Article Text

Abstract
Objective Transcatheter aortic valve implantation (TAVI) has become an alternative to surgical aortic valve replacement (sAVR) in selected high risk patients. While improvement in left ventricular function after TAVI has been demonstrated, little is known about the impact on right ventricular (RV) function. Since postoperative RV dysfunction is linked to adverse outcomes, the authors sought to investigate the effect of TAVI and aortic valve replacement (AVR) on RV function using speckle tracking echocardiography.
Design Cross-sectional study in tertiary healthcare setting.
Setting 101 patients with severe symptomatic aortic stenosis (age 81±11 yrs) who underwent TAVI and 22 patients who underwent sAVR were included. RV function was assessed using 2D longitudinal strain (RV-LS), fractional area change and tricuspid annular plain systolic excursion before and after sAVR and TAVI (median 89 days).
Results Although the TAVI group had worse baseline characteristics, RV function remained unchanged in this group whereas significant deterioration of RV function was observed in patients undergoing conventional AVR: RV-LS (−25.2±6.1 vs −20.0±7.0%; p=0.009), RV-fractional area change (47.0±7.0 vs 39.8±10.7%, p=0.019) and tricuspid annular plain systolic excursion (24±5 vs 16±4 mm, p=0.0001).
Conclusion While TAVI did not affect RV function it deteriorated significantly in patients undergoing sAVR. The authors speculate that this may be related to the detrimental effects of pericardiotomy and, to a lesser degree, cardiopulmonary bypass. While further studies are required to assess the clinical significance of this finding, these data suggest that patients with pre-existing RV dysfunction may benefit from TAVI and that RV function should be incorporated into future risk scores.
- Cardiac function
- congenital heart disease
- echocardiography
- pericardial disease
- valvular disease
- imaging and diagnostics
- heart failure
- interventional cardiology
- percutaneous valve therapy
Statistics from Altmetric.com
- Cardiac function
- congenital heart disease
- echocardiography
- pericardial disease
- valvular disease
- imaging and diagnostics
- heart failure
- interventional cardiology
- percutaneous valve therapy
Introduction
Transcatheter aortic valve implantation (TAVI) has become an alternative to surgical aortic valve replacement (sAVR) in selected patients considered to be at a high risk for conventional cardiac surgery. Risk stratification is usually based on score systems such as the EuroSCORE or the Society of Thoracic Surgeons' risk model.1–3 Early results of TAVI have been published showing high procedural success and a low complication rate.4
While the impact of sAVR or TAVI on the function of left ventricle has been studied with various imaging modalities, little is known about the impact on right ventricular (RV) function.5–9 RV failure after cardiac surgery, although not frequent, has been linked to adverse outcome in this setting.10 ,11 The aetiology of postoperative RV dysfunction is likely multifactorial and related to factors such as pericardiotomy with perturbation of myocardial blood flow, hypothermia and immune-inflammation on cardiopulmonary bypass. Interestingly, both the EuroSCORE and the Society of Thoracic Surgeons' risk model do not account for preoperative RV dysfunction although it is one of the strongest predictors of RV failure after cardiac surgery.2 ,3 ,11 ,12 Since TAVI does not require cardiopulmonary bypass or pericardiotomy, we hypothesised that it may have less detrimental impact on RV function. In the current study, we sought to assess the impact of sAVR and TAVI on the RV function using conventional echocardiographic parameters as well as speckle tracking echocardiography.
Patients and methods
Patients
We studied all 101 consecutive adult patients with severe aortic stenosis in whom TAVI was performed between February 2008 and May 2010 at our institution. The sAVR group consisted of 22 consecutive patients with adequate preoperative and postoperative echocardiograms in whom sAVR was performed at our institution between May 2008 and July 2009.
Echocardiographic measurements
Transthoracic echocardiography was performed prior to intervention (median time 19 days (IQR 7–32 days) in the TAVI group and 18 days (IQR 11–36 days) in the sAVR group) and after intervention (70 days (IQR 26–106 days) in the TAVI group and 100 days (IQR 68–117 days) in the sAVR group). With the subject in the left lateral position, transthoracic examinations were conducted according to current guidelines.13–15 Echocardiographic studies were performed in all subjects with a Vivid 7 Dimension system (Vingmed, General Electric, Milwaukee, Wisconsin, USA). All recordings were stored digitally and analysed offline. Tricuspid annular plane systolic excursions (TAPSE) were measured in the apical 4-chamber view using M-Mode echocardiography. TAPSE was defined as the maximal excursion at the lateral aspect of the tricuspid annulus.
The cine loops for assessment of peak longitudinal 2D strain of the right ventricle were recorded in apical 4-chamber views and optimised by changing the transducer scan width to achieve a frame rate of at least 40/s. Further analysis was conducted with dedicated, commercial software (EchoPac, GE Vingmed). The speckle tracking analysis consisted of marking the endocardium, defining the width of the region of interest, reflecting the mean distance from endocardium to pericardium and using the analysis software package.
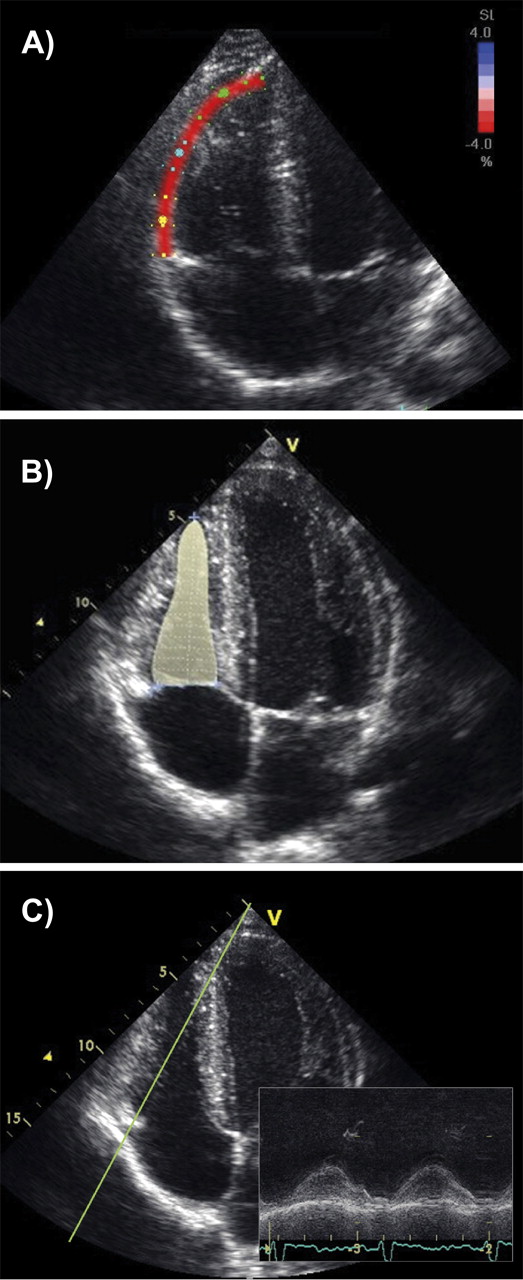
Peak 2D longitudinal strain (LS) and strain rate were defined as the peak negative value on the strain curve during the entire cardiac cycle. The global LS and strain rate value for the RV was calculated as a mean value for the basal and middle segment of the free RV wall. Figure 1 shows an example of echocardiographic measurements of RV function.

Example of echocardiographic measurements of right ventricle (RV) function including 2D longitudinal RV strain (A), fractional shortening (B) and tricuspid annular plane systolic excursion (C).
Statistical analysis
All values are presented as mean ± SD. Comparisons between groups were made using two-tailed Student t test or Welch test and non-parametric methods depending on data distribution. The change of RV function over time in the sAVR compared with the TAVI group was evaluated using an ANOVA test for the interaction effect of time-point and treatment group.
Regression analysis was used to assess the relation of independent variables to the change in the RV function parameters. Statistical analyses were performed using R V.2.13.0 (R Foundation for Statistical Computing, Vienna, Austria) and MedCalc 11.3.3.0 Software (Mariakerke, Belgium).
Results
Patient characteristics and postprocedural status
Baseline characteristics are presented in table 1. As expected, patient groups differed significantly. Patients in the TAVI group were older (81±11 vs 71±12 years, p=0.0004) compared with the sAVR group and presented with more pronounced symptoms. None of them was in New York Heart Association Functional Class (NYHA) I, and 17% presented with symptoms at rest (NYHA IV). There was a trend towards more patients with previous cardiac surgery and renal impairment (Creatinine >200 μmol/l) in the TAVI compared with the sAVR group (25% vs 5% and 31% vs 9%, respectively; p=0.07 for both) and the perioperative risk estimated by EuroSCORE was markedly higher in the TAVI than in the aortic valve replacement (AVR) group (24.3±14.6% vs 7.2±4.7%, p<0.0001).
Baseline characteristics of the transcatheter aortic valve implantation (TAVI) and surgical aortic valve replacement (sAVR) group
In the sAVR group, two patients received a mechanical aortic valve prosthesis (St. Jude Medical bileaflet valve), while the remaining patients received bioprostheses (Carpentier Edwards bioprosthesis, 4; Carpentier Edwards Perimount Bioprosthesis, 16). In this group, 19 patients underwent isolated AVR (four with aortic surgery), while three patients required additional coronary artery bypass graft surgery. The surgical access was via a conventional median sternotomy in all patients. Patients were operated in mild hypothermia (core temperature being 33.1, range 28.0–36.9°C) and all received retrograde blood cardioplegia. The cross-clamp time was 66.8±18.7 min and cardiopulmonary bypass time 110.8±29.6 min. There were no significant differences in the cross-clamp time and cardiopulmonary bypass time between patients with isolated AVR and those with additional procedures. All surgical patients had a favourable postoperative course without any serious 30-day complications.
In the TAVI group, the majority (60 patients) underwent transfemoral aortic valve implantation while 41 patients had limited vascular access and required a transapical approach. Overall, 95 patients received an Edwards Sapien valve, while six patients underwent implantation of an Edwards Sapien XT valve. The 30-day mortality was 10% and was due to bleeding, sepsis, stroke, aortic haematoma, endocarditis, multiple organ failure or pneumonia in two, two, two, one, one, one and one patients, respectively. Strokes occurred in 5% and 6% of the patients required a pacemaker implantation. There was a significant difference in the prevalence of clinically relevant pleural effusion between groups (32% in sAVR group vs 10% in TAVI group, p=0.018). This may, at least in part, be related to RV dysfunction.
Transthoracic echocardiography and speckle tracking analysis
Echocardiographic data are shown in table 2. Aortic valve area before TAVI and sAVR was similar with 0.61±0.20 cm2 and 0.73±0.24 cm2 (p=0.7). The valve area reached after intervention was also comparable (1.60±0.34 cm2 vs 1.60±0.44 cm2, p=1.0).
Echocardiographic data for the transcatheter aortic valve implantation (TAVI) and surgical aortic valve replacement (sAVR) group before and after the procedure
Impact of intervention on RV size and function
Preinterventional RV size did not significantly differ between TAVI and sAVR patients (table 2). End diastolic RV inflow diameters increased in the sAVR group postoperatively compared with preoperative values (41.7±4.1 vs 39.3±4.7 mm; p=0.048), while the end diastolic RV area did not change significantly (17.2±4.3 vs 16.3±3.4 cm2; p=0.31). In the TAVI group, RV inflow diameters and end diastolic RV area remained unchanged after valve implantation compared with preinterventional values.
RV systolic pressure, as measured invasively, was similar in the TAVI and sAVR groups (46.5±16.7 vs 44.7±19.7 mm Hg; p=0.7), suggesting that both groups had similar degrees of secondary pulmonary hypertension.
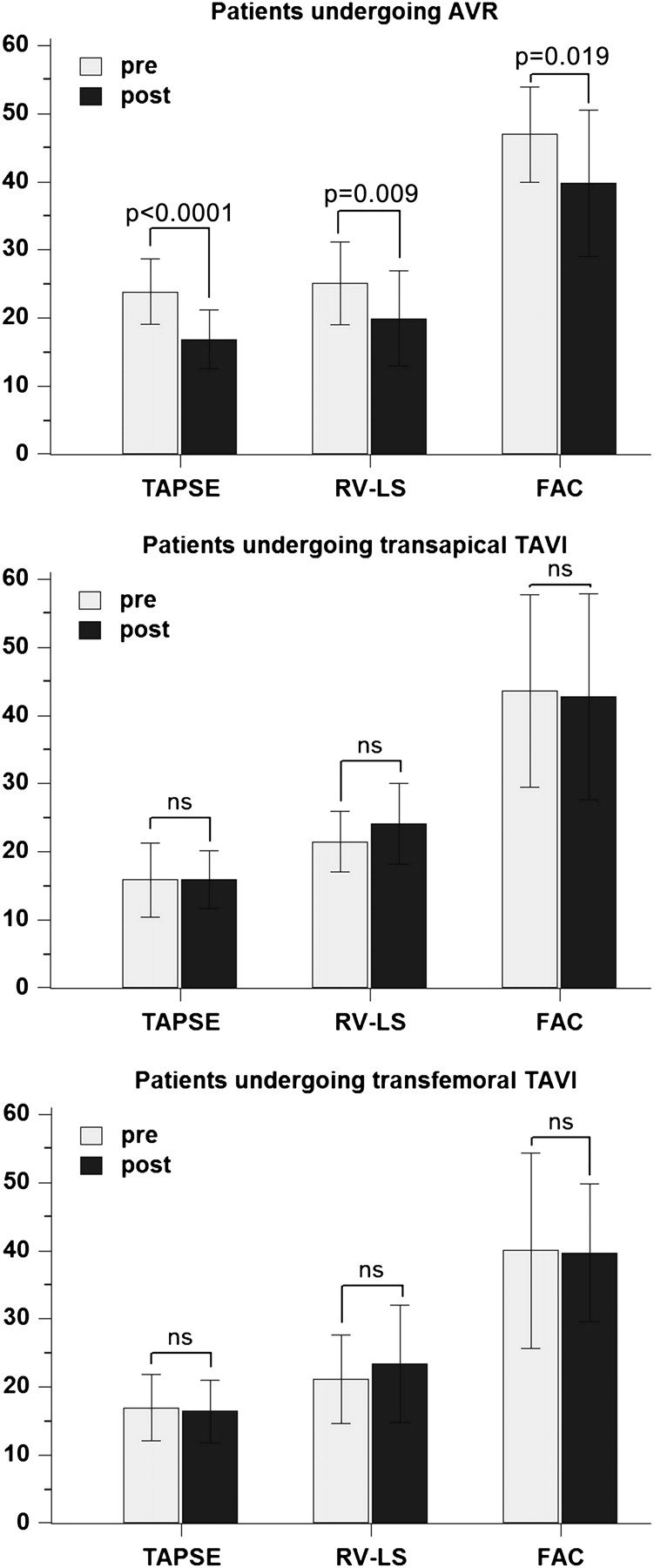
Baseline RV systolic function was significantly better in the sAVR compared with the TAVI group based on TAPSE and RV-LS measurements (24.1±5.0 mm vs 15.9±4.7 mm, p<0.0001 and −25.2±6.1% vs −21.3±5.8%, p=0.006, respectively). After TAVI, however, these parameters did not change significantly (table 2 and figure 2), while a marked deterioration in TAPSE (24.1±0.5.0 vs 15.9±4.1 cm; p<0.0001), RV-LS (−25.2±6.1 vs −20.0±7.0%; p=0.009) and RV fractional area change (FAC) (47.0±7.0 vs 39.8±10.7%; p=0.019) was found in the sAVR group. Considering a reduced RV function with a TAPSE or FAC below 16 mm or 35%, respectively, there were three patients (14%) before but 13 patients (62%) after the surgery who had impaired RV function in the sAVR group. The change in none of the parameters of RV function correlated with the cross-clamp and bypass time. There was no significant deterioration of any parameter of RV function after TAVI neither in patients undergoing transapical nor transfemoral TAVI (figure 2).

{kind=link}
{kind=link}
Changes in the right ventricle (RV) function parameters in patients undergoing surgical aortic valve replacement (AVR), transapical transcatheter aortic valve implantation (TAVI) and transfemoral TAVI. TAPSE, tricuspid annular plane systolic excursion (mm); RV-LS, RV- longitudinal strain, absolute value of the global RV-LS (%); FAC, RV fractional area change (%); p values relate to paired t tests between groups.
Paired t test showed a significant reduction in RV function in patients undergoing sAVR while no such effect was seen in the TAVI group (figure 2).
The ANOVA test for the interaction effect of time point (pretreatment; 0–2, 2–4, 4–6 and >6 months post-treatment) and group (sAVR–TAVI) confirmed that the change of RV function over time was significantly different for sAVR compared with TAVI (p value for the interaction effect 0.0016 and 0.007 for TAPSE and RV-LS, respectively).
In all, 42% of patients in the surgical group had a non-dominant right coronary artery (RCA) on preoperative coronary angiography. There was no significant difference in postoperative RV function between this group and patients with a dominant RCA (p=0.77, p=0.61, p=0.98 for TAPSE, FAC and RV-LS, respectively).
On the univariate regression analysis including all categorical parameters used for EuroSCORE calculation and study group assignment, only the latter was found to be significantly related to the change in RV-LS and TAPSE (R2=0.17, p=0.002 and R2=0.34, p<0.0001, respectively). On this analysis, however, there was no significant relation of assignment of study group to the change in RV-FAC (R2=0.12, p=0.056).
Discussion
This study evaluated the possibly different effects of TAVI and sAVR on RV function. Including novel parameters of intrinsic myocardial function, we found a significant deterioration in RV function after conventional AVR, while RV function was largely unaffected by TAVI. This difference between the groups persisted after accounting for the different baseline risk profile. The deterioration in RV function as a consequence of cardiac surgery in general is consistent with the results of previous surgical studies.16–18 RV function and its changes with TAVI have so far not been studied in detail in larger patient populations. Although reporting only very small patient groups (≤20 patients) and providing limited information on RV function (TAPSE only in one study and largely angle dependent tissue Doppler measurements in the other study), two very recent publications support the finding that TAVI—in contrast to sAVR—does not negatively affect RV function.19 ,20 Pericardiotomy that has been reported to result in perturbation of myocardial blood flow in the right ventricle and to negatively affect RV end diastolic pressure could be one explanation.21 ,22 The systemic inflammatory response due to the release of pro-inflammatory cytokines in association with cardiopulmonary bypass could be another reason for the damage of RV myocardium.23 A recent intraoperative study, however, has highlighted that RV myocardial function declines almost immediately after the opening of the pericardium, suggesting that cardiopulmonary bypass is not the major cause of the observed deterioration in RV function.24 Instead, loss of the pericardial support and the resulting increase in transmural pressure with increased wall stress, which could injure the myocardium or make it susceptible to a change in behaviours when the pericardial constraint is lost, may be the predominant mechanism for this finding. The lack of a detrimental effect of TAVI on the RV may be especially important for high operative risk patients as the development of postoperative RV dysfunction in high risk patients has been reported to be associated with increased morbidity and mortality.25 ,26 To date, baseline RV function is not routinely considered when selecting patients for TAVI or sAVR. The results of the current study suggest that in patients with pre-existing RV dysfunction, sAVR could lead to further deterioration of RV function, while no further deterioration is to be expected with TAVI. Interestingly, no deterioration in RV function was found in TAVI patients who underwent transapical valve implantation suggesting that while extensive pericardiotomy to expose the heart fully adversely affects RV function, the limited pericardiotomy required for transapical TAVI does not have the same negative impact on RV function.
In addition, pulmonary hypertension and depressed RV function increase the risk of non-cardiac surgery. Even for TAVI, therefore, procedural risk may be increased in this setting.27 ,28
Limitations of the study
The follow-up time of approximately 3 months in our study was relatively short. Further studies with a longer follow-up period are required to assess the long-term impact of TAVI and sAVR on the RV function. It is also unclear at present how much impact on outcome the different effects of sAVR and TAVI on RV function have.
The differences in baseline characteristics may be considered as a limitation of this study in general. However, the fact that RV function was not affected in TAVI patients despite their significantly worse baseline characteristics makes it highly unlikely that the different effects of TAVI versus sAVR on RV function should not be present in patient groups with comparable baseline characteristics.
We cannot completely exclude the possibility that sAVR patients who underwent repeat postsurgical echocardiograms and were included in the study represent a biased subgroup with a higher risk profile. We do not, however, operate a policy to determine timing of echocardiographic reassessment based on preoperative risk profile.
The TAVI cohort which consists of two subgroups is significantly larger than the sAVR group included. This may be regarded as a major limitation of the study; however, the study results are significant with the given group size and it is unlikely that including more sAVR patients would relevantly alter the results of the study.
The follow-up time in our study was limited. Furthermore, this is primarily an echocardiographic study and we were not able to demonstrate differences in clinical outcome between both subgroups that could be related to differences in RV function. A potential impact on clinical outcome needs to be evaluated in a larger prospective trial with longer follow-up.
Conclusions
While RV function is not affected by TAVI, it appears to deteriorate at least temporarily after sAVR. We speculate that this may be related to the detrimental effects of pericardiotomy and to a lesser degree to cardiopulmonary bypass. While further studies are required to assess the clinical significance of this finding, these data suggest that patients with pre-existing RV dysfunction may benefit from TAVI and that RV function should be incorporated into future risk scores.
Key messages
While transcatheter aortic valve implantation did not affect right ventricular (RV) function, it deteriorated significantly in patients undergoing surgical aortic valve replacement. We speculate that this may be related to the detrimental effects of pericardiotomy and to a lesser degree to cardiopulmonary bypass. While further studies are required to assess the clinical significance of this finding, these data suggest that patients with pre-existing RV dysfunction may benefit from transcatheter aortic valve implantation and that RV function should be incorporated into future risk scores.
References
Footnotes
See Editorial, p 1265
Funding The Adult Congenital and Valvular Heart Disease Center, University Hospital of Muenster has received support by the EMAH Foundation Karla Voellm, Krefeld, Germany. AK was supported by the Deutsche Herzstiftung e.V.
Competing interests HB acts as a consultant and proctor for ‘Edwards Lifesciences’; all the other authors have no disclosures. For HB, the ICMJE form will be uploaded.
Ethics approval The ethics approval was provided by the Research Ethics Committee, University of Muenster, Germany.
Provenance and peer review Not commissioned; internally peer reviewed.