Article Text

Abstract
Background: Reduction of radiation burden of multidetector computed tomography coronary angiography (CTCA) has remained an important task.
Objective: To compare effective radiation dose of low-dose 64-slice CTCA using prospective ECG-triggering versus diagnostic invasive coronary angiography (CA).
Methods: 42 patients referred for elective invasive CA owing to suspected coronary artery disease (CAD) were prospectively enrolled to undergo a low-dose CTCA without calcium scoring within the same day before CA. Dose-area product of diagnostic invasive CA and dose-length product of CTCA were measured, converted into effective radiation dose and compared using Mann-Whitney U tests. In addition, accuracy of CTCA to detect CAD (coronary artery narrowing ⩾50%) was assessed using invasive CA as standard of reference. On an intention-to-diagnose basis all non-evaluative vessels were included in the analysis and censored as positive.
Results: The estimated mean effective radiation dose was 8.5 (4.4) mSv (range 1.4–20.5 mSv) for diagnostic invasive CA, and 2.1 (0.7) mSv (range 1.0–3.3 mSv) for CTCA (p<0.001). 19 patients (42.9%) had no CAD by invasive CA. 40 (95.2%) patients have been correctly classified as having CAD (23/23) or no CAD (17/19). Over 97% (551/567) of segments were evaluable. Vessel-based analysis revealed sensitivity, specificity, positive and negative predictive value of 94.2% (CI 0.8% to 1.0%), 94.8% (CI 09% to 1.0%), 89.0% (CI 0.8% to 1.0%), 97.4% (CI 09% to 1.0%) and an accuracy of 94.6%.
Conclusions: Low dose CTCA allows evaluation of CAD with high accuracy, but delivers a significantly less effective radiation dose to patients compared to diagnostic invasive CA.
Statistics from Altmetric.com
Since the implementation of 64-slice computed tomography (CT) scanners, CT coronary angiography (CTCA) has developed as a non-invasive tool with high accuracy for the evaluation of coronary artery disease (CAD).1 However, effective radiation dose (E) to patients and its risk of cancer induction have remained issues of concern, although only few quantitative data on the dose-risk relation are available.2 The latter is mainly based on epidemiological studies from atomic bomb survivors from the Hiroshima and Nagasaki tumour registries, studies of people exposed for medical reasons and studies of nuclear workers.3 The risk of cancer from exposure to low levels of ionising radiation, defined as effective dose below 1 mSv and up to 100 mSv, may proceed in a linear fashion to increasing radiation dose without a lower threshold. Thus, small radiation doses to patients may cause a small increase in risk.3 The American Heart Association states that a CT with an effective radiation dose of about 10 mSv may be associated with an increase in the possibility of fatal cancer.4 Brenner et al estimated a lifetime cancer mortality risk of 0.08% attributable to a full-body CT scan with an effective radiation dose of 12 mSv in a 45-year-old male adult.5 Although this may appear justifiable under certain clinical circumstances the risk may be higher in younger patients and female patients. Therefore, any successful reduction of radiation dose is important. By using ECG-modulation the radiation burden of CTCA could be reduced from initially over 20 mSv6 to 10–15 mSv,7 and with optimised protocols below 8 mSv.8 A milestone in the reduction of E could be achieved by a new scanning protocol using prospective ECG-triggering where radiation is administered at only one predefined end-diastolic time point instead of during a whole phase of the cardiac cycle.9 First reports demonstrated the feasibility10 11 and latest results confirm maintained high diagnostic accuracy12 13 of this new technique.
Although the United Nations Scientific Committee on the Effects of Atomic Radiation cites a typical value of about 7 mSv for E from invasive CA,14 no data on direct head-to-head comparison in the same patient between E from CTCA and CA are available.
The aim of the present study was to assess E of diagnostic invasive CA and low dose CTCA using prospective ECG-triggering in the same patient.
Patients and methods
Study population
Among 74 consecutively screened patients with no known CAD, nine refused to give consent and could not be included. Of the 65 enrolled patients 14 were deemed ineligible due to renal insufficiency (creatinine levels >150 μmol/l, or >1.7 mg/dl) (n = 8); allergy to iodinated contrast agent (n = 3), non-sinus rhythm or known premature ventricular or supraventricular beats (n = 12). The final study population consisted of 42 prospectively enrolled patients, different from patients included in previously reported studies on the feasibility11 and accuracy12 of low dose CTCA with prospective ECG-triggering. The pre-test probability for CAD was estimated using the Duke clinical score, which includes the type of chest discomfort, age, gender and traditional risk factors.15 All patients were referred for elective invasive CA because of suspected CAD with the following symptoms: dyspnoea (n = 9), typical angina pectoris (n = 7), atypical chest pain (n = 19) and pathological exercise test or ECG (n = 14). CTCA and invasive CA were successfully performed in all 42 patients (29 male, 13 female; age 62 (8.4) years, range 42–82 years) on the same day. Thirteen patients were on β-blocker therapy as part of their baseline medication. Additional intravenous metoprolol (2–20 mg) (Beloc, AstraZeneca, London, UK) was administered for heart rate control before CTCA in 22 patients (mean 5.7 (6.6) mg) yielding a mean heart rate of 55.4 (6.2) bpm (range 36–70 bpm) and a mean heart rate variability of 1.6 (1.7) bpm (range 0.3–9.7 bpm). The mean body mass index (BMI) was 26.9 (4.4) kg/m2 (range 18.6–44.8 kg/m2). The study protocol was approved by the local ethics committee and written informed consent was obtained.
Data acquisition and post-processing
All patients received a single dose of 2.5 mg isosorbide dinitrate sublingually (Isoket, Schwarz Pharma, Monheim, Germany) 2 minutes before the scan. In addition, intravenous metoprolol was administered, if necessary to achieve a target heart below 65 bpm before the start of the scan. Heart rate was monitored and heart rate variability was assessed as the standard deviation of the heart rate throughout the scan as previously reported.16 For CTCA, 80 ml of iodixanol (Visipaque 320, 320 mg/ml, GE Heathcare, Bucks, UK) at a flow rate of 5 ml/s followed by 50 ml saline solution was injected into an antecubital vein via an 18-gauge catheter. Bolus tracking was performed with a region of interest placed into the ascending aorta, and image acquisition was started 4 seconds after the signal density reached a threshold of approximately 120 Hounsfield units. All CTCA examinations were performed with a LightSpeed VCT XT scanner (GE Healthcare) and prospective ECG-triggering9 using a commercially available protocol (SnapShot Pulse, GE Healthcare) and the following scanning parameters as previously reported11: slice acquisition acquisition 64 mm × 0.625 mm, smallest x-ray window (only 75% of the RR-cycle, setting the padding to 0 ms), z-coverage 40 mm with an increment of 35 mm, gantry rotation time 350 ms, BMI adapted tube voltage (100 kV: BMI <25 kg/m2, 120 kV: BMI ⩾25 kg/m2) and effective tube-current (450 mA: BMI <22.5 kg/m2, 500 mA: BMI 22.5–24.9 kg/m2, 550 mA: BMI 25.0–27.4 kg/m2, 600 mA: BMI 27.5–30 kg/m2, 650 mA: BMI >30 kg/m2). The CT scan was performed from below the tracheal bifurcation to the diaphragm, choosing three to four scan blocks (field of view 11–14.5 cm). By restricting the scan to the smallest possible window at only one distinct end-diastolic phase of the RR-cycle (that is, 75%) we ascertained the lowest achievable effective dose delivery. CTCA images were reconstructed with a slice thickness of 0.6 mm, using a medium-soft tissue convolution kernel (standard). In case of vessel wall calcifications, additional images were reconstructed using a sharp-tissue convolution kernel (detail) and preferably analysed using a bone window setting (window width: 1500 HU; window level: 500 HU) to compensate for blooming artefacts. All images were transferred to an external workstation (AW 4.4, GE Healthcare).
CT image analysis
Coronary arteries were segmented as suggested by the American Heart Association.17 The right coronary artery (RCA) was defined to include segments 1–4, the left main artery (LMA) to include segment 5, the left anterior descending artery (LAD) to include segments 6–10, and the left circumflex artery (CX) to include segments 11–16; the intermediate artery was designated as segment 16, if present. All segments with a diameter of at least 1.5 mm at their origin were included. Step artefacts at junctions of different image blocks may not necessarily lead to misinterpretations. However, as a hidden lesion within the artefact cannot be excluded with absolute certainty we have categorised any step artefact as non-evaluative. On an intention-to-diagnose basis all non-evaluative segments classified the whole vessel as not evaluative which was censored as positive and included in the final analysis. Two readers experienced in cardiac radiology assessed all coronary vessels for the presence of haemodynamically significant stenoses, defined as narrowing of the coronary luminal diameter ⩾50%. In case of multiple lesions in one segment, the segment was classified by the worst lesion. For any disagreement in data analysis between the two observers, consensus agreement was achieved.
Invasive coronary angiography
Invasive CA through the femoral artery was performed on an Allura 9 and an Allura XPER FD10/10 (Philips Medical Systems) catheterisation equipment in an experienced catheterisation laboratory of a teaching hospital (University Hospital Zurich) following a protocol, which consists of a biplane angiography of the left coronary artery with two radiation exposures in four orientations and of the right coronary artery with two exposures in two orientations, as is routinely performed in our cardiology department. With one tube, the left coronary artery was imaged in the following orientations: posteroanterior, 30° right anterior oblique with 20° caudal angulation, and 15° right anterior oblique with 30° cranial angulation. With the other tube, the left coronary artery was imaged in the following orientations: 90° left anterior oblique, 40° left anterior oblique with 20° cranial angulation, and 50° left anterior oblique with 60° caudal angulation. Angiography of the right coronary artery was performed in the following orientations: 30° right anterior oblique and 15° left anterior oblique with 15° cranial angulation with one tube, and 60° left anterior oblique and 90° left anterior oblique with the other tube.
Additional views could be performed at the operator’s discretion if necessary. In cases where a left ventricular angiogram was performed this part of radiation exposure was excluded. An experienced observer blinded to the results from CTCA evaluated the angiograms. Coronary arteries were included in the analysis if the luminal diameter was at least 1.5 mm, excluding those vessels distal to complete occlusions. Each vessel was visually scored as being normal or significantly stenosed (defined as a diameter reduction of ⩾50%) reflecting daily clinical routine in our catheterisation laboratory.
Effective radiation dose estimation (E)
Values for E were estimated for CTCA as a product of the dose-length product (DLP) × a conversion coefficient for the chest (k = 0.017 mSv/mGy × cm) as adapted by the European Commission in the European guidelines on quality criteria for computed tomography.18 Similarly, E was estimated as a product of the dose-area product (DAP) of the diagnostic coronary scenes × a conversion factor for chest (k = 0.22 mSv/mGy × cm2) for invasive CA based on the National Radiological Protection Board tables.19
Statistical analysis
Quantitative variables were expressed as mean (SD) and categorical variables or percentages. Man-Whitney U tests were performed for comparison of effective radiation dose between CTCA and invasive CA in all patients and different BMI subgroups by using SPSS software. A p value of <0.0083 was considered as significant using the Bonferroni-adjustment for multiple testing. Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated from χ2 tests of contingency. The 95% confidence intervals (CI) and the positive and negative likelihood ratios (LR) were calculated.
Results
Effective radiation doses (E)
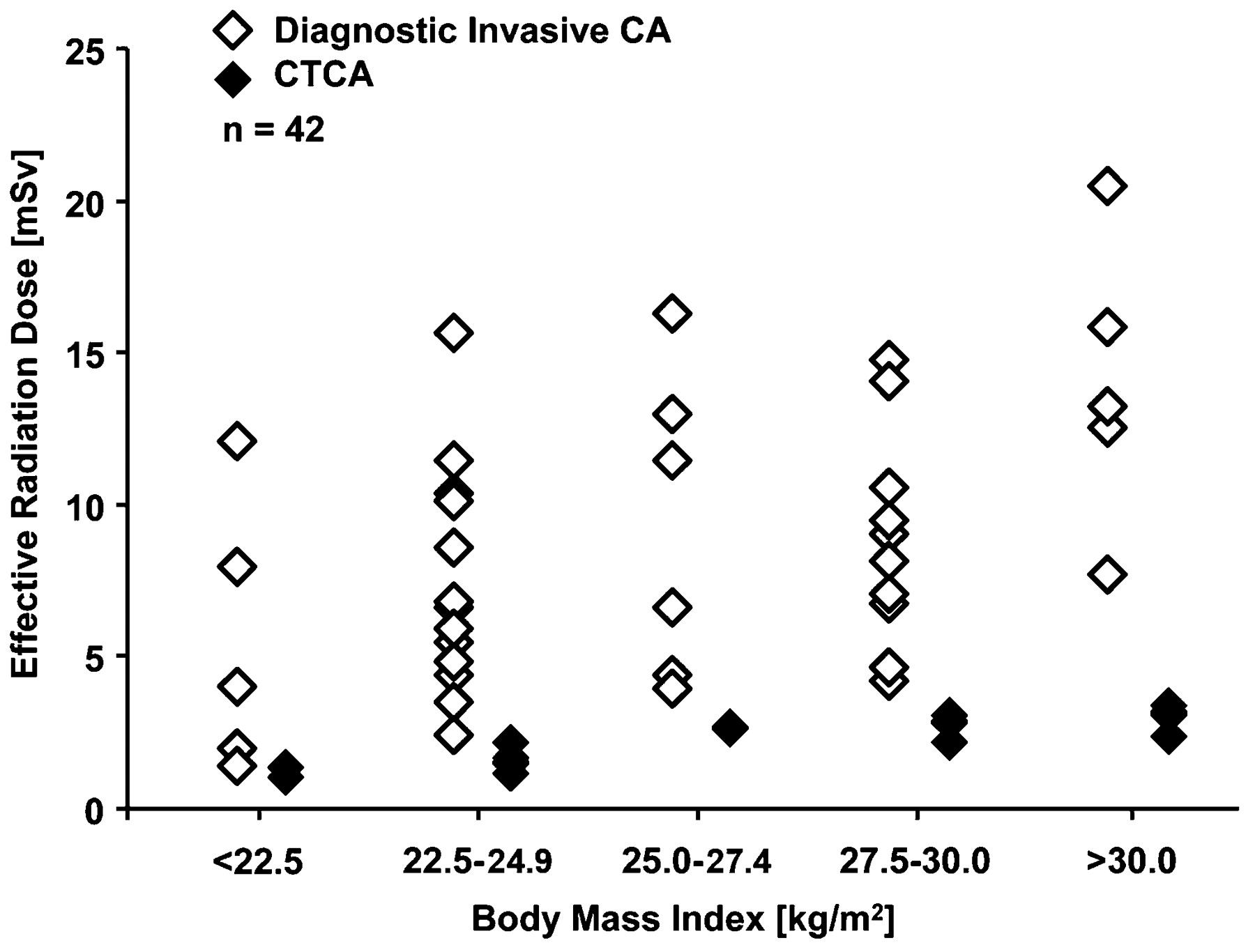
For CTCA the mean DLP was 122.4 (42.1) mGy cm, resulting in a mean E of 2.1 (0.7) mSv. The variations of E between all patients (DLP: 58.5–193.2 mGy cm, E: 1.0–3.3 mSV) and within different BMI subgroups were small (fig 1).

Effective radiation doses for each patient from the two different methods—that is, diagnostic invasive coronary angiography (CA) and CT coronary angiography (CTCA).
For diagnostic invasive CA the DAP was 38.7 (4.4) mGy cm2, resulting in a mean E of 8.5 (4.4) mSv. The doses varied widely between all patients (DAP: 6.4–93.0 mGy cm2; E: 1.4–20.5 mSv) and within different BMI subgroups (fig 1). There was no significant difference in E of invasive CA between patients with stenoses (mean 9.4 (4.4) mSv; range 1.4–20.5 mSv) and those with no CAD (mean 7.5 (4.3) mSv, range 2.0–14.7 mSv).
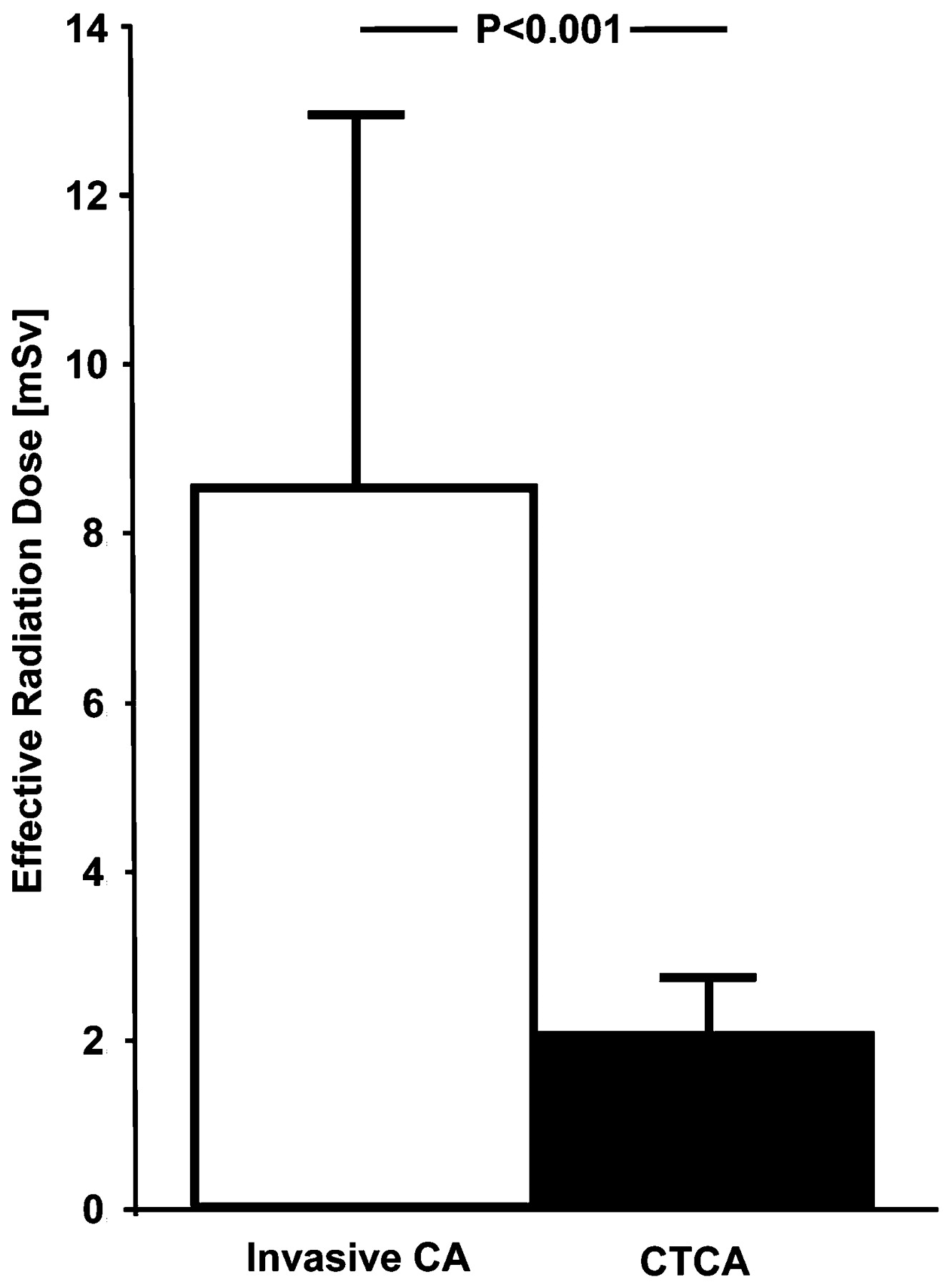
Mean E was significantly higher in invasive CA versus CTCA in all analysed patients (p<0.001) (fig 2). The mean DLP, DAP and E for all patients and different BMI subgroups as well as their differences are given in table 1.

Comparison of mean effective radiation dose (SD) of diagnostic invasive coronary angiography (CA) and CT coronary angiography (CTCA).
Effective radiation dose: CTCA versus invasive CA
Image quality with CTCA
Of 672 theoretically possible segments in 42 patients with 16 coronary segments, 64 were missing because of anatomical variants, 33 had a diameter of less than 1.5 mm at their origin (by both methods) and eight segments have been occluded. Thus, 64 segments were missing for reasons not associated with the methodology as these segments simply did not exist. The remaining 33 segments were categorised as lower than 1.5 mm and thus not evaluable by the gold standard invasive CA. Thus, the missing data do not seem to introduce a selection bias.
Image quality of 551/567 segments (97.18%) was diagnostic. Thus, 16 segments (2.82%) were non-diagnostic and were considered as positive.
Diagnostic accuracy and impact of CTCA on pretest probability
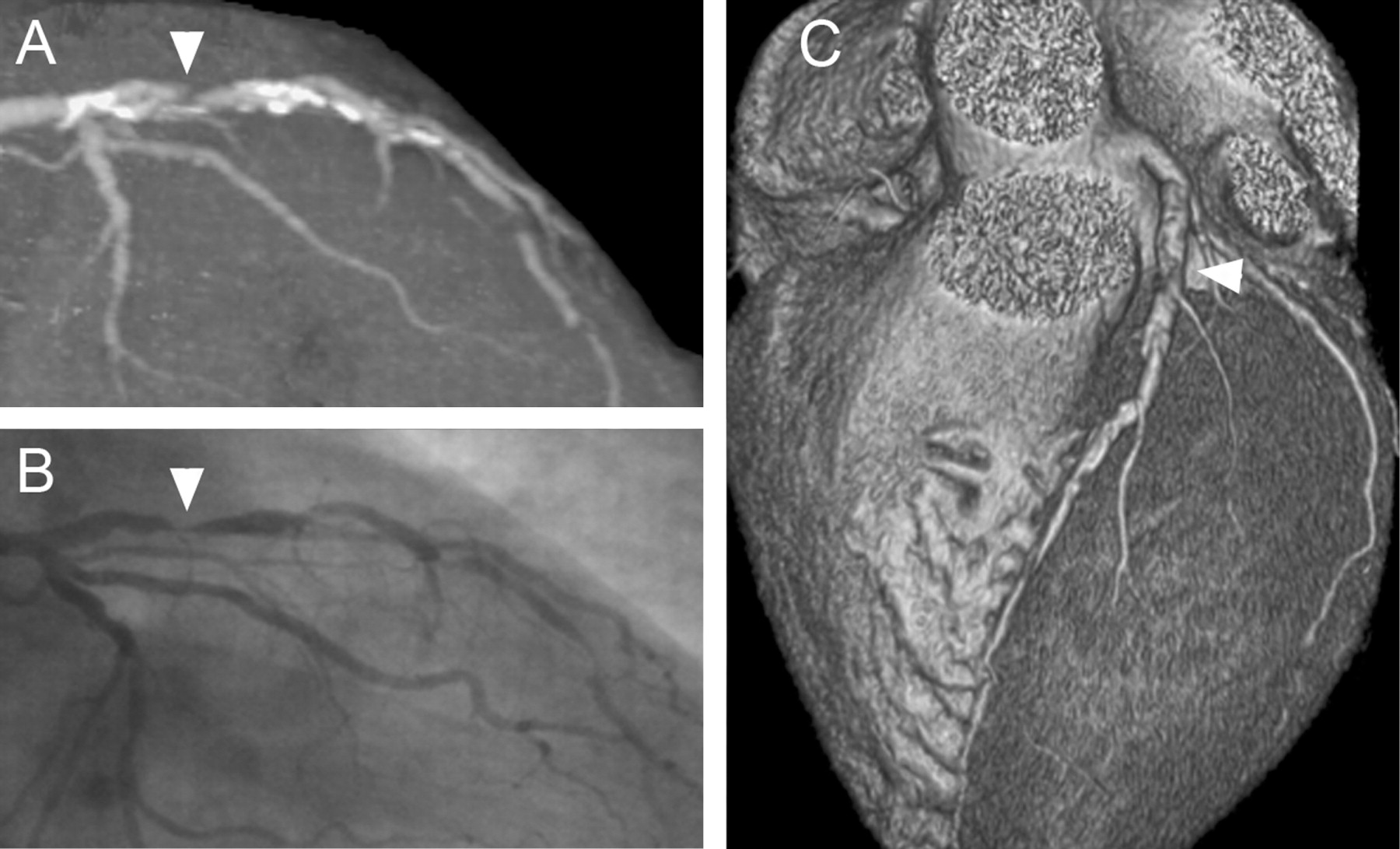
In 23 (54.8%) patients and 52 (31.0%) vessels, 80 coronary artery stenoses were recognised with invasive CA. Nineteen patients (42.9%) had no CAD by invasive CA. Forty (95.2%) patients have been correctly classified as having CAD (23/23) (example: fig 3) or no CAD (17/19) (example: fig 4).

Multiple calcified an uncalcified coronary lesions of an left descending artery are visualised on an angiographic view by CT coronary angiography (A) and on an invasive coronary angiography image with matching angulations (B). The arrowhead indicates the most severe lesion in (A) and (B) as well as on the three-dimensional volume rendered image (C). The mean effective radiation dose was 2.1 mSv for CT and 7.3 mSv for invasive coronary angiography.

Left descending artery without coronary lesions is visualised on an angiographic view by CT coronary angiography (A), on an invasive coronary angiography image with matching angulations (B) and on the three-dimensional volume rendered image (C). The mean effective radiation dose was 1.1 mSv for CT and 5.9 mSv for invasive coronary angiography.
On a per-vessel analysis, there was 94.2% (49/52; CI 0.8% to 1.0%) sensitivity, 94.8% (110/116; 95% CI 0.9% to 1.0%) specificity, 89.0% (49/55; 95% CI 0.8% to 1.0%) positive predictive value (PPV) and 97.4% (110/113; CI 0.9% to 1.0%) negative predictive value (NPV), yielding an accuracy of 94.6% (CI 09% to 1.0%) (table 2).
Diagnostic accuracy and predictive value for CTCA
On a per-patient analysis, there was 100% (23/23; CI 0.9% to –1.0%) sensitivity, 89.5% (23/25; CI 0.7% to 1.0%) specificity, 92.0% (18/20, 95% CI 0.7% to 1.0%) PPV and 100% (17/17; CI 0.8% to 1.0%) NPV, yielding an accuracy of 95.2% (CI 0.8% to 1.0%) (table 2). The estimated pretest and post-test probabilities for significant CAD after CTCA scans are given in figure 5.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Impact of CT coronary angiography (CTCA) on pretest probabilities of significant coronary artery disease (CAD). 1Calculated using the Duke clinical score. 2Calculated using Bayesian statistics (post-test odds = pretest odds × likelihood ratio).
Discussion
While the gold standard for the detection of coronary lesions remains invasive CA, its associated costs,20 morbidity and mortality have driven the search for non-invasive alternatives like CTCA.
However, the radiation burden to patients has remained a concern and has led to hesitation to use non-invasive cardiac imaging with CT, although the introduction of tube modulation and optimised scanning parameters has allowed us to decrease E of CTCA from over 20 mSv to below 10 mSv and may explain the large variability between different centres.8 New scanner technologies such as dual-source,21 as well as latest scanner generations with 25622 and more slices23 may allow the reduction of motions artefacts; the issue of radiation burden is not solved by these technical advances alone. In fact, in a preliminary study using 256-slice radiation administered to the patient has been reported to be as high as 33 mSv.22
As the strength of CTCA lies in its ability to exclude CAD (that is, its high NPV) the general perception is to use this technique mainly in low-to-intermediate probability populations.1 The latter however will not only have a low prevalence of CAD but inherently also bear a low risk of cardiovascular events, which makes it unlikely that any diagnostic procedure or therapeutic intervention would further improve the outcome. This may explain why it seems to be a particular challenge for CTCA to keep a positive balance of harms and benefits. It is in this context that the recently introduced scanning protocol using prospective ECG-triggering—where scanning is limited to a narrow predefined end-diastolic phase resulting in a massive reduction in radiation exposure11 12—was well received, as documented by a growing body of literature.13 24 25 26 27 28 29 30 31 32 The present paper is the first to report on the head-to-head comparison of E from invasive CA versus CTCA with prospective ECG-triggering in the same patients. Our results not only confirm the feasibility and reliability (accuracy versus invasive CA) of this low-dose CTCA protocol but also show that E is significantly lower by about 75% than in CA. This holds true for each patient and is independent of the BMI and was not subject to a large inter-individual variability. By contrast, E values from CA showed a large variability, in line with previous reports relating this variability to variances in procedure complexity, operator experiences or laboratory equipment.33 In fact, in patients with complex coronary anatomy such as diffuse wall alterations and multiple lesions with intermediate severity or those with bypass grafts E from CA may increase considerably owing to the need for longer irradiation time, while the latter would not be affected using CTCA. Although in the present study we have excluded patients with known CAD, thus eliminating patients with bypass grafts and reducing the probability of complex CAD, we still found a significantly higher E from CA with a substantial inter-individual variance as opposed to CTCA. This strengthens our data and indicates that the findings may remain valid even if extrapolated to various patient populations with different CAD probabilities.
As the same field of view was used in virtually all patients the E from CTCA is mainly determined by the patient’s physique because we used a BMI-adapted protocol for tube voltage and current. However, even after stratifying patients for BMI the variability of E from CTCA was negligible while it remained high for CA.
Such a massive reduction in E achieved by using prospective ECG-triggering of CTCA may have a profound impact on the perception of the optimal patient population benefiting most from non-invasive CTCA. It is an accepted rule that for reasons of radiation protection the total dose applied to a given population should be kept as low as reasonably achievable (ALARA). This dramatically shifts the benefit-to-harm balance supporting the hypothesis that low-dose CTCA may serve as a gatekeeper to CA in patient populations with CAD prevalence anywhere below 75%. Outcome trials are needed to establish whether such a strategy may improve outcome. Theoretically, for each saved CA due to a normal CTCA (saved dose 6 mSv) we can afford three patients with CTCA plus CA (added dose of 2 mSv compared to CA alone). The use of CTCA as gate keeper breaks even with regard to radiation exposure of the patient population with a prevalence of 75%. The fact that the accuracy of CTCA does not reach 100% may negatively affect this balance. On the other hand preventing an unnecessary CA may confer more benefits than just reducing total radiation exposure as even elective purely diagnostic CA are associated with a low but not negligible morbidity and mortality. In addition, findings of coronary luminal narrowing often trigger coronary interventions that are associated with an even higher mortality despite no proved outcome benefits in chronic stable CAD patients.34 The values of E clearly favour CTCA over CA, although the conversion factor for estimating E from DLP in CA may be affected by a 10–20% uncertainty.33 However, even with a conversion factor lower than the one used in our study the values remain significantly lower for CTCA. The advantage of prospective ECG-triggering as a new CTCA protocol to reduce E lies in its universal applicability. In fact, this is not limited to the 64-slice CT scanners but can be implemented into the latest (dual-source) and future scanner generations such as those with 320 slices allowing full coverage of the heart in one rotation. The following technical limitations of CTCA have to be considered. Image quality is affected by coronary calcification, motion artefacts and body mass index.35 Furthermore, sinus rhythm and heart rate control are mandatory for prospective ECG-triggering,36 explaining the frequent β-blocker administration in this study. In addition, as the acquisition is limited to one phase the use of prospective ECG-triggering does not allow functional assessment of the left ventricle. Of note a substantial fraction of consenting patients had to be excluded for medical reasons. These contraindications, however, such as renal dysfunction or iodine allergy apply equally to spiral scanning and, therefore, do not represent specific limitations of prospective ECG-triggered CTCA. Moreover, in contrast to some other centres we do not routinely add unenhanced CT for calcium scoring to our CTCA, because there is no evidence supporting the idea that the additional radiation dose from calcium score is justified by an improvement in the accuracy of CTCA.1 Thus, we did not perform a calcium score scan in this study which contributed to the low radiation dose of the CTCA.
Although the relatively small population in this study may limit the power of the accuracy analysis for CTCA vs invasive CA this was not the primary goal of the study, which aimed at comparing the effective radiation dose of both techniques.
Conclusions
Low-dose CTCA allows evaluation of CAD with high accuracy, but a significantly less effective radiation dose to patients compared to diagnostic invasive CA.
REFERENCES
Footnotes
Funding The study was supported by a grant from the Swiss National Science Foundation (SNSF-professorship grant No PP00A-114706) and by the ZIHP (Zurich Center for Integrative Human Physiology, University of Zurich, Switzerland).
Competing interests None.
Provenance and Peer review Not commissioned; externally peer reviewed.
Ethics approval The study is approved by the local research ethics committees.