaggerated exposure to MCE performed with CARDIOsphere at the clinical dose with MI⩽1.2 or at a dose multiple of 10X with MI⩽1 did not cause any changes in cardiac function, ECG abnormalities or microvascular damage.
contrast echocardiography; safety; triggered imaging
242 REAL-TIME 3D COLOUR DOPPLER QUANTIFICATION OF AORTIC REGURGITATION-OBJECTIVE, FEASIBLE AND SIMPLE
E. Ho, S. Kapetanakis, S. Turner, M. Monaghan.Dept of Cardiology, King’s College Hospital, London, UK
Background: Current 2D echocardiographic methods of aortic regurgitation (AR) quantification yield variable results, being subject to geometric assumptions and haemodynamic factors. Real-time 3D colour Doppler captures in a single dataset the entire flow velocity profile of the region of interest in three dimensions. Having previously validated flow quantification using real-time 3D colour Doppler, we assessed its applicability to AR quantification.
Methods: 59 consecutive, unselected patients with AR of varying severity underwent 2D and 3D colour Doppler imaging at the level of the aortic valve, and left ventricular inflow and outflow tracts. 2D echocardiographic qualitative grading of AR severity was done on a 4-point scale by an experienced observer and quantified using jet height/left ventricular outflow tract (LVOT) height ratio, vena contracta width and pressure half-time measurements. 3D datasets were acquired from the apical window and viewed with mip-map rendering to allow qualitative assessment of the regurgitant jets without tissue cropping (fig 1).

Abstract 242
3D colour Doppler flow quantification of AR, expressed as the regurgitant fraction derived from LVOT and mitral stroke volumes, was performed offline using dedicated software.
Results: Adequate 2D and 3D colour Doppler images were obtained from all patients. Correlation between 2D and 3D imaging qualitative assessment of AR severity was good (weighted kappa = 0.96). Aortic regurgitation quantification was well correlated between the 3D colour Doppler and VC width (r = 0.8, p<0.0001, n = 46) and JH/LVOT height (r = 0.94, p<0.0001, n = 52, mean difference −0.6% (SD 11.3)%) although eccentric jets tended to be underestimated by 2D analysis. Acquisition and analysis for 3D datasets took just under 5 minutes. Real-time 3D-derived AR regurgitant fraction reliably differentiates between the grades of AR severity derived from multiple 2D Doppler parameters (fig 2, one-way ANOVA and post-hoc analysis p<0.0001 for all groups).

Abstract 242
Conclusion: 3D colour Doppler provides a simple, objective quantification of aortic regurgitation, particularly in the presence of eccentrically directed jets, which are not easily amenable to 2D analysis. It represents a single measurement, requiring minimal acquisition and analysis time, providing similar information provided by time-consuming multiple 2D measurements.
real-time 3D echocardiography; aortic regurgitation; flow quantification
243 A NOVEL METHOD TO IDENTIFY DYSSYNCHRONOUS CONTRACTION THROUGH REGIONAL TIME DIFFERENCES IN PEAK STRAIN AND STRAIN RATE
N. Artis1, D. Oxborough2, K. George3, R. Shave4, T. Cable3, E. Dawson5, G. Williams2, C. Pepper2, L. Tan2.1University of Leeds, Leeds, UK; 2Leeds General Infirmary, Leeds, UK; 3John Moores University, Liverpool, UK; 4Brunel University, London, UK; 5Copenhagen Muscle Research Centre, Copenhagen, Denmark
Introduction: 2D Strain imaging using speckle-tracking is a new method which enables simultaneous analysis of myocardial strain in both the radial and circumferential dimensions. The time-to-peak 2D strain and strain-rate of left ventricular segments using this technique have not been reported. We compared the values and patterns obtained from a cohort of patients with LV dysfunction (LVD) v healthy controls.
Methods: Thirty-two subjects with no known history of cardiac disease and 12 subjects with LVD (LVEF<35%) were assessed. Images were acquired using a Vivid 7 (GE Vingmed) ultrasound system and analysed offline using dedicated 2-D strain software. A parasternal short-axis view at papillary muscle level was used to assess circumferential and radial strain. The time from Q wave of the ECG to peak strain, and both systolic (SRs’) and diastolic (SRe’) strain rates were measured in six segments of the LV (septal, lateral, inferior, anterior, anteroseptum and posterior segments).
Results: Myocardial contractions were highly synchronous in all segments in healthy controls as shown by low scatter of data points of peak strain, SRs’ and SRe’, unlike the marked scatter indicative of dyssynchrony in LVD as shown in the figures. The variance (SD of time to peak strain) was low in the normal individuals and significantly higher in the impaired LV group (p<0.001).
Conclusion: 2D strain imaging in the radial and circumferential dimensions shows highly synchronous contractions in healthy controls in contrast to marked dyssynchrony found in patients with LVD. Unlike Tissue-Doppler imaging, this new method has the added advantage because it can identify dyssynchronous contraction independently of angle of insonation.
echocardiography; dyssynchrony; strain
244 ASSESSMENT OF MECHANICAL INTRAVENTRICULAR DYSSYNCHRONY BY REAL-TIME 3 DIMENSIONAL ECHOCARDIOGRAPHY USING REGIONALVOLUMETRIC CHANGES: A FEASIBILITY AND REPRODUCIBILITY STUDY
O. Al Sharef, E. Liodakis, D. Dawson, P. Nihoyannopoulos.Hammersmith Hospital, London, UK
Background: Mechanical ventricular dyssynchrony (MVD) is a common finding in progressive heart failure (HF) and with the introduction of cardiac resynchronisation therapy (CRT) as a novel therapy for HF, it has become crucial to accurately quantify MVD.
Although, Colour-Tissue Doppler Imaging has been very useful to quantify MVD, it is still evaluating only one plane at a time and the heart exists as a volume.
Real-Time 3-Dimensional Echocardiography (RT3DE) has been validated for its accuracy for quantifying LV volumes in several studies and therefore it provides a potentially powerful tool for assessing MVD of the heart as a volume.
MVD can be quantified using Dyssynchrony Index (DI), defined as the standard deviation of the mean time for the 16 segments (ASE model) to reach their minimal systolic volume.
Objectives: We sought to assess the feasibility and reproducibility of quantifying MVD by measuring regional LV volume changes over time using RT3DE.
Methods: We studied 65 subjects (35 normal and 30 had HF).
Full volume RT3D scanning was performed using SONOS 7500 and X4 transducer The volumetric data was then analysed offline using Tom Tec 4D LV-Analysis-CRT software to derive the LV regional volumes and DI (fig 1).

Abstract 243
Results: The mean DI was 28.6 (SD 12.6) for normal and 84.0 (22.0) for HFgroup. DI measurements showed strong inter-observer and intra-observer reproducibility (ICC = 0.90, p<0.001 and ICC = 0.93, p<0.001 respectively) in both groups. The receiver operated curve (ROC, fig 2) for DI with area under curve of 97% (p<0.001) showed that cut-off value of ⩾54 msec provided optimal sensitivity and specificity to predict significant MVD.

Abstract 243
Conclusion: RT3DE is a robust tool that allows accurate quantification of MVD by measuring regional LV volumetric changes. A DI ⩾54 msec marks the presence of significant MVD.
mechanical intraventricular dyssynchrony; real-time three-dimensional echocardiography; heart failure
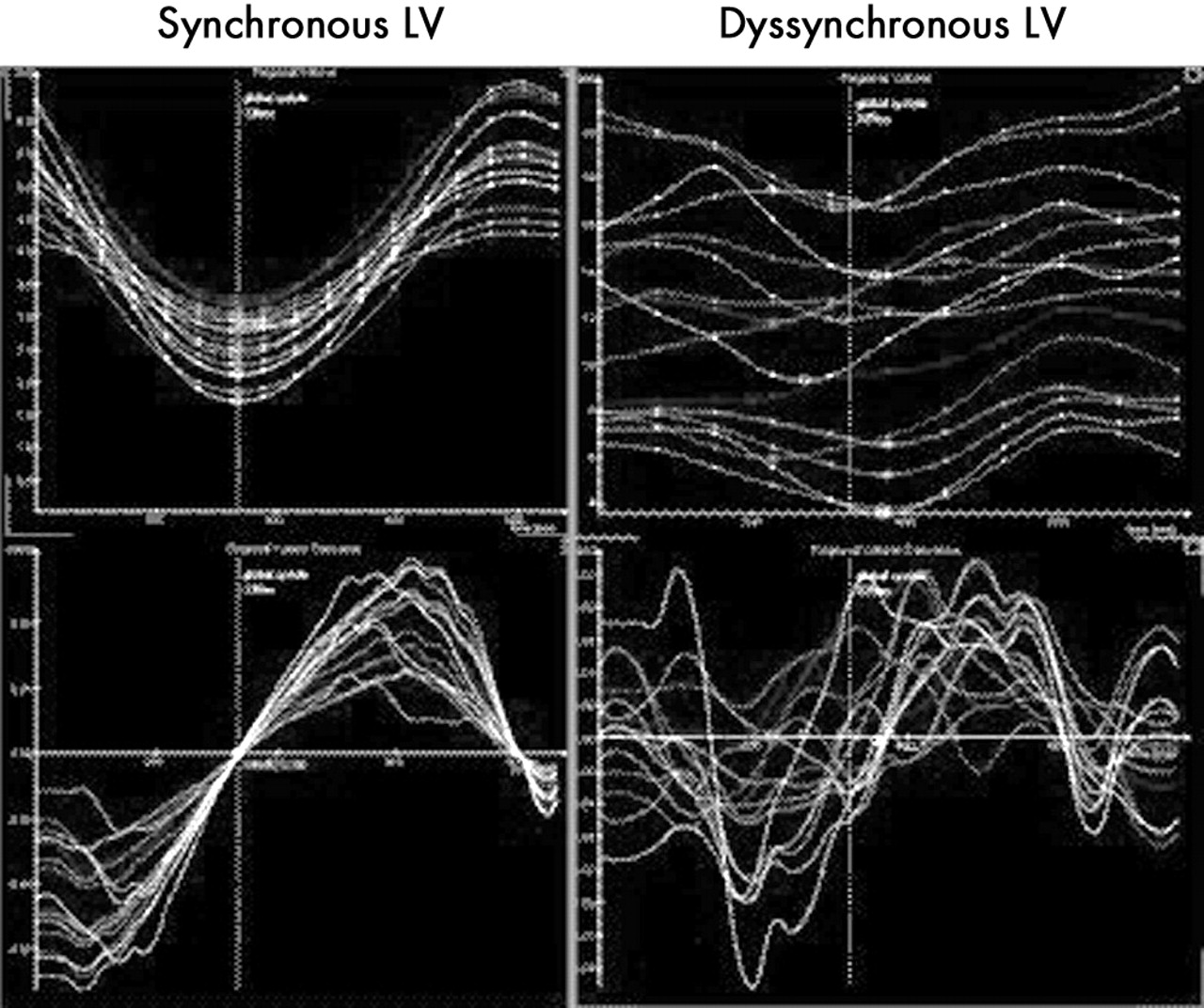
Abstract 244

Abstract 244
245 ECHOCARDIOGRAPHIC ASSESSMENT OF LEFT VENTRICULAR FUNCTION IN PACEMAKER PATIENTS: BENEFITS OF RIGHT VENTRICULAR SEPTAL LEAD PLACEMENT AND IMPLICATIONS FOR ASSESSMENT OF THE PACED VENTRICLE
A. Marsh1, G. Ng2, H. Marshall3, M. Gammage1.1Department of Cardiovascular Medicine, University of Birmingham, Birmingham, UK; 2Department of Cardiovascular Medicine, University of Leicester, Leicester, UK; 3University Hospital Birmingham NHS Foundation Trust, Birmingham, UK
A number of recent studies have demonstrated the potentially detrimental effects of right ventricular apical (RVA) pacing, but whether these effects can be mitigated by pacing from elsewhere in the right ventricle remains unclear. In addition, many early studies utilised short time course follow-up which may not allow adequate time for the remodelling process. We studied 58 unselected, consecutive patients presenting with high-degree heart block (mean age 74.7+11.5 years, 36 male), randomised to receive a passive RVA lead or an active fixation RV septal (RVS) lead. Follow-up was at 24 hours, 1, 6, 12 and 18 months. Fractional shortening (FS)(%), left ventricular atrioventricular plane displacement (LVAVPD, mm), tricuspid annular plane systolic excursion (TAPSE, mm) and mitral regurgitation severity (MR, semi-quantitative scale, 0 (none) to 3 (severe)) were measured by 2-dimensional echocardiography. There were no significant changes in FS in either group over the 18 months (RVA 33.95+11.20 v RVS 30.19+8.45 at 24 hours)(30.24+9.89 RVA v 30.46+10.22 at 18 months). LVAVPD fell more in the RVA than the RVS group between 24 hours and 18 months (RVA: 12.9+3.3 to 9.1+2.4, p<0.05)(RVS: 13.3+3.5 to 11.3+2.3, NS); RVA was lower than RVS at 18 months (p<0.01). TAPSE showed no significant changes within or between groups over the follow up period. Severity of MR increased in the RVA patients between 24 hours and 18 months (0.46+0.65 v 1.20+0.80, p<0.05) but was not significantly changed in RVS (0.62+0.89 v 0.90+0.84, NS). No parameters showed any differences between groups at implant or at 24 hours post implant. In agreement with other recent studies, significant differences in LV function resulting from different ventricular pacing sites did not develop until 12–18 months after pacemaker implantation.
Conclusions: Most parameters of LV function show significant deterioration after 18 months of RVA pacing. RVS pacing shows significantly better LV function than RVA at 18 months, but traditional echocardiographic assessments utilising formulae derived from short axis measurements, eg FS, are not suitable to detect this. These data support the use of non-RVA pacing sites for improving medium-term LV function, and demonstrate the need to utilise more sophisticated echocardiographic assessment of LV function in paced patients.
ventricular pacing; septum; function
246 PULMONARY HEMODYNAMIC EFFECTS OF NOVEL ULTRASOUND IMAGING AGENT CARDIOSPHERE AND DIPYRIDAMOLE INFUSION IN PATIENTS WITH NORMAL AND ELEVATED PULMONARY ARTERY SYSTOLIC PRESSURE
M. Main1, A. Ehlgen2, T. Tremblay2, N. Schiller3, J. Goldman2.1Cardiovascular Consultants, Kansas City, US; 2POINT Biomedical Corp., San Carlos, US; 3University of California, San Francisco, US
Background: Intravenous administration of microspheres used as ultrasound contrast agents have the potential for compromising the pulmonary microvasculature and thereby inducing hemodynamic change. The ultrasound contrast agent CARDIOsphere contains nitrogen/polymer/protein microspheres intended for use with dipyridamole in myocardial perfusion echocardiography. The microspheres have diameter of 3 µm (range 2–6 µm). The effects of CARDIOsphere alone or in combination with dipyridamole on pulmonary hemodynamics measured by pulmonary artery systolic pressure (PASP), pulmonary vascular resistance (PVR), and pulmonary valve velocity time integral (PVVTI) have not been previously described.
Methods: 20 patients (mean age 69; 12 females) with clinically suspected coronary artery disease and no intracardiac shunting were studied; 10 patients had elevated baseline PASP (>35 mmHg). Doppler-derived pulmonary hemodynamics (PASP, PVR, PVVTI) were determined using echocardiographic methods previously validated against invasive method. 10 patients (5 with normal, 5 with elevated screening PASP) received a 30 minutes CARDIOsphere infusion (0.175 mg/kg diluted in 150 ml dextrose) at an infusion rate of 150 ml/h. 10 patients (5 with normal, 5 with elevated screening PASP) received a 30 minutes placebo infusion (150 ml Dextrose) at an infusion rate of 150 ml/h. All patients received dipyridamole (DP) (0.56 mg/kg) after 15 minutes. Pulmonary hemodynamics were obtained at defined timepoints throughout the entire infusion. Patients were monitored for clinical signs of acute pulmonary hypertension.
Results:
Abstract 246
During CARDIOsphere/placebo infusion, there were no significant changes in PASP, PVR, or PVVTI compared to baseline (p>0.05). Following dipyridamole, there was a statistically significant increase in PASP and PVVTI (p<0.05) and a statistically significant reduction in PVR (p<0.05) in patients receiving CARDIOsphere and placebo infusion (see table). The above changes occurred in patients with normal as well as elevated screening PASP. No patient showed clinical signs of acute pulmonary hypertension and there were no serious adverse events.
Conclusion: CARDIOsphere infusion does not alter pulmonary hemodynamics. An increase in pulmonary artery pressure and pulmonary flow and a decrease in pulmonary vascular resistance is seen following dipyridamole administration.
contrast echocardiography; myocardial perfusion imaging; pulmonary hypertension
247 A CARDIAC TECHNICIAN - LED TRANSOESOPHAGEAL ECHOCARDIOGRAPHY SERVICE
L. Drummond, R. Sharma, I. Simpson.Southampton General Hospital, Southampton, UK
Objective: We report the development of a cardiac technician based, unsupervised transoesophageal echocardiography (TOE) service, a procedure traditionally performed by medical staff and examined its feasibility and safety in a busy cardiothoracic unit.
Methods: Following development of a programme for technician led TOE, an experienced (MTO5) sonographer was trained in obtaining consent, venous cannulation, sedation administration, probe intubation and manipulation, data acquisition and interpretation over a 12 month period. Unsupervised midazolam sedation and local anaesthetic administration was approved by the hospital trust pharmacy committee under cardiac anaesthesia guidance. The sonographer attended the clinical skills department cannulation course. The principles and practice of obtaining patient consent were learnt under the guidance of trust risk management. We present the data for the first 146 unsupervised cases over a subsequent 16 month period. All TOE were included for a technician led study apart from those with suspected aortic dissection, haemodynamic instability or intraoperative cases.
Results: In total 146 procedures were performed unsupervised. These included mitral valve assessment (n = 27), aortic valve assessment (n = 7), suspected endocarditis (n = 38), thromboembolic cause (n = 25), prosthetic valve assessment (n = 6), grown up congenital heart disease (n = 27), other (n = 16). There were no significant adverse events related to the procedure. Probe intubation was unsuccessful in 5 patients of which 2 could not be passed by an experienced cardiologist. Mean procedure time was 30 minutes. Mean number of patients per list was 4. Mean midazolam dose was 3mg per patient. When data interpretation was compared with an experienced doctor, interobserver agreement was 95% (k = 0.87). The differences (n = 7) were minor and predominantly related to scallop assessment of the mitral valve (n = 4), anomalous pulmonary venous drainage (n = 2), post Fontan repair assessment (n = 1). No significant lesions were missed that affected patient management.
Conclusion: A fully unsupervised TOE list by an appropriately trained cardiac technician is safe and feasible allowing modernisation of traditional TOE services and extended roles for advanced echo technicians.
transoesophageal echocardiography; cardiac sonographer; national health service modernisation
248 PERCUTANEOUS LEFT ATRIAL APPENDAGE TRANSCATHETER OCCLUSION (PLAATO) IN PATIENTS WITH HIGH RISK ATRIAL FIBRILLATION
J. Foran, A. Theodosis-Georgilas, N. Bunce, A. Bajpai, A. Kapoor, S. Ahmadvazir, A. Camm, E. Rowland.St George’s Hospital, London, UK
In patients with chronic atrial fibrillation (AF) the left atrial appendage (LAA) is known to be a common source of thrombus formation, which may result in thromboembolic stroke. Warfarin remains the treatment of choice for such patients but a significant minority possess contraindications to Warfarin therapy. Surgical LAA exclusion has been advocated at the time of mitral valve surgery in patients with chronic AF in an effort to reduce stroke risk but cannot currently be justified as a stand-alone procedure and a number of percutaneous techniques have been developed to occlude the LAA with the intention being to reduce stroke risk in chronic AF patients who cannot be treated with Warfarin. The PLAATO device is a self-expanding Nitinol semi-spherical hooked cage covered on 2/3 of its surface with an ePTFE membrane, designed for occlusive placement in the proximal LAA via a percutaneous transseptal approach. We report our experience with the PLAATO device in 10 patients (2 female), aged 64 (SD 12) years, with high-risk chronic AF in whom Warfarin was contraindicated. The mean duration of AF was 75 (94) months and prior CVA/TIA was documented in 4/1 patients respectively. Nine patients had previously been treated with Warfarin, which had to be discontinued as a result of life-threatening haemorrhage in n = 6. Transoesophageal echocardiography revealed spontaneous echo contrast in 6/10 patients and the mean LA dimension was 4.9 (1.1) cm. PLAATO device deployment was attempted in 9/10 patients and successful in 8/10 patients; the 2 untreated patients possessed LAA diameters which were too large to safely occlude using the largest available device. The median procedure time was 58 minutes. There were no acute complications from PLAATO device implantation. During 16 (9) months of follow-up there have been no CVA/TIA events in the treated patients. One patient died 7 months post procedure following a witnessed out-of-hospital VF arrest, which did not respond to external DC cardioversion. One patient, who had a normal echo post procedure and no symptoms at the time of their 1 month follow-up, developed pericardial pain 5 weeks post PLAATO implantation; repeat echocardiography demonstrated a small amount of pericardial fluid which resolved completely with the use of ibuprofen. We conclude that LAA occlusion using the PLAATO device is associated with a good safety profile and may thus be considered a reasonable therapeutic option in patients with high-risk chronic AF who are unsuitable for Warfarin therapy.
atrial fibrillation; left atrial appendage; PLAATO
249 MYOCARDIAL INFARCTION INDUCED BY ALCOHOL SEPTAL ABLATION FOR HYPERTROPHIC CARDIOMYOPATHY DOES NOT ACTIVATE PLATELETS
E. Smith1, R. Anthony2, R. Mo2, A. Jain1, M. Preston1, K. McConnell1, M. Macey3, M. Rothman1, A. Mathur1, C. Knight1.1London Chest Hospital, London, U K; 2Queen Mary University of London, London, UK; 3Royal London Hospital, London, UK
Acute myocardial infarction (AMI) is characterised by heightened platelet activation (PA). However, it remains uncertain whether PA is a cause of AMI, or a reaction to ischaemia, inflammation or myocyte necrosis. We investigated PA following therapeutic myocardial infarction in the absence of coronary plaque rupture.
Methods: 14 patients underwent percutaneous ventricular septal reduction for hypertrophic cardiomyopathy. Patients with angiographic coronary disease were excluded. 1–2 mls of absolute alcohol (AA) was injected into a septal artery causing local infarction. Blood was collected via a femoral venous sheath prior to angiography, immediately before AA injection, and at 15 min, 30 min, 1 hr, 2 hr and 24 hr post procedure. Plasma sCD40 ligand, P-selectin and Interleukin-6 were assayed by ELISA. Creatine kinase (CK) was measured at 24 hours for infarct size.
Results: Mean CK at 24 hours was 849 (SD 467) i.u. The graph demostrates platelet activation and inflammatory marker levels up to 24 hours following septal ablation, data expressed as mean+/−SEM. IL-6 remained constant at 0–30 min, but rose significantly at each time point thereafter (T = 0–1, p = 0.002; T = 1–2, p = 0.003; T = 2–24, p = 0.017). sCD40L and P-selectin remained unchanged at all time points.
Conclusions: Despite causing substantial myocyte necrosis and inflammation, myocardial infarction in the absence of a coronary plaque event does not result in platelet activation. These data suggest that elevated platelet activation in the clinical setting of acute myocardial infarction signifies coronary plaque disruption.
hypertrophic cardiomyopathy; alcohol septal ablation; platelet activation

Abstract 249
250 PERCUTANEOUS CORONARY INTERVENTION IN THE MODERN ERA: A SIMPLIFIED TARGET LESION AND VESSEL CLASSIFICATION SYSTEM MAY BE WARRANTED
E. Roberts, A. Alahmar, A. Grayson, R. Stables, R. Perry.Liverpool Cardiothoracic Centre, Liverpool, UK
Background: The original American College of Cardiology (ACC)/American Heart Association (AHA) classification of lesion and vessel characteristics according to percutaneous coronary intervention (PCI) outcomes arose from the pre stent era. Subsequent modifications developed in line with increasing stent usage, culminating in the simplified Society for Cardiovascular Angiography and Interventions (SCAI) system, whereby four groups were proposed based on vessel patency and ACC/AHA type C/non C characteristics. This classification system was a good predictor of outcomes among SCAI registry cases between 1998 and 2000, for which stent usage was 74.5%. Current practice differs in terms of type and prevalence of stent usage, radial access, increased left main stem procedures, and aggressive antiplatelet therapy. This study evaluates the predictive power of target lesion and vessel characteristics for angiographic outcomes in the current era.
Methods: Data for 6719 consecutive PCIs in 10 800 lesions from January 2000 to December 2004 were classified according to ACC/AHA type and entered into a database. Multivariate forward stepwise logistic regression was used to identify predictors of lesion failure.
Results: Stents were used in 10 126 (93.8%) lesions, radial procedures comprised 29.2% of cases, and left main stem interventions comprised 1.2% of cases. There were 10 505 successful angiographic outcomes on a lesion-by-lesion basis (97.3%), defined as <50% residual stenosis. Success rates did not differ between ACC/AHA type A (945 of 955, 98.9%), B1 (1534 of 1550, 99.0%), and B2 lesions (4312 of 4351, 99.1%), but each was higher than the success rate for type C lesions (3714 of 3944, 94.2%) (p<0.001, p<0.001, and p<0.001 respectively). There were 295 angiographic failures, for which predictors were total occlusion >3 months, total occlusion <3 months, severe calcification, excessive target vessel tortuosity, graft intervention, and lesion angulation >90 degrees (see table). Characteristics such as lesion length, ostial location, bifurcation lesions, and presence of thrombus were not significantly associated with angiographic failure. There were no angiographic failures for left main stem procedures.
Conclusions: Previously influential lesion and vessel characteristics are no longer predictive of angiographic success or failure following PCI. A simplified classification based on the predictors detailed here may be appropriate.
Abstract 250
percutaneous coronary intervention; lesion classification; angiographic success

Abstract 251
251 DRUG-ELUTING STENTS IN CLINICAL PRACTICE: EARLY RESULTS IN A PROPENSITY-MATCHED COHORT
A. Alahmar, E. Roberts, A. Grayson, M. Jackson, R. Perry.Cardiothoracic Centre Liverpool, Liverpool, UK
Background: Randomised control trial evidence has shown that drug-eluting stents (DES) offer significant reductions in restenosis rates compared to bare metal stents (BMS). Trial cohorts, however, are always different from real clinical practice. We aimed to assess the impact of DES in routine clinical practice on target-lesion revascularisation (TLR).
Methods: In order to account for differences in case-mix, we performed a propensity-matched analysis on angioplasty performed between April 2003 and March 2004. Logistic regression was used to develop a propensity score for DES group membership. The propensity score included demographics, lesion length, vessel diameter, diabetes. The C statistic for this model was 0.80. Clinically driven TLR at 1-year were described using the product-limit methodology of Kaplan-Meier, censoring for death.
Results: 427 patients received DES compared to 1176 patients with BMS during the study period. DES compared to BMS had more diabetics (42.2% v 5.2%, p<0.001), lesions with diameter <2.5 mm (42.2 v 30.9, p<0.001), and lesions >20 mm in length (48.5% v 41.3%, p = 0.011).TLR rate was 3.5% with DES to 6.5% with BMS (p = 0.025). 291 DES patients were matched with 291 BMS patients who had an identical propensity score producing well matched groups (see table). TLR rates in propensity-matched groups were 3.8% with DES to 8.6% with BMS (p = 0.016, see figure).
Abstract 251
Conclusion: In our own routine clinical practice the clinically-driven 1-year TLR rates in DES and BMS are lower than that in large randomised trials. After adjusting for case-mix differences with propensity-matching, DES significantly reduced TLR compared to BMS.
DES drug eluting stent; TLR target lesion revascularisation; BMS bare metal stent
252 IS SIROLIMUS BETTER FOR DIABETICS THAN PACLITAXEL? A CONTEMPORARY COMPARATIVE ANALYSIS OF OUTCOMES AFTER SIROLIMUS- AND PACLITAXEL-ELUTING STENT IMPLANTATION
S. Corbett1, J. Cosgrave1, R. Babic1, G. Melzi1, T. Aranzulla2, N. Morici2, C. Godino2, A. Chieffo2, I. Michev2, F. Airoldi2, M. Montorfano2, M. Carlino2, G. Sangiorgi1, A. Cololmbo1.1Centro Cuore Columbus, Milan, Italy; 2San Raffaele Hospital, Milan, Italy
Background: Despite drug-eluting stents (DES), diabetes mellitus remains an important predictor of repeat revascularisation after percutaneous coronary intervention. Recent data suggests an advantage for sirolimus-eluting stents (SES) over paclitaxel-eluting stents (PES) in diabetic patients. In light of this, we compared the outcomes after PES and SES implantation in a real world cohort of diabetics.
Methods: After PES and SES implantation in diabetics we analysed: late loss, binary restenosis and a composite of death, myocardial infarction and target vessel revascularisation (MACE) at 9 months.
Results: 696 lesions were treated in 367 diabetic patients between March 2003 and December 2004. PES and SES were implanted in 182 and 185 patients respectively. There were no significant differences in the baseline clinical and angiographic parameters, or rate of angiographic follow-up in the PES and SES groups. Lesion complexity was high in both groups with >70% AHA/ACC type B2/C lesions and the average stent length per lesion was over 28 mm. Late loss was greater for PES at 0.64 (SD 0.77) mm v 0.39 (0.87) mm for SES (p = 0.004). Despite this, binary restenosis was similar in PES and SES (25.7% v 28.6%, p = 0.54) as were the rates of MACE (28.6% v 35.1%, p = 0.25) and target lesion revascularisation (14.4% vs. 18.8%, p = 0.125).
Conclusions: The advantage in late loss for SES in diabetics does not translate into a measurable clinical benefit in our large series of patients with complex lesions. After DES implantation in diabetics, MACE rates remain substantially higher in the real world than in randomised trials.
drug-eluting stent; diabetes mellitus; revascularisation
253 SELECTIVE USE OF DRUG ELUTING STENTS IS NOT ASSOCIATED WITH HIGH ADVERSE CLINICAL EVENT RATES IN REAL WORLD CARDIOLOGY PRACTICE
B. Gordon, J. Riddell, N. McKenna, M. Rice, N. Herity, C. Hanratty.Belfast City Hospital, Belfast, UK
Background: The exclusive use of drug eluting stents (DES) is being advocated as a superior coronary interventional strategy. Data suggests less target lesion failure compared to bare metal stents (BMS). However, clinical restenosis rates for certain groups are actually very low using BMS. We sought to determine our outcomes following percutaneous coronary intervention (PCI) when a selective approach was adopted to DES use, based on clinical indication.
Methods: All PCI cases carried out at Belfast City Hospital during 2004 were included. Suggested criteria for DES deployment were; target vessel diameter<3 mm, lesion length>20 mm, proximal LAD lesion, diabetes mellitus or clinical need at the discretion of the cardiologist based on anatomy of the vessel and/or clinical presentation. Patients were followed up at 6 months by telephone contact to determine major adverse cardiac events (defined as death, myocardial infarction or target lesion revascularisation- TLR).
Results: 815 patients had PCI in 2004. The total number of stents deployed was 1067 and 248 of these were DES (23.2%). As well as the defined selection criteria, the use of DES was limited by financial constraints and availability. Follow up data is available for 804/815 (98.7%). 57/804 (7.1%) had a clinical indication for repeat coronary angiography. 30/804 (3.7%) had target vessel failure (acute thrombosis or clinically significant restenosis). Of these, 5/30 had a DES deployed originally. Major adverse cardiac events occured in 51/804 (6.3%).
Conclusions: Our 2004 results demonstrate a 6.3% major adverse cardic event (MACE) rate and a 3.7% target vessel failure rate six months after PCI with 23.2% DES usage. In real world cardiology practice we suggest a pragmatic approach to the use of drug eluting stents is an appropriate interventional strategy. A very acceptable rate of clinical events and TLR can be achieved by careful stent selection based on clinical and vessel/lesion characteristics.
percutaneous coronary intervention; drug eluting stents; restenosis
254 THE IMPACT OF A POLICY OF SELECTIVE DRUG ELUTING STENT IMPLANTATION UPON CLINICAL RESTENOSIS: A ‘REAL WORLD’ REGISTRY
A. Siotia1, S. Mofidi1, A. Morton2, C. Wales1, C. Newman1, J. Gunn1.1Sheffield Teaching Hospitals NHS Trust, Sheffield, UK; 2Sheffield Teaching Hospitals NHS Trusts, Sheffield, UK
Background: Drug eluting stents (DES) reduce the risk of restenosis as compared to bare metal stents (BMS) in randomised, controlled trials. A significantly higher cost of these stents, however, makes their use in all patients undergoing percutaneous coronary intervention (PCI) problematic. Two years ago, we argued for a policy of selective implantation of DES, restricting their use in arteries of small calibre requiring a long stent, with extra allowance for diabetic patients (table 1).
Aim: To test whether this policy of selective implantation of DES has led to a clinically useful reduction in the overall institutional clinical restenosis rate.
Methods: In the 6 month period preceding the introduction of DES in our institution, 485 patients underwent PCI (pre-DES group). We studied an identical number of consecutive patients after the introduction of DES (post-DES group). We then examined the catheter laboratory database of both groups to determine the rate of clinical restenosis within 12 months of the index procedure.
Results: In the pre-DES group (n = 485), 420 (87%) underwent stent implantation and 696 BMS were implanted. In the post-DES group (n = 485), 452 (93%) underwent stent implantation and 796 stents were implanted, of which 559 (70%) were BMS and 237 (30%) DES. The number of stents/patient was 1.7 in both groups. In the pre-DES group, 22 (5.2%) patients underwent clinical restenosis compared with 21(4.6%) in the post-DES group (p = ns), of which 18 were in BMS and 3 in DES.
Conclusions: The clinical restenosis rate in our pre-DES group was surprisingly low and, overall, was not reduced by a policy of targeting DES to the 30% of lesions thought to be at highest risk of restenosis. Possible causes include poor adherence to the guidelines, improving performance of BMS and a limited relationship between ‘late loss’ and real world re-presentation.
percutaneous coronary intervention; drug eluting stents; restenosis

Abstract 254
255 DAY CASE TRANSFER WITH A RADIAL ARTERY APPROACH: A REGIONAL SOLUTION FOR THE EARLY INVASIVE STRATEGY IN NON-ST ELEVATION ACUTE CORONARY SYNDROMES
Y. Raja, S. Jain, J. Stubbs, P. Henry-Wilkins, S. Baines, A. Qasim, P. Glennon.1Walsgrave Hospital, Coventry, UK
Introduction: Early angiography and revascularisation are beneficial in patients with Non-ST elevation acute coronary syndromes (ACS), and are now recommended by national and international guidelines. This early invasive approach can be achieved within interventional centres, but delays in transferring patients to tertiary centres due to bed shortages have been a major obstacle. We proposed that transfer of ACS patients using standard elective day case unit (DCU) facilities would be a safe and effective solution to this problem.
Methods: Audit demonstrated that the mean waiting time to transfer for angiography in ACS was 5.9 (range 2–14) days.In the day case transfer (DCT) system patients are transferred to trolleys in the DCU and returned to the referring hospital after their procedure on the same day. A higher risk group was identified and these patients are listed for conventional transfer. Referral proformas are faxed from the district hospital to the nurse coordinator who arranges for DCT or bed transfer in accordance with specified DCT criteria. In order to simplify care of arterial access sites on return to the referring hospital the radial artery approach is encouraged, and an Angioseal closure device is deployed if the femoral artery is used.
Results: In 2002 365 patients were transferred for early angiography in ACS with a mean wait to transfer of 5.9 (range 2–14) days. Following the introduction of the DCT system in 2003 in total 403 patients were transferred including DCT and conventional transfer and the mean time to transfer was reduced to 2.9 (range 0–10) days (p<0.05). In 2004 560 patients were transferred with mean waiting time 1.7 (range 0–10) days (p<0.05). In the first 8 months of 2005 455 patients were transferred with a mean wait of 2.5 (range 1–9) days (p<0.05).
In 8 consecutive months in 2005, 455 patients were referred for transfer for early angiography in ACS/NSTEMI. 245 (53%) were accepted for DCT, and the remainder were listed for conventional transfer. In DCT patients angiography was performed from the radial route in 165 (67%) and femoral route in 80 (33%) of patients. PCI was performed in 124 (50.6%) patients, and 12 (5%) of patients were referred for inpatient CABG. 25 (10%) of DCT patients remained at the tertiary centre following angiography: 12 for urgent CABG surgery, 7 following complex multivessel PCI, 3 due to transport problems, and 3 because of non-coronary vascular complications. No patients that were transferred back to the referring hospital after a DCT procedure required inpatient transfer back to the tertiary centre.
Conclusions: The DCT system significantly reduced the delay in transferring patients for early angiography in ACS. The DCT system has required flexible and cooperative interactions between medical, nursing, ambulance and administrative staff. It has provided a safe and effective mechanism to allow an early invasive strategy in patients presenting with ACS/NSTEMI.
ACS; NSTEMI; PCI
256 SHOTGUN STENTING OF LEFT MAIN BIFURCATION STENOSIS
A. Siotia, A. Morton, J. Gunn.Sheffield Teaching Hospitals NHS Trust, Sheffield, UK
Background: There is no single, widely accepted interventional technique for treating left main stem (LMS) bifurcation stenosis. We performed a prospective, safety and feasibility study of treating such lesions with the “shotgun” (kissing) stent technique.
Methods: 30 consecutive patients with LMS bifurcation stenosis were treated using a shotgun technique. Drug-eluting stents were used when technically feasible (28/30 cases). Balloon counterpulsation was used in 3 patients and 25 received abciximab. All patients were scheduled for 6 month clinical and angiographic follow-up.
Results: Mean age was 63 years, 19 were male, 26 were elective, 3 urgent and 1 emergency. The procedure was successful in all cases. There was 1 in-hospital death (a 65 y old man with anterior myocardial infarction, LMS, LAD and OM stenoses, recurrent ventricular fibrillation (VF), ejection fraction 40% and bronchopneumonia who had been turned down for CABG). Following a successful emergency PCI, he could not be resuscitated after a third episode of VF. There was no other major adverse cardiac event. 23 follow-up angiograms have been performed so far and 2 patients (9%) required target lesion revascularisation for restenosis. One of these two had bare metal stents implanted. At follow up of 10 (SD 3.4) months, the remaining 27 patients remain well and free of angina.
Conclusion: The shotgun technique for treating bifurcation disease of the LMS is safe and feasible. Medium term results are good.
left main stem; percutaneous coronary intervention; shotgun stent

Abstract 256
257 SHORT-TERM VENTRICULAR PACING INDUCES GAP JUNCTIONAL REMODELLING IN THE MURINE HEART
R. Kaba1, A. Kontogeorgis1, J. Sereysky2, S. Lewitton2, A. Wit3, N. Peters1, D. Gutstein2.1Imperial College London, St Mary’s Hospital, London, UK; 2New York University School of Medicine, New York, US; 3Columbia University College of Physicians and Surgeons, New York, US
Background: Structural gap junction remodelling (GJR), characterised by abnormal localisation and/or altered abundance of connexin43 (Cx43) in the cardiomyocyte, is a process that accompanies pathologic cardiac conditions such as ischaemia, hypertrophy and dilatation. The contribution of GJR to the arrhythmic substrate is well established in both human disease states and in animal models. We hypothesised that structural GJR in the mouse heart could be induced by ventricular pacing and that remodelling might become evident over a short period of time.
Methods: Under general anaesthesia a mid-line laparotomy was performed and a trans-diaphragmatic approach used to position a pacing electrode on the right ventricle in close proximity to the apex. Mice were paced at 10%–15% above their average anaesthetised sinus rate and monitored to ensure 1:1 capture for the duration of the experiment. Surface-lead electrograms were recorded in each experiment and echocardiographic data was obtained before and after pacing.
Results: Pacing-induced GJR was not limited to areas in close proximity to the stimulating electrode, but was evident throughout the right and left ventricles. Despite extensive redistribution of Cx43 to the lateral borders of myocytes in the paced hearts, cadherin - a critical component of adherens junctions - remained localised to the intercalated discs. Although all echocardiographic, and most ECG, parameters were unaltered by pacing, QRS amplitude was significantly diminished after pacing in a time-specific manner (p = 0.002).
Conclusions: Development of a reliable procedure for inducing GJR in the mouse heart may facilitate the study of the remodelling process. Since GJR may be preventable or reversible in cardiac disease states, elucidating the pathways involved in the development of GJR may allow for the pharmacologic targeting of intermediaries in those pathways and the prevention of arrhythmic complications of GJR. Diminished QRS amplitude after pacing may signify altered electrical activation patterns within the myocardium.
gap junctions; pacing; arrhythmias
258 INTRACELLULAR AND GAP-JUNCTION CONDUCTANCE CORRELATES WITH CONNEXIN43 QUANTITY IN LEFT VENTRICULAR SEPTAL MYOCARDIUM IN PATIENTS WITH HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
P. Dhillon1, P. Patel2, R. Gray3, A. Jacques4, R. Chowdhury2, Y. Aguiar Martins2, V. Tsang5, S. Marston4, C. Fry3, W. McKenna5, N. Peters2.1Imperial College, London, UK; 2Imperial College St Mary’s Campus, London, UK; 3University College, London, UK; 4Imperial College Brompton Campus, London, UK; 5The Heart Hospital, London, UK
Introduction: Hypertrophic obstructive cardiomyopathy (HOCM) is characterised by asymmetric septal hypertrophy and is associated with lethal ventricular arrhythmias. The electrophysiological characteristics of the septal region have yet to be determined. Gap junction remodelling and associated alterations of tissue impedance may lead to slowing of cardiac action potential conduction which may predispose to arrhythmias. We measured tissue impedance in seven left ventricular septal myectomy preparations from patients diagnosed with HOCM (5M, mean 45 (SD 10.6) years, all NYHA III) and quantitatively determined levels of the major ventricular gap junction protein connexin 43 (Cx43) in each patient. Only one patient had a history of ventricular tachycardia (VT).
Methods: Tissue impedance. Strips from the left ventricular septum (5.2 (SD 1.1) mm×1 (0.2) mm) were pulled across a three compartment bath; the middle chamber filled with mineral oil and the outer chambers with oxygenated Tyrode’s solution (37°C). Alternating current (frequency 20 Hz–300 kHz) was passed along preparations. The longitudinal impedance was analysed in terms of an equivalent circuit consisting of an intracellular and extracellular pathway. Values were determined for intracellular resistance (Ri) gap junctional resistance (Rj) and cytoplasmic resistance (Rc). Cx43. Quantitative measurements were made using standard Western blotting techniques.
Results: Mean Ri, Rj and Rc were as follows, 865 (271), 586 (235) and 279 (47) Ω.cm. A Plot of values of Ri, Rj and Rc for each patient against their relative Cx43 quantity is shown below. There was a negative correlation between Cx43 and Ri and Rj (Pearson r of −0.88 and −0.89 respectively, p<0.05 in both cases). There was no correlation between Cx43 and Rc. Intriguingly the highest Ri and Rj values were measured in the patient with a history of VT.
Conclusion: There is a direct relationship between whole tissue impedance and the quantity of Cx43 in the hypertrophied septum of patients with HOCM. A reduction of Cx43, and a consequent rise in Ri, may predispose to arrhythmias.
gap junction; cardiomyopathy, hypertrophic; myocardial impedance

Abstract 258
259 MURINE MYOCARDIAL INFARCTION CAUSES REMODELLING OF CONNEXIN43 IN THE PERI-INFARCT ZONE
R. Chowdhury1, D. Cervantes2, R. Kaba1, W. Hussain1, P. Patel1, Y. Aguiar-Martins1, A. Wit2, N. Peters1.1Imperial College London, London, UK; 2Columbia University, New York, US
Introduction: Gap junctions, containing connexins (Cxs), form the basis of intercellular connections for coordinated electrical activity. Myocardial infarction predisposes to lethal ventricular arrhythmias, which may be related to gap junction remodelling. As spatial reorganisation of gap junctions soon after myocardial infarction is poorly understood, we sought to study gap junction remodelling in a murine infarct model.
Methods: 10 week old mice (n = 9) underwent ligation of the left anterior descending artery via a lateral thoracotomy. After 3 days recovery VT induction was attempted by epicardial pacing through a median stenotomy. The mice were killed and the hearts were snap frozen in liquid nitrogen to undergo immunohistochemical analysis. Serial sections of 10 µm were cut through the ventricles from apex to base and every 30th sister sections were immunolabelled for Cx43 or stained by H&E. Sections were also immunolabelled for Cx40.
Results: Large left ventricular infarcts were identified in each heart, predominantly involving the apex to mid ventricle. Each infarct was commonly seen to be transmural, with slight sparing of the subendocardial region. No obvious epicardial border zone was visible. The peri-infarct region showed extensive cellular reorganisation of Cx43 with labelling also found at the lateral membranes. In some cases this area of remodelling penetrated into parts of the infarcted area. Regions more distant from the infarct but adjacent to the Cx43 remodelled zone demonstrated normal distribution of Cx43 labelling at the intercalated discs only. VT was induced consistently in 5 of the hearts (approximately 56%).
Conclusion: Induced myocardial infarction in the mouse ventricle causes remodelling of Cx43 in a well defined, but extensive zone lying between the infarction and the non-ischaemic myocardium. Such remodelling may contribute to the elevated risk of malignant arrhythmias post infarction.
connexion; myocardial infarction; remodelling
260 INCREASED CONNEXIN43 EXPRESSION IN THE LEFT VENTRICULAR SEPTUM IS ASSOCIATED WITH A FAMILY HISTORY OF SUDDEN CARDIAC DEATH IN PATIENTS WITH HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY
P. Dhillon1, P. Patel1, R. Gray2, A. Jacques3, S. Marston3, V. Tsang4, C. Fry2, W. McKenna4, N. Peters1.1Imperial College St Mary’s Campus, London, UK; 2University College, London, U K; 3Imperial College Brompton Campus, London, UK; 4The Heart Hospital, London, UK
Introduction: Hypertrophic obstructive cardiomyopathy (HOCM) is associated with sudden cardiac death (SCD) presumed to be due to ventricular arrhythmias. Studies have correlated features of the arrhythmogenic substrate, such as myocyte disarray, fibrosis and small vessel disease with risk profiles for SCD and clinical outcome. The expression of cardiac gap junction proteins are known to be associated with arrhythmias in several disease states including left ventricular hypertrophy. Our aim was to determine whether the quantity of the ventricular gap junction protein connexin 43 (Cx43) in the hypertrophied septum of patients with HOCM was associated with a family history of SCD.
Methods: Fourteen HOCM patients (11 male, 44 (SD 9.5) years NYHA grade 2.9 (0.3)) were referred for surgical septal myectomy. Left ventricular septal samples were snap frozen and used for quantitative Cx43 Western blotting.
Results: Four patients (29%) had a positive family history of SCD. There were no differences between this group and the remaining patients for age, sex, NYHA grade, resting outflow tract gradients, septal thickness, left ventricular systolic/diastolic dimensions or fractional shortening. Values of Cx43 were normalised to the mean value of the group without a family history of SCD. Those patients with a positive family history had a mean of 62% (28)% more Cx43 compared to those with no family history (p<0.01). A scatter plot of the two groups is shown below.
Conclusion: There is a 62% increase in Cx43 in the septum of patients with HOCM who have a family history of SCD compared to those who do not. The increased Cx43 may be related to arrhythmias predisposing to SCD.
gap junction; cardiomyopathy, hypertrophic; sudden cardiac death

Abstract 260
261 REGULATION OF P53 TETRAMERISATION AND NUCLEAR EXPORT BY ARC
R. Foo1, Y. Nam2, R. Kitsis2.1University of Cambridge, Cambridge, UK; 2Albert Einstein College, New York, US
There is now convincing evidence that cardiac myocyte apoptosis contributes to heart failure, and in at least 2 genetic mouse models of cardiomyopathy, inhibition of apoptosis reverses the progression of myocardial dilatation. Apoptosis repressor with caspase recruitment domain (ARC) is a recently discovered cardiac-enriched anti-apoptotic protein that is also upregulated in cancer. Since p53 is a pro-apoptotic protein that is central to both carcinogenesis and hypoxia-induced cardiac myocyte apoptosis, we set out to investigate the relationship between ARC and p53. We hypothesise that ARC suppresses p53 activity, hence maintaining cell survival in the case of myocytes but contributing to carcinogenesis where it inactivates the tumour suppressor p53. While we found firstly that ARC inhibits p53-induced apoptosis, using luciferase vectors bearing p53-binding sites, we determined also that ARC inhibits p53-transcriptional activity. The latter was further confirmed by downregulation of p53-target gene products such as MDM2 and p21. Next using co-immunoprecipitation and radiolabelled in vitro transcribed proteins respectively, we determined that ARC and p53 interact both endogenously and directly. To get at the exact mechanism by which ARC inactivates p53, we made His-tagged recombinant proteins and determined that ARC interacts with the tetramerisation domain of p53. The tet-domain of p53 bears a nuclear export signal which is hidden when p53 is tetramerised (p53tet). P53tet has many-fold higher transcriptional activity than monomeric p53. We demonstate that ARC disrupts p53 tetramerisation and inactivates p53 by nuclear hyper-export. In addition by disruption of p53 tetramerisation alone, ARC is also able to independently downregulate p53 transcriptional activity. This is the first demonstration that disruption of p53 tetramerisation is able to uncouple the control of p53 transcriptional activity and the p53 nuclear export. ARC therefore represents a important potential therapeutic target for both heart disease and cancer.
heart failure; apoptosis; p53
262 FAILURE TO ISCHAEMIC POSTCONDITION THE DIABETIC HEART
D. Hausenloy, A. Tsang, D. Yellon.The Hatter Institute, University College London, London, UK
A recent clinical study has reported that ischaemic postconditioning, a phenomenon which describes the cardioprotection conferred by interrupting myocardial reperfusion with transient episodes of ischaemia, reduces myocardial infarct size in patients treated with primary percutaneous coronary intervention. Whether the diabetic heart is amenable to protection by ischaemic postconditioning is an unanswered and fundamental question given the prevalence of ischaemic heart disease among diabetic patients. Previous studies have reported that signalling through the PI3K-Akt kinase pathway is required for postconditioning protection, and other studies have separately found impaired PI3K-Akt signalling in the diabetic myocardium. We hypothesised that the diabetic heart cannot be protected by ischaemic postconditioning and that this may be due to impaired signalling through the PI3K-Akt pathway. Hearts isolated from the in-bred lean model of type II diabetes (the Goto-Kakizaki rat), were randomised to either control or treatment with ischaemic postconditioning. Control hearts were mounted on a Langendorff apparatus and subjected to 35 minutes of myocardial ischaemia followed by either: (a) 10 minutes of myocardial reperfusion, at the end of which the myocardium at risk was excised and snap-frozen in liquid nitrogen for subsequent Western blot analysis for Akt phosphorylation, as a measure of signalling through the PI3K-Akt pathway or (b) 120 minutes of reperfusion at the end of which myocardial infarct size was determined using tetrazolium staining, as a measure of cardioprotection. Hearts treated by ischaemic postconditioning were subjected to six-10 second episodes of alternate myocardial ischaemia and reperfusion applied at the end of the 35 minutes ischaemic period. Treatment with ischaemic postconditioning did not reduce myocardial infarct size (mean 46.6 (SD 5.2)% in control hearts versus 41.0 (3.2)% in hearts treated with ischaemic postconditioning; n = 6 per group; p = NS), demonstrating failure of postconditioning to protect the diabetic heart. In addition, there was no difference in Akt phosphorylation between the two groups (42.6 (3.4) arbitrary units in control hearts v 35.1 (1.9) arbitrary units in hearts treated with ischaemic postconditioning; n = 6 per group; p = NS), suggesting impaired signalling through the PI3K-Akt pathway in the diabetic heart, given that previous studies in non-diabetic rat hearts had demonstrated enhanced Akt activation in postconditioned hearts.
In conclusion, the diabetic rat heart cannot be protected by ischaemic postconditioning which may be due to insufficient activation of Akt. Given the prevalence of diabetes in patients with ischaemic heart disease, the failure to ischaemic postcondition the diabetic rat heart may have important implications if this cardioprotective intervention is to be accepted as routine adjunctive therapy in the setting of primary percutaneous coronary intervention.
ishaemic postconditioning; diabetes; Akt

Abstract 262
263 PHARMACOLOGICAL REMODELLING OF HUMAN ATRIAL K+ CURRENTS BY CHRONIC BETA-BLOCKADE
G. Marshall1, A. Rankin1, K. Kane2, A. Workman1.1University of Glasgow, Glasgow, UK; 2University of Strathclyde, Glasgow, UK
Background: The chronic treatment of patients with a beta-blocker is associated with prolongation of the atrial action potential duration (APD), potentially contributing to its ability to prevent atrial fibrillation (AF). This may involve pharmacological remodelling of atrial K+ currents which affect APD.
Aims: To test the hypothesis that various characteristics of human atrial K+ currents, including voltage, time and rate dependency, differ between patients treated and not treated with a beta-blocker.
Methods: Myocytes were isolated enzymatically from right atrial appendage tissue obtained from consenting patients, in sinus rhythm, undergoing cardiac surgery. Currents were recorded by whole cell patch clamp at 35–37°C.
Results: Patients who received a beta1-selective blocker for at least 4 weeks immediately before surgery (n = 13) had a significantly lower heart rate than non beta-blocked patients (54 (SD 1) v 75 (4) beats/min, student’s t-test p<0.05, n = 15). Chronic beta-blockade was associated with a 41% reduction in the transient outward potassium current (ITO) density (9.3 (0.8) v 15.7 (1.1) pA/pF, p<0.05) and a reduction in the Ba2+ (0.5 millimolar)-sensitive, inwardly rectifying potassium current, IK1, at −120 mV (−1.7 (0.0) v −2.5 (0.2) pA/pF, p<0.05; n = 18–33 cells, 11–15 patients). The sustained outward current, IKSUS was unaffected (10 (0.6) v 11.4 (1.1) pA/pF, p>0.05). In cells from the non beta-blocked patients, the voltages for half maximal activation and inactivation of ITO were 24 (1) and −20 (1) mV, respectively, with corresponding slope factors of 9 (0) and 5 (0) mV. The decay of ITO was bi-exponential with fast and slow time constants of 6.8 (0.4) and 52.2 (6.3) ms. Reactivation was mono-exponential with a time constant of 31.4 (1.9) ms. None of the variables for voltage or time dependency were significantly different in cells from the beta-blocked patients. The density of ITO decreased significantly with increasing rate between 75 and 500 beats/min in both beta-blocked and non beta-blocked patient groups. Nevertheless, ITO density remained significantly reduced in beta-blocked patients at all rates studied, including 500 beats/min (3.5 (0.4) v 5.5 (0.8) pA/pF, n = 17–27 cells, 6–11 patients).
Conclusion: Chronic treatment of patients with a beta-blocker remodelled atrial K+ currents by reducing the densities of ITO and IK1, but not IKSUS. These changes may contribute to beta-blocker induced APD prolongation but the voltage, time and rate dependent characteristics of ITO do not. The preservation of ITO reduction at fast rates may contribute to the ability of beta-blockers to prevent AF.
Supported by BHF (FS/04/087)
beta-blockade; potassium currents; human atrial myocytes
264 INCREMENTAL VALUE OF TRANSIENT ISCHAEMIC DILATION OVER EXERCISE AND GATED SPECT MYOCARDIAL PERFUSION SCINTIGRAPHY VARIABLES FOR PREDICTING EVENT-FREE SURVIVAL IN TYPE 2 DIABETES
V. Dhakshinamurthy1, E. Lim1, U. Raval1, L. Shaw2, D. Lipkin1, A. Lahiri1.1Cardiac Imaging Centre, Wellington Hospital, London, UK; 2Cedars Sinai Medical Centre, Los Angeles, US
Background: Transient ischaemic dilatation (TID) is a marker of severe and extensive CAD which has been shown to be of prognostic value in the general population. We examined whether TID also had incremental prognostic value over exercise and gated SPECT myocardial perfusion scintigram (MPS) variables in patients with Type 2 diabetes.
Methods: Asymptomatic subjects with Type 2 diabetes and no history of coronary artery disease were studied. Gated SPECT MPS was performed on a 2 day protocol using dipyridamole stress and symptom-limited treadmill exercise. Perfusion was scored semi-quantitatively using a 17-segment model and the summed stress, rest and difference scores were calculated. The SDS was converted to percent myocardium ischaemic by dividing the SDS by 68 - the maximum potential score and multiplying by 100. LV volumes and ejection fraction were measured using automated programmes (Presence of TID was assessed visually by two independent, blinded expert readers. Subjects were followed up for a median of 2.2 years for the occurrence of cardiovascular events (myocardial infarction, stroke, death, late revascularisation).
Results: 180 subjects (mean age 53 years, 61% male) were studied. 57 (32%) had perfusion abnormalities, the majority of which were reversible (89%). TID was found in 30 patients (17%). 20 events occurred during follow-up. In a Cox proportional hazards survival model, the univariate predictors of survival were: extent of myocardial perfusion abnormality (p<0.0001), stress ESV (p = 0.023), stress EF (p = 0.002), rest EF (p = 0.045), stress and rest wall motion scores (p<0.0001 and p = 0.007 respectively). In a model stratified by ischaemic burden, the multivariate predictors were: TID (p = 0.018), Stress ESV (p = 0.028) and stress EF (p = 0.038). There was significant interaction between ischaemic burden and stress EF for prediction of event-free survival (table), for example in patients with LVEF<50% event-free survival was lowest in patients with >5% myocardial ischaemic burden.
Conclusion: TID has incremental value over exercise and gated SPECT MPS variables for predicting event-free survival in asymptomatic patients with Type 2 diabetic subjects.
Abstract 264
myocardial ischaemia; transient ischaemic dilation; prognosis
265 MYOCARDIAL PERFUSION MAGNETIC RESONANCE IMAGING FOR THE DETECTION OF MYOCARDIAL ISCHAEMIA AS DETERMINED BY PRESSURE WIRE DERIVED FRACTIONAL FLOW RESERVE
S. Watkins1, T. Steedman1, J. Lyne2, S. Frohwein3, J. Foster1, B. Groenning1, I. Ford4, H. Dargie1, K. Oldroyd1.1Western Infirmary, Glasgow, UK; 2Royal Brompton Hospital, London, U K; 3American Cardiovascular Research Institute, Atlanta, US; 4Robertson Centre for Biostatistics, Glasgow, UK
Introduction: First pass myocardial perfusion MRI for the detection of functionally significant coronary heart disease (CHD) has previously been validated by comparison with radioisotope perfusion imaging and/or quantitative coronary angiography (QCA). Neither of these techniques represents a true gold standard and in particular there is only an approximate relationship between angiographic parameters of lesion severity and functional significance. In previous studies, pressure wire derived fractional flow reserve (FFR) values <0.75 correlate with objective evidence of reversible ischaemia. Accordingly we have compared first pass perfusion MRI with FFR to determine the sensitivity, specificity, positive (PPV) and negative predictive values (NPV) of this technique.
Methods: Forty two patients with chest pain were referred for coronary angiography/intervention and underwent first pass perfusion MRI imaging in the week prior to angiography. This was performed on a Siemens Sonata 1.5Tesla scanner with perfusion imaging of 3 short axis slices obtained using a turboFLASH sequence (TI 90 ms, TE 0.99 ms, TR 173 ms, Flip Angle 8°, Matrix 80×128). Maximal hyperaemia was achieved using intravenous adenosine (140 µg/kg/min). The first pass bolus contained 0.1 mmol/kg of gadolinium power injected at 5 ml/sec followed by a 20 ml saline bolus. During coronary angiography the FFR was recorded in all patent major epicardial coronary arteries using a coronary pressure wire (RADI) with hyperaemia induced using intravenous adenosine as above. An FFR value of <0.75 was taken as the cut off for the diagnosis of significant CHD. MRI scans were analysed by a blinded independent experienced observer. QCA was performed for all major epicardial coronary arteries with stenoses ⩾70% being considered significant (Centricity CA1000, GE).
Results: Thirty two of 42 (76%) patients were male. The mean age was 59 years (SD = 9, Range 37–80). First pass perfusion MRI revealed 57 perfusion defects in 124 coronary artery segments (46%). Forty-four of these were confirmed to be physiologically abnormal with an FFR <0.75, giving a PPV of 77%. There were 67 normally perfused coronary artery territories, 64 of which had FFR <0.75 giving a NPV of 96%. The sensitivity of perfusion MRI for the detection of significant CHD was 94% and the specificity was 83%. In comparing perfusion MRI with QCA 27 territories with abnormal perfusion scans had a <70% stenosis giving a PPV of 53%. The sensitivity, specificity and NPV were 97%, 71% and 99%.
Conclusion: First pass perfusion MRI can detect significant CHD with good sensitivity, specificity, PPV and NPV when compared to FFR. Specificity and PPV are lower when compared to QCA. This adds support to the growing evidence for the use of this technique as a potential alternative to nuclear perfusion techniques.
coronary heart disease; first pass perfusion MRI; fractional flow reserve
266 CARDIOVASCULAR MAGNETIC RESONANCE MYOCARDIAL PERFUSION IMAGING: COMPARISON OF THREE SEQUENCES WITH PARALLEL ACQUISITION
J. Lyne, P. Gatehouse, R. Assomull, G. Smith, D. Firmin, D. Pennell.CMR Unit, Royal Brompton Hospital, London, UK
Introduction: CMR perfusion imaging has a number of advantages over existing techniques but the optimal pulse sequence for this application has not yet been determined. A direct comparison of the three main sequences for myocardial perfusion imaging is now warranted. Furthermore, utilisation of intergrated parallel acquisition techniques (IPAT) may reduce acquisition time, increasing myocardial coverage or spatial resolution but with a reduced CNR.
Methods: All studies were performed on a 1.5T MR scanner with a 12 element (6 anterior and 6 posterior coil elements) phased array coil. In 16 subjects we acquired first pass perfusion images (0.1 mmol/kg gadolinium DTPA) at rest and stress (iv adenosine infusion 140 mcg/kg/min for 4 minutes) with all three sequences, each on a separate occasion. The three sequences were set with approximately equivalent spatiotemporal resolution. Each sequence had an IPAT incorporated, hybrid echo planar imaging (HEPI) with TSENSE, steady state free precession (SSFP) with TSENSE and turbo fast low angle shot imaging (TFLASH) with GRAPPA. Within regions of interest the myocardial enhancement was calculated by dividing the difference between the peak and baseline signal intensity (average of four cycles) in the myocardium. We calculated the CNR of each scan by dividing the myocardial enhancement by the noise value for each scan. The noise value was calculated by switching off all radiofrequency pulses whilst acquiring 10 images. Two experienced blinded observers scored the presence and severity of artefacts, diagnostic confidence, transmurality and area of inducible perfusion defects.
Results: Greatest CNR was recorded with TFLASH-GRAPPA and least with the HEPI-TSENSE sequence (p<0.001). Most artefacts were recorded in the SSFP-TSENSE and least with HEPI-TSENSE (p<0.001). Observers were significantly more confident in reporting HEPI-TSENSE images (p<0.001) with no difference in transmurality or area of inducible hypoperfused myocardium with each sequence.
Conclusions: This study is the first direct comparison of the three main perfusion pulse sequences with utilisation of parallel acquisition techniques. This acceleration resulted in the ability to acquire 3 short axis slices in all subjects at both rest and stress with all three sequences such that the comparison is valid for clinically suitable ventricular sampling. The CNR of the TFLASH-GRAPPA sequence was higher than the TSENSE sequences probably due to the incorporation of coil reference data within the centre of k-space and magnification of noise within the TSENSE sequences from unwrapping of aliased images. However the greater effective acceleration of TSENSE and relatively short acquisition time with HEPI may suppress motion artefacts that would have lowered diagnostic confidence. Therefore HEPI-TSENSE despite a lower CNR appears likely to be the preferred perfusion sequence.
perfusion; CMR; pulse sequences

Abstract 266

Abstract 266
267 ASSESSMENT OF MYOCARDIAL SCAR; COMPARISON BETWEEN 18F-FDG PET, CMR AND 99TC-SESTAMIBI
A. Crean1, S. Khan2, L. Davies3, R. Coulden1, D. Dutka3.1Papworth Hospital, Cambridge, UK; 2Cardiovascular Medicine, Addenbrooke’s Hospital, Cambridge, UK; 3Addenbrooke’s Hospital, Cambridge, UK
Patients with heart failure and coronary artery disease may benefit from revascularisation if viable dysfunctional myocardium is present. The identification of viable versus scarred myocardium relies on imaging. In this study we have compared the utility of 3 commonly used imaging modalities in the detection of myocardial scar.
This prospective, descriptive study was carried out in a tertiary referral centre cardiac centre. 35 patients (29 male, average age 70 years) with coronary artery disease and at least NYHA class II heart failure underwent assessment of myocardial scar by 99Technetium-sestamibi (MIBI), 18F-flurodeoxyglucose (FDG) and cardiac magnetic resonance (CMR). The presence or absence of scar for each modality was compared using a 20 segment model.
More segments were identified as nonviable scar using MIBI than with FDG or CMR. FDG identified the least number of scar segments per patient (7.4 (SD 4.8) segments with MIBI, 5.8 (5.0) with CMR, 4.9 (4.2) with FDG, p = 0.0001 by ANOVA). This difference was present for all tertiles of ejection fraction. Overall levels of agreement were fair with kappa values of 0.56 to 0.69 but there was considerable variation depending upon the location of the scar. The strongest agreement between modalities was in the anterior wall with the weakest in the inferior wall.
Abstract 267
There is considerable variation amongst these 3 techniques in identifying scarred myocardium in patients with coronary disease and heart failure. Both MIBI and CMR identify more areas of scar when compared to FDG. We would not recommend MIBI as a sole method of imaging in patients undergoing myocardial viability assessment.
viability assessment; pet; cardiac imaging
268 BLOOD OXYGEN LEVEL-DEPENDENT MAGNETIC RESONANCE IMAGING IN PATIENTS WITH DYPIRIDAMOLE INDUCED ISCHEMIA; A PET COMPARATIVE STUDY
M. Egred1, G. Waiter2, T. Redpath2, S. Semple2, A. Al-Mohammad3, M. Norton2, M. Metcalfe4, S. Walton4.1Cardiothoracic Centre, Liverpool, UK; 2University of Aberdeen, Aberdeen, UK; 3Northern General Hospital, Sheffield, UK; 4Aberdeen Royal Infirmary, Aberdeen, UK
Background: Blood oxygen level dependent (BOLD) MRI relies on changes in deoxyhaemoglobin level in tissues under stress for signal variation and may be used for detection of ischaemic myocardium.
Methods: 15 patients with stress induced myocardial ischemia on PET scanning underwent rest and dipyridamole stress MRI using a double breath hold T2* weighted, ECG gated sequence to produce BOLD contrast images, and cine-MRI for wall thickening assessment. Signal change on BOLD MRI and wall thickening were compared between rest and stress images in ischaemic and non-ischaemic myocardial segments.
Results: Using PET, 156 segments were identified with reversible ischemia and 324 as non-ischaemic. The ischaemic segments were found on BOLD MRI to have an average signal change between rest and stress of −16.7 % compared to −14% in the non-ischaemic segments (p = 0.04). The average wall thickening was 7.8 mm in the ischaemic segments compared with 9.5 mm in the non-ischaemic segments (p<0.0001).
Conclusion: BOLD MRI with wall thickening assessment may differentiate ischaemic from non-ischaemic myocardium in patients with stress induced myocardial ischemia. Larger studies with improved spatial resolution may establish its potentials, help define a threshold for detection of ischaemia, as well as determine the technique’s sensitivity and specificity.
BOLD magnetic resonance imaging; positron emission tomography; coronary arrtery disease
269 STATIN TREATMENT RAPIDLY REDUCES AORTIC ATHEROSCLEROSIS AND IMPROVES VASCULAR FUNCTION: A CARDIOVASCULAR MAGNETIC RESONANCE STUDY
J. Lee, C. Shirodaria, J. Francis, C. Jackson, M. Robson, C. Leeson, S. Neubauer, K. Channon, R. Choudhury, F. Wiesmann.1Department of Cardiovascular Medicine, University of Oxford, Oxford, United Kingdom
Introduction: Cardiovascular magnetic resonance (CMR) can non-invasively assess vascular structure and function with excellent spatial and temporal resolution. Statin treatment rapidly improves endothelial function and also reduces plaque size, assessed by CMR after 6–24 months. However, the relationship between structural and functional changes and their relative timings are not well established. We hypothesised that improvement in vascular function following statin initiation would precede and predict regression of atherosclerosis, providing an early measure of treatment response.
Methods: 34 newly diagnosed coronary artery disease patients underwent imaging at 1.5 Tesla before as well as 3 and 12 months after commencing statins. Aortic distensibility (relative change in cross-sectional area per mm Hg of pulse pressure) was measured using trueFISP cine (in plane resolution 2 mm, temporal resolution approx. 50 msec). For endothelial function, brachial artery flow mediated dilatation or FMD (maximum relative change in area during postischemic hyperemia) and maximum response to 400 mcg sublingual glyceryl trinitrate (GTN) was measured using trueFISP cine. Transverse black blood turbo spin echo images of the descending thoracic aorta were acquired to quantify vessel wall area (in plane resolution 0.8 mm).
Results: All patients received statin treatment (>80% simvastatin 40 mg daily). Mean total cholesterol was 5.30 (SD 0.17) mmol/L at baseline, 3.92 (0.12) mmol/L at 3 months and 4.00 (0.14) mmol/L at 12 months. Mean aortic wall cross sectional area decreased by 2.5% at 3 months and by 5.4% at 12 months (fig. 1a). Mean aortic lumen area remained stable throughout (p = NS between timepoints) implying that regression of atherosclerosis involves reversal of positive remodelling. Significant (p<0.05) increases in distensibility of the ascending (AA), proximal descending (PD) and distal descending (DD) aorta respectively occurred after 3 (and 12) months of 39% (46%), 37% (58%) and 28% (72%) (fig. 1b). Mean brachial artery FMD response improved from 8.1% to 12.8% (p<0.003) at 3 months and 13.7% at 12 months (p<0.001). Response to GTN did not change significantly. Importantly changes between 0 and 3 months were strongly correlated with changes between 0 and 12 months, for aortic distensibility (r = 0.55, p<0.01), FMD (r = 0.49, p<0.05) and aortic wall area (r = 0.77 p<0.001).

Abstract 269
Conclusions: Using only 34 patients CMR detected significant changes in aortic atherosclerosis and distensibility, and brachial artery FMD within 3 months of starting a statin. 3 month changes correlate well with 12 months, suggesting that ‘pan-vascular’ assessment with MRI may allow early quantification of response to treatment.
statin; atherosclerosis; endothelium
270 ASSESSMENT OF LEFT VENTRICULAR ABNORMALITIES IN MILD-MODERATE CHRONIC KIDNEY DISEASE
N. Edwards, C. Ferro, J. Townend, R. Steeds.1University Hospital Birmingham, Birmingham, UK
Background: Premature cardiovascular disease is a major cause of mortality among patients with chronic kidney disease (CKD). A near linear relationship exists between the rate of cardiovascular events and severity of renal function below a glomerular filtration rate (eGFR) of 81 mls/min. Approximately 80% of patients with end-stage CKD have left ventricular (LV) abnormalities (uraemic cardiomyopathy) on echocardiography and late gadolinium enhancement (LGE) indicative of infarction or fibrosis has been documented in 29% of dialysis patients on cardiac magnetic resonance (CMR). Despite the established increased CV risk with milder forms of CKD, the time of onset of LV abnormalities synonymous with uraemic cardiomyopathy remains unclear.
Methods: Forty patients (median age 58 years [range 35–78]; males 58%), with mild (eGFR 60–80 mls/min) or moderate (eGFR 40–59 mls/min) CKD secondary to non-diabetic renal disease and 10 normotensive age matched controls, all with no known history of cardiovascular disease were prospectively studied. Patients underwent ECG and 24 hour ambulatory blood pressure monitoring. Left ventricular geometry, function and myocardial gadolinium (Gd) uptake was assessed with standard CMR techniques. Inversion recovery images were performed at 10–15 minutes after 0.2 mmol/Kg Gadolinium-DTPA (Magnevist) injection.
Results: All patients and controls had normal ECG. Patients with mild CKD (58%) had mean 24 hour ambulatory BP of 122/74 (range systolic 138–101, diastolic 85–63) and moderate CKD (42%) 123/74 (range systolic 140–101, diastolic 90–52). Data was indexed to body surface area (BSA m2). Ten patients (5 mild CKD, 5 moderate CKD) had an increased LV mass index (LVMI) above reported normal gender-specific limits and were significantly increased compared with controls (mean male LVMI 69 g/m2, female LVMI 60 g/m2) (p<0.001). Mean LVMI in males with LV hypertrophy (LVH) was 88 g/m2 (range 84–93) and females 79 g/m2 (range 71–90). Left ventricular dimensions and function were within gender specific limits for all patients and controls. late gadolinium hyper-enhancement (LGE) was present in two patients, one with mild CKD had discrete subendocardial LGE consistent with previous infarction and one with moderate CKD had diffuse midwall LGE similar to that seen in late ESRD and DCM.
Conclusion: Left ventricular hypertrophy with preserved ventricular function was evident in a quarter of patients with mild-moderate CKD despite excellent blood pressure control. We speculate that LVH develops early in the course of CKD in response to stimuli other than BP alone. The presence of LGE in this cohort suggests that myocardial fibrosis/infarction is not limited to a dialysis population as previously described. Further studies are required to define the development LV abnormalities with progressive renal disease which might allow targeted primary prevention therapies.
cardiac magnetic resonance ; chronic kidney disease; Left ventricular hypertrophy
271 INSIGHTS INTO CARDIAC AND VASCULAR REMODELLING IN ATHLETES BY MULTI-MODAL MAGNETIC RESONANCE IMAGING
S. Petersen, S. Neubauer, K. Channon.1John Radcliffe Hospital,Department of Cardiovascular Medicine,University of Oxford, Oxford, UK
Introduction: Oestrogen has an anti-proliferative and testosterone a proliferative stimulus in situations of cardiac pathological remodelling. However, little data exist for sex-specific effects on chronic physiological remodelling. We studied young adult elite athletes with age-and sex-matched sedentary controls to assess sex-specific differences for LV and RV dilatation and hypertrophy as well as for LV contraction and relaxation. Physical activity has well-known beneficial effects on vascular function in subjects with endothelial dysfunction. We hypothesised that structural and functional adaptive changes to chronic physiological cardiac remodelling would be sex-specific. Furthermore, we sought to determine whether exercise training in healthy young adults is associated with vascular remodelling and functional evidence of desensitised vascular NO signalling.
Methods: Elite athletes and age-sex matched sedentary controls underwent cardiovascular MR imaging (1.5 Tesla). LV and RV volumes and mass were determined using steady state free precession cines. Contraction and relaxation was assessed using cine phase contrast velocity MR imaging. We used high-resolution non-invasive MR imaging to provide detailed characterisation of vascular function and structure, including endothelial-dependent and independent brachial artery dilation, and quantification of central and peripheral arterial distensibilities.
Results: Male and female athletes showed similar increases in LV and RV volume and mass indices when compared to controls (ranging between 15 and 42%). No sex-specific differences in training effect on LV and RV volumes, mass indices and ejection fractions, or LV to RV ratios of these volume and mass indices (parameters of balanced LV and RV dilatation and hypertrophy) were observed (all p for interaction >0.05). Similarly, no sex-specific differences in training effect on cardiac contraction and relaxation were found (all p for interaction >0.05). Vessel distensibilities (mm Hg-1) were similar for elite rowers when compared to sedentary controls at the level of the ascending, proximal and descending aorta, the carotid artery and the brachial artery (p >0.05 for all). Endothelial-dependent dilation (%) was similar for rowers and controls (p>0.05), but rowers showed reduced endothelial-independent dilation (rowers: 25 (SD 14)% v controls: 52 (18)%, p = 0.015).
Conclusions: Adaptive structural and functional changes to exercise training in young adult elite athletes are not sex-specific. This is in accordance with the benign nature of the hypertrophy associated with athlete’s heart. Young elite rowers demonstrate normal endothelial-dependent, but reduced endothelial-independent dilation, likely reflecting smooth muscle cell desensitisation to nitric oxide. Chronic, whole body, combined endurance-and strength-training does not lead to changes in arterial stiffness, but to vascular remodelling.
exercise; magnetic resonance imaging; remodelling
272 SHORT-TERM FOLIC ACID TREATMENT IMPROVES CENTRAL AND PERIPHERAL VASCULAR FUNCTION IN PATIENTS WITH CORONARY ARTERY DISEASE - A CARDIOVASCULAR MAGNETIC RESONANCE STUDY
C. Shirodaria1, J. Lee1, C. Antoniades1, C. Jackson1, M. Robson1, J. Francis1, S. Moat2, C. Ratnatunga3, R. Pillai3, S. Neubauer1, K. Channon1.1University of Oxford, Oxford, UK; 2University of Wales, Cardiff, U K; 3John Radcliffe Hospital, Oxford, UK
Background: Homocysteine (Hcy) is an independent predictor of cardiovascular events. Folic acid 400 mcg daily significantly lowers plasma Hcy, but only daily doses of 5 mg and above have been shown to improve endothelial function using brachial artery ultrasound. The effects of folic acid on central arterial function are unknown. High-resolution magnetic resonance imaging allows quantification of vascular function at both central and peripheral sites within the vascular tree during one examination.
Purpose: To test the hypothesis that early changes in arterial function occur with low and high dose folic acid treatment, and that these changes could be assessed accurately and non-invasively using magnetic resonance imaging (MRI).
Methods: In a double-blind placebo-controlled trial, 56 patients with coronary artery disease (mean age 63 (SD 1) y) were randomised to receive folic acid 400 µg/d (n = 20), folic acid 5 mg/d (n = 22), or placebo (n = 14). Non-invasive high-resolution cine MRI at 1.5 Tesla was performed to assess distensibility of the aorta (ascending, proximal descending and abdominal) and carotid arteries (CA) before and after 6 weeks treatment. Distensibility was measured as the relative change in cross-sectional area per mm Hg of pulse pressure. Flow-mediated dilatation (FMD) was measured as the maximum relative change in brachial artery area during post-ischemic hyperemia.
Results: Hcy levels were similarly decreased after treatment with folic acid 400 µg daily (13.0 µmol/l to 11.4 µmol/l, p<0.05) or 5 mg daily (13.7 µmol/l to 11.6 µmol/l, p<0.01) and were unchanged with placebo (15.0 µmol/l to 14.4 µmol/l, p = 0.36). Aortic distensibility was significantly improved in ascending ((1.84 (0.33) to 1.8 (0.33) 10−3 mm Hg−1 (p = 0.82) with placebo, 1.5 (0.23) to 2.0 (0.23) 10−3 mm Hg−1 (p<0.01) with 400 µg, 1.9±0.31 to 2.4±0.35 10−3 mmHg−1 (p<0.05) with 5 mg), proximal descending (figure 1) and abdominal segments (mean 3.8 (SD 0.63) to 3.5 (0.53) 10−3 mmHg−1 (p = 0.22) with placebo, 3.0 (0.33) to 3.7 (0.27) 10−3 mm Hg−1 (p<0.05) with 400µg, 3.3 (0.43) to 4.3 (0.41) 10−3 mm Hg−1 (p<0.05) with 5 mg) after daily treatment with both folic acid 400 µg and 5 mg, but not with placebo. Carotid distensibility was also improved in both folic acid groups but not in the placebo group (figure. 1). Similarly, FMD was increased in both the 400 µg and 5 mg groups but not in the placebo group (figure 2).

Abstract 272
Conclusion: Both low and high dose folic acid improve arterial distensibility and endothelial function as quantified by MRI. These beneficial actions on vascular structure and function suggest that folic acid treatment may be a promising therapeutic opportunity in patients with coronary artery disease.
MRI; folic acid; endothelium
273 A PREOPERATIVE CARDIAC RISK INDEX SCORE TO STREAMLINE CARDIOLOGY REFERRALS AND INCREASE BETA-BLOCKADE USE IN HIGH-RISK PATIENTS UNDERGOING NON-CARDIAC SURGERY
K. Soulsby, L. Hudsmith, J. Bell, K. Luxton, C. McKenna, W. Orr.Department of Cardiology, Royal Berkshire Hospital, Reading, UK
In non-cardiac surgery, cardiovascular morbidity and mortality represents 45% of all perioperative complications (NCEPOD). Medical optimisation of high-risk patients should greatly minimise risk. Assessment of these patients is now a significant part of cardiology practice as an increasingly elderly population undergo elective surgery.
Method: (Audit 1) Notes of 85 orthopaedic patients referred for preoperative cardiology assessment reviewed retrospectively for age, reason for referral, type of surgery planned, investigations performed and treatment instituted. Using currently available evidence, a Cardiac risk index score (CRIS) was developed:
(Audit 2) Pilot study of CRIS system run prospectively in orthopaedic theatres. All patients assessed on day of operation for CRIS, beta-blocker use, and senior anaesthetist’s assessment of risk and need for cardiology review.
Results: Audit 1 89% patients >65 years. Referrals for assessment of ischaemic heart disease 35 %, valvular disease 24 %, arrhythmias 20 % or heart failure 12 %. High investigation rates (echo 59% and angiography 16%). Only 25% patients beta-blocked. Audit 2 78 prospective cases assessed using CRIS. 6.5% scored >10 indicating need for referral: anaesthetic agreement in 4/5 cases. 19% scored 5–9, indicating need for perioperative beta blockade but not referral: only 6/15 had been beta blocked.
Discussion: There is a high level of cardiovascular risk in patients presenting for elective surgery. This study demonstrates the potential utility of a simple risk scoring tool to optimise preoperative care, reducing unnecessary referrals, increasing the use of beta-blockers in those likely to benefit, and ensuring rapid cardiological referral highest risk patients. This is likely to reduce the cardiovascular risk of non-cardiac surgery and prevent long waiting times and frequent last-minute cancellations.
peri-operative care; non-cardiac surgery; risk score

Abstract 273
274 CLOPIDOGREL AND THE RISK OF NON-CARDIAC SURGERY: AN AUDIT OF ANAESTHETISTS AND SURGEONS UNDERSTANDING
L. Hudsmith1, J. De Bono2, K. Luxton2, C. Mckenna2, P. Foex3, W. Orr2.1Department Of Cardiology, The Royal Berkshire Hospital, Reading, U K; 2Department Of Cardiovascular Medicine, The John Radcliffe Hospital, Oxford, U K; 3Nuffield Department of Anaesthetics, The John Radcliffe Hospital, Oxford, UK
Background: Dual antiplatelet therapy is used in almost all patients now treated for acute coronary syndrome or undergoing percutaneous coronary intervention with stents. Major concerns exist about these patients if they subsequently require non-cardiac surgery and there are few data and no clinical guidelines available to guide management decisions. Continuing clopidogrel is likely to lead to increased bleeding but premature cessation increases the risk of major ischaemic events.
Method and Results: Anonymous questionnaire sent to anaesthetists and non-cardiac surgeons in 2 large acute trusts. 80 replies analysed (41 anaesthetists and 39 surgeons, 90% consultants). All had treated patients taking aspirin and 51% had experienced bleeding complications which they attributed to it. 76% had treated patients who were taking clopidogrel at the time and 39% of these had experienced bleeding problems, 29% life-threatening but no reported deaths. 73% (95% of anaesthetists) would avoid or modify emergency procedures if the patient was taking clopidogrel but only 10% have used drugs and blood products to try to reverse its effect. 54% (80% of anaesthetists) would not use spinal anaesthesia in this group and many have experienced major post-op problems with analgesia. For elective surgery, clopidogrel is stopped 0–28 days pre-operatively (median 7 days) and most would also stop aspirin (0–14 days, median 4 days). There was great variation in re-starting clopidogrel post-procedure and uncertainty about the increased thrombotic risks with different types of stents.
Conclusions: Aggressive antiplatelet therapy is increasingly used in a wide spectrum of patients with coronary disease and strongly supported by NICE guidelines. Anaesthetists and non-cardiac surgeons are uncertain about best practice when treating these patients. Cardiologists need carefully consider stent choice in patients potentially facing non-cardiac surgery, and be clear about the indications and timing of treatment with clopidogrel as well as the likely risks of early or temporary cessation of therapy. Though the evidence-base is thin, clinical guidelines are urgently required.
clopidogrel; non-cardiac surgery; audit
275 PROLONGED COMBINATION ANTI-PLATELET THERAPY IS IMPRACTICAL IN MANY SUBJECTS - A 1000 PATIENT REAL WORLD EXPERIENCE
H. Mirjafari, P. Saravanan, B. Prendergast.Wythenshawe Hospital, Manchester, UK
Introduction: Prolonged combination therapy with aspirin and clopidogrel reduces major adverse cardiac events (MACE) following percutaneous coronary intervention (PCI), particularly in patients who receive drug eluting stents. However, the practicality and potential adverse effects of such treatment in routine clinical practice are currently unknown.
Methods: We identified 1000 consecutive patients who underwent PCI between June 2003 and May 2004 in whom a routine 12 month course of aspirin and clopidogrel was recommended. Questionnaire followup through their GP determined compliance with the anti-platelet regime and the incidence of MACE and/or major/minor bleeding.
Results: The response rate was 61% describing outcome in 424 males and 181 females (mean age 62 yrs, range 32–86 years). 455 patients (76%) completed the 12 month course (group A) and compliance was incomplete in 150 (24%, group B) for reasons that remained largely unclear in 108 (72%). Overall MACE was lower in group A with a significant reduction in cardiac cause of death (table 1), and prolonged combination had no impact on major or minor bleeding (table 2). Sub-group analysis demonstrated worse compliance in the elderly (>65 yrs) with higher incidence of MACE, and, both major and minor bleeding (table 3).
Abstract 275 Table 1
Abstract 275 Table 2
Abstract 275 Table 3
Discussion: Prolonged regimes of combination anti-platelet therapy are frequently recommended following PCI. These data demonstrate the clinical benefit of such treatment with acceptable risk profile, though highlights the issue of poor compliance despite clear patient education and advice. Adverse outcomes in the elderly population were associated with particularly poor compliance. Use of bare metal stents allowing abbreviated regimes of combination anti-platelet therapy may be a more appropriate clinical strategy in this group.
antiplatelet therapy; major adverse cardiac events ; bleeding
276 PREDICTING SERIOUS UPPER GASTRO-INTESTINAL BLEEDING AFTER PERCUTANEOUS INTERVENTION
P. Foley1, R. Anderson2, I. Simpson1.1Wessex Cardiac Centre, Southampton, UK; 2University Hospital of Wales, Cardiff, UK
Introduction: Gastrointestinal bleeding (GIB) after percutaneous intervention (PCI) is a difficult management problem as anti-platelet therapy is regarded as contraindicated in patients with active bleeding, but is essential to avoid stent thrombosis. This therapeutic dilemma is best avoided by, if possible, preventing gastro-intestinal bleeding. The aim of this study was to determine its incidence immediately after PCI, evaluate the importance of previous GIB and how anti-platelet therapy was managed.
Methods: Patients were retrospectively identified from a database of 5226 patients undergoing PCI at a single institution over a four year period. Patients who experienced GIB or requiring blood transfusion were identified, and their medical records reviewed. The primary outcomes were death, transfusion requirement, length of stay. We determined the management of glycoprotein IIbIIIa antagonists and oral anti-platelet therapy.
Results: Six patients had gastrointestinal bleeds over the four year period, the mean age was 63.5. PCI was performed for failed thrombolysis (2), electively (2), (1) primary PCI (on warfarin) and for a non-ST elevation myocardial infarct (1). No patients had renal failure, mean creatinine 108. There was no previous history of GIB. All patients received abciximab. In all cases GIB occurred within 48 hrs of PCI. The mean blood transfusion requirement was 2.7 units. 2 patients had platelet infusions to reverse anti-platelet therapy. All patients 6 received a proton pump inhibitor (PPI) after GIB. 4 patients underwent therapeutic gastroscopy without complication. The causes of GIB were angiodysplasia, benign DU, oesophageal veins and pre-pyloric ulcer. Aspirin was stopped in 1 case and withheld in 3 for a mean of 3 days. Clopidogrel was continued in all but one case. There was no clinical rebleeding, acute stent thrombosis or deaths. The mean length of stay after PCI was 13 days (5 patients). One patient required further investigation of ventricular tachycardia.
Conclusions: GIB is rare after PCI. We found that neither a previous history of gastrointestinal bleeding nor renal impairment were helpful in identifying the at risk patients. However, it is interesting that all patients had received abciximab and the site of bleeding was varied. Patients who experienced GIB had a prolonged length of stay in hospital and required considerable blood product transfusion.
gastrointestinal bleeding; percutaneous intervention; anti-platelet therapy
277 RECOGNITION OF ATRIAL FIBRILLATION IN PACE MAKER POPULATION
I. Ahmad, T. Hammond, D. Pitcher, A. Scriven.Worcestershire Royal Hospital, Worcester, UK
Introduction: In patients with permanent pacemakers (PPM), the onset of atrial fibrillation (AF) may be unrecognised because the cardiac rhythm remains regular. The majority of UK PPM clinics are technician led and directed towards the assessment of pacemaker function. The incidence of AF increases with age, and the majority of the PPM population is older and at risk of chronic or paroxysmal AF, and thromboembolic complications (CVE). We prospectively assessed PPM patients to identify new onset paroxysmal and chronic AF since pacemaker implant. Using a questionnaire, we also attempted to determine whether UK PPM clinics use a systematic or protocol driven approach to diagnose underlying AF in their PPM population and to take appropriate action.
Methods: Patients were prospectively assessed during routine PPM review. Cardiac rhythm was assessed by 12-lead ECG and interrogation of pacemaker diagnostics. Data was also collected for (1) type of pacemaker eg : VVI/DDD/AAI (2) cardiac rhythm at implant (3) current cardiac rhythm (4) pacemaker mode switching (5) current antithrombotic/anticoagulant therapy and (6) thromboembolic events.
Results: Out of 397 patients M = 203/F = 194 (age range 35–101 years, majority 63–91 years).
DDD group: 262 patients had DDD pacemaker and were in sinus rhythm at implant. 47 (18%) of these developed new chronic AF.
VVI group: 113 patients had VVI pacemaker. 65 (58%) were already in AF at the time of implant, and 23 patients had new onset of chronic AF.
Abstract 277 Table 1
DDD group with mode switching: In a sub-group analysis of the DDD group, although this group did not develop AF as such but 91 patients were noted to have mode switching. We divided this group according to the percentage of time they stayed in abnormal rhythm:
-
<5%: 82 patients (91%), 13 (15%) of them had CVE.
-
5–10%: out of 4 (4%) none had CVE.
-
11–24%: out of 3 (2%) 1 had a CVE.
-
25–50%: out of 2 (4%), 1 had a CVE.
Abstract 277 Table 2
Overall out of total 91 patients (range <1%–50%), 17 (19%) were on warfarin, 74 (81%) were not on warfarin. 15 patients (16%) had CVE.
This group was compared with the remaining 124 patients in DDD group who neither developed chronic AF nor demonstrated mode switching and 6 had a CVE (6.5%). The result was statistically significant with p value = <0.05 (Mode switch group v Non mode switch group).
Questionnaire: Of 200 UK pacemaker clinics surveyed by questionnaire, 95 responses received suggests that 66% of clinics has no written protocol for detecting and highlighting these patients.
Conclusion: New onset AF is common in a PPM population, and may not be recognised unless specific diagnostic measures are taken. In addition, Paroxysmal AF may be present when pacemaker diagnostic records indicates pacemaker mode switching. Our data shows a significantly higher prevalence of CVE in the group with evidence of mode switching.
atrial fibrillation in patients with permanent pacemakers ; CVE in patients with permanent pacemakers ; mode switching
278 DEPRESSION AS AN AETIOLOGIC AND PROGNOSTIC FACTOR IN CORONARY HEART DISEASE: A META-ANALYSIS OF 6608 EVENTS AND 150217 PARTICIPANTS IN 63 OBSERVATIONAL STUDIES
A. Nicholson1, H. Kuper2, H. Hemingway1.1University College London, London, UK; 2London School of Hygiene and Tropical Medicine, London, UK
Background: The role of depression as an aetiological or prognostic factor in coronary heart disease (CHD) remains controversial, particularly in the light of two negative randomised controlled trials.
Objectives: To quantify the effect of depression on CHD etiology and prognosis and assess the extent of confounding by coronary risk factors and reverse causality.
Methods: Meta-analysis of prospective cohort studies measuring depression with follow up for fatal CHD and incident myocardial infarction (aetiological) or all cause mortality/fatal CHD (prognostic). We searched MEDLINE and Science Citation Index until December 2003.
Results: In 24 aetiological studies (131 497 patients, mean follow-up 10.9 years) the random effects pooled relative risk of future CHD associated with depression was 1.76 (95% CI 1.51 to2.05). Only 13 studies reported both unadjusted and adjusted results, and adjustment often omitted established risk factors. These adjustments reduced the crude effect from 1.91 (1.57 to 2.34) to 1.77 (1.41 to 2.22). In 39 prognostic studies (18720 patients, mean follow up 2.8 years), the random effects pooled relative risk was 1.76 (1.50 to 2.07). Only 10 studies reported adjustment for left ventricular function or other marker of the severity of coronary disease; and this attenuated the relative risk from 2.04 to 1.45 (1.14 to 1.84), a 48% reduction. In both aetiological and prognostic studies, papers which did not report adjusted results had lower unadjusted effect sizes than those which did report adjusted results.
Conclusions: Depression has not been established as an independent risk factor for developing or dying from CHD because of incomplete and biased reporting of adjustment for conventional risk factors and the severity of coronary disease.
meta-analysis; depression; coronary heart disease
279 RADIATION DOSES TO THE SHIN AND HEAD IN INVASIVE CARDIOLOGY; IS ADDITIONAL PROTECTION NECESSARY
K. Taylor1, B. Epps2, R. Butler2.1Keele University, Stoke on Trent, UK; 2University Hospital of North Staffordshire, Stoke on Trent, UK
Aim: Cardiologists receive a considerable radiation dose during invasive cardiac catheterisation procedures. This pilot study investigates whether significant radiation to the head and shin bones exists; which may increase the stochastic and deterministic radiation exposure risks. Stochastic risks include tumour genesis and genetic damage, where the risk of damage is proportional to the exposure, but the manifestation of the effect is all or nothing (you do not get a worse osteosarcoma because of additional x ray dose). Deterministic effects are those where the effect is proportional to dose such as radiation sickness or cataract.
Cataracts, brain tumours, osteosarcomas and haematological malignancy are all potential consequences in cardiologist, with excessive exposure to head and shin.
Methods: The accumulated radiation dose was measured using thermoluminescent dosimeters (TLD) secured to these thyroid, waist, both shins and circumferentially around the head. Three operators did not wear lead lined shin pads and two did. All wore the circumferential headband. Monitoring was carried out over a seven week period by KT. All procedures by each operator were included. The TLD exposure were calibrated and normalised to the sum of dose area product/time (ΣDAPt) over time, an index of workload.
Standard x ray protection techniques such as keeping the image intensifier as low as possible, short acquisition runs and utilising the mobile shielding.
Results: The radiation dose was recorded for TLD on a circumferential headband, with 0° at the back and 90° at the right hand side, and on the shins with operators A and E wearing shin guards under which the TLD were placed.
Abstract 279
The radiation dose to the head follows a trend according to the relation of each aspect to the source of the radiation (figure 1), with the highest mean RD of 492 ìGy at 270°
Abstract 279

Abstract 279
Multiplying this by the coefficient 0.2 gives a mean RD to the brain of 100 ìGy. The mean RD to the exposed shins 4461 ìGy and 1852 ìGy, to the left and right respectively, was markedly different to 87 ìGy and 53 ìGy to the protected shins (figure 2). The mean annual brain RD was 744 ìSv however there is no established risk coefficient for adult radiation-induced brain cancer.

Abstract 279
Discussion: Radiation exposure is of critical importance to staff and patients alike, and it is important to attempt to keep the dose as low as reasonably achievable (ALARA). We currently utilise standard x ray shielding, but feel this does not go far enough. The vivid images of calf depilation from cardiologists is Blackpool published recently in HEART is an example of the effects of x ray exposure.
We plan to follow this work with a further study to confirm the effectiveness of lead lined shin pads, lead glasses and skull caps when combined with effective use of standard protection.
radiation protection; catheter lab; x ray
280 A CARDIOLOGY ON-CALL ROTA IN THE DISTRICT GENERAL HOSPITAL - IS IT WORTH IT?
I. Mahy1, C. Parnell1, C. Carey1, P. Keeling1, G. Gribbin1, S. Shaw2.1Torbay Hospital, Torquay, UK; 2University of Plymouth, Plymouth, UK
Introduction: Many District General Hospitals (DGH) are not able to provide continuous specialist-based cardiology cover. Patients with acute coronary syndromes (ACS) are initially cared for by a general physician and then passed on for continuing care. Delays in specialist input are particularly likely for patients admitted at a weekend. It is uncertain whether this variation in care affects outcomes.
In July 2004 the cardiology on-call rota at our large DGH was separated from the general medical ‘take’ rota and routine weekend cardiology ward rounds were introduced. Patients with ACS now come directly under the care of a cardiologist irrespective of the day of admission.
Methods: Audit data collected before and after the change enabled coincident changes in patient outcome to be assessed. Data was analysed for all patients with a final diagnosis of myocardial infarction (NSTEMI or STEMI) during the period July 2002 to July 2005. Main outcome measures were hospital length of stay, in-hospital mortality and variation in mortality according to day of admission.
Results: For the 3 years a total of 1967 patients (708 female, mean age 72.6 years) were identified, of whom 258 died in hospital. Following introduction of the on-call cardiology service there was a fall in hospital length of stay (median 7.0 days (range 1–80) v 5.0 (1–122), p = 0.016). Total in-hospital mortality did not alter significantly (13.6% v 11.8%, ns). However, when patients admitted during the week were analysed separately from those admitted at weekends there was a small excess mortality for the weekend group prior to the new rota, but not afterwards, due to a fall in mortality for patients admitted at weekends after July 2004 (15.6% v 9.1%, p = 0.02).
Conclusion: Introduction of a seven day cardiology service at our hospital has been associated with a reduction in length of stay for patients with ACS. In this study temporal changes in patient outcomes are consistent with previous data suggesting that patients with acute coronary syndromes benefit from early specialist care.
audit; acute coronary syndromes; mortality
281 NATIONAL 30-DAY ACUTE CORONARY SYNDROMES MORTALITY: USING THE EMMMACE RISK MODEL TO ADJUST FOR DEATH RATES
C. Gale1, S. Manda2, A. Hall1.1Academic Unit of Cardiovascular Medicine, Leeds General Infirmary, Leeds, UK; 2Centre for Epidemiology and Biostatistics, University of Leeds, Leeds, UK
The EMMACE risk model uses patient age, admission heart rate and systolic BP to adjust mortality rates in patients with acute coronary syndromes (ACS) by case mix. We evaluated this model nationally using the MINAP database. 176 963 unique patient entries were studied by discharge diagnosis.
Total 30-day mortality was 10.2% (1-year = 17%). Overall probability of death by 30 days (P30) was 1/(1+exp (-L30) and L30 = −6.057+(0.072 × age)+(0.010 × heart rate) − (0.017 × systolic BP) and differed only modestly from the EMMACE model.
Areas under the receiver operating characteristic curves confirmed the performance of the original (C index, 95% CI: 0.774, 0.769 to 0.778) and recalibrated (C index, 95% CI: 0.776, 0.771 to 0.781) EMMACE models. The best performance was observed for a discharge diagnosis of ‘chest pain of uncertain origin’ (original EMMACE model, C index, 95% CI: 0.830, 0.753 to 0.908; recalibrated model, 0.841, 0.766 to 0.916) and worst for ‘unconfirmed MI’ (original EMMACE model, C index, 95% CI: 0.739, 0.693 to 0.785; recalibrated model, 0.733, 0.690 to 0.783).
This analysis demonstrates that the EMMACE risk model can be applied nationally to subcategories of ACS populations to form the basis of a simple indicator of standard of care in disparate centres as well as consecutive individual patients and allows case mix adjustment of 30-day mortality rates for ACS.
acute coronary syndrome; mortality; EMMACE
282 5-METHYL-TETRAHYDROFOLIC ACID INCREASES NITRIC OXIDE BIOAVAILABILITY AND DECREASES SUPEROXIDE PRODUCTION BY IMPROVING ENOS COUPLING IN HUMAN VESSELS IN VIVO: EFFECTS ON INTRACELLULAR TETRAHYDROBIOPTERIN OXIDATION
C. Antoniades1, C. Shirodaria1, P. Leeson1, J. Lee1, N. Warrick1, C. Ratnatunga2, R. Pillai2, K. Channon1.1University of Oxford, Cardiovascular Medicine Department, John Radcliffe Hospital, Oxford, UK; 2John Radcliffe Hospital, Department of Cardiothoracic Surgery, Oxford, UK
Background: Uncoupled endothelial nitric oxide synthase (eNOS) appears to be a source of superoxide radicals (SOO) in human atherosclerosis. We hypothesised that 5-methyl-tetrahydrofolic acid (5MTHF), the active metabolite of folic acid, may improve eNOS coupling by preventing the intracellular oxidation of eNOS cofactor tetrahydrobiopterin (BH4).
Methods: Fifty-six patients undergoing coronary artery bypass graft (CABG) were randomised to receive intravenous bolus 5MTHF (0.13 mg/kg of body weight, n = 24) or placebo (n = 32) preoperatively, 45 minutes before graft harvesting. Vascular superoxide production was determined in paired samples of human saphenous veins (HSV) and internal mammary arteries (IMA) using 5µM lucigenin chemiluminescence, in the presence or absence of NOS inhibitor L-NAME. Vasomotor responses to acetylcholine (ACh) and nitroprusside (SNP) were determined by organ bath isometric tension studies, while vascular 5-MTHF and biopterin levels were measured by (HPLC).
Results: 5MTHF improved vasomotor response to ACh (fig a) and decreased SOO production in both HSV and IMA (1.0 (SD 0.15) and 0.97 (0.15) RLU/sec/mg in 5MTHF-treated v 2.27 (0.37) and 5.01 (0.62) RLU/sec/mg in placebo treated patients, respectively, p<0.01 for both). L-NAME reduced the SOO signal in both HSV and IMA in the placebo group, an effect reversed by 5MTHF (fig b). 5MTHF increased total biopterins (tBIO), BH4 and the tBio/BH4 ratio (fig c). Furthermore, vascular 5MTHF levels were correlated with the BH4/tBio ratio in both the whole population (r = 0.406, p = 0.001 in HSV and r = 0.334 p = 0.043 in IMA respectively) and in the placebo-treated patients (r = 0.352, p = 0.03 in HSV and r = 0.464 p = 0.026 in IMA respectively). Vascular 5MTHF was also correlated with the maximum relaxations of HSV to ACh (r = 0.314, p = 0.016).
Conclusions: Vascular 5MTHF levels are related to NO-mediated endothelial function and the BH4/tBio ratio in patients with coronary artery disease (CAD). Moreover, intravenous administration of 5MTHF rapidly increases nitric oxide bioavailability, improves eNOS “coupling” and decreases superoxide production in human vessels, by preventing intracellular BH4 oxidation in vivo. Restoration of BH4 availability may have beneficial effects in human vascular disease states.
endothelium; tetrahydrobiopterin; 5-methyl-tetrahydrofolic acid

Abstract 282
283 EFFECTS OF 5-METHYL-TETRAHYDROFOLIC ACID ON ENDOTHELIAL FUNCTION AND VASCULAR SUPEROXIDE PRODUCTION IN HUMAN CORONARY ARTERY DISEASE
C. Antoniades1, C. Shirodaria1, P. Leeson1, J. Lee1, N. Warrick1, D. Taggart2, C. Ratnatunga2, R. Pillai2, K. Channon1.1University of Oxford, Cardiovascular Medicine Department, Oxford, UK; 2John Radcliffe Hospital, Department of Cardiothoracic Surgery, Oxford, UK
Introduction: 5-methyltetrahydrofolic acid (5MTHF), the active form of folic acid, may have antiatherogenic properties by reducing homocysteine, but its direct effects on vascular function in atherosclerosis are unclear. We evaluated the direct effect of 5MTHF on endothelial function and superoxide (SOO) production in human saphenous veins (HSV) and internal mammary arteries (IMA) from patients undergoing CABG.
Methods: Vasomotor responses to acetylcholine (ACh) were evaluated ex-vivo in vessel segments at baseline and after 45 minutes incubation with 5MTHF at 0, 1, 10 or 100 µM (n = 35 patients). Vascular superoxide (SOO) production was measured using 5 µM lucigenin chemiluminescence, in the presence of 5MTHF 0, 1, 10 or 100 µM, in paired samples of HSV and IMA from the same patients. The possible SOO-scavenging capacity of 5MTHF was quantified using a xanthine/xanthine oxidase system, using similar concentrations of vitamin C as positive control.
Results: All concentrations of 5MTHF similarly improved the vasomotor responses of HSV to ACh (figure a). Whereas 5MTHF at high concentrations (100 and 1000 µM) had direct SOO scavenging effect, no direct scavenging was observed with concentrations <10 µM (figure b), in contrast to the direct superoxide scavenging properties of vitamin C even at 1ìM (figure b). All the used concentrations of 5MTHF decreased SOO in both HSV and IMA compared to control, although there was no difference in SOO production between vessels exposed to 1, 10 and 100 µÌ 5MTHF (figures c and d).
Conclusions: 5MTHF improves endothelial function and decreases superoxide production in vessels from patients with CAD, by a mechanism other than the direct scavenging of superoxide radicals. These data suggest that 5MTHF may be useful for the treatment of increased oxidative stress in human atherosclerosis, by decreasing vascular superoxide production and improving NO bioavailability.
coronary artery disease; oxidative stress; nitric oxide

Abstract 283
284 INCREASED ENDOTHELIAL TETRAHYDROBIOPTERIN SYNTHESIS REDUCES VEIN GRAFT ACCELERATED ATHEROSCLEROSIS IN APOLIPOPROTEIN E-KNOCKOUT MICE
Z. Ali, A. Tatham, J. Bendall, J. De Bono, D. Greaves, N. Alp, K. Channon.University of Oxford, Oxford, UK
Accelerated atherosclerosis is associated with reduced endothelial nitric oxide (NO) bioavailability. Tetrahydrobiopterin (BH4) is a required cofactor for NO synthesis by endothelial nitric oxide synthase (eNOS). We aimed to investigate the importance of BH4 in regulating eNOS activity using a transgenic mouse with endothelial-targeted overexpression of the rate-limiting enzyme in BH4 synthesis, GTP-cyclohydrolase I (GCH), in a vein bypass graft model of accelerated atherosclerosis. Transgenic mice crossed onto hypercholesterolemic ApoE-KO background (GCH-Tg/ApoE-KO) or their ApoE-KO littermates underwent interposition bypass grafting of donor caval vein to the carotid artery. Grafts were harvested 28 days post surgery. Vascular BH4 levels were 5-fold higher in GCH-Tg/ApoE-KO vena cava compared with ApoE-KO mice (p<0.001). BH4 augmentation reduced total vessel wall area (*61%, p<0.001) compared to ApoE-KO controls. Furthermore, increased BH4 dramatically reduced macrophage content by almost 90% (p<0.01).
The majority of endothelial cells in vein grafts undergo necrosis or apoptosis early post surgery followed by repopulation by circulating and bone-marrow derived progenitor cells. Thus, to confirm the phenotype we found in GCH-Tg/ApoE-KO mice we grafted veins between the genotypes. When donor veins from ApoE-KO mice were grafted into recipient GCH-Tg/ApoE-KO mice the reduction in lesion area was maintained (# 48%, p<0.001). Conversely, when GCH-Tg/ApoE-KO donor veins were grafted into recipient ApoE-KO mice there was no reduction in lesion area compared to ApoE-KO controls. In keeping with these findings, we measured vascular BH4 in vein graft homogenates. Four weeks postoperatively, BH4 levels in ApoE-KO veins grafted into GCH-Tg/ApoE-KO recipients reached similar levels to GCH-Tg/ApoE-KO veins grafted into GCH-Tg/ApoE-KO mice (36+5 vs 31+12; p = 0.10). Interestingly, BH4 levels in GCH-Tg/ApoE-KO veins grafted into ApoE-KO mice remained higher compared to ApoE-KO controls (4.6+0.1 v 1.1+0.8; p<0.01).
These results indicate that reduction in graft atherosclerosis is conferred by endothelial overexpression of GCH, and furthermore that graft phenotype is conferred by the recipient animal genotype. These findings highlight the importance of endothelial BH4 in accelerated atherosclerosis.
tetrahydrobiopterin; endothelium; vein graft atherosclerosis

Abstract 284
285 INCREASED ATHEROSCLEROSIS BY ENDOTHELIAL NITRIC OXIDE SYNTHASE UNCOUPLING FROM TETRAHYDROBIOPTERIN DEFICIENCY
J. Khoo, C. Bursill, S. Cai, J. Bendall, J. de Bono, Z. Ali, M. McAteer, N. Alp, K. Channon.John Radcliffe Hospital, University of Oxford, Oxford, UK
Nitric oxide (NO), produced from endothelial NO synthase (eNOS), is critical in vascular homeostasis. Loss of NO due to higher oxidative stress has been implicated in atherosclerosis. Without its cofactor tetrahydrobiopterin (BH4), eNOS can become uncoupled, producing superoxide instead of NO. However, the effect of BH4 deficiency on atherosclerosis is uncertain. We hypothesised that BH4 deficiency would accelerate atherosclerotic progression, due to effects on eNOS function. To investigate the effects of BH4 deficiency on atherosclerosis, we crossed HPH mice, which have 80% deficiency of GTP Cyclohydrolase I (GCH; the rate-limiting enzyme in BH4 synthesis), with ApoE-/- (e) mice, generating ApoE-/-hph (eH) mice. To specifically restore endothelial BH4 levels, AH mice were further bred with GCH-Tg mice (which have endothelium-targeted GCH over-expression), generating ApoE-/-hphGCH (eHG) mice.
Aortic BH4, measured by HPLC in littermates fed a 12-week high-fat diet, was lower in eH mice v e mice (0.23 (SD 0.03) v 0.69 (SD 0.11) pmoles/mg protein, p<0.01), but restored in eHG mice (0.82±0.04 pmoles/mg protein). Aortic NO production, assessed by percentage of 14C-arginine-to-citrulline conversion and HPLC, was reduced in eH mice v e mice (0.28 (0.02) v 0.33 (0.02), p<0.05), but enhanced in eHG mice (0.40 (0.02), p<0.05). Endothelial superoxide, measured by dihydroethidium fluorescence, was greater in eH mice v e mice (1450 (150) v 940 (80) arbitrary units, p<0.01), but not in eHG mice (940 (50) arbitrary units, p<0.01). The excess superoxide in eH mice originated from uncoupled NOS, as it was abolished by NOS inhibition with L-NAME. Importantly, aortic root atherosclerosis was greater in BH4-deficient eH mice v e mice (plaque area/total vessel area: 0.32 (0.01) v 0.25 (0.02), p<0.01), but this was prevented in eHG mice (plaque area/total vessel area: 0.24 (0.02)). Accordingly, immuno-staining with smooth muscle α-actin antibodies revealed loss of vessel wall media smooth muscle content in eH mice v e mice (0.061 (0.005) v 0.079 (0.005) mm2, p<0.05), but not in eHG mice (0.086(0.007) mm2). Vessel lumen area was also reduced in eH mice v e mice (0.60 (0.03) v 0.67 (0.02) mm2, p<0.05), but not in eHG mice (0.69 (0.02) mm2). Systemic blood pressures, measured with tail-cuff plethysmography, were similar in all mice, and hence do not account for the observed differences in atherosclerotic progression.
In conclusion, eNOS uncoupling from BH4 deficiency increases atherosclerosis, which was prevented by endothelial BH4 restoration. BH4-dependent eNOS coupling is thus a potential therapeutic target in atherosclerosis.
nitric oxide; atherosclerosis; tetrahydrobiopterin
286 THE P2Y12 RECEPTOR REGULATES THE VESSEL WALL RESPONSE TO ARTERIAL INJURY AND THROMBOSIS
D. Evans, D. Crosdale, K. Norman, S. Francis, R. Storey.Cardiovascular Research Unit, University of Sheffield, Sheffield, UK
Platelets are believed to play an important role in atherogenesis and the vessel response to vascular injury. The P2Y12 receptor (P2Y12) plays a central role in amplifying platelet aggregation, dense granule and α-granule secretion, P-selectin expression, microparticle formation and pro-coagulant membrane changes regardless of the activating stimulus. We hypothesised that P2Y12 deficiency might reduce the vessel wall response to vascular injury as well as thrombosis in a murine ferric-chloride injury model. P2Y12 deficient (-/-) mice and littermate controls were bred on a C57 BL/6 background. Platelet aggregation was measured in whole mouse blood by single platelet counting and P-Selectin expression by FACS.
Vascular injury was induced by treatment of a 2 mm section of carotid artery with a 10% FeCl3 solution for 3 minutes. Vessels were perfusion fixed in situ and harvested at 21 days post injury. P2Y12 -/- platelets had no sustained aggregation response to adenosine diphosphate and markedly reduced P-selectin expression in response to TRAP. At 21 days post injury, neointima formation in P2Y12 -/- arteries was significantly less than that observed in control strain arteries. This difference remained significant regardless of whether neointimal area measurements of each artery were derived from the average neointimal area of multiple artery sections (P2Y12 -/-, 0.011 (SD 0.0007) mm2, n = 4 vs. P2Y12 +/+, 0.061 (0.006) mm2, n = 4; P = 0.0286; figure 1) or from the individual section with the largest neointima (P2Y12 -/-, 0.014 (0.0004) mm2, n = 4 vs. P2Y12 +/+ 0.074±0.008 mm2, n = 4; P = 0.0286). These data demonstrate a role for P2Y12 in the vessel wall response to arterial injury and thrombosis and highlight the relationship between early thrombotic response and later neointima formation following arterial injury. This illustrates how platelets may contribute to atherogenesis and restenosis.

Abstract 286
platelet; restenosis; arterial injury
287 PROTEASE-ACTIVATED RECEPTOR-1 ACTIVATION CAUSES VENOCONSTRICTION IN VIVO IN MAN
I. Gudmundsdottir1, D. Webb2, D. Newby2.1Cardiovascular Sciences, University of Edinburgh, Edinburgh, UK; 2University of Edinburgh, Edinburgh, UK
Introduction: Protease-activated receptor type 1 (PAR-1) is a G-protein coupled receptor that mediates the majority of the cellular actions of thrombin in man. PAR-1 appears to regulate vasomotor control and platelet activation, and PAR-1 antagonists are in clinical development as potential anti-platelet therapies. The effects of PAR-1 agonism have not previously been described in vivo in man. During inflammation, protease-activated receptor type – 2 (PAR-2) is up regulated and may modulate vascular responses.
Methods: Dorsal hand vein diameter was assessed by the Aellig technique in 14 healthy human volunteers. Noradrenaline (1–128 ng/min) was infused to induce and maintain stable venoconstriction during PAR-1 activating peptide (SFLLRN-NH2: 0.05-5 nmol/min), and PAR-2 activating peptide (SLIGKV-NH2: 1.6, 16 and 160 nmol/min), infusions. Subsequently, the influence of platelet aggregation on the vasomotor response (figure 1) was determined by co-infusing SFLLRN-NH2 (0.05-15 nmol/min) with and without the GPIIb/IIIa antagonist tirofiban (125 ng/min).

Abstract 287
Results: SFLLRN-NH2 and SLIKGV-NH2 caused dose-dependent venoconstriction (n⩾6, p<0.001) and venodilatation (n = 6, p = 0.015) respectively. SFLLRN-NH2 induced venoconstriction was unaffected by tirofiban co-infusion (n = 6, p = ns). Vein patency was maintained at all times with no in situ thrombus formation.
Conclusions: PAR-1 and PAR-2 activation cause venoconstriction and venodilatation respectively in vivo in man. PAR-1 mediated venoconstriction is independent of platelet aggregation. We conclude that thrombin causes direct PAR-1 induced venoconstriction in man and that PAR mediated vasomotor responses may depend on the inflammatory state of the vasculature. Modulation of PAR receptors is likely to be of therapeutic importance and further studies of their physiological role in man are warranted.
protease activated receptors; human; venoconstriction
288 PLATELET PROTEASE-ACTIVATED RECEPTOR 1 DENSITY, TRAP-INDUCED PLATELET RESPONSES, AND THE EFFECT OF COMPLETE P2Y12 RECEPTOR BLOCKADE
S. Smith, H. Judge, M. Daly, R. Storey.University of Sheffield, Sheffield, UK
Introduction: Inhibition of the P2Y12 ADP receptor reduces platelet reactivity in response to many agonists, including thrombin. Thrombin activates platelets via 3 receptors, one of which is protease-activated receptor 1 (PAR-1). We investigated whether platelet PAR-1 density influences platelet responses to thrombin receptor activating peptide (TRAP) in the presence and absence of complete P2Y12 blockade with Cangrelor.
Methods: Blood was drawn from 52 subjects and anticoagulated with hirudin. Optical aggregometry (OA), whole-blood single platelet counting aggregometry, and flow-cytometric measurement of platelet procoagulant activity assessed as annexin V expression and microparticle formation within whole-blood and platelet rich plasma (PRP), and platelet calcium mobilisation within PRP, were assessed in response to TRAP. Experiments were performed with and without the invitro addition of Cangrelor 1 uM. Platelet PAR-1 density was assessed by incubating PRP with PE-labelled anti-PAR-1 antibody, correcting the median fluorescence value with that from an isotype control, and calculating an absolute number against a standard line generated using fluorochrome beads.
Results: Inter-subject PAR-1 density ranged from 638 to 1504 (median 886). Dividing subject PAR-1 density into tertiles revealed a clear relationship between receptor number and platelet responses to TRAP in whole-blood and PRP. Subjects within the bottom tertile of PAR-1 density (median 721, IQR 683–764, n = 17) had lowest responses to all assays in both the presence and absence of Cangrelor (p<0.001). Subjects within the middle tertile (median 882, IQR 851–909, n = 17) had lower OA responses than those within the top tertile (median 1018, IQR 986–1158, n = 18) to moderate concentrations of TRAP or to higher concentrations of TRAP in the presence of Cangrelor (p<0.01), but uninhibited high concentrations of TRAP were not discriminatory. Procoagulant data, however, was only higher in the top tertile compared to the middle tertile when uninhibited high concentrations of TRAP were used (p<0.01).
Conclusions: Platelet PAR-1 density clearly influences TRAP-induced platelet responses. Complete P2Y12 blockade significantly inhibits TRAP-induced responses in all patients, but aggregometry responses remain greater in subjects with the highest PAR-1 density. Further studies will determine whether PAR-1 density, or factors which influence it such as the PAR-1 IVSn-14 A>T polymorphism, are of clinical relevance.
platelets; protease activated receptor 1; cangrelor
289 INSULIN-LIKE GROWTH FACTOR BINDING PROTEIN-1: A VASCULOPROTECTIVE PROTEIN IN OBESITY AND TYPE II DIABETES MELLITUS
V. Ezzat, E. Duncan, S. Wheatcroft, A. Shah, M. Kearney.King’s College London, London, UK
Introduction: Insulin-like growth factor-I (IGF-I) and IGF binding protein-1 (IGFBP-1) are believed to have complimentary roles in the regulation of glucose homeostasis. Observational studies suggest that patients with insulin resistance have lower levels of circulating IGF-I. Low levels of IGF-I and IGFBP-1 have also been implicated in the development of cardiovascular disease. We characterised the longitudinal changes in IGF-I, IGF-I sensitivity and IGFBP-1 expression in dietary-induced obesity and insulin resistance in mice. Furthermore, the effects of IGFBP-1 overexpression on the metabolic and vascular sequelae of diet-induced obesity/type II diabetes were assessed.
Methods: Male C57 Bl/6 wildtype mice (WT) received an obesogenic or standard chow diet from weaning (n = 6–16). Morphometrics were recorded and whole body insulin sensitivity was assessed by intraperitoneal (IP) insulin tolerance tests. Fasting IGF-I levels were measured by ELISA. Hepatic IGFBP-1 expression was measured by real-time PCR. Subcutaneous IGF-I tolerance tests (0.2 µg/g) were performed. Transgenic mice (TG) overexpressing human IGFBP-1 were also fed the obesogenic diet and underwent IP insulin tolerance testing. Body weight, fat pad mass and fat cell size were measured. Vascular insulin and IGF-I sensitivities were assessed ex-vivo in organ bath studies on thoracic aortic rings from high fat-fed TG and WT. Rings were studied for constriction to phenylephrine pre- and post-incubation in 100 mU/ml insulin or 100 nM IGF-I solution.
Results: WT receiving a high-fat diet had a higher body weight, larger fat pad mass and fat cell size than those fed chow diet and demonstrated significantly decreased insulin sensitivity (ANOVA, p<0.01). In addition the hypoglycaemic effect of IGF-I was decreased (p<0.001) and circulating IGF-I levels were found to be higher (298 ng/ml vs. 404 ng/ml, p<0.05). Native IGFBP-1 expression was similar to controls. TG fed a high-fat diet had similar body weights and adiposity as WT littermates, however insulin resistance was significantly attenuated (41.8% decrease in blood glucose at 30 mins. v32.3%, p<0.02). Insulin and IGF-I did not alter the effect of phenylephrine on aortic rings of WT mice, however in TG mice there was significant blunting of vasoconstriction (pEC50 1.47×10–7M v. 2.87×10–7M for insulin, figs 1 and 2, and 1.4×10–7M vs. 2.38×10–7M for IGF-I, p<0.05) in keeping with preserved vascular insulin sensitivity.

Abstract 289

Abstract 289
Conclusions: These data, contrary to previous observations, demonstrate that IGF-I levels increase as insulin sensitivity decreases and that there is an accompanying decrease in IGF-I sensitivity. Murine IGFBP-1 expression in the liver remains unchanged however overexpression of human IGFBP-1 protects against the development of insulin resistance in both peripheral tissues and the vasculature despite the development of obesity.
This work was supported by the British Heart Foundation.
insulin-like growth factor binding protein-1; Insulin-like growth factor-I; diabetes
290 IN-STENT STENOSIS IN APOLIPOPROTEIN-E KNOCKOUT MICE: A NOVEL MOUSE MODEL OF BALLOON ANGIOPLASTY AND STENTING
Z. Ali1, N. Alp1, H. Lupton2, N. Arnold3, M. Wheatcroft3, Y. Hu4, D. Greaves1, J. Gunn3, K. Channon1.1University of Oxford, Oxford, UK; 2Brivant Medical Engineering, Galway, Ireland; 3University of Sheffield, Sheffield, UK; 4St. George’s Hospital Medical School, London, UK
The principal cause of PCI failure is in-stent stenosis. Greater understanding of the molecular mechanisms underlying this process could provide new therapeutic targets. We developed a novel mouse model of angioplasty and stenting to allow investigation of these mechanisms using genetically modified strains. Thoracic aortic segments from hypercholesterolemic ApoE -/- or C57Bl/6 wild-type mice (n = 5/group) were grafted into the carotid artery of isogenic recipients using a cuff technique - either as untreated aortic grafts (control), following balloon angioplasty, or after stenting with a 1.0×3.0 mm stainless steel slotted tube stent deployed on a 1.25 mm balloon inflated to 10 atmospheres. Vessels were harvested 28 days later. Uninjured ApoE -/- control vessels developed minimal neointimal hyperplasia. However, balloon angioplasty caused significant neointima formation compared to control vessels (*3-fold, p<0.001), leading to luminal narrowing four weeks postoperatively (60%, p<0.01). ApoE -/- stented animals developed reproducible in-stent stenosis, with significantly greater neointimal area compared to balloon angioplasty (**2.2 fold, p<0.001). However, stenting greatly increased total vessel area, and although neointima was increased in the stented animals, lumen area was increased by 71% (p<0.001).
Interestingly, in C57Bl/6 wild-type mice, despite equal stent expansion, neointimal area was decreased by 30% (# P<0.01). This model reproduces important features of human PCI and provides proof of principle that the utility of stenting in genetically modified mice provides the potential to investigate molecular pathways and explore novel therapeutic targets for in-stent stenosis.
balloon angioplasty and stenting; restenosis; mouse model

Abstract 290
291 ELECTROANATOMIC REMODELLING OF THE RIGHT ATRIUM FOLLOWING THE FONTAN PROCEDURE: AN ELECTROPHYSIOLOGICAL AND FUNCTIONAL ANALYSIS.
D. Abrams, M. Earley, S. Sporton, R. Schilling.St. Bartholomew’s Hospital, London, UK
Purpose: To investigate electroanatomic remodelling of the right atrium (RA) after the Fontan procedure as relates to electrophysiological (EP) characteristics, arrhythmia mechanism and functional capacity.
Methods: EP study was performed using simultaneous non contact (NCM) and electroanatomic mapping, recorded during sinus rhythm, pacing and arrhythmia. Both systems were analysed to define arrhythmia mechanism and guide irrigated radiofrequency ablation (RFA). Off-line analysis of bipolar voltage maps was used to identify abnormal endocardium (AE); defined as scar (bipolar contact amplitude <0.05 mV) and low voltage endocardium (LVE) (<0.5 mV). The contributory role of scar and LVE to differing arrhythmia mechanism was assessed. Conduction velocity (CV) was measured on contact activation maps perpendicular to 5 ms isochrones. NCM was validated by correlating the morphology and timing difference between reconstructed and contact unipolar electrograms (EGM) at varying distances from the multi-electrode array (MEA). Cardiopulmonary exercise testing and health surveys were completed before and 6 months after RFA. End points were arrhythmia freedom and changes in functional capacity.
Results: 25 patients aged 26.9 (SD 9.1) years were studied 8.2 (6.2) years after the Fontan procedure. Atrial arrhythmias had been documented for 6.3 (4.4) years. AE was 44.5 (20.7)% of the RA area (scar 18.6 (13.6)% and LVE 26.5(11.9)%). A significant correlation was seen between scar and age at Fontan (p = 0.012), although no increase was seen with multiple bypass procedures. Conversely LVE was associated with arrhythmia duration (p = 0.004). 42 RA arrhythmias were identified; reentrant (n = 32), focal (n = 9) and AVNRT (n = 1). The reentrant mechanisms were scar-related (n = 3), periannular (n = 4) and varying degrees of fixed or fixed and functional conduction block at the crista terminalis (n = 15). CV was significantly reduced in LVE (p<0.0001). All reentrant, but only 4/9 focal arrhythmia were associated with AE. RFA resulted in arrhythmia termination and/or modification in 95%. Although recurrence has been seen in 10/24, only 1 remains clinically significant. A significant improvement in exercise duration (p = 0.04), physical (p = 0.009) and mental (p = 0.02) quality of life was seen following RFA (n = 10). NCM was beneficial in 66% of cases, but hindered by poor EGM correlation >40 mm from the MEA (r = 0.39 (0.38)). There were no complications.
Conclusion: Increased age at surgery and hence duration of cyanosis leads to infarction and scar, whereas arrhythmia induced remodelling after the Fontan causes a progressive increase in LVE exacerbated by the chronically abnormal haemodynamic load placed on the RA. RFA is safe and associated with improved functional capacity and quality of life.
arrhythmia mechanism; atrial remodelling; adult congenital heart disease
292 BY PACING AT INCREASED RATES AT REST IT IS POSSIBLE TO PREDICT THE HAEMODYNAMIC OPTIMAL ATRIOVENTRICULAR DELAY OF BIVENTRICULAR PACING DETERMINED DURING EXERCISE
Z. Whinnett1, J. Davies1, C. Briscoe1, K. Willson2, R. Foale1, D. Davies1, A. Hughes1, J. Mayet1, D. Francis1.1St Mary’s Hospital and Imperial College London, London, UK; 2The Royal Brompton Hospital, London, UK
Background: Ideally optimisation of atrioventricular (AV) delay of cardiac resynchronisation therapy would be performed during exercise, as this is when patients are most symptomatic. However, this can be technically difficult and inconvenient for the patient. It may be possible to use fast pacing at rest to simulate exercise, however, account has be taken for the difference in optimal AV delay between atrial pacing and sensing.
We test a pacing model for exercise, to determine whether it is possible at rest to predict the haemodynamic peak AV delay determined during exercise.
Method and Results: We performed AV delay optimisation, using non-invasive haemodynamics recorded using the Finometer device, in 12 biventricular pacemaker patients, using our system for maximising signal-to-noise ratio. We calculated the difference between the haemodynamic optimal AV delay for atrial paced and atrial sensed AV delay at resting rates (the “sensed-paced optimum difference”). We subtracted this from the optimal AV delay found with atrial pacing at 100 bpm, in order to create a “predicted exercise AV optimum”.
Patients separately underwent haemodynamic optimisation during actual treadmill exercise (∼100 bpm), to test the validity of the resting prediction. All patients showed a clear optimum.
The actual exercise optimal AV delay was shorter than the 100 bpm pacing value and was closely predicted by our resting formula (r = 0.93, p<0.001). The root-mean-square difference between predicted and actual was only 14 ms.
Conclusions: Actual exercise haemodynamic optimisation is possible, in patients able to exercise for several minutes. The exercise optimum for AV delay can be determined from resting optimisation, if the sensed-paced difference is also measured. This may allow appropriate exercise AV delays to be selected without the need for optimisation during exercise.
atrioventricular delay optimisation; exercise; biventricular pacing

Abstract 292
293 ANALYSIS OF ACTION POTENTIAL DURATION RESTITUTION DURING SYMPATHETIC NERVE STIMULATION V PACING - EFFECT OF IKS INHIBITION
R. Mantravadi1, B. Choi2, G. Salama2, G. Ng3.1University of Leicester, Leicester, UK; 2University of Pittsburgh, Pittsburgh, US; 3Glenfield Hospital/University of Leicester, Leicester, UK
Restitution kinetics (RK) of action potential duration (APD) has been suggested to be a predictor of arrhythmia vulnerability in various pathologies. RK is usually studied experimentally with pacing and the relationship between APDs and preceding diastolic intervals (DI) plotted in a RK curve. In vivo, APD adaptation to heart rate (HR) follows sympathetic activity rather than pacing. To measure RK in more physiological conditions, we used a novel isolated rabbit heart preparation with intact sympathetic innervation and applied optical mapping to measure APD using voltage-sensitive dye (Di-4ANEPPS) over the ventricular surface (n = 5). RK was measured during sympathetic nerve stimulation (SNS) and compared to ventricular pacing with the identical sequence of HR change.
Results: (figure): During SNS (10 Hz), APD continued to decrease after HR reached its peak resulting in a negative slope in the RK curve. After stopping SNS, HR and APD recovered to baseline values, completing a hysteresis loop. Pacing produced ∼50% less APD shortening than SNS (14.7 (SD 2.8)% v 7.9 (1.7)%, p<0.005). Enhanced activation of numerous ion channels could account for the APD shortening and DI prolongation during SNS. These changes were examined in the presence of a selective IKs blocker HMR 1556 (0.5 µM) since IKs is highly dependent on adrenergic activity. With HMR, the negative slope of RK persisted but there was no difference in APD loops between SNS and Pacing (13.4 (2.1)% v 12.9 (2.0)%, p = NS, fig. B).
Conclusion: These results show that SNS produced shorter APD and longer DI at peak constant HR over and above changes achieved with Pacing. For identical HR changes in Pacing and SNS, loop differences are attributable to adrenergic modulation of APD that are reduced by IKs inhibition. These changes may be important in arrhythmogenic mechanisms underlying pathological conditions such as Long QT syndrome.
restitution kinetics; sympathetic nerve stimulation; ion channels

Abstract 293
294 CHANGES IN ATRIOVENTRICULAR DELAY OF CARDIAC RESYNCHRONISATION THERAPY HAVE A SIGNIFICANTLY LARGER HAEMODYNAMIC EFFECT COMPARED WITH ALTERING INTERVENTRICULAR DELAY
Z. Whinnett1, J. Davies1, K. Willson2, C. Manisty1, A. Chow3, R. Foale1, D. Davies1, A. Hughes1, J. Mayet1, D. Francis1.1St Mary’s Hospital and Imperial College London, London, UK; 2The Royal Brompton Hospital, London, UK; 3The Heart Hospital, London, UK
Background: Little is known about the characteristics of the haemodynamic response curves to changes in atrioventricular (AV) and interventricular (VV) delay of cardiac resynchronisation therapy. In this study we assess in detail these characteristics and compare the magnitude and relative importance of adjustment in AV and VV delay.
Method and Results: 36 different combinations of AV and VV delay were tested using digital photoplethysmography (Finometer) with repeated alternations, to measure systolic blood pressure relative to a reference pacing configuration (SBPrel), in fifteen patients with cardiac resynchronisation devices for heart failure.
Changing AV and VV delay both had a curvilinear effect. However, AV delay had a significantly larger effect compared with changes in VV delay (range of SBPrel 21 versus 4.2 mm Hg p<0.001).
The curve of response to AV delay fitted extremely closely to a parabola (average R2 = 0.99, average residual variance 0.8 mm Hg2). The response to VV delay was significantly less curved (quadratic coefficient 67 versus 1194 mm Hg•s−2 p = 0.003) and therefore although the residual variance was equally small (0.8 mm Hg2) the R2 value was 0.7.
Conclusions: : Changing AV and VV delay results in a curvilinear acute blood pressure response. This shape fits very closely to a parabola, which may be valuable information in developing a streamlined clinical protocol. VV delay adjustment provides an additional, albeit smaller, haemodynamic benefit to AV optimisation.
atrioventricular delay; interventricular delay; haemodynamics

Abstract 294
295 CARDIAC RESYNCHRONISATION THERAPY IS EFFECTIVE IN PATIENTS WITH LESS SEVERE SYMPTOMS
J. Cleland1, N. Freemantle2, L. Tavazzi3, M. Calvert2, E. Erdmann4, L. Kappenberger5, D. Gras6, J. Daubert7.1University of Hull, Kingston upon Hull, UK; 2University of Birmingham, Edgbaston, UK; 3IRCCS Policlinico S.Matteo, Pavia, Italy; 4University of Cologne, Cologne, Germany; 5Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland; 6Nouvelles Cliniques Nantaises, Nantes, France; 7Hospital Pontchaillou, Rennes, France
Background: It is uncertain whether cardiac resynchronisation therapy (CRT) is effective in patients with mild symptoms of heart failure.
Aims: To assess whether the benefits of CRT were different in patients with milder symptoms of heart failure in the CARE-HF programme.
Methods: Patients with New York Heart Association (NYHA) class III or IV heart failure, LVEF <35% and evidence for cardiac dyssynchrony were enrolled into the CARE-HF study. Patients were asked to rate the severity of their symptoms and impairment of quality of life using NYHA classification, EuroHeart Failure Survey questionnaire (EHFSQ) and Euroqol EQ-5D. The effect of cardiac resynchronisation on the primary end point of the main study (death or unplanned hospitalisation for a major cardiovascular event), of the extension study (all-cause mortality) and NYHA class at 18 months (with death or heart transplant assigned a rank of V on this scale) were assessed according to patient-perceived disease severity at baseline. All analyses were conducted by intention to treat.
Results: Of the 813 patients enrolled in CARE-HF, 783 (96%) provided self-reported symptoms at baseline and 175 (22%) rated themselves as NYHA class I or II. Compared to patients who rated themselves as NYHA III or IV, these patients had similar LVEF (Mean 26% for each; mean difference −0.1%, 95% CI −1.2 to 0.9) but lower N-Terminal Brain Natriuretic Peptide (Mean 2706 pg/ml I/II vs. 3862 pg/ml III/IV; mean difference -1156 pg/ml, 95% CI −2129 to 184). Only 399 (50%) patients felt that breathlessness greatly limited their ability to do normal activities (score 4 or 5) and only 229 (29%) rated their overall health as poor or very poor (score 5 or 6) on the EHFS questionnaire. The effect of CRT on all three endpoints was similar regardless of the baseline severity of symptoms. However, patients with EQ-5D score above the median (better quality of life) had a smaller benefit from CRT in terms of mortality and NYHA class at 18 months.
Abstract 295
Conclusion: Patients with less severe symptoms of heart failure appear to obtain long-term benefit from CRT in terms of reduced morbidity and mortality.
cardiac resynchronisation; heart failure; symptoms
296 CLINICAL MODEL TO EVALUATE THE EFFECTS OF DRUGS ON CARDIAC REPOLARISATION: NON-INVASIVE ELECTROPHYSIOLOGICAL STUDY OF IVABRADINE
I. Savelieva1, S. Jones2, K. Dougal1, M. Malik1, E. Rowland1.1St George’s University of London, London, UK; 2St George’s Hospital, London, UK
Ivabradine (IVA) is a selective inhibitor of the sinus node If current with specific bradycardic and potential antiarrhythmic actions. Slowing of the heart rate (HR) with IVA is associated with marked prolongation of the QT interval. Attempts to correct the QT interval using the Bazett and Fridericia formulae led to overcorrecting (QTc shortening) or undercorrecting (QTc lengthening), respectively. Therefore, instead of correcting for HR, the effects of IVA on ventricular repolarisation were evaluated using a new model of direct comparisons of the QT interval during atrial pacing at different fixed rates before and after IVA administration.
Methods: To avoid the limitations of invasive electrophysiological studies, we studied 25 pts (63 (SD 10) years; M/F 16/9; sinus node disease (SND), 14; 1 or 2 degree AV block (AVB), 11, incl. AVB+bundle branch block (BBB), 5) with dual chamber pacemakers with non-invasive programmed stimulation (NIPS) in the prospective randomised, double blind, placebo-controlled study of oral IVA 5 mg (n = 8) or 10 mg (n = 8) bd. Atrial pacing (AP) at 80, 90, 100, 110 bpm and ventricular ERP (VERP) measurements were performed at baseline and after 3½ days of treatment when the therapeutic steady-state was achieved. A continuous 12-lead digital Holter ECG recording was used for the subsequent analysis and a custom-designed algorithm was applied to all QT measurements.
Results: IVA did not prolong the QT interval during AP compared with placebo (figure: left, Superimposed ECG tracings recorded on placebo, IVA 5 mg, and IVA 10 mg bd during AAI at 90 bpm; right, Difference in the QT interval v baseline, mean±SD). The pre-specified subgroup analysis in SND and AVB±BBB showed identical results. IVA 10 mg bd slightly but significantly increased VERP v baseline (IVA: 274 (SD 21) v 264 (20) ms; p = 0.033; placebo: 266 (36) v 258 (36) ms; p = 0.055). IVA 5 mg bd had no effect on VERP (271 (16) v 267 (17) ms).
Conclusions: The study demonstrated the feasibility of using NIPS in patients with atrial or dual chamber pacemakers as a model for assessing the electrophysiological effects of oral agents. Control of HR by AP at series of AP at identical rates showed that IVA had no direct effect on ventricular repolarisation.
ivabradine; repolarisation; pacing

Abstract 296

Abstract 296
297 PROPRANOLOL INCREASES TRANSMURAL DISPERSION OF REPOLARISATION IN δKPQ SCN5A (LONG QT3) MOUSE HEARTS
G. Thomas, M. Killeen, C. Goddard, N. Ghais, R. Balasubramaniam, J. Fraser, W. Colledge, A. Grace, C. Huang.1University of Cambridge, Cambridge, UK
Introduction: Gain-of-function mutations within Scn5a, that include the ΔKPQ1505-1507 deletion in the inactivation domain associated with compromised myocardial repolarisation, have been implicated in human long QT3 syndrome (LQT3). Our experiments explored the electrophysiological basis for the high arrhythmic mortality in LQT3, persistent despite β-adrenoreceptor blocker therapy, using Langendorff-perfused whole heart preparations from a ΔKPQ Scn5a+/Δ murine model of LQT3.
Methods and Results: Simultaneous endocardial and epicardial monophasic action potential (MAP) recordings from Scn5a+/Δ hearts (n = 7) demonstrated epicardial MAP durations (APD90 64.8 (SD 1.9) ms) that were prolonged relative to corresponding values in wild-type (WT) controls (48.9 (1.3) ms) (n = 5) (p = <0.0001) but endocardial APD90 values similar to WT (48.7 (0.4) ms v 49.1 (1.2) ms respectively) (n = 5) (p>>0.05).
This gave mean transmural dispersion of repolarizations (TDR), expressed as ΔAPD90 by calculating endocardial APD90 minus epicardial APD90 values, of −16.1 (1.9) in the Scn5a+/Δ compared to only +0.2 (1.8) ms in WT controls. Scn5a+/Δ hearts (5 out of 7 preparations) but never WT hearts (n = 5) showed multiple early afterdepolarisations (EADs) (fig 1A). and episodes of polymorphic ventricular tachycardia (pVT) (fig 1B) both of which were completely suppressed by 1 µM propranolol (fig 1C).

Abstract 297
In contrast, propranolol prolonged the epicardial APD90 to 72.5 (1.2) ms in Scn5a+/Δ hearts (n = 7) and 61.6 (1.8) ms in WT controls (n = 5) (p = <0.0001). Yet it reduced the endocardial APD90 to 24.5 (0.3) ms in Scn5a+/Δ hearts (n = 5), with no significant effect in WT controls (51.4 (0.7) ms) (n = 5). Propranolol thus exacerbated ΔAPD90 to −48 (1.4) ms in Scn5a+/Δ hearts compared to +10.2 (1.9) ms in WT controls. Finally, applications of premature extra stimuli (S2) during programmed electrical stimulation (PES), induced triggered beats and pVT in all Scn5a+/Δ hearts (n = 7) (fig 2A), but never in WT controls (n = 5). Propranolol suppressed all such S2-induced triggered activity in Scn5a+/Δ hearts (n = 7), yet a sufficiently premature stimulus induced pVT in all hearts (fig 2B).

Abstract 297
Conclusions: These findings suggest a hypothesis in which β-adrenoreceptor blockade with propranolol in Scn5a+/Δ hearts exerts an anti-arrhythmic action through suppression of EADs and triggered beats that may in turn initiate pVT but specifically enhances re-entrant substrate by increasing ΔAPD90 in the Scn5a +/Δ.
long QT syndrome; propranolol; mouse
298 EFFECT OF SEQUENTIAL VERSUS SIMULTANEOUS CARDIAC RESYNCHRONISATION THERAPY UPON PEAK OXYGEN CONSUMPTION
D. Fox1, A. Fitzpatrick1, S. Williams2, R. Khattar1, A. Borg2, N. Clayton2, N. Davidson2.1Manchester Heart Centre, Manchester Royal Infirmary, Manchester, UK; 2North West Regional Cardiac Centre, Wythenshawe, Manchester, UK
Background: Cardiac resynchronisation therapy (CRT) improves exercise capacity and prognosis in patients with congestive heart failure (CHF). Peak oxygen uptake (VO2) provides objective assessment of exercise capacity and correlates with survival. New CRT devices can pace either ventricle ahead of the other (V-V offset) and echocardiographic studies have demonstrated acute haemodynamic benefits of optimising V-V offset but no data exist as to what effect changing the V-V offset has upon peak VO2.
Methods: Twenty-three patients with CHF undergoing CRT (21 men, mean age 62.4 (SD 9.5), NYHA class III or IV), QRS prolongation >120 ms and LVEF <30% had a baseline cardiopulmonary exercise test (CPX) to measure peak VO2 prior to implantation. Post implantation, patients were randomised in a double blind fashion to 6 weeks each of active CRT with 4 different V-V offsets (constant A-V delay 100 ms). The four different V-V offsets used were: Simultaneous RV and LV pacing, RV 20 ms ahead of LV (RV-20), LV 20 ms ahead of RV (LV-20) and LV 40 ms ahead of RV (LV-40). After each of the four different paced periods each patient underwent a repeat CPX.
Results: Mean [±SEM] baseline peak VO2 was 12.55 (SD 0.80) mls/kg/min. Mean increases in peak VO2 (mls/kg/min) from baseline were: Simultaneous: +1.28 (1.05) (p = 0.03), RV-20: +0.87 (0.92) (p = NS), LV-20: +1.65 (0.97) (p = 0.004) and LV-40: +1.15 (0.96) (p = 0.04). Graph 1 demonstrates the changes in peak VO2 seen with the 4 different settings.
Conclusions: Although simultaneous LV and RV pacing significantly improves peak VO2, there is a trend towards further improvements when the LV is paced 20 ms ahead of the RV. Further work is required to determine whether echocardiographic optimisation at baseline can predict the optimal V-V offset for individual patients.
cardiac resynchronisation therapy; sequential biventricular pacing; peak oxygen consumption

Abstract 298
299 EFFECTS OF ANGIOTENSIN RECEPTOR BLOCKADE ON ATRIAL REMODELING AND THE “SECOND FACTOR” IN A GOAT MODEL OF ATRIAL FIBRILLATION
M. Hall1, S. Kirubakaran1, N. Peters2, C. Garratt1.1Manchester Heart Centre, Manchester, UK; 2Imperial College, London, UK
Background: Atrial fibrillation (AF) is known to cause atrial electrophysiological changes which predispose to itself-perpetuation (electrical remodelling). More recently the contribution of additional factors (second factors) has been characterised. Several groups have postulated that atrial remodeling and self-perpetuation of AF may be suppressed by blockade of the renin angiotensin system (RAS). Published experimental work is limited by short-term protocols, very high doses of RAS blockers and the confounding effects of LV impairment. We evaluated candesartan in a long-term goat model of lone AF in which electrical remodelling and “second factors” are well characterised.
Methods: Following preliminary studies demonstrating oral bioavailability of candesartan, we adapted Wijffels’s conscious goat model to deliver atrial burst pacing via a pacemaker-based system. The effects of RAS blockade on acute atrial electrical remodeling was assessed in 24 goats (12 candesartan 0.5 mg/kg/day, 12 placebo) during a 4 week burst pacing protocol utilising repetitive AF reinduction. Atrial refractory period (AERP), AF stability (duration of induced AF episodes), AF cycle length (AFCL), ventricular cycle length (VCL) and sinus cycle length (SCL) were measured. To assess the effects of RAS blockade on “second factors” 16 of these goats underwent further 4 week periods of burst pacing (total 2 months in 16 goats, 3 months in 8 goats) each separated by 7 days of sinus rhythm.
Results:
Acute electrical remodeling. There was no difference between placebo and candesartan in terms of SCL, VCL or AFCL or the rate or degree of fall in AERP, i.e. no demonstrable effect on acute electrical remodeling. The t½ (time for AERP to fall to half of difference between baseline and nadir) was 20.0 (SD 4.7) hours (placebo) and 18.3 (2.5) hours (candesartan) (p = ns).
Cumulative AF stability. There was a progressive increase in AF stability from month 1 to month 3 in both groups (ANOVA p<0.05) but there was no difference between candesartan and control groups.
Conclusion: Contrary to previous studies, we found that RAS blockade does not influence acute electrical remodelling or AF self-perpetuation due to “second factors” in a chronic goat model of lone AF. These findings suggest that any beneficial effects of blockade of the RAS in patients with AF are likely to be due to improvements in haemodynamics or left ventricular function rather than any direct effects on the remodeling process itself. These studies do not support the use of RAS blockade in patients with AF in the absence of structural heart disease.
atrial fibrillation; angiotensin receptor antagonist; atrial remodeling

Abstract 299
300 SERVICE DELIVERY AND DIAGNOSTICS FOR SUSPECTED HEART FAILURE: WHICH MODEL DO GENERAL PRACTITIONERS PREFER?
A. Fuat1, J. Murphy1, A. Mehrzad2.1Darlington Memorial Hospital, Darlington, UK; Hospital, Bishop Auckland, UK
Background: The NSF for chronic heart disease (CHD) recommends that echocardiography be offered to all patients with suspected heart failure(HF) and proposes service models that include cardiology clinics, open access echocardiography (OAE) or specialist heart failure clinics(OSDC) for diagnosis of LVSD. Furthermore, NICE and recent European Society of Cardiology guidelines have suggested that natriuretic peptides and electrocardiography be used in the diagnostic triage of patients with suspected HF by general practitioners (GPs). GPs in South Durham have had access to all 3 service models over the past 9 years and were provided with NT proBNP use for suspected HF in 600 consecutive patients.
Methods: A questionnaire survey asked 179 South Durham GPs whether they had used NT proBNP and which service model they preferred. GPs were also asked about confidence in interpretation of investigations/procedures used in the diagnosis of HF due to LVSD.
Results: The response rate was 75%(n135). 74% had used NT proBNP, 23% had not and 3% did not reply.
Abstract 300 Table 1
Most GPs prefer a OSDC run by a GP specialist and supervised by a cardiologist/physician, with prior triage using NT proBNP. 64%(n 86) favoured use of NT proBNP before referral. However about a third of GPs did not feel NT proBNP was useful. Of the 32 GPs preferring OAE, 41% (n13) would not have initiated a beta-blocker, 4 would not initiate spironolactone or digoxin(n2).
Abstract 300 Table 2 Confidence in interpretation and use of investigations or clinical assessment alone, where 1 is very confident and 5 not at all confident
A quarter of GPs felt they could diagnose HF due to LVSD on clinical assessment alone. Only 23% of GPs felt confident in interpretation of the ECG. 49% of GPs were confident in using NT proBNP, 40% the CXR and 63% echocardiogram.
Conclusions: Most GPs expressed a preference for a OSDC with prior NT proBNP use. GPs need further education in interpretation of ECGs, but seem to be more comfortable in using tests where either a numerical value is provided or a clinical report supplied. If the ECG and natriuretic peptides are to be used for triage of patients with suspected HF further education and diagnostic systems are needed. We believe this study strengthens the case for establishment of specialist HF clinics in the NHS.
heart failure; service models; diagnostics
301 HOW DO PRIMARY CARE TRUSTS PROVIDE HEART FAILURE CARE IN ENGLAND?
J. Murphy1, R. Chakraborty1, R. Brennan1, A. Fuat1, J. Cleland2, M. Davies3.1Darlington Memorial Hospital, Darlington, UK; 2Castle Hill Hospital, Hull, UK; 3Queen Elizabeth Hospital, Birmingham, UK
Introduction: Establishing an accurate diagnosis is essential for appropriate management of heart failure. As the symptoms are often non-specific, the National Institute for Clinical Excellence and European Society of Cardiology suggest using natriuretic peptides and/or electrocardiography to triage referrals. The National Service Framework recommends different service models including open access echocardiography (OAE) or heart failure clinics (HF clinics) as the next stage. Increasingly primary care trusts (PCTs) are expected to commission these services and provide chronic disease management. This survey was conducted on behalf of the British Society for Heart Failure to examine the resources available to, and services currently provided by, PCTs in England.
Method: Questionnaires were sent to all 303 PCTs with two further mailings for non-responders. To date 210 (69%) replies have been received.
Results:
Primary care diagnostics: 55 (26%) have used/are using natriuretic peptides (B type natriuretic peptide (BNP) 46, NT pro-BNP in 9). 151 (72%) use OAE and 88 (42%) can refer to a dedicated HF clinic. 48 (23%) have a GP with special interest in heart failure or cardiology. Secondary care: leading HF services in the main referring hospital was a cardiologist in 127 (60%), an elderly care physician in 29 (14%) and other physicians in 46 (22%). Eight PCTs felt there was no coordinated secondary care service. Of the 88 HF clinics, 78 (89%) were provided by cardiologists and the remaining 10 by elderly care physicians, 30 involved GPs, all had HF nurses and 13 (15%) pharmacists. Disease management: 130 (63%) of PCTs employed/had access to HF nurses, including 56 who have more than 1. A further 39 (20%) had coronary heart disease nurses who saw patients with heart failure. In a further 12 (6%), HF patients were seen by the practice nurses. Of the 130 HF nurses, 122 titrate beta-blockers, 101 in hospital clinics, 43 through GP surgeries and 56 when seeing patients at home. 55 PCTs provide some form of rehabilitation for HF patients.
Conclusion: This survey confirms wide variation in PCT approaches to heart failure resulting in different models of care. Natriuretic peptide measurement has been adopted by a minority of PCTs whereas OAE is more widely but not universally available. Less than half the PCTs have access to a heart failure clinic, which if present is generally provided by a cardiologist. Elderly care physicians and other physicians are seen to lead HF services a third of the time. More than 1/3 of PCTs do not have HF nurses so coronary heart disease nurses or practice nurses are often used. The majority of HF nurses now titrate beta-blockers, usually in hospital but often in other environments. This survey highlights a number of areas where sharing of good practice is required to optimise patient care.
heart failure; primary care; diagnosis
302 NATIONAL DATA ON MANAGEMENT PATTERNS OF 7632 PATIENTS ADMITTED WITH HEART FAILURE IN THE UK: ON BEHALF OF THE HEALTHCARE COMMISSION AND THE BRITISH SOCIETY FOR HEART FAILURE
B. Fittall1, A. Bakhai2, R. Jobanputra1, J. Cleland3, T. McDonagh4, H. Dargie5, M. Cowie4.1Acute Hospital Portfolio, Healthcare Commission, London, UK; 2Barnet & Chase Farm NHS Trust, London, UK; 3Castle Hill Hospital, University of Hull, Kingston-upon-Hull, UK; 4National Heart & Lung Institute, Imperial College, London, UK; 5Western Infirmary, University of Glasgow, Glasgow, UK
Aim: Practice patterns of management of patients admitted with heart failure vary with respect to investigations, medical therapies and mortality. We sought to undertake a contemporary review of the management of such patients as part of the Healthcare Commission survey of acute admissions and its overall improvement review of Heart Failure services.
Methods: Trusts in England, Wales and Northern Ireland were asked to submit data electronically using a survey of at least 50 unselected patients admitted as an emergency and discharged or deceased with a diagnosis of heart failure (ICD 10 codes I50) prior to 30 September 2005.
Results: Preliminary results on the first 7632 records received from 141 acute trusts are tabled, subdivided by age 75.
Abstract 302
Conclusions: In 2005, following an emergency admission involving heart failure, one in six patients do not survive to discharge with higher death rates in the elderly. For the majority of patients, echo data appear to be unavailable during admission and the use of evidence-based therapies is not optimial, particularly in older patients. A concerted and multidisciplinary approach is urgently needed to significantly reduce mortality and improve the management of heart failure patients nationally.
heart failure; national improvement programme; mortality
303 IMPROVED OUTCOMES FOLLOWING HOSPITALISATION IN PATIENTS WITH A NEW DIAGNOSIS OF HEART FAILURE: RESULTS FROM A RANDOMISED CONTROLLED TRIAL OF A NOVEL, NURSE-LED SELF-MANAGEMENT INTERVENTION
A. Zaphiriou1, K. Mulligan2, P. Hagrave3, D. Patterson4, M. Cowie5, S. Newman2, S. Hardman4.1National Heart & Lung Institute, Imperial College and Whittington Hospital, London, UK; 2The Centre For Behavioural And Social Sciences In Medicine, UCL, London, UK; 3Clinical Cardiology, Whittington Hospital, London, UK; 4Clinical and Academic Cardiology, Whittington & UCL Hospitals, London, UK; 5National Heart & Lung Institute, Imperial College, London, UK
Background: Readmission and mortality rates are high following hospitalisation with heart failure. Interventions have shown reductions in admissions due to heart failure. Variable mortalities have been observed. We report a randomised controlled trial (RCT) of a low-intensity intervention. This was designed to improve self-management using a problem-solving approach. The aim of the RCT was to establish whether or not the intervention would confer benefit in a setting where inpatient optimisation of heart failure care was standard.
Methods: Patients admitted with heart failure (ESC diagnostic criteria) were managed according to a protocol including shared care with heart failure cardiologists and inpatient optimisation of therapy. Patients were recruited to the RCT when stable on optimal treatment. Those allocated to the intervention were visited, twice in hospital and then once at home within 10 days, by the heart failure nurse specialist delivering the intervention.
Results: A total of 165 patients were recruited, median age 74 (range 21–94), 58% male, LV systolic impairment was severe, moderate, and mild in 37%, 36% and 17% of patients (10% had AF and/or valve disease). 85 were randomised to the intervention. At presentation patients were NYHA III or IV. By recruitment 8% were NYHA I and 67%, 24% and 1% were NYHA II, III, and IV, respectively. At one year there were no significant differences in readmission rates, inpatient days, or all-cause mortality (29 deaths or 17.6%) between the randomised groups. However, a secondary analysis revealed that the intervention was effective in the 90 patients admitted to hospital with incident (new) heart failure. In the intervention group the time to first event (admission due to heart failure or death) increased (p = 0.012) and at 12 months fewer patients had reached this endpoint (p = 0.012). There were also fewer patients admitted (p = 0.013), and a reduction in total admissions (p = 0.01) and inpatient days (p = 0.011) for worsening heart failure. There were fewer deaths in the intervention group but this was of borderline statistical significance (p = 0.052).
Abstract 303
Conclusions: This low intensity intervention, designed to encourage patient self-management, improved 1 year outcomes for patients admitted to hospital with incident heart failure, including heart failure readmission rates and duration of those admissions, without any mortality cost. Indeed there was a reduction in death and heart failure readmissions and a strong trend towards a reduction in mortality, in the context of an already low mortality rate for the whole cohort, relative to the published literature. Given the high risk population studied, the overall mortality likely reflects optimisation of inpatient management as standard care. The additional benefits reported suggest patients with incident heart failure may be more amenable to the problem-solving approach used in the intervention to improve self-management of their heart failure. This was in contrast to those who have been diagnosed with heart failure for some time and who are likely to have established patterns of behaviour to deal with their condition.
heart failure; outcomes; self management

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
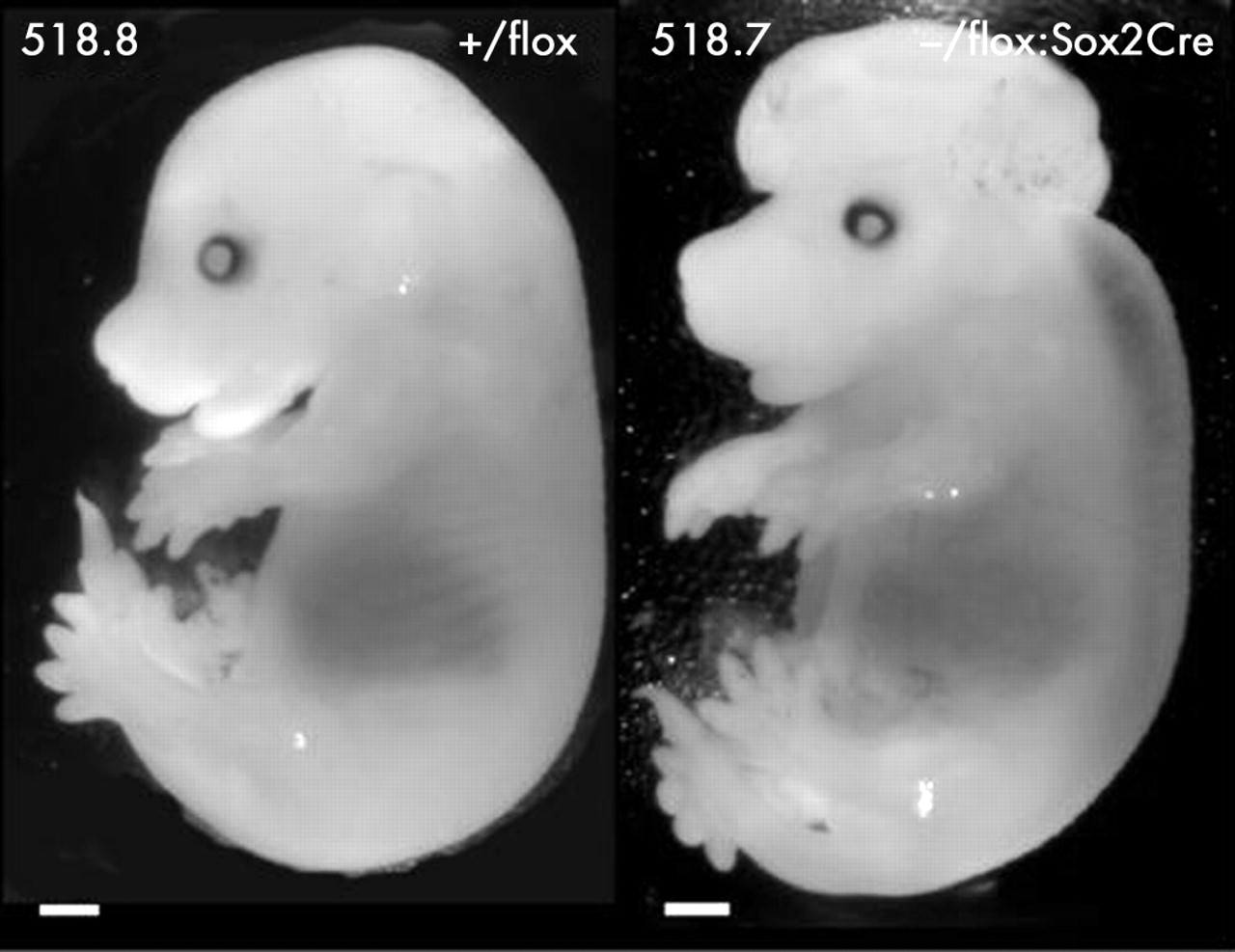{kind=link}
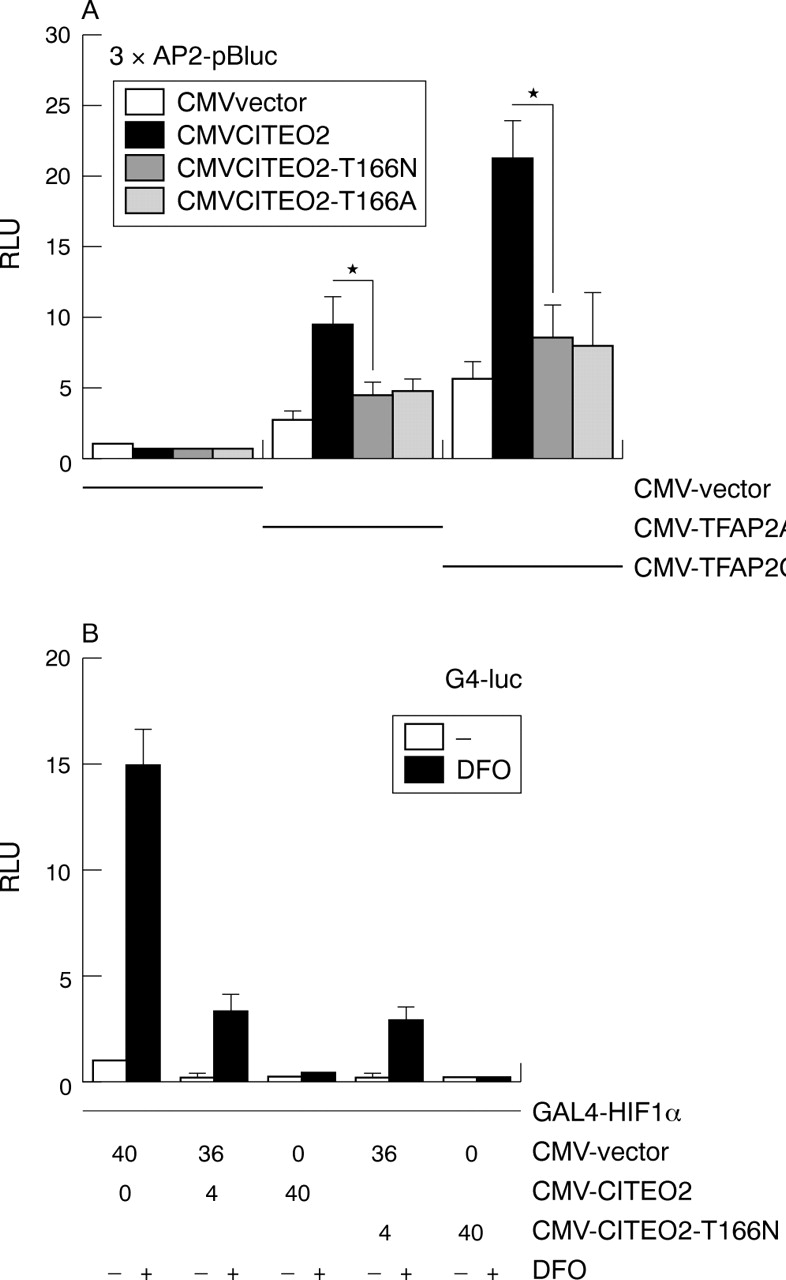{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
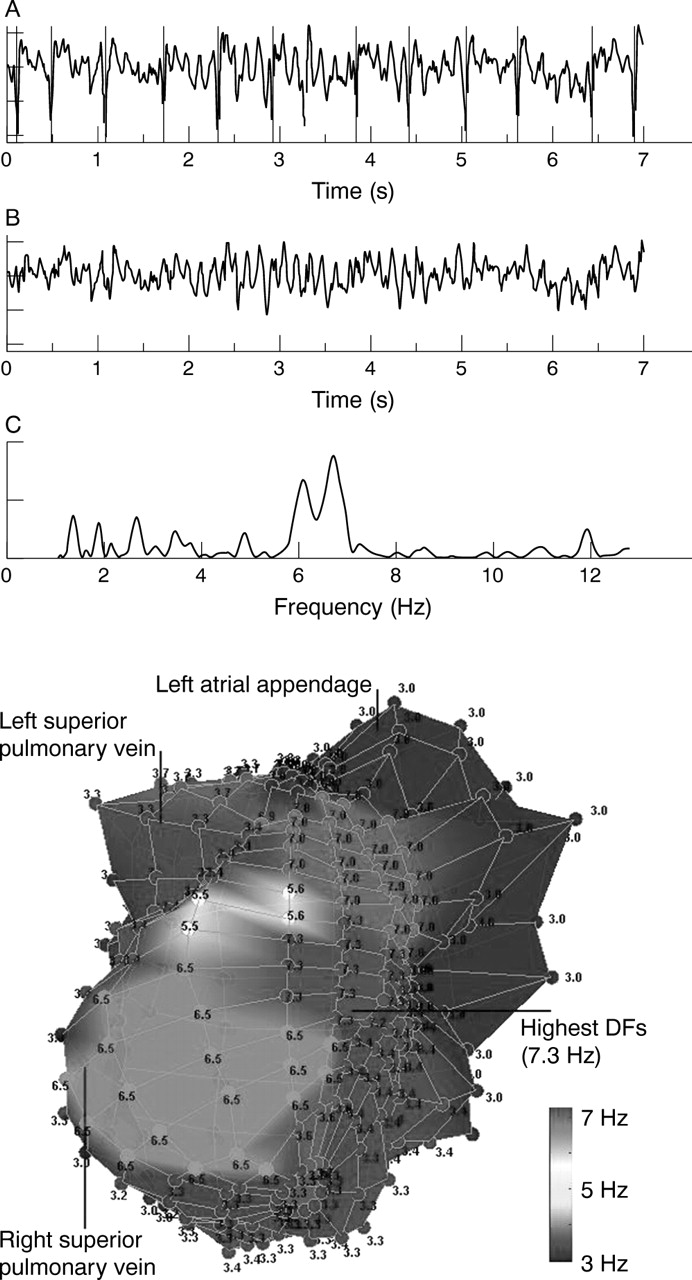{kind=link}
{kind=link}
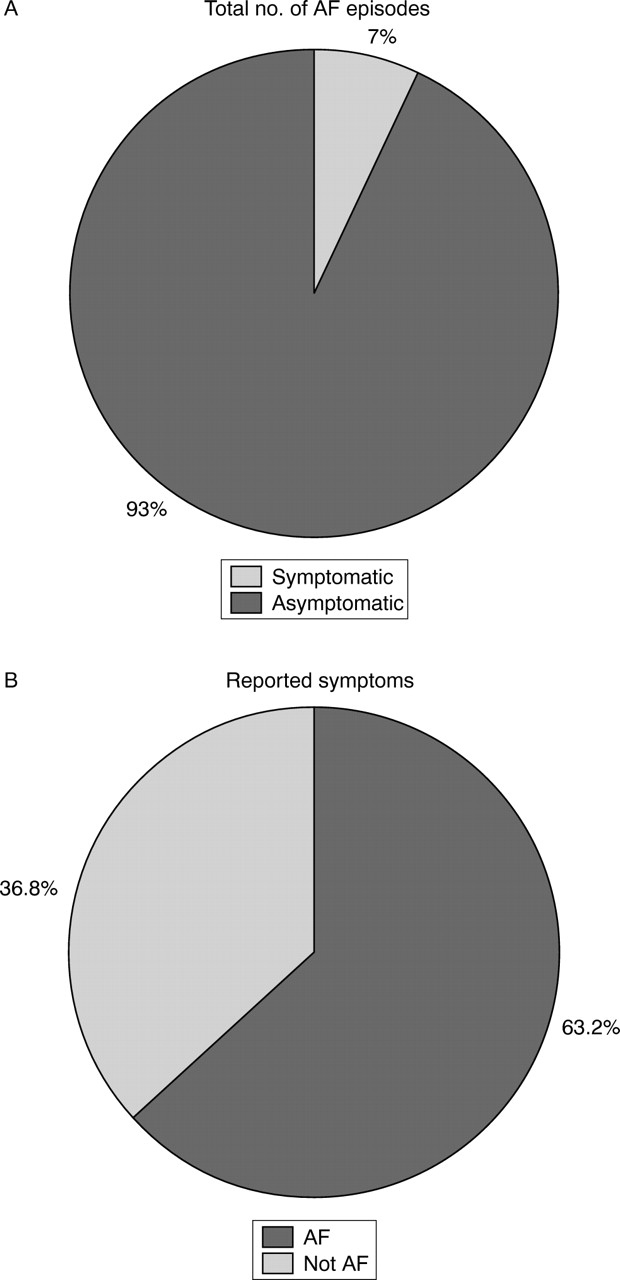{kind=link}
{kind=link}
{kind=link}
{kind=link}
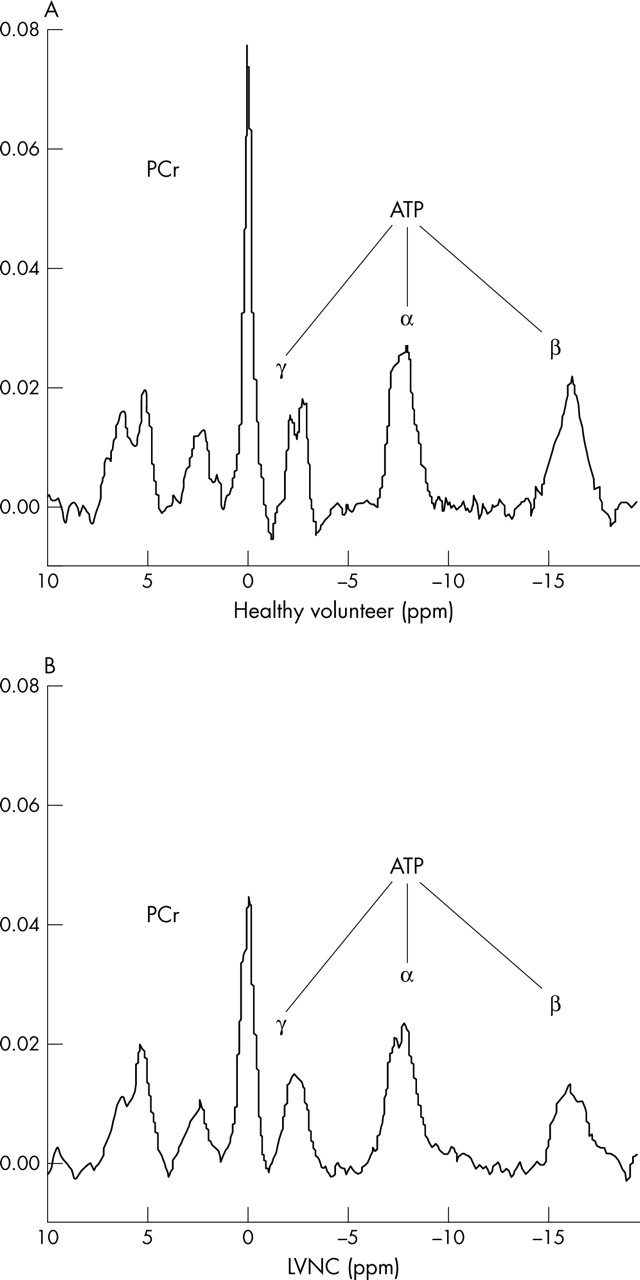{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
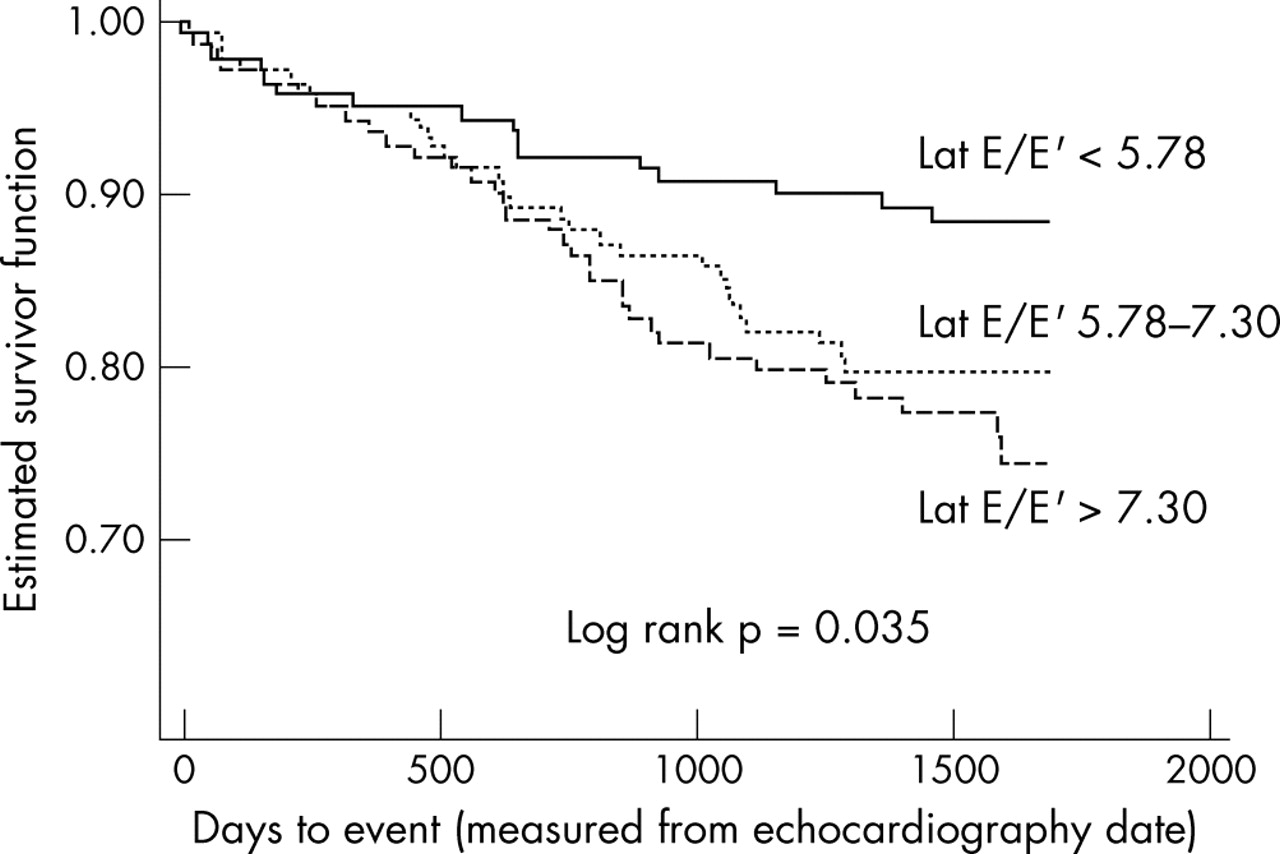{kind=link}
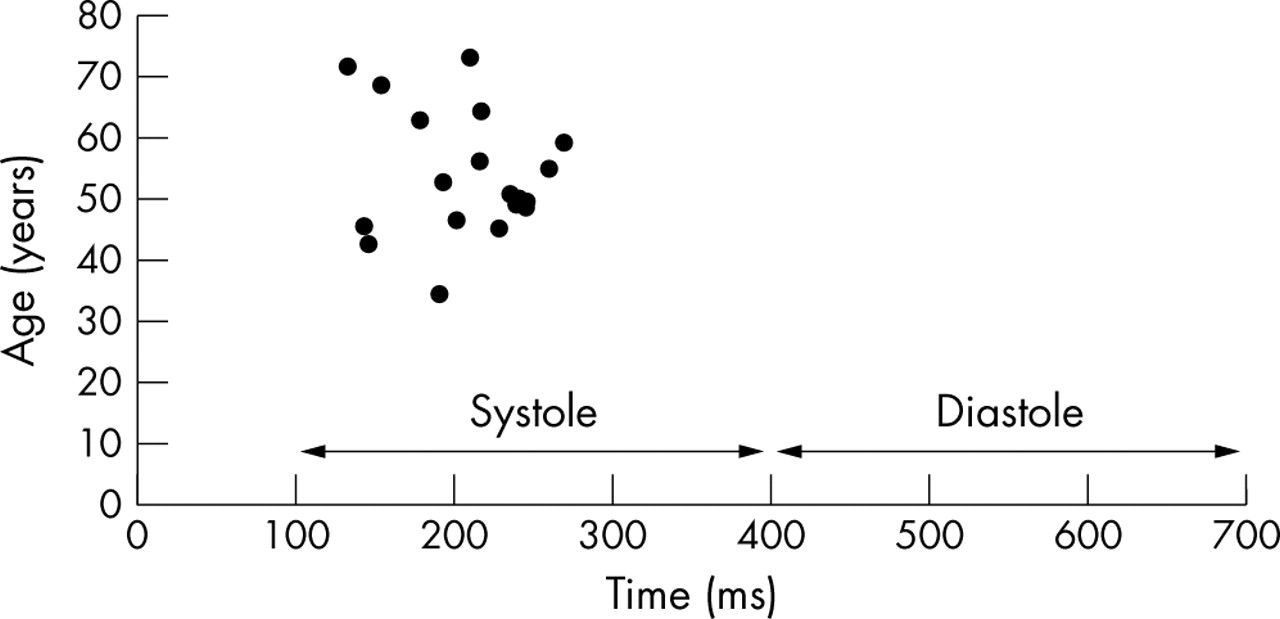{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
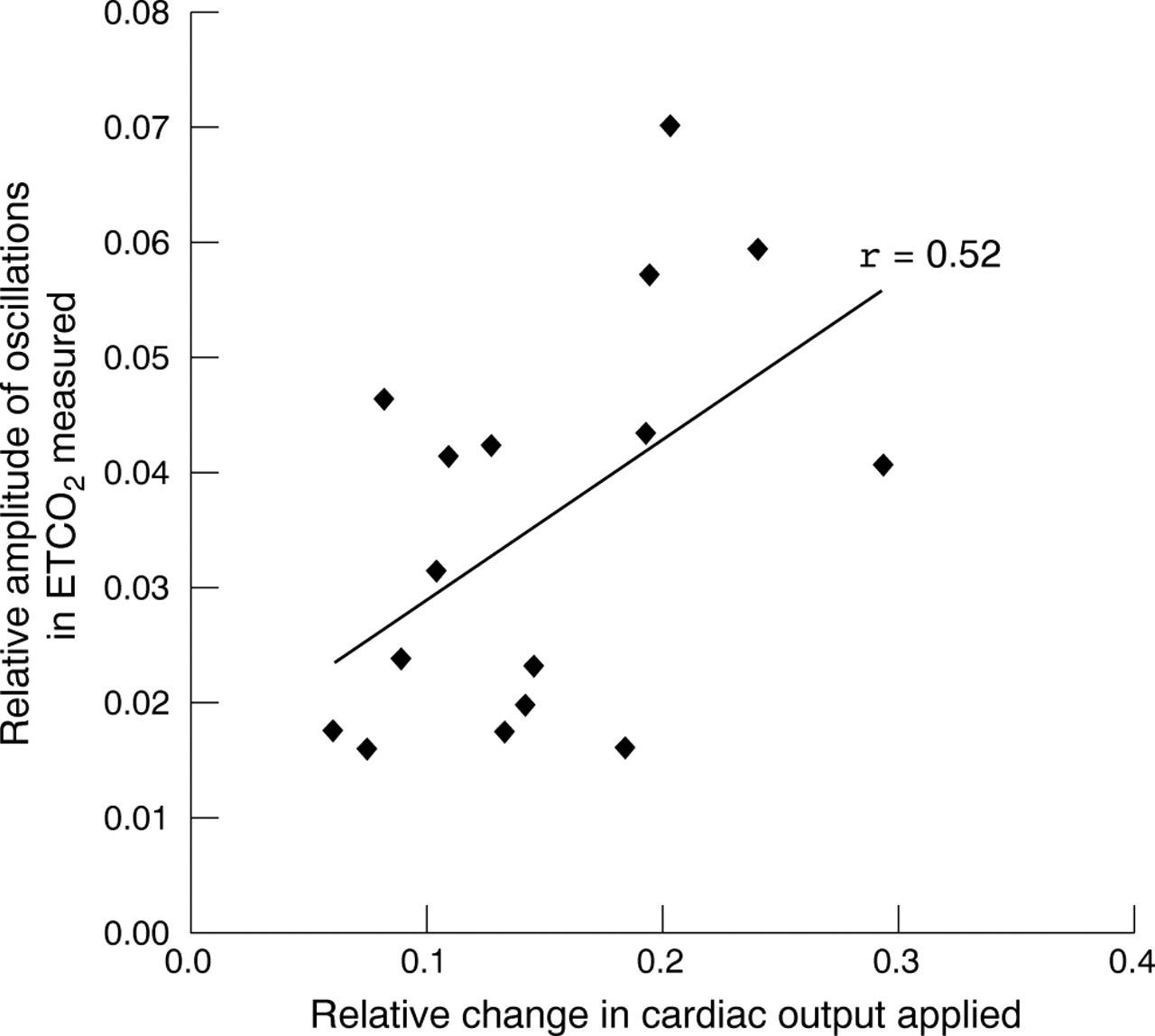{kind=link}
{kind=link}
{kind=link}
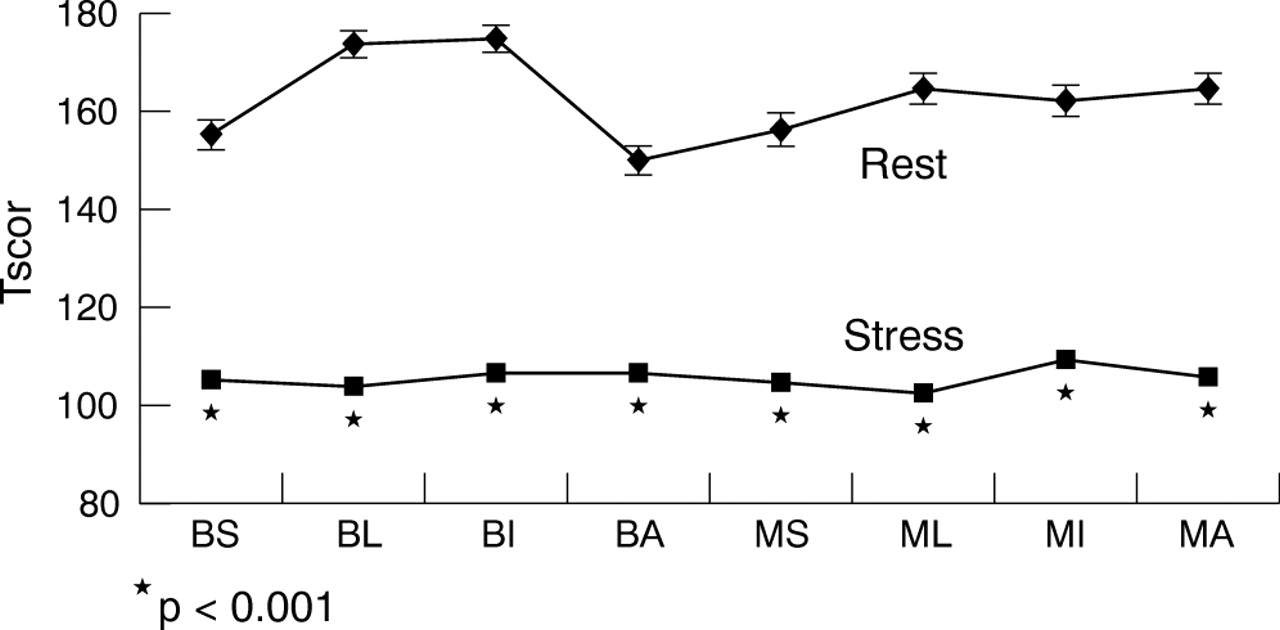{kind=link}
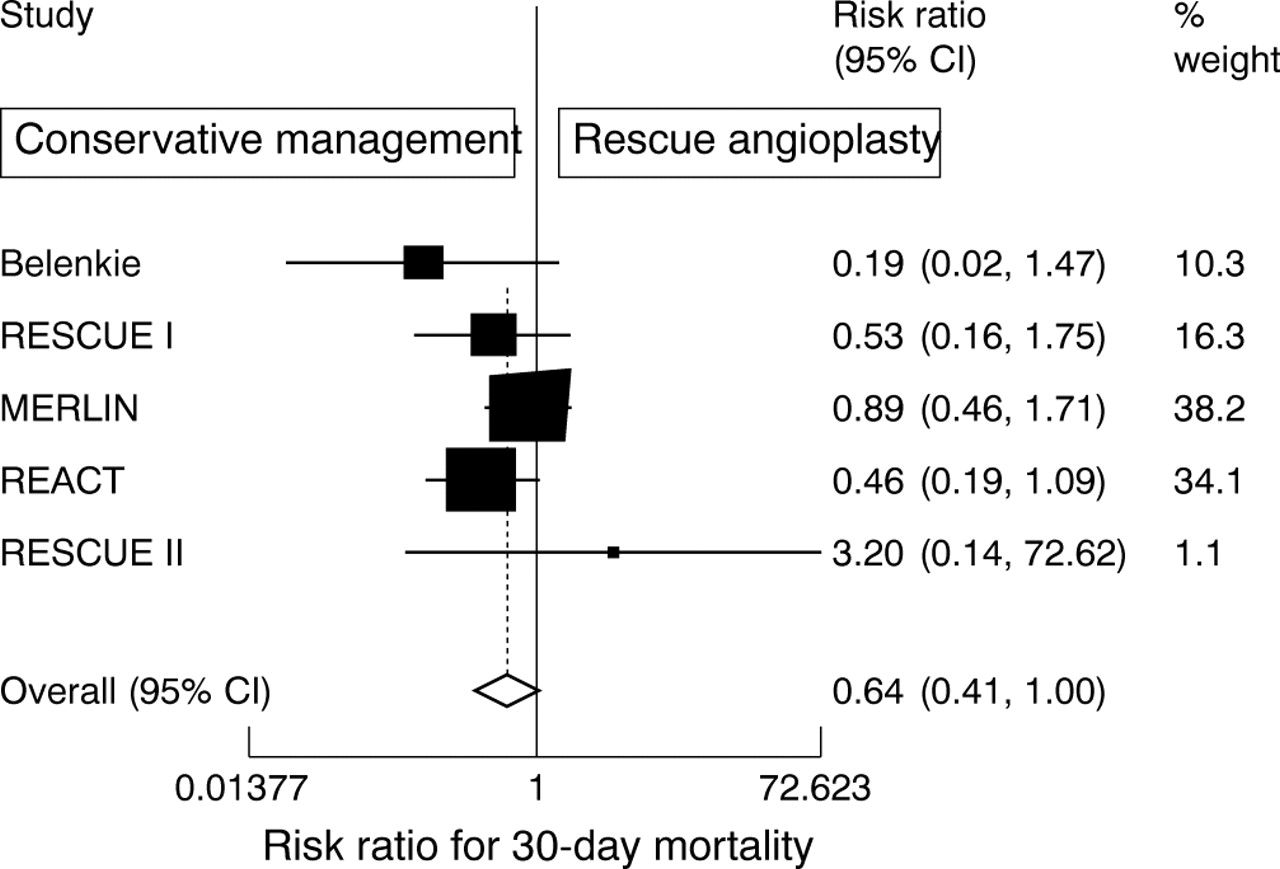{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
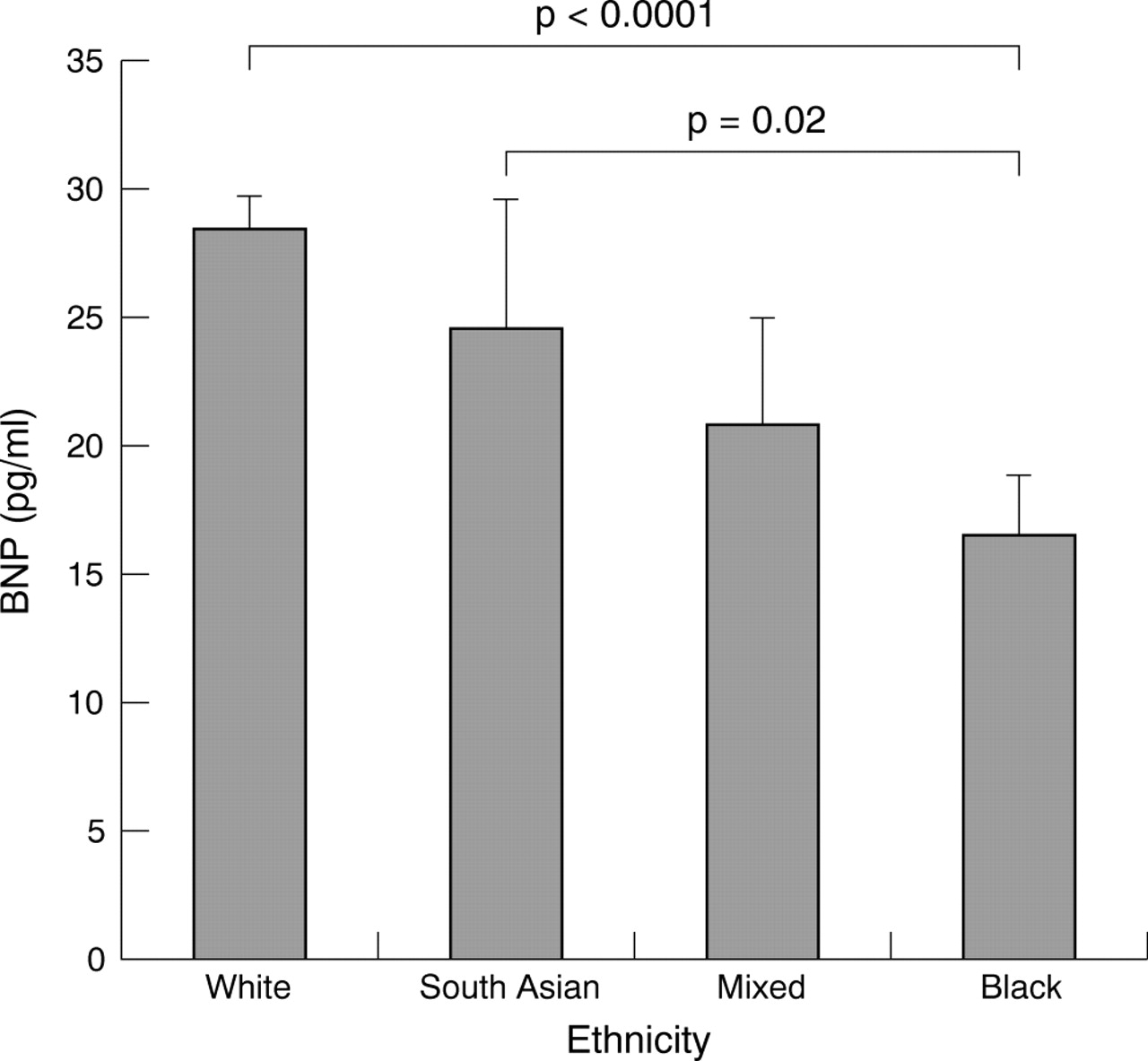{kind=link}
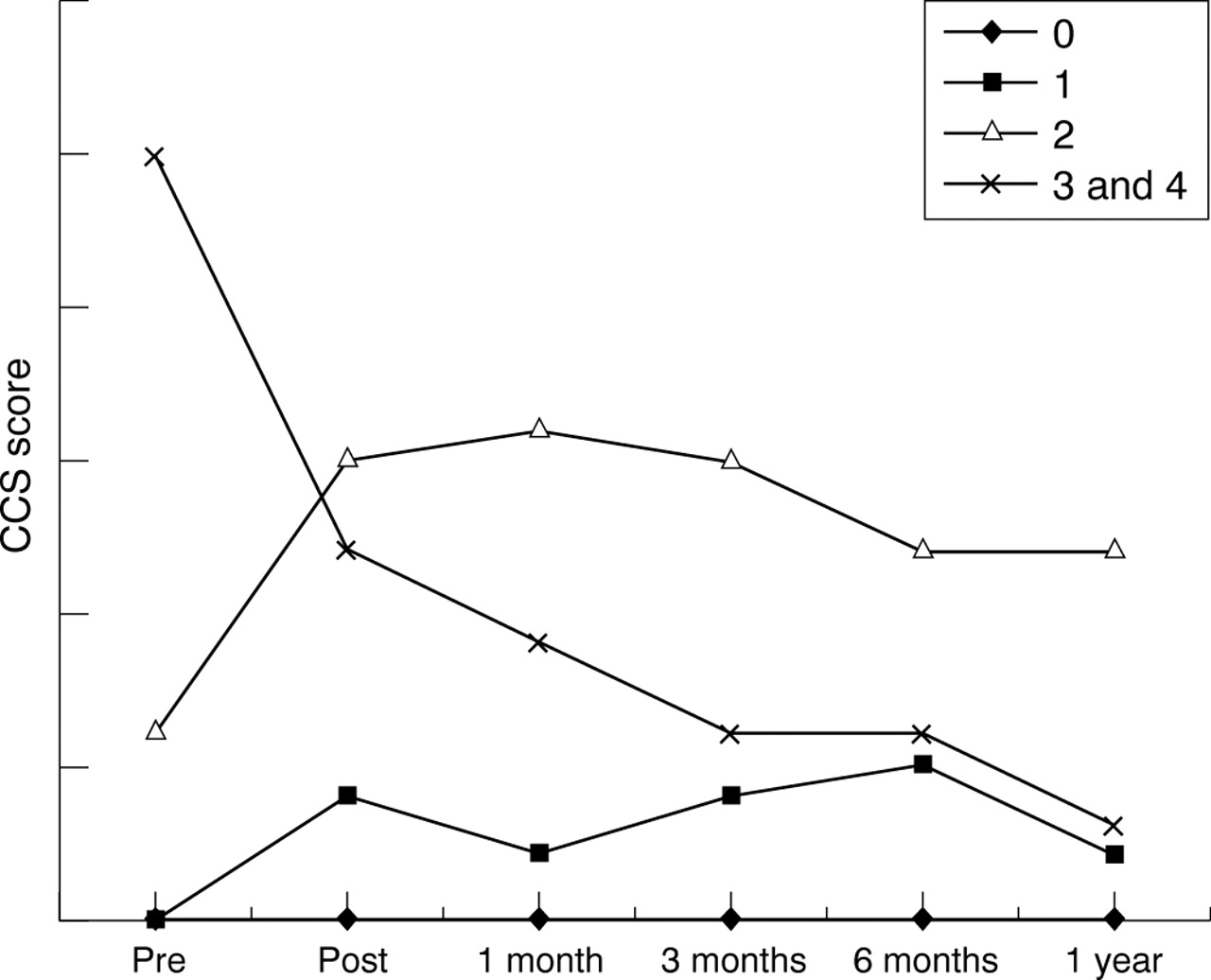{kind=link}
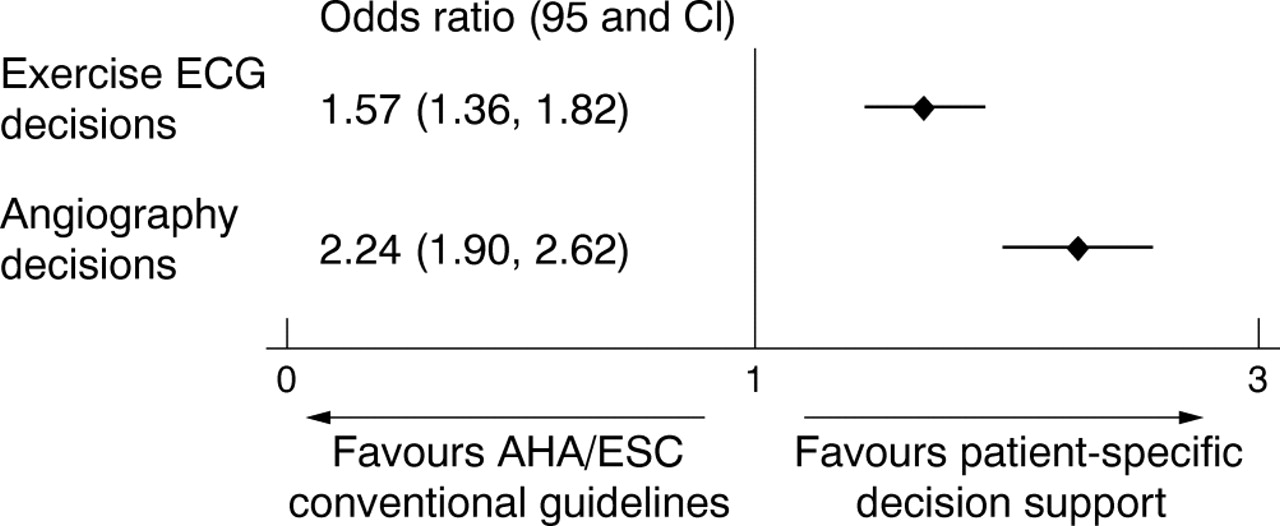{kind=link}
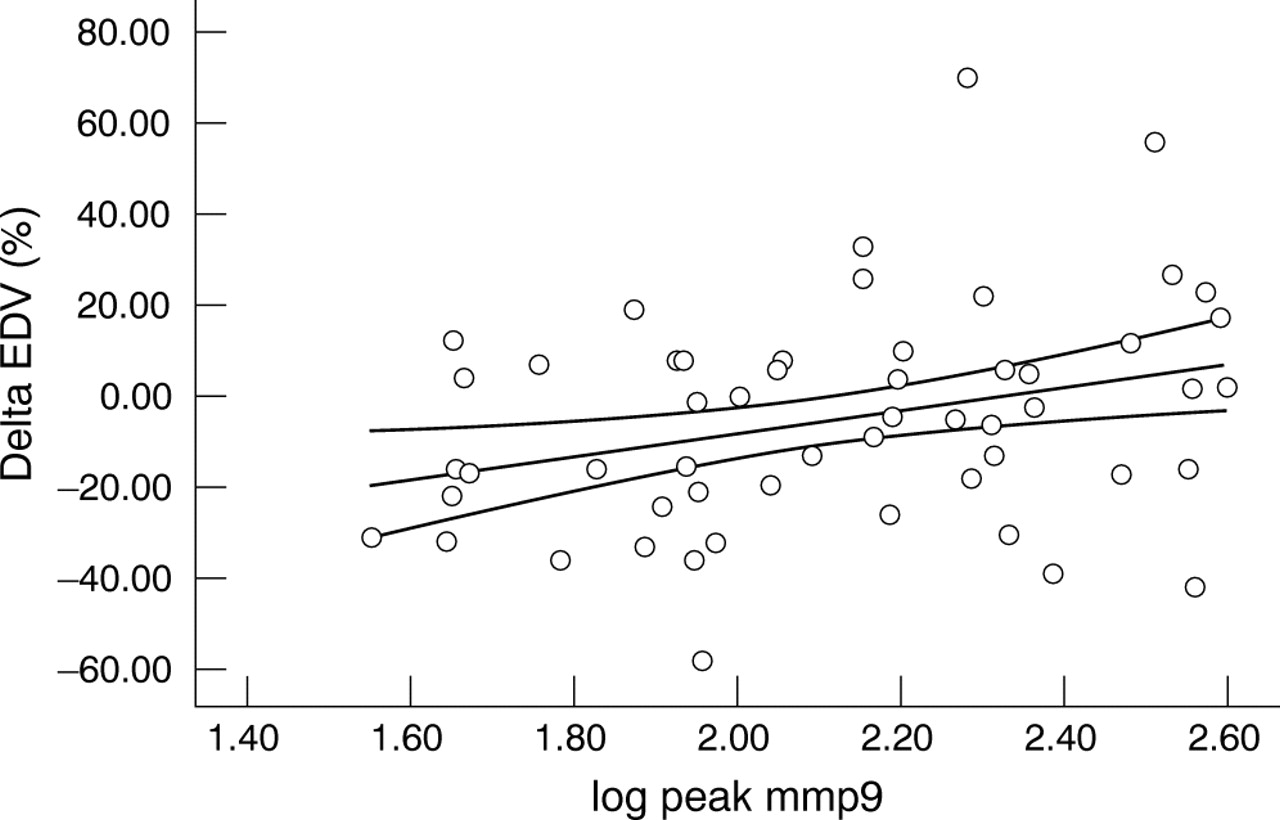{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
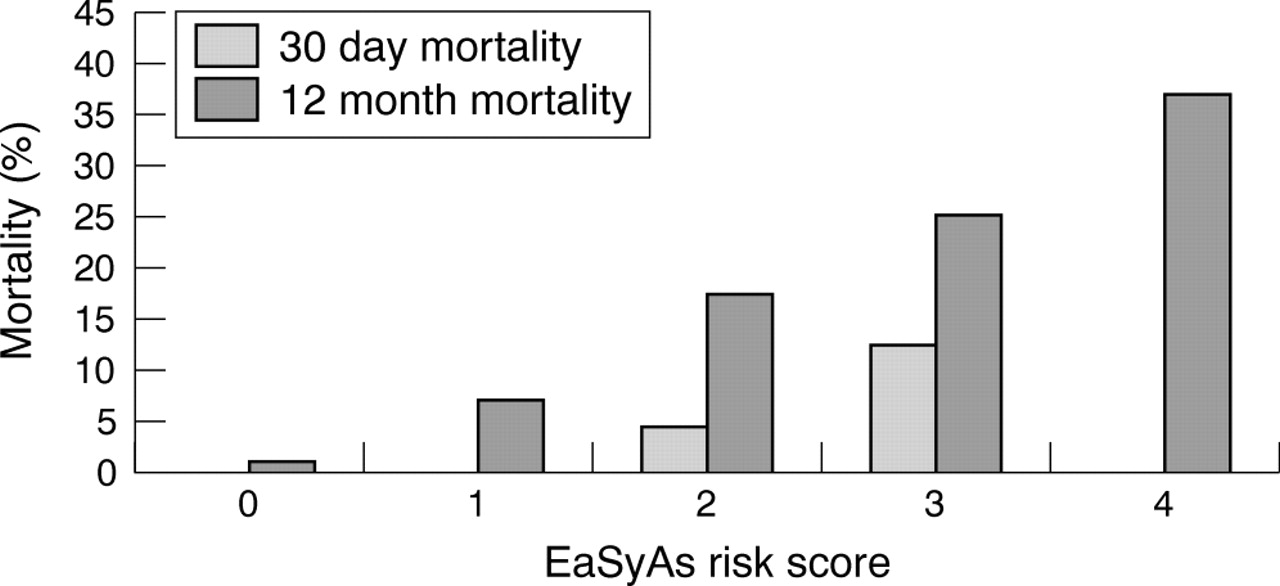{kind=link}
{kind=link}
{kind=link}
{kind=link}
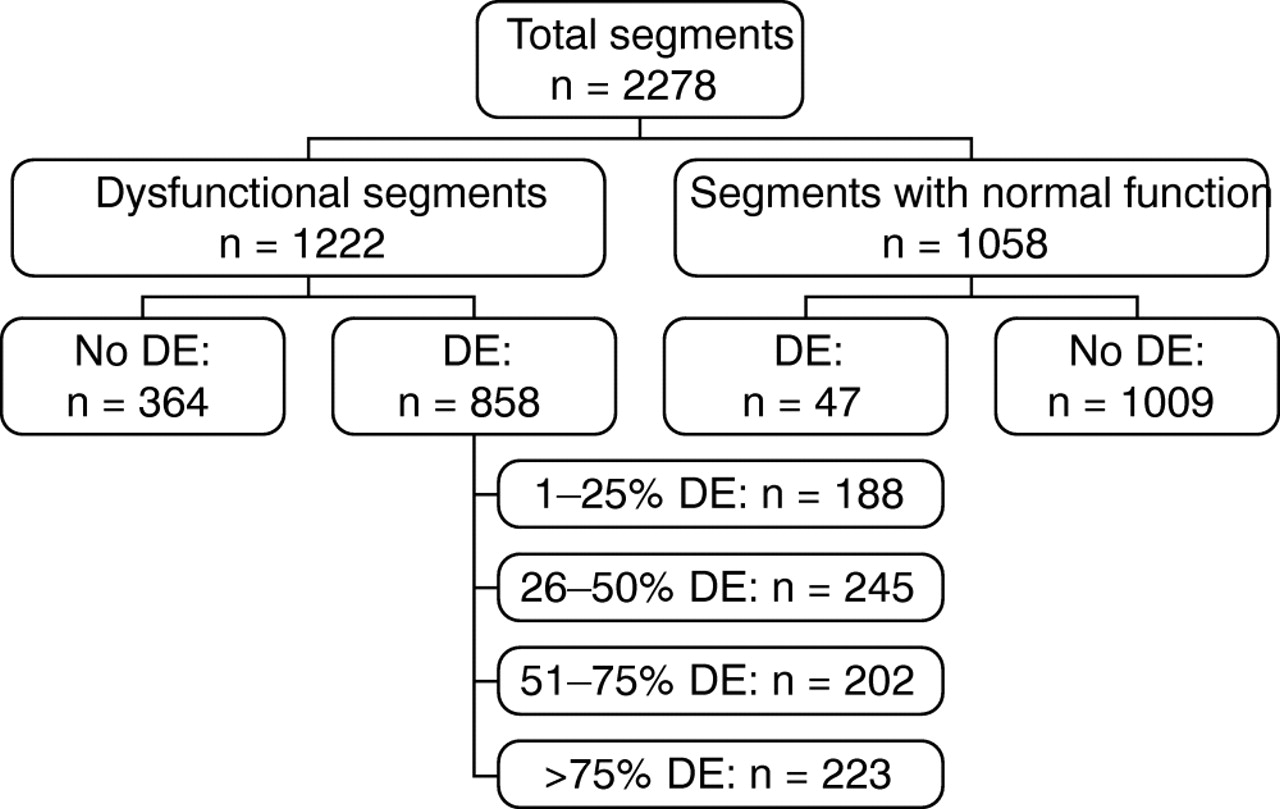{kind=link}
{kind=link}
{kind=link}
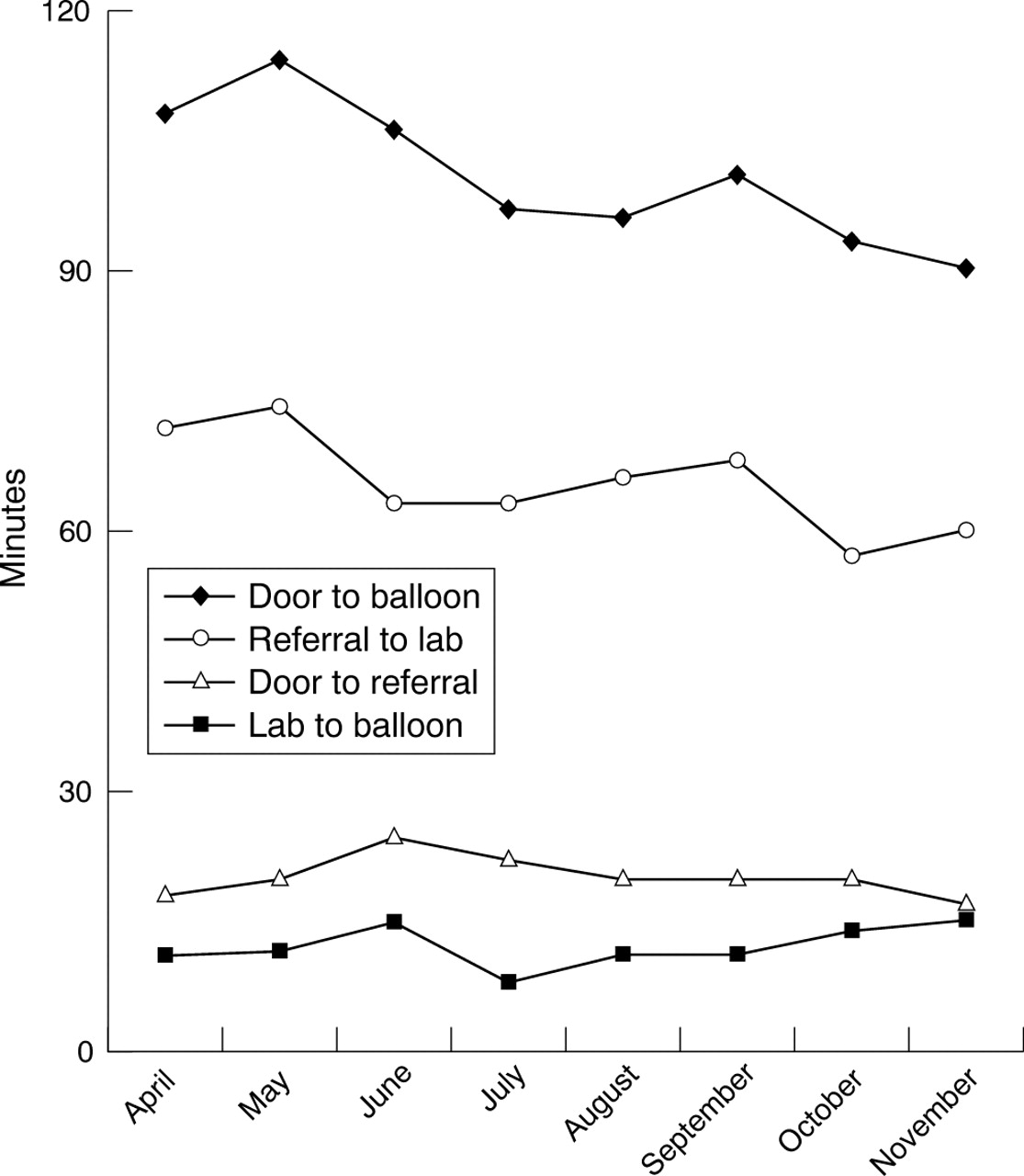{kind=link}
{kind=link}
{kind=link}
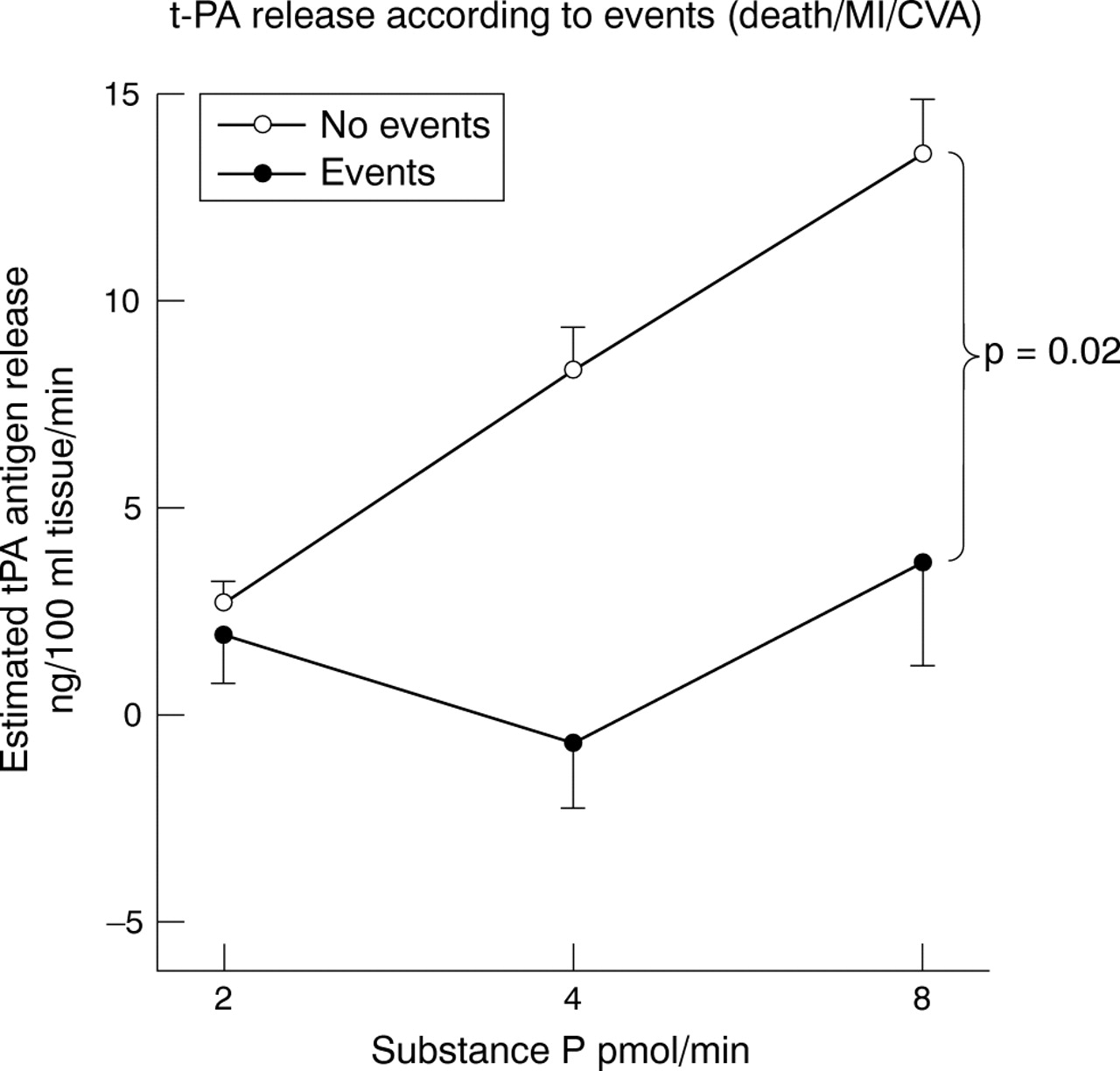{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
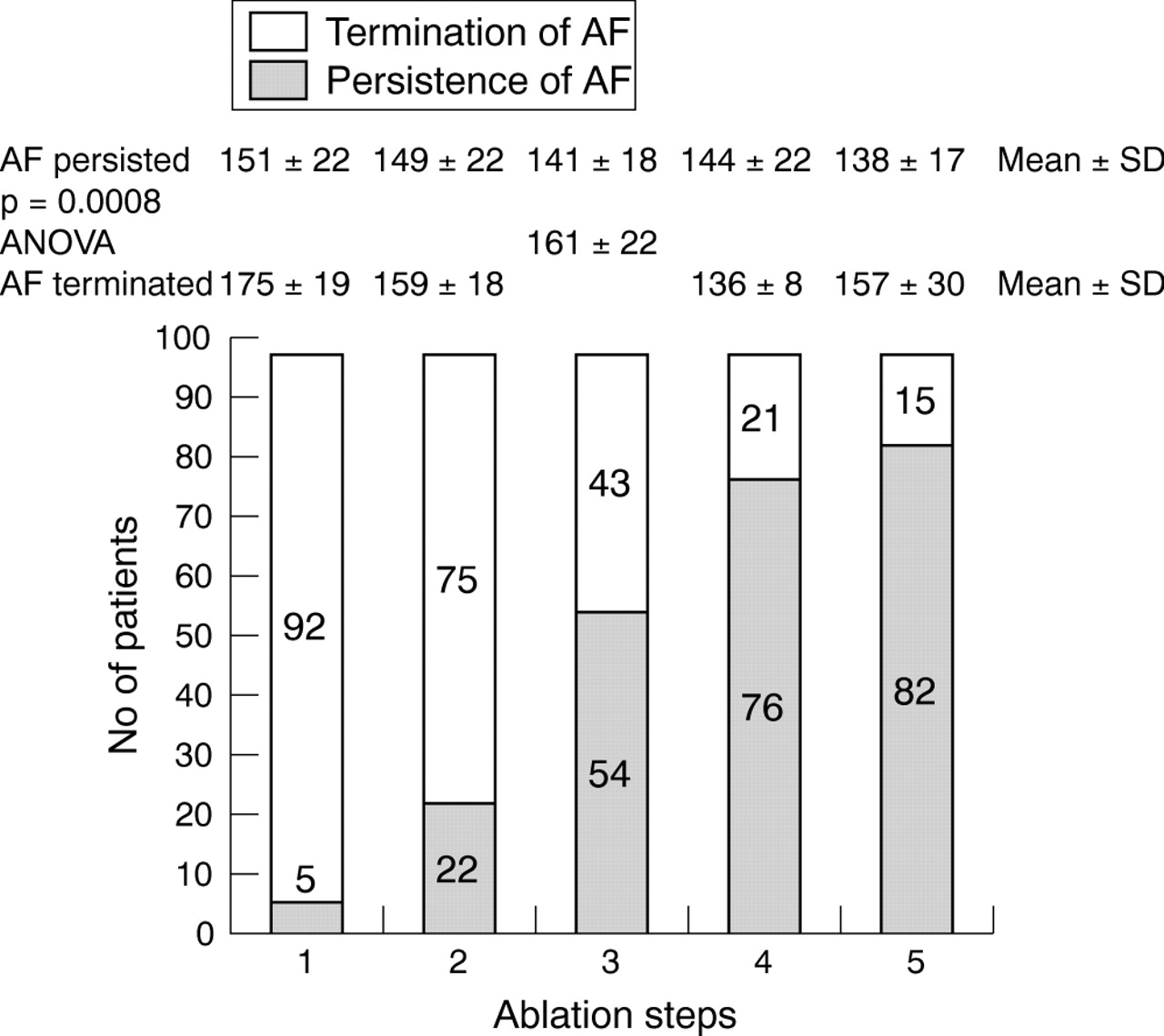{kind=link}
{kind=link}
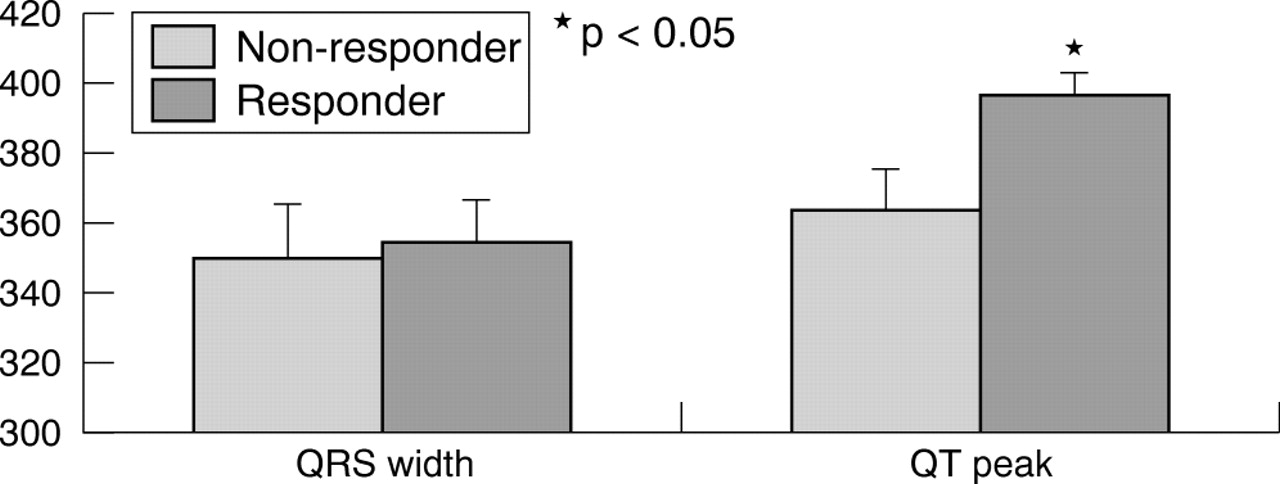{kind=link}
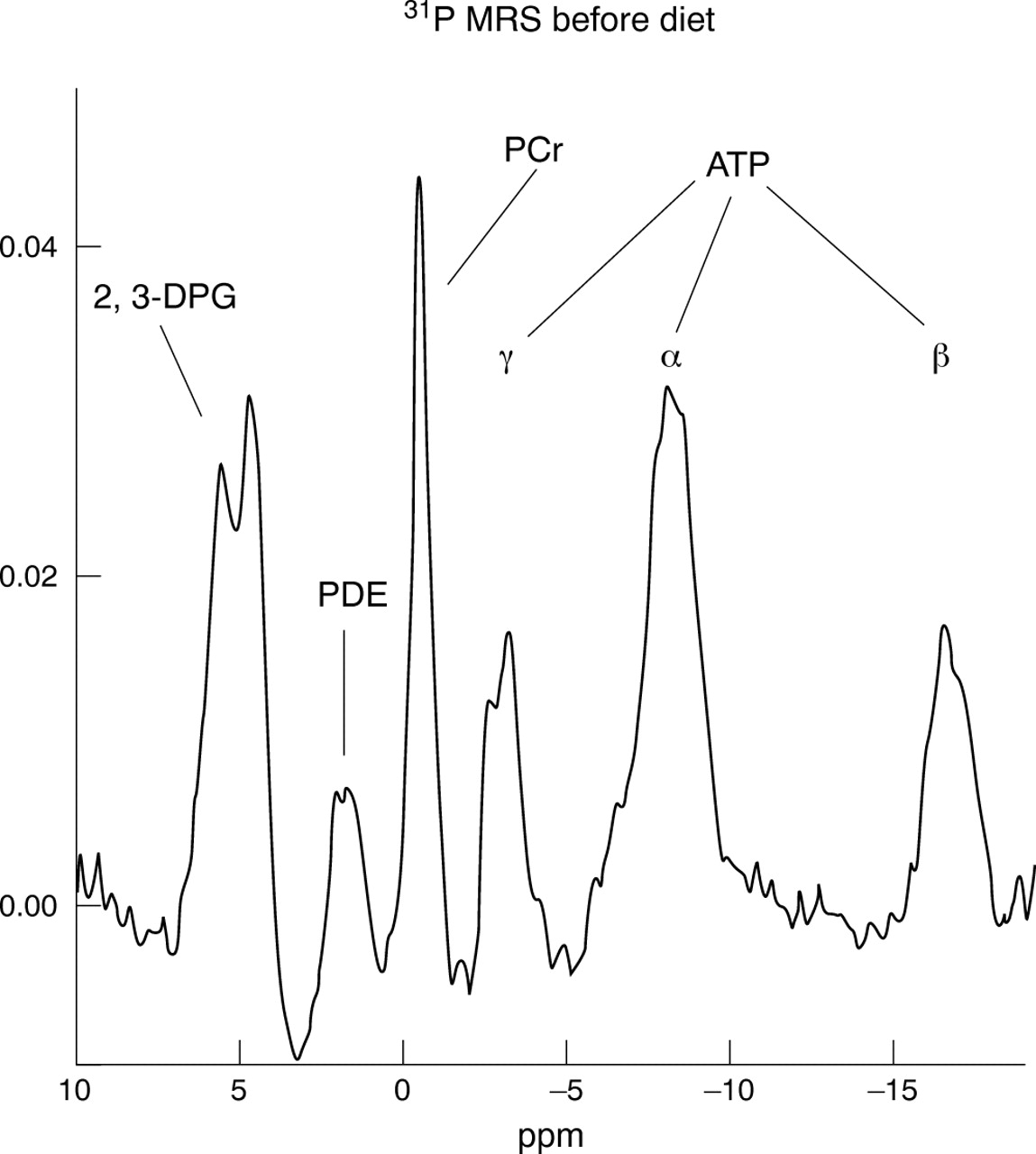{kind=link}
{kind=link}
{kind=link}
{kind=link}
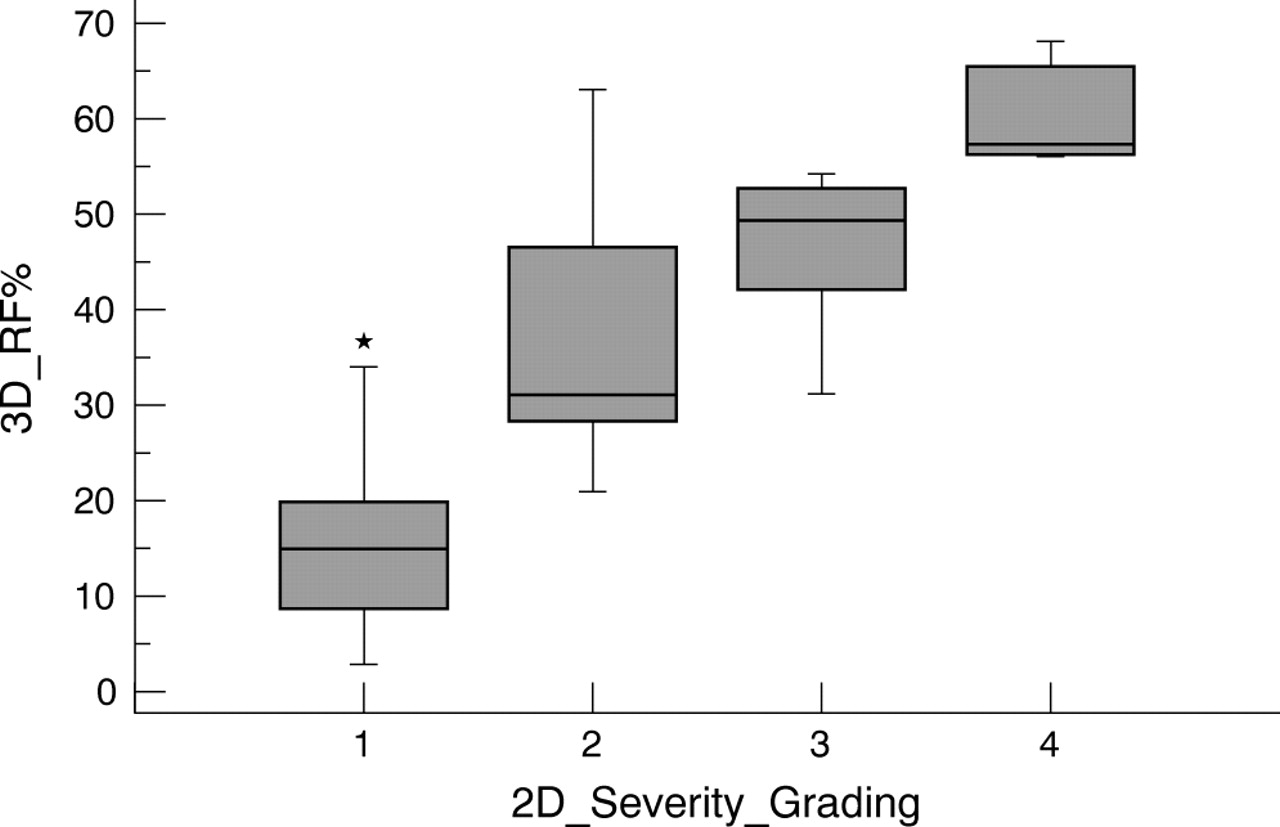{kind=link}
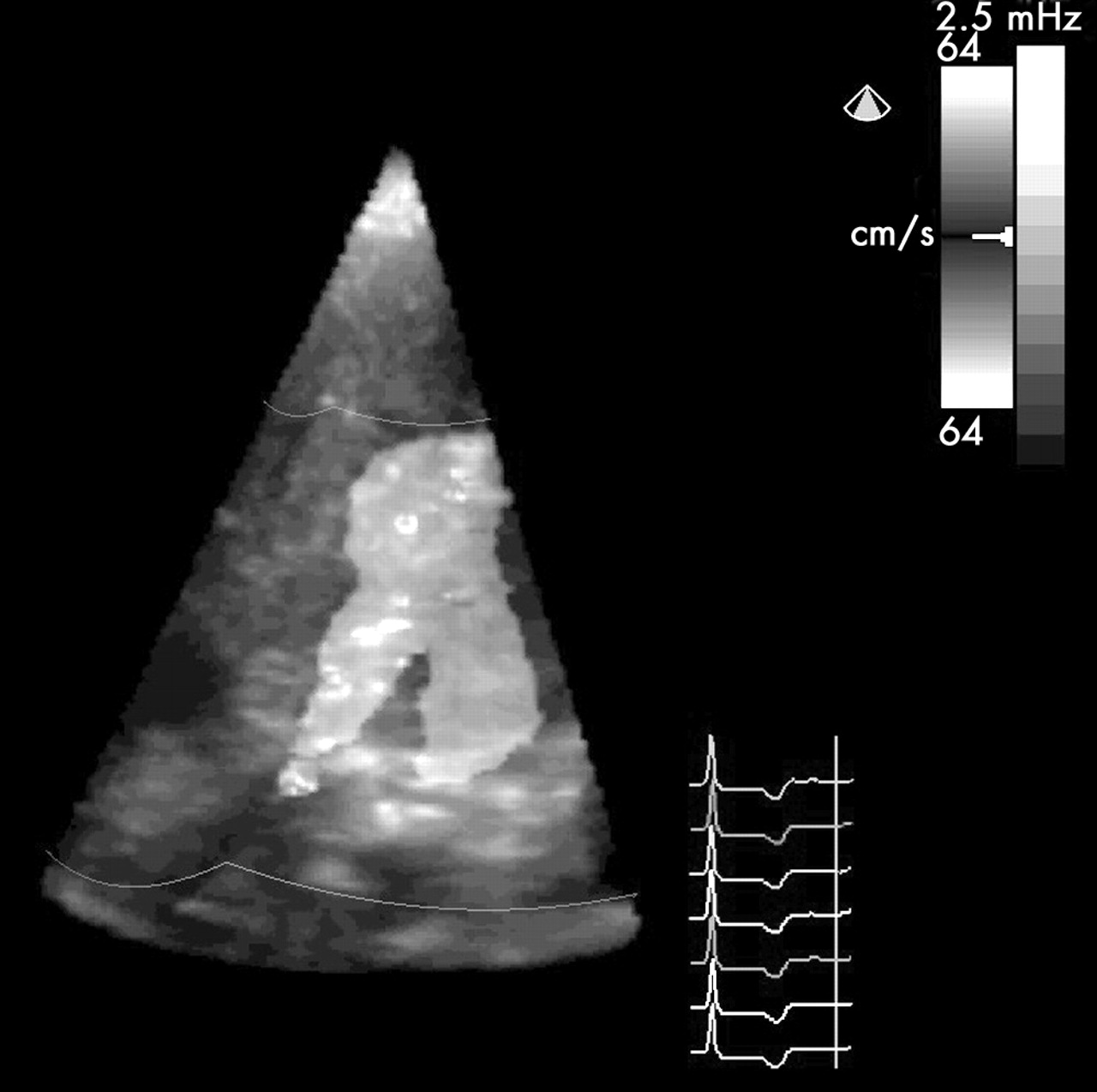{kind=link}
{kind=link}
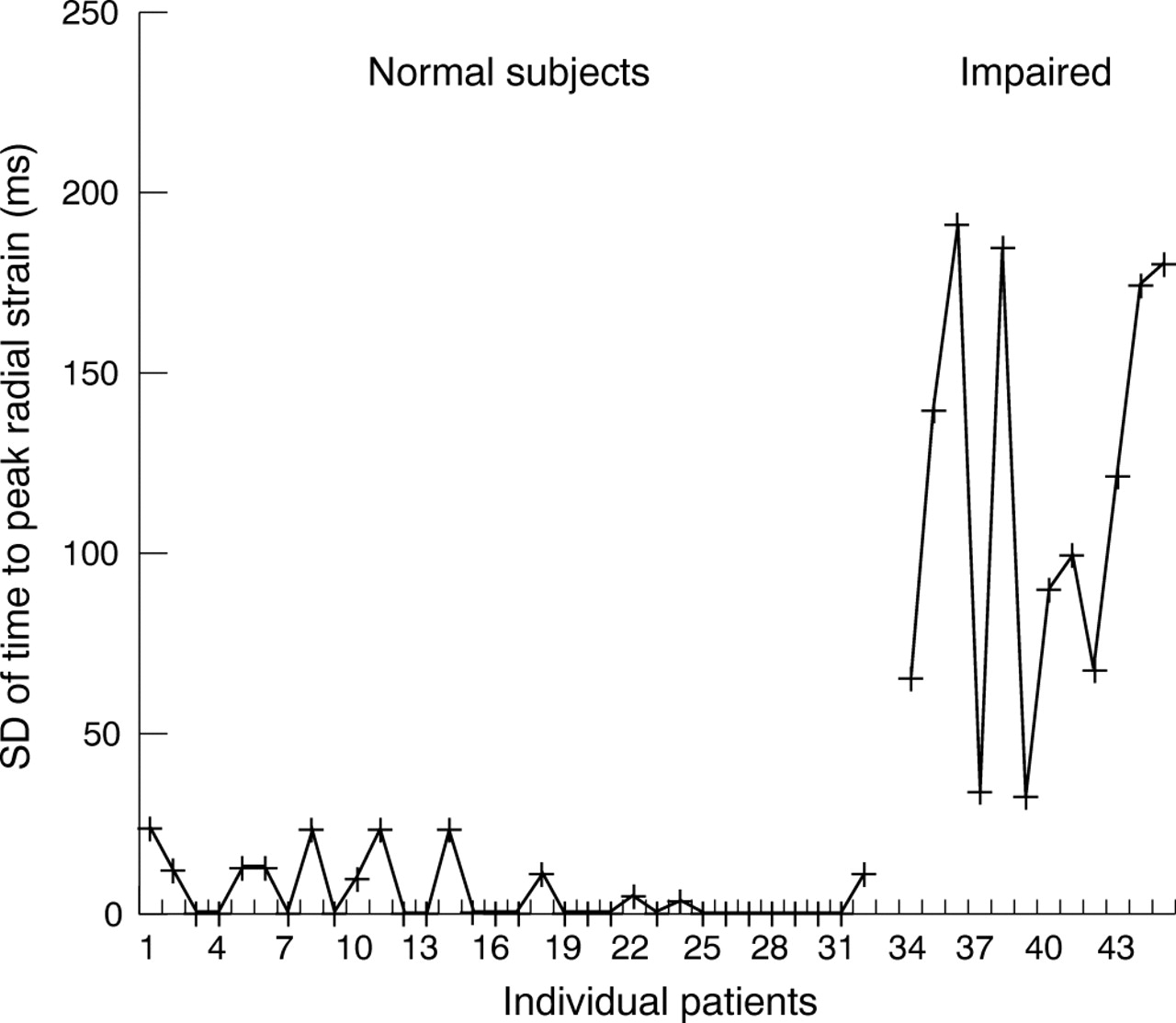{kind=link}
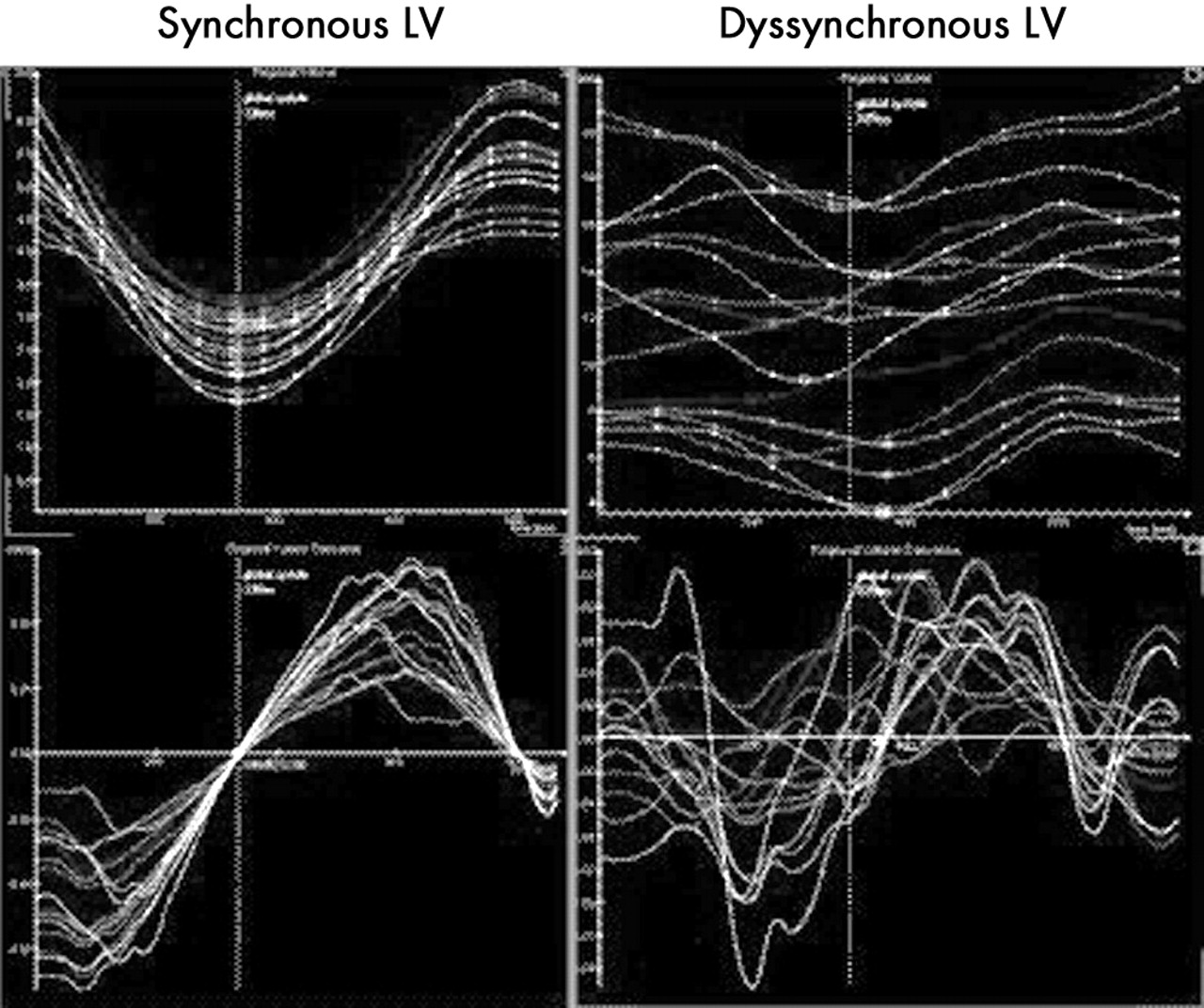{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract G303 Patients with incident heart failure.
304 A RANDOMISED CONTROLLED TRIAL OF HOME-BASED MEDICATION REVIEW AND LIFESTYLE ADVICE BY COMMUNITY PHARMACISTS FOR PATIENTS WITH HEART FAILURE
R. Holland1, I. Brooksby2, E. Lenaghan1, K. Ashton1, L. Hay3, R. Smith1, L. Shepstone1, A. Howe1, A. Lipp4, C. Daly1, I. Harvey1.1University of East Anglia, Norwich, UK; 2Norfolk and Norwich University Hospital NHS Trust, Norwich, UK; 3ISD Scotland, Edinburgh, UK; 4Great Yarmouth Primary Care Trust, Gt Yarmouth, UK
Introduction: Multi-disciplinary interventions including medication review, symptom self-management and lifestyle advice reduce admissions and mortality in heart failure. However, most trials have used small numbers of specialist staff to deliver interventions. Previous studies have not tested whether community pharmacists can deliver effective interventions to this patient group.
Methods: A randomised controlled trial recruiting patients from three acute hospitals in Norfolk if they were an emergency admission, had heart failure and were to be discharged home. The intervention involved two home visits by one of 18 community pharmacists within 2 and 8 weeks of discharge. Pharmacists reviewed medications and gave symptom self-management and lifestyle advice. Controls received usual care. The primary outcome was total hospital readmissions (all cause) at 6 months. Secondary outcomes included mortality, quality of life (Minnesota Living with Heart Failure questionnaire (MLHFQ) and EQ-5D), medication adherence (Medication Adherence Rating Scale), and behaviour change (European Heart Failure Self-Care Behaviour Scale).
Results: 339 patients were recruited; 47 patients were excluded after randomisation (18 died before discharge, 17 the heart failure diagnosis was not confirmed, 7 were not discharged home, and 5 were excluded for other reasons), leaving 292 patients in the trial (148 intervention, 144 control). 136 intervention patients (92%) received one or more visit. Interventions lasted a mean of 6 h, including approximately 2 h in patients’ homes, 2 h on administration and 2 h travelling. Self-report data has been collected with an overall response of 92% excluding deaths (75% when deaths are included). There were a total of 63 admissions reported in the intervention group and 71 in controls (rate ratio 0.82, 95% CI 0.57 to 1.19, p = 0.31, poisson model). 31 intervention patients died compared with 24 controls (Hazard ratio 1.24, 95% CI 0.72 to 2.11, p = 0.44). Although EQ-5D scores favoured the intervention group, MLHFQ scores favoured controls, but neither difference was statistically significant. Both groups reported good medication adherence with no difference observed, and improved heart failure self-care with results favouring the intervention group non-significantly.
Conclusion: This trial has failed to demonstrate that community pharmacist visits to heart failure patients post-hospital discharge providing advice and review, can lead to the gains in admissions, mortality, or quality of life observed in more intense specialist services. The decrease in admissions seen (18%) is in line with that demonstrated by systematic reviews, however, this was not statistically significant. Equally, there is the possibility of a Type II error as the study was powered to demonstrate a change of 40%. These are interim results, hospital episode statistics will be available in February 2006.
medication review; lifestyle/symptom self-management; pharmacist
305 OUTCOME AND RESPONSE TO CONTEMPORARY TREATMENT FOR ADVANCED SYSTOLIC HEART FAILURE IN BLACK AFRICANS
J. Byrne, J. DeCourcey, H. Williams, A. Ajembe, R. Buckley, M. Kearney.King’s College Hospital, London, UK
Introduction: Several previous studies have suggested that Black patients with chronic heart failure (CHF) secondary to left ventricular (LV) systolic dysfunction have a poorer prognosis than White European patients, and a blunted response to treatment. Our objective was to determine racial differences in aetiology, outcome and response to treatment in Black Africans attending a multi-disciplinary CHF clinic.
Methods: All patients presenting to the CHF service were included in the analysis; data were collected prospectively. All patients had confirmed LV systolic dysfunction. Patients received standard CHF therapy with nurse and pharmacist led follow-up and optimisation of medical therapy. Mortality data were obtained from local records. Statistical analysis was performed using the Student’s t test for continuous variables and the chi-square or Fisher’s exact test for nominal variables. Data are presented as mean (SD); p<0.05 considered significant.
Results: 341 patients were included in the analysis, 76 were Black African and 265 were White European. 57% of Black African and 50% of White European had been hospitalised at the time of referral. Baseline echocardiographic dimensions were similar in both groups (LV end diastolic dimensions: Black African 6.5 (1.3) v White European 6.4 (1.1) cm. LV end systolic dimensions: Black African 5.4 (1.2) v 5.3 (1.2) cm. Fractional shortening: Black African 17.4 (11) v White European 17.4 (9) %; p = NS for all parameters). Mean follow-up was similar (Black African 15 (8) v White European 13 (8) months; p = NS). Demographics and outcome are presented in the table. Black African patients with CHF were younger and a higher proportion were female. Blood pressures were similar between both groups at baseline (Black african 125 (27) v White European 114 (21) mm Hg) and at follow-up, renal function was also similar in both groups at baseline and follow-up (baseline creatinine: Black African 123.6 (69) v White European 138.6 (16) mmol/l; p = NS. Follow-up: Black African 114 (14) v White European 119 (51) mmol/l; p = NS). A high proportion of patients were established on both ACE inhibitor treatment and beta-blockers at the time of follow up (ACEI: Black African 89.5 v White European 94.7%) (Beta-blockade: Black African 94.7 v White 90.2%). Levels of treatment for both agents improved throughout the period of the study in both groups. A mean reduction in NYHA class was seen in both groups during follow-up although no difference was seen in total mortality.
Conclusion: This is the first study to demonstrate that with contemporary treatment, response to treatment and outcome are similar in Black African and White European patients with advanced CHF. This study suggests that an improvement in functional class coupled with a low mortality can be achieved in both Black African and White European patients with modern heart failure therapy and intensive follow-up in a dedicated heart failure clinic.
Abstract 305
congestive heart failure; afrocaribbean; mortality
306 TOLERABILITY OF CHARM-ADDED CANDESARTAN IN REAL-LIFE PATIENTS WITH ADVANCED CHRONIC HEART FAILURE
M. MacDonald1, N. Hawkins2, M. Shaw1, J. McMurray3, H. Dargie3, M. Petrie1.1Glasgow Royal Infirmary, Glasgow, UK; 2Stobhill Hospital, Glasgow, UK; 3Western Infirmary, Glasgow, UK
Introduction: The CHARM-added trial demonstrated that the addition of candesartan to standard therapy with angiotensin converting enzyme inhibitors (ACE-inhibitors) and beta-blockers resulted in a significant reduction in cardiovascular deaths and hospital admissions for chronic heart failure (CHF) patients with a low ejection fraction. Many clinicians have not adopted the addition of candesartan as standard therapy. There is concern that in real-life practice, there may be an increase in adverse events. We examined the tolerability of candesartan in addition to ACE-inhibitors and beta-blockers in an advanced heart failure population.
Methods: We retrospectively examined consecutive case notes of patients currently attending the Scottish National Advanced Heart Failure Service, a quartenary referral centre. Follow-up is through the service, the local heart failure liaison nurse services, general practitioners and referring hospitals.
Results: 107 patients (mean age 53) were included. Mean ejection fraction was 17.6. Mean creatinine was 120. 22% were on spironolactone. 12 patients were ACE-inhibitor intolerant of whom 8 were on an angiotensin II receptor blocker alone. 57 were not established on optimal doses of beta blockers or ACE inhibitors and were not yet challenged with candesartan. 38 patients were initiated on candesartan in addition to maximum tolerated doses of ACE-inhibitors and beta-blockers. Of these 13 (34%) had reached a maximum tolerated dose of candesartan; 13 (34%) were undergoing candesartan titration; 12 (32%) were intolerant of candesartan. Of the 13 on a maximum tolerated dose, the mean dose achieved was 24 mg. Eight patients were established on the top dose of 32 mg. Of the remaining five patients, titration was limited by the following: two had symptomatic hypotension; one had worsening renal function; one developed hyperkalaemia; one felt non-specifically unwell.
Of the 12 patients intolerant to candesartan, the reasons for discontinuation were: seven developed symptomatic hypotension; two developed hyperkalaemia; two felt non-specifically unwell; one had asymptomatic severe hypotension. No patient was discontinued for worsening renal function. Those on a maximal tolerated dose of candesartan had a mean reduction in BP of 8/5, whereas those who were intolerant to candesartan had a mean reduction in BP of 13/14.
Conclusion: In a population of young patients with advanced heart failure, a third were titrated to maximum tolerated doses of candesartan over and above established therapies and a third were undergoing titration. One third were intolerant primarily due to symptomatic postural hypotension. The addition of candesartan to established therapy in this population is achievable and safe with appropriate monitoring.
heart failure; candesartan; left ventricular dysfunction
307 PROGRESSIVE HEART FAILURE, RATHER THAN SUDDEN DEATH, ACCOUNTS FOR MOST EARLY DEATHS IN PATIENTS WITH NEWLY DIAGNOSED HEART FAILURE
P. Mehta1, S. Dubrey2, H. McIntyre3, D. Walker3, S. Hardman4, G. Sutton1, T. McDonagh1, M. Cowie1.1Imperial College, London, UK; 2The Hillingdon Hospital, London, UK; 3The Conquest Hospital, East Sussex, UK; 4The Whittington Hospital, London, UK
Background: Mortality remains high in patients with heart failure, particularly in the early period after a new diagnosis, with up to 25% not surviving six months. Clinical trials evaluating the mode of death in chronic heart failure demonstrate that approximately 50% of patients die suddenly. The mode of death for newly diagnosed heart failure in the general population has not been evaluated.
Aims: To describe the mode of death in patients during the first six months after a new diagnosis of heart failure.
Design: Two centre, population-based observational study.
Setting: The Hillingdon Hospital, London and The Conquest Hospital, East Sussex.
Methods: New cases of heart failure were identified by daily surveillance of acute hospital admissions and general practitioner referral. A diagnosis of heart failure was made based on the European Society of Cardiology criteria. A panel of three cardiologists reviewed all deaths occurring within six months and assigned a mode of death, according to pre-specified criteria.
Results: Between January 2004 and September 2005, 379 patients with incident heart failure were identified. Median age was 75.3 (SD 12.6) years. Based on drug data available for 357 patients (94%), 81% tolerated an ACE inhibitor or angiotensin receptor blocker, 33% a β-blocker and 29% both, prior to initial discharge or death. Four (1%) patients underwent successful ICD implantation. To date, there have been 68 deaths over a median follow-up of 6.6 months; 91% (n = 62) were cardiovascular deaths. Of the cardiovascular deaths, 10% (n = 6) occurred within 14 days of an acute myocardial infarction. The mode of death was progressive heart failure (PHF) in 69% (n = 43), sudden death in 18% (n = 11) and other cardiovascular modes of death in 13% (n = 8). Based on detailed clinical data available for 41 cardiovascular deaths, sudden death (v other modes) was associated with greater left ventricular dilatation at baseline: mean left ventricular end diastolic diameter (6.2 (0.7) v 5.5 (0.7) cm; p = 0.04) and left ventricular end systolic diameter (5.3 (1.0) v 4.3 (0.9) cm; p = 0.035). Dying suddenly (v other modes) was not related to age, gender, NYHA class, aetiology of heart failure, cardiac rhythm, or QRS duration.
Conclusions: Over two-thirds of cardiovascular deaths are related to progressive heart failure in the first six months after a new diagnosis of heart failure in the general population. Sudden death accounts for less than one-fifth of cardiovascular deaths and is associated with greater left ventricular dilatation at baseline. These data further support the early use of therapies known to delay progression of heart failure, such as ACE inhibitors and β-blockers. However, identification of those at risk of early sudden death for specific therapy such as ICD implantation is not straightforward.
heart failure; mode of death; sudden death
308 EMERGING EVIDENCE FOR IMPROVED SURVIVAL FOR PATIENTS WITH NEWLY DIAGNOSED HEART FAILURE IN THE UK
P. Mehta1, S. Dubrey2, H. McIntyre3, D. Walker3, S. Hardman4, G. Sutton1, T. McDonagh1, M. Cowie1.1Imperial College, London, UK; 2The Hillingdon Hospital, London, UK; 3The Conquest Hospital, East Sussex, UK; 4The Whittington Hospital, London, UK
Background: Heart failure remains a major public health problem with approximately 60 000 incident (new) cases each year in the UK. In the mid-1990s, two London-population-based (Hillingdon and Bromley) studies demonstrated a poor prognosis for patients with incident heart failure, particularly in the early period after diagnosis. In the combined cohort, mortality was 16% at one month, 22% at three and 25% at six months. Population-based studies in the US suggest survival may have improved in the past decade, but data from comparable studies in the UK are lacking.
Aims: To describe the survival of a population-based cohort of patients in the first six months after a new diagnosis of heart failure.
Design: Two-centre, population-based observational study.
Setting: Combined population of 400 000 served by two district general hospitals (The Hillingdon Hospital, London and The Conquest Hospital, East Sussex).
Methods: Case ascertainment was as in the London studies—new cases of heart failure were identified by daily surveillance of acute hospital admissions and general practitioner referral. Patients with suspected heart failure underwent clinical assessment, chest radiography, electrocardiography and echocardiography. A diagnosis of heart failure was made based on the European Society of Cardiology criteria. Patients were flagged at the Office of National Statistics for mortality.
Outcome Measures: All-cause and cardiovascular mortality.
Results: Between January 2004 and September 2005, 379 patients (61% males, 81% in-patients) with incident heart failure were identified. Median age was 75.3 (SD 12.6) years. At the time of presentation, 33% of patients were in NYHA class III and 56% in NYHA class IV. Based on drug data available for 357 patients (94%), 81% tolerated an ACE inhibitor or angiotensin receptor blocker, 33% a β-blocker and 29% both, prior to initial discharge or death. Four (1%) patients underwent successful ICD implantation. To date, there have been 68 deaths over a median follow up of 6.6 months; 91% (n = 62) were cardiovascular deaths. All cause mortality rates were 9% (95% CI 6–12%) at 1 month, 15% (11–18%) at 3 months and 18% (14–22%) at 6 months. Mortality rates were lower at each time-point, when compared to the London studies (p<0.05). On multivariable analysis, older age, lower serum sodium and higher serum urea were independently associated with the risk of cardiovascular death, but gender, aetiology of heart failure and left ventricular function were not.
Conclusions: This study demonstrates that the mortality among patients with a new diagnosis of heart failure in the UK remains unacceptably high. However, when compared with the earlier London studies of incident heart failure, which used similar methodology in comparable populations, our data suggest mortality has improved over the past decade.
survival; prognosis; heart failure