Article Text

Abstract
Background Idiopathic recurrent acute pericarditis (IRAP) is a rare disease of suspected, yet unproved, immune-mediated origin. The finding of serum heart-specific autoantibodies in IRAP would strengthen the autoimmune hypothesis and provide aetiology-specific non-invasive biomarkers.
Objective To assess frequency of serum anti-heart (AHA), anti-intercalated-disk (AIDA) and non-cardiac-specific autoantibodies and their clinical and instrumental correlates in patients with IRAP.
Patients 40 consecutive patients with IRAP, 25 male, aged 37±16 years, representing a large single-centre cohort collected at a referral centre over a long time period (median 5 years, range 1–22 years). Control groups included patients with non-inflammatory cardiac disease (NICD) (n=160), ischaemic heart failure (n=141) and normal subjects (n=270).
Methods AHA (organ-specific, cross-reactive 1 and 2 types) and AIDA were detected in serum samples from patients, at last follow-up, and control subjects by indirect immunofluorescence (IIF) on human myocardium and skeletal muscle. Non-cardiac-specific autoantibodies were detected by IIF, and anti-Ro/SSA, anti-La/SSB by ELISA.
Results The frequencies of cross-reactive 1 AHA and of AIDA were higher (50%; 25%) in IRAP than in NICD (4%; 4%), ischaemic (1%; 2%) or normal subjects (3%; 0%) (p=0.0001). AHA and/or AIDA were found in 67.5% patients with IRAP. Of the non-cardiac-specific antibodies, only antinuclear autoantibodies at titre ≥1/160 were more common in IRAP (5%) versus normal (0.5%, p<0.04). AIDA in IRAP were associated with a higher number of recurrences (p=0.01) and hospitalisations (p=0.0001), high titre (1/80 or higher) AHA with a higher number of recurrences (p=0.02).
Conclusions The detection of AHA and of AIDA supports the involvement of autoimmunity in the majority of patients with IRAP.
- Pericarditis
- antibodies
- autoimmunity
- immunology
- myocarditis
Statistics from Altmetric.com
Introduction
Pericarditis may account for about 5% of presentations to emergency departments for non-ischaemic chest pain.1 Recurrences occur in up to 15–32% of patients.2–7 Recurrent acute pericarditis is generally idiopathic or post-cardiac injury, and is often a frustrating problem, for both patients and doctors.2–7 Idiopathic recurrent acute pericarditis (IRAP) is a disease of suspected, yet unproved, immune-mediated pathogenesis.8–11
Patients with autoimmune conditions have a high frequency of circulating autoantibodies to the diseased target organ as well as other unaffected tissues.12 Serum anti-heart (AHA) and anti-intercalated disk autoantibodies (AIDA) detected by indirect immunofluorescence (IIF) represent autoimmune markers in patients with biopsy-proven myocarditis, dilated cardiomyopathy and in their relatives.13–18 We assessed the frequency of AHA, AIDA and of other non-cardiac-specific autoantibodies in a consecutive Italian series of patients with IRAP, as potential autoimmune markers.
Patients and methods
Patients and inclusion criteria
Sixty-three consecutive patients with recurrent acute pericarditis who fulfilled the inclusion criteria were assessed. Patients were included if they presented with a first attack of acute pericarditis defined by all the following features: typical chest pain (with or without a pericardial friction rub), suggestive electrocardiographic (ECG) changes, pericardial effusion, normal creatine kinase-MB and increased C-reactive protein.10 19 The minimum criteria for diagnosis of recurrences were the combination of typical chest pain, increased C-reactive protein, ECG and/or echocardiographic alterations. C-reactive protein had to be elevated in all cases during an acute attack.10 19 Only two patients were lost to follow-up; 13 patients had a post-cardiac injury syndrome; in five patients, initially labelled as ‘idiopathic’, a diagnosis of rheumatoid arthritis in one case and of Sjögren syndrome in four patients was made. In 43 patients the pericarditis remained ‘idiopathic’ at the end of a very long follow-up (mean 8.3 years, range 2–43 years); serum at last follow-up was available in 40 of them for autoantibody testing; these 40 patients are included in this study (25 men, aged at onset 37±16, range 13–67 years).
We used a previously detailed multidrug treatment protocol: non-steroidal anti-inflammatory drugs at high dosages (indometacin 75–150 mg, or aspirin 1500–2400 mg, or ibuprofen 1200–1800 mg/day); a very slow tapering of the corticosteroid if a steroid had already been started; colchicine (0.5–1 mg/day) if tolerated; immunosuppressive agents in selected cases.10 19 20
AHA and AIDA testing by standard indirect immunofluorescence
Serum samples from patients with pericarditis, taken at the last follow-up evaluation, were tested for AHA and AIDA by IIF at 1/10 dilution on 4 μm thick unfixed fresh frozen cryostat sections of blood group O normal human atrium and skeletal muscle; AHA- and AIDA-positive sera were subsequently titrated to end point by double dilutions.13–17 Organ-specific and cross-reactive 1 AHA patterns were classified as described.13–17
Briefly, organ-specific AHA gave diffuse cytoplasmic staining of atrial myocytes, but were negative on skeletal muscle; cross-reactive 1 or partially organ-specific AHA gave a fine striational staining on atrium, but were negative or only weakly stained skeletal muscle; cross-reactive 2 AHA gave a broad striational pattern on longitudinal sections of heart and skeletal muscle.13–17 Absorption studies with relevant tissues had confirmed the organ-specificity and cross-reactivity of the AHA patterns.13
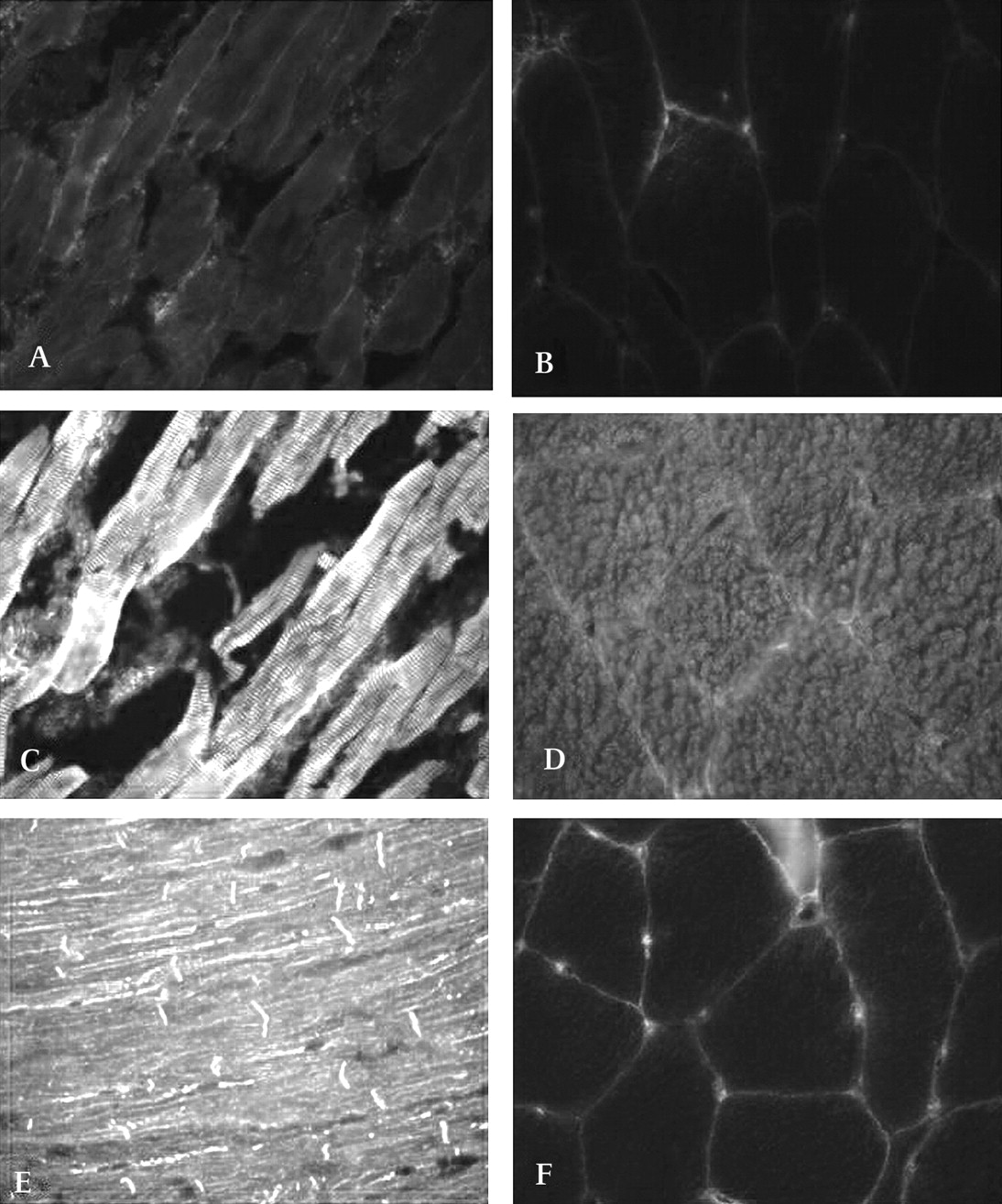
AIDA gave a linear staining of the intercalated disks between cardiac myocytes (figure 1). Two serum samples were used as standard positive and negative controls and titrated in every assay. All sera were read blindly against these standards using a fluorescence microscope (Zeiss Axioplan 2 imaging; Zeiss, New York, USA). An additional positive control serum was titrated to assess reproducibility. Endpoint titres for this serum were reproducible within one double dilution in all assays.14–17 The frequency of AHA and of AIDA in pericarditis was compared with that observed in our established control groups of subjects with non-inflammatory cardiac disease (n=160, 80 male, aged 37±17 years, of whom n=55 had rheumatic heart disease, n=67 hypertrophic cardiomyopathy, n=38 congenital defects), ischaemic heart disease (n=141, 131 male, aged 44±14 years) and normal subjects (n=270, 123 male, age 35±11).14–17 Forty-one of the 141 ischaemic patients, aged 47±12 years, 28 male; 31 in New York Heart Association (NYHA) III and 10 in NYHA IV, had had a myocardial infarct 6 months to 10 years (median 2 years) previously; ejection fraction ranged from 16% to 44% (mean 30±7).14–17
{kind=link}
Anti-heart autoantibody (AHA) immunofluorescence patterns. Blood group O normal human atrium (left panels) and skeletal muscle (right panels) stained with (A,B) AHA-negative serum from a normal subject. No myocyte or muscle staining is present. (C,D) Serum from a patient with idiopathic recurrent acute pericarditis (IRAP), containing cross-reactive (partially organ-specific) AHA. A fine striational fluorescence is visible on atrial tissue; skeletal muscle is weakly positive. (E,F) Serum from a patient with IRAP, containing both organ-specific AHA and anti-intercalated-disk autoantibodies (AIDA). Organ-specific AHA give a diffuse cytoplasmic indirect immunofluorescence technique staining on atrial myocytes, AIDA produce a linear staining of the intercalated disks between cardiac myocytes; skeletal muscle is negative. Magnification ×400.
Non-cardiac-specific autoantibody tests
Antinuclear antibodies were tested by IIF on HEp2 cells and anti-mitochondrial antibodies by IIF on rat liver and kidney. Other non-cardiac-specific autoantibodies, including anti-thyroid, anti-gastric parietal cell, anti-islet cell, and anti-adrenal cell were tested by IIF on rat thyroid gland, rat stomach, human pancreas, human adrenal gland, respectively. For all these antibodies, 375 healthy subjects, 211 male and 164 female, aged 38±12 years were considered as controls.
Anti-Ro/SSA (52 kDa and 60 kDa) and anti-La/SSB antibodies were tested using a commercially available ELISA (INOVA Diagnostics, San Diego, California, USA); controls included 75 subjects, 46 male, aged 37±3.
Statistical analysis
Results for quantitative features are given as means ± SD. Student t test, one-way analysis of variance, χ2 (with Yates's correction) or Fisher's exact test was used as appropriate. All p values were two tailed; p values <0.05 were considered to indicate statistical significance. All antibodies were tested in the same sample (eg, at the same time point). All statistical analyses were performed using the StatView software version 5.0 for Apple Macintosh (SAS Institute).
Results
Clinical and diagnostic features in patients with IRAP
Main clinical and diagnostic features of the patients with IRAP are detailed in table 1. At the time of last follow-up, when serum was taken for the immunological antibody tests, 21 (52%) were still receiving treatment as detailed in table 1, all but one were in NYHA class I, one was mildly symptomatic (class II), with a normal echocardiographic left ventricular ejection fraction.
Clinical features in patients with idiopathic recurrent acute pericarditis (n=40)
Frequency of AHA, AIDA and other autoantibodies in IRAP
The frequency and AHA of IgG class in IRAP and controls is shown in table 2. Representative examples of AHA and AIDA patterns are shown in figure 1. The frequencies of cross-reactive 1 AHA and AIDA were higher in IRAP than in control subjects (p=0.0001). Conversely, the frequencies of cross-reactive 2 and organ-specific AHA were similar in IRAP, and control subjects respectively (p=NS). AHA of any type and/or AIDA were found in 27 (67.5%) patients with pericarditis; AHA of the cross-reactive 1 type and/or AIDA were found in 22 (55%). AHA titres among the 25 antibody positive sera were as follows: 1/10 in eight (32%), 1/40 in 10 (40%), ≥1/80 in seven (28%). AIDA titres among the 10 antibody-positive sera were as follows: 1/10 in six (60%), 1/40 in three (30%) and 1/80 in 1 (10%).
Frequency of anti-heart autoantibodies (AHA) and of anti-intercalated-disk autoantibodies (AIDA) by immunofluorescence in patients with idiopathic recurrent acute pericarditis (IRAP) and in controls
The frequency of other autoantibodies in the study groups is shown in table 3. The frequency of positive (titre ≥1/160) antinuclear antibody was higher in pericarditis than in normal subjects (p<0.04). Other non-cardiac-specific antibodies were all negative in IRAP, but two were parietal cell antibody positive and one anti-Ro/SSA positive. The patient who was anti-Ro/SSA positive did not have Sjögren syndrome. None of the patients with IRAP with non-cardiac-specific antibodies had co-occurring autoimmune conditions. Overall 27 (67.5%) patients with IRAP were positive for AHA, AIDA and/or other autoantibodies.
Frequency of non-cardiac-specific autoantibodies by immunofluorescence and ELISA in patients with idiopathic recurrent acute pericarditis (IRAP) and in normal control subjects
Clinical correlates of AHA, AIDA and other autoantibodies in IRAP
Comparison of clinical and diagnostic features in relation to AHA and AIDA status is shown in tables 4–6. There were no differences between patients with AHA and those without (table 4). AHA-positive patients tended to be more frequently receiving combined drug treatment at last follow-up compared with those without (p=0.07). Conversely, patients with high titre (≥1/80) AHA had longer symptom duration (p=0.006), higher number of recurrences (p=0.02), higher end-diastolic posterior wall thickness (p=0.02) and tended to have longer follow-up (p=0.06) and more frequent treatment with combined treatment at the last follow-up (p=0.08) compared with those with low-titre (<1/80) or negative AHA (table 5). AIDA-positive patients had a higher number of recurrences (p=0.01) and of hospitalisations (p=0.0001); AIDA-positive status tended to be more common among patients with refractory symptoms, treated at some stage during follow-up with immunosuppressive drugs and/or pericardiocentesis or pericardiectomy (p=0.05) (table 6). Sensitivities, specificities, positive and negative predictive values for the various AHA and AIDA patterns in IRAP are shown in table 7.
Clinical features and anti-heart autoantibody (AHA) status in idiopathic recurrent acute pericarditis
Clinical features and anti-heart autoantibody (AHA) titre in idiopathic recurrent acute pericarditis
Clinical features and anti-intercalated-disk autoantibody (AIDA) status in idiopathic recurrent acute pericarditis
Sensitivities, specificities, positive (PPV) and negative predictive values (NPV) of anti-heart autoantibody (AHA) and anti-intercalated-disk AIDA autoantibody patterns in idiopathic recurrent acute pericarditis (IRAP)
Discussion
In this study we found an increased frequency of cross-reactive 1 AHA and AIDA in patients with IRAP compared with control subjects, in keeping with autoimmune involvement in at least 55% of patients. Cross-reactive 1 AHA, which are increased in IRAP, have partial cardiac specificity and are also more frequently found in myocarditis or dilated cardiomyopathy than in controls.13–18 Since true IRAP is a rare disease, the series reported here is the largest single-centre cohort collected at a referral centre during a long period and the first to undergo immunological screening for cardiac autoimmunity. Other previously recognised autoimmune features in IRAP12 include its chronic/recurrent course; detection of proinflammatory cytokines in the pericardial fluid but not in plasma, suggesting a local inflammatory reaction8; familial aggregation and a weak association with the HLA-B14 and DRB1*01 alleles that have been associated with other immune-mediated conditions9 21; and efficacy of anti-inflammatory or immunosuppressive treatments.9–11 20–23
In this study positive AIDA status was associated with a high number of relapses, hospitalisations and refractory symptoms, suggesting higher immune activation during the “hot” phases of pericardial inflammation. In addition, higher AHA titres were associated with longer symptom duration and high number of recurrences. These findings further reinforce the autoimmune hypothesis in IRAP. Cross-reactive 1 AHA and AIDA frequency was high in spite of a long duration of symptoms and in some instances of immunosuppressive treatment. However, most immunosuppressive drugs do not lower autoantibody titres.24 In keeping with this, we have recently reported that positive AHA status is an independent predictor of high rejection burden in patients with a longstanding heart transplant receiving chronic dual or triple immunosuppressive regimens comparable to those used in IRAP.25
Surprisingly, the frequency of organ-specific AHA was similar in patients with IRAP and in controls, whereas in biopsy-proven myocarditis and in dilated cardiomyopathy, organ-specific AHA frequency is increased compared with control groups.13–18 There are possible explanations for the discrepancy. First, in autoimmune disease, different antibody specificities are associated with distinct clinical phenotypes12; thus cross-reactive 1 AHA may be more prevalent in pericarditis, organ-specific AHA in myocarditis. This view is supported by earlier reports of serum cross-reactive AHA in other forms of suspected immune-mediated pericarditis—for example, the post-pericardiotomy syndrome or the Dressler syndrome.26 27 Second, in autoimmune disease some autoantibodies are detected earlier in the disease course and others in advanced phases and/or during relapses.28 Longitudinal studies in IRAP should clarify the temporal sequence of appearance of each autoantibody specificity; it may be that organ-specific AHA are early markers, followed by AIDA and cross-reactive AHA in advanced IRAP. This would mirror the temporal sequence observed in patients with dilated cardiomyopathy, where organ-specific AHA are early markers that become undetectable in advanced disease.13–15 29
Three of the autoantigens recognised by the AHA detected by IIF in dilated cardiomyopathy were identified by us as α and β myosin heavy chain and myosin light chain-1v isoforms by western blotting30 and confirmed by others.31 32 It is highly likely that the same autoantigens are also responsible for AHA and AIDA found in IRAP, since AHA and AIDA in IRAP (figure 1) and in biopsy-proven myocarditis with or without concurrent pericarditis16 or in dilated cardiomyopathy sera13 14 17 exhibit the same localisation patterns by IIF. The autoantigen(s) responsible for AIDA have not yet been identified, but there are many candidates.33 So far this is the first study showing increased AHA and AIDA in IRAP. Small variable amounts of sera were available. This prevented us from further testing for autoantigen specificity. We aim at identifying additional autoantigens in newly diagnosed patients; in keeping with other autoimmune diseases, autoantigens involved in early disease stages are more closely related to primary pathogenetic mechanisms and are more likely to be pathogenetically relevant than those which have a role in secondary immunopathogenesis.12 The search for additional antibodies should be extended using pericardial substrate, though it is cumbersome to obtain normal pericardial tissue for analysis. For this reason it is presently unknown whether AHA and AIDA cross react with pericardial tissue.
So far, evidence for a direct pathogenic role of the AHA and AIDA detected by IIF in patients with myocarditis or dilated cardiomyopathy is lacking.13–17 34 However, animal data as well as in vitro and early clinical observations suggest that some of the antibodies (eg, anti-β1 adrenergic receptors, anti-myosin, anti-troponin) detected by other immunological techniques may have a functional role in a patient subset.34–46 Further work is needed to clarify this issue in IRAP, although the lack of clinical and echocardiographic evidence of ventricular dysfunction in our patients at the time of serum testing argues against a direct pathogenic role of AHA or AIDA.
Study limitations
It is not known if myocarditis was associated with pericarditis in our patients. None of the patients had echocardiographic findings suggestive of myocardial involvement (regional or global wall motion abnormalities, increased wall thickness) or increased creatine kinase-MB,47 but endomyocardial biopsy was not performed. Since the diagnosis of myocarditis is based on endomyocardial biopsy, myocarditis cannot be theoretically excluded.48 49 However, typical acute pericarditis findings as those described in this study for the first episode were uncommon in our recent large prospective series of biopsy-proven myocarditis.16 In addition, biopsy-proven myocarditis leads to death or heart transplantation in 27% of patients at 6 years16; conversely, IRAP has a benign prognosis, as confirmed in the present cohort with a long follow-up.19 In support of our conservative approach, none of the patients with IRAP described here presented with one of the clinical scenarios (eg, heart failure or life-threatening arrhythmia) that warrant endomyocardial biopsy according to the recent guidelines.50 Our hypothesis, in keeping with previous observations,5 7 is that myocarditis is unlikely to be present in IRAP.
Current guidelines suggest that the diagnosis of autoimmune pericarditis should be based upon pericardial/epicardial biopsy findings.6 A limitation of our study is that pericardial biopsy was not performed. However, experts advocate that once collagen vascular disease, previous cardiac surgery or myocardial infarction are ruled out, as for our patients, relapsing pericarditis is almost invariably immune-mediated with or without a viral trigger.4 5 7 Pericardial biopsy is not widely used.4 5 7 Last but not least IRAP has a benign prognosis, as reported1 19 45 and confirmed here, thus an invasive approach may not be justified, at least in the majority of patients.4 5 7
Conclusion
The high prevalence of AHA and AIDA shown here strongly suggests that IRAP is an autoimmune disease in a large subset of patients. Whether or not these autoantibodies may provide clinically useful biomarkers of pericarditis relapses and/or non-invasive tools to tailor immunosuppressive treatment warrants future assessment.
References
Footnotes
Funding This work was supported by the Ministry for University Scientific and Technological Research (MURST) Target Projects (1999–2000, Myocarditis: therapeutic impact of etiological diagnosis based upon molecular and immunological findings; 2003–2005, Myocarditis: identification of clinical, molecular and immunological markers for risk stratification), and the Ministry of Health Target Project (2004–2007, Inflammatory cardiomyopathy), Rome, Italy.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Ospedale Niguarda, Milan, Italy.
Provenance and peer review Not commissioned; externally peer reviewed.