Article Text

Abstract
Objectives To investigate the respective associations and clinical usefulness of the metabolic syndrome (MetS) and its individual components to predict the risk of first coronary heart disease (CHD) events in elderly.
Design The Three-City is a French prospective multisite community-based cohort.
Setting Three large French cities: Bordeaux, Dijon and Montpellier.
Participants 7612 subjects aged 65 and over who were free of CHD at baseline.
Main outcome measures The MetS was defined by the 2005 National Cholesterol Education Program Adult Treatment Panel III criteria.
Results During a median follow-up of 5.2 years, 275 first CHD events were adjudicated. The MetS was associated with increased risks of total (adjusted HR: 1.78; 95% CI 1.39 to 2.28), fatal (HR: 2.40; 95% CI 1.41 to 4.09) and non-fatal (HR: 1.64; 95% CI 1.24 to 2.17) CHD events. The association with total CHD was significant in women (HR: 2.56; 95% CI 1.75 to 3.75) but not in men (HR: 1.39; 95% CI 0.99 to 1.94; p for interaction=0.012). When in the same multivariable model, hyperglycemia and abdominal adiposity in women, hyperglycemia, lower HDL cholesterol and abdominal adiposity (inverse association) in men were the components significantly associated with CHD. The components of the MetS but not the MetS itself improved risk prediction beyond traditional risk factors (NRI= 9.35%, p<0;001).
Conclusion The MetS is a risk marker for CHD in community-dwelling elderly subjects but may not be useful for CHD risk prediction purposes compared to its individual components.
- Metabolic syndrome
- coronary heart disease
- elderly
- risk stratification
- psychology/psychiatry
- epidemiology
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Introduction
The metabolic syndrome (MetS) has been widely associated with incident type II diabetes, cardiovascular disease (CVD) and total mortality risks primarily in the middle-aged.1–4 The incidence rate of CHD and the prevalence of the MetS both increase with age, suggesting that assessing the association between the MetS and CHD risk in elderly may have public health implications. In a recent cross-sectional analysis of the Three City Study involving French community-based older adults, participants with the MetS at baseline had higher degree of subclinical atherosclerosis as measured by the presence of carotid plaques and intima-media thickness.5 This suggests that the MetS may be a risk marker for CHD in older adults. So far however, this issue has been addressed by only few studies.6–9 Except the Cardiovascular Health Study, these studies covered a restricted age range (60–79 years or 70–79 years) and in one study, participants were all women.6–9 Most studies used the 2001 NCEP ATP III criteria although significant changes and new definitions occurred since 2005.10–13 The impact of these changes on the association between the MetS and subsequent CHD has yet not been systematically evaluated in the elderly population. Moreover, there is still controversy as to whether the MetS adds predictive information for CHD risk beyond its individual components. This is a major question as it raises the clinical usefulness of the MetS.
Therefore, our aims were first to quantify the associations between the MetS and its individual components with the risk of CHD and second to evaluate the added value of the MetS for CHD risk prediction beyond its individual components. These two issues were addressed in older men and women who were participants of the Three City Study.14
Methods
Study population
The Three-City Study is a French multicentre prospective cohort investigating the determinants of CHD, stroke and dementia in community-dwelling elderly. Details of the protocol have been previously described.14 Briefly, community-dwellers aged 65 years and over were selected from the electoral rolls of three large cities and then invited to participate in the study. Overall, 9294 subjects (3649 men and 5645 women) agreed to participate in the study including 2104 from Bordeaux (South-West), 4931 from Dijon (North-East) and 2259 from Montpellier (South). The study protocol had been approved by the Ethical Committee of the University Hospital of Kremlin-Bicêtre. Each participant had signed an informed consent.
Baseline data collection and examination
Trained interviewers conducted face-to-face interviews, using a standardised questionnaire. A wide range of information was collected including demographic characteristics, educational level, occupation, daily life habits such as smoking and alcohol consumption and functional status. Past history of CHD included history of angina pectoris, myocardial infarction or revascularisation procedure (percutaneous transluminal angioplasty or coronary bypass graft surgery). Information on all medications they had regularly used in the past month was also recorded. Brachial blood pressure was measured twice after at least 5 min of rest in a seated position, with an appropriately sized cuff placed on the right arm, using a validated digital electronic tensiometer (OMRON M4, OMRON Corp., Kyoto, Japan). Height and weight were measured in a subject in a light dressing. Blood was collected following overnight fasting and centralised standard measurements of lipids and glucose levels were performed. Diabetes was defined as a fasting blood glucose level ≥7 mmol/l and/or drug treatment for diabetes. LDL cholesterol level was calculated using Friedewald equation for triglycerides values ≤4.5 g/l.
MetS definitions
The main analysis was performed using the 2005 revised National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) definition (11), requiring the presence of at least three of the following criteria: abdominal obesity (waist circumference ≥102 cm in men and ≥88 cm in women); triglycerides level ≥150 mg/dl (1.7 mmol/l) or nicotinic acid or fibrate treatment; HDL cholesterol level <40 mg/dl (1.0 mmol/l) in men and <50 mg/dl (1.3 mmol/l) in women or nicotinic acid or fibrate treatment; fasting glycaemia ≥100 mg/dl (5.6 mmol/l) or medication for diabetes; systolic blood pressure ≥130 mm Hg or diastolic blood pressure ≥85 mm Hg or antihypertensive medication use. In additional analyses, the International Diabetes Federation (IDF) definition and the original 2001 NCEP ATP III criteria were used for comparisons.10 12
Follow-up and CHD events ascertainment
At each follow-up visit, subjects were asked to report any new severe medical event or hospitalisation since the last contact. For all subjects reporting a possible CHD event, all available clinical information was collected including emergency medical service and hospitalisation reports, interview with the patient's physician or the family. CHD events were validated by an independent expert committee. CHD was defined as hospitalised angina pectoris, hospitalised myocardial infarction, CHD death (I210-I219, I251-I259 and I461 ICD-10 codes), or revascularisation (percutaneous intervention or coronary artery bypass-grafting). Incident CHD status was known for 97% of the participants.
Statistical analysis
The baseline characteristics were compared according to the presence of the MetS using χ2 tests (or Fisher's exact test when appropriate) and Student tests for categorical and continuous variables respectively. Cox proportional hazard regression was used to estimate the HRs of the MetS for CHD over 6 years. HRs were adjusted for age, gender, study center, educational level (<9, 9–11, ≥12 years), living alone, incapacity in IADL, smoking status (never, former, current), LDL cholesterol level and statin treatment on an a priori basis. Analysis was performed in the whole cohort and by gender. An interaction term between gender and the MetS was included in the model and the Wald test was used to evaluate the statistical significance of the interaction term. To identify the criteria of the MetS the most predictive of CHD events, all components of the MetS were considered in a single model together with the baseline confounders mentioned above. To assess the respective association of the MetS and its individual components with CHD, all the components of the MetS and the MetS were then included in the same model together with the baseline confounders. In additional analyses, the analyses were repeated using either the IDF or the 2001 NCEP criteria. The added value of the MetS for CHD risk prediction was quantified by calculating net reclassification improvement (NRI) between the risk factors base model that included age, gender, study center, educational level (<9, 9–11, ≥12 years), living alone, incapacity in IADL, smoking status (never, former, current), LDL cholesterol level and statin treatment, and the ‘novel’ model additionally including the MetS.15 For comparison, we also calculated the NRI between the risk factors base model and a model additionally including the five components of the MetS in their continuous form. We used the 10-year Framingham CHD risk categories (<10%, 10%–20% and over 20%) interpolated to 6 years of follow-up (<6%, 6%–12% and over 12%) to compute the NRI. We also calculated the Harell-C index, an extension of the area under the receiving operating curves suited for censored data, to separately estimate whether the addition of the MetS and of its individual components increased the discrimination ability of the risk factors base model.16 The 95% CIs of the Harell-C indexes of each model together with differences between the Harell-C indexes, were internally validated by bootstrapping with 1000 replications. The proportional hazards assumption of the Cox proportional hazard model was checked using Schoenfeld's global test. All statistical tests were two-sided using a type I error of 0.05. Analyses were computed using STATA® (release 11).
Results
Baseline characteristics
Of the 9294 study participants, 1114 were excluded since they had a personal history of CHD at baseline (n=1105) or had their baseline CHD status unknown (n=9). There were 568 additional subjects with missing information on the MetS status at baseline. They were 3 years older on average, more often women, alone, hypertensive, diabetics, less educated, and had higher mean triglycerides and lower mean HDL cholesterol than the 7612 subjects with available MetS at baseline (Flow chart on supplemental figure 1).
The median age of the 7612 participants was 73.2 years (inter quartile range: 69.5–77.4) and 63% were women. The MetS as defined by the 2005-revised NCEP ATP III criteria was present in 29.2% of the participants, 29.4% in women and 28.9% in men. The baseline characteristics of the participants according to the presence of the MetS are reported in table 1 separately in women and men.
Baseline characteristics by gender according to the presence of the MetS*
Association between the MetS and new CHD events
During a median follow-up of 5.2 years, 110 subjects with the MetS (10 with revascularisation, 39 with angina, 33 with myocardial infarction and 28 with fatal CHD) and 165 without the MetS (two with revascularisation, 67 with angina, 66 with myocardial infarction, and 30 with fatal CHD) experienced a first CHD event. This yielded a mean annual CHD incidence rate of 10.63 (95% CI 8.67 to 12.81) per 1000 person-years in subjects with the MetS compared to 6.40 (95% CI 5.49 to 7.45) per 1000 person-years in subjects without the MetS (p<0.001). CHD incidence rates were significantly higher in subjects with compared to subjects without the MetS in women only (Supplemental figure 2).
As shown in table 2, in multivariate adjusted analysis, subjects with the MetS had a significant increased risk of total CHD (HR: 1.78; 95% CI 1.39 to 2.28), fatal CHD (HR: 2.40; 95% CI 1.41 to 4.09) and non-fatal CHD events (HR: 1.64; 95% CI 1.24 to 2.17). There was a significant quantitative interaction with gender: the multivariable HRs for total CHD were 2.56 (95% CI 1.75 to 3.75) in women compared to 1.39 (95% CI 0.99 to 1.94) in men (p for interaction: 0.012). After excluding subjects with type 2 diabetes at baseline (n=665; 62 CHD events), the association with the MetS remained highly significant for fatal CHD events in the overall cohort and in women.
Incidence rates of CHD and HRs of the MetS* for CHD
Respective association of the MetS and its components with new CHD events
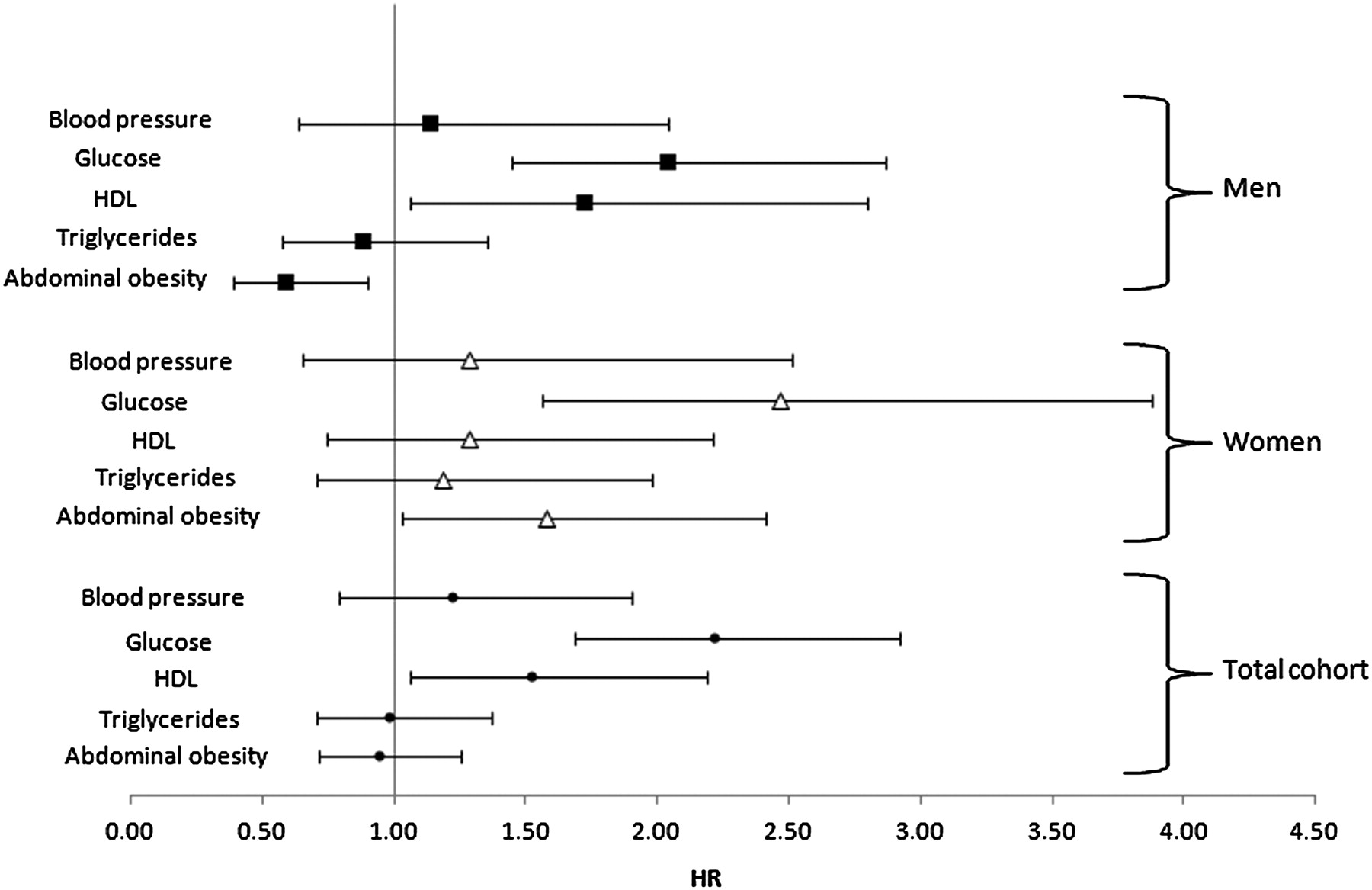
As shown in figure 1, when all the MetS components were in the same Cox model together with baseline confounders, elevated fasting glycaemia (HR: 2.22; 95% CI 1.69 to 2.92) and lower HDL cholesterol (HR: 1.52; 95% IC: 1.06-2.18) were the criteria significantly associated with total CHD events in the overall cohort. In women, they were elevated fasting glycaemia (HR=2.47; 95% CI 1.56 to 3.87) and elevated abdominal adiposity (HR=1.57; 95% IC: 1.03-2.41). In men they were elevated fasting glycaemia (HR=2.04; 95% CI 1.45 to 2.87), lower HDL cholesterol (HR=1.72; 95% CI 1.06 to 2.79) and elevated abdominal adiposity (HR=0.59; 95% CI 0.39 to 0.90). After further adjustment for the MetS, the significant components and the magnitude of their association with CHD remained the same whereas the MetS was no longer associated with CHD (HR: 0.89; 95% CI 0.53 to 1.49) in the overall cohort. The same findings were observed in analyses stratified by gender (not shown).

{kind=link}
Mutually adjusted HRs of the individual components of the MetS* for CHD. The Three City Study.
Improvement in discrimination for CHD risk associated with the MetS and its components
As shown in table 3, adding the MetS to a risk factors base model that comprised age, gender, study center, educational level, living alone, incapacity in IADL, smoking status, LDL cholesterol and statin treatment modestly improved discrimination, that is, the capacity to differentiate those who will suffer a CHD event from those who will not, since 3.12% of the individuals were reclassified in adequate risk categories (p=0.06). By contrast, adding the components of the MetS (in their continuous form) significantly improved discrimination of the risk factors base model, since 9.35% of the individuals were reclassified in adequate risk categories (p<0.001). Similarly, adding the MetS to the risk factors base model marginally improved the value of the Harell-C-index (from 0.706 to 0.718) contrary to the addition of the individual components of the MetS (from 0.706 to 0.761).
Harell-C index and net reclassification improvement associated with the MetS and its individual components
Additional MetS definitions
The frequency of the MetS remained similar when the IDF definition was used (28.6%) but was of 14.2% when the 2001 NCEP ATP III criteria were employed. By contrast associations with CHD were of comparable magnitude whatever the MetS definitions used (Supplemental table 1).
Discussion
In this large prospective cohort of community-dwelling subjects aged 65 and over the MetS as defined by the revised 2005 NCEP ATP III was associated with an 80% increased risk of total CHD events independently of baseline confounders, with a significantly stronger association in women compared to men. However, the MetS failed to improve significantly discrimination for CHD risk, contrary to its individual components.
With the Cardiovascular Health Study, this is the sole community based cohort of elderly subjects covering a wide range of age over 65 years.6 Remaining studies covered a narrowed age range, 70–79 years in the Health Ageing and Body Composition Study, 65–74 years in a Finn study and 60–79 years in the British Women's Heart and Health Study.7–9 Most previous studies used the MetS as defined by the 2001 NCEP ATP III criteria in which treatments for hypertension, dyslipidemia and hyperglycemia are not considered. Elderly subjects represent a highly treated population and exclusion of these treatments may affect the frequency of the MetS and the strength of its association with CHD events in this population. As shown here, the frequency of the MetS was twice less frequent using the 2001 NCEP ATP III criteria compared to the 2005 ATP criteria or the IDF definition that include treatments. By contrast, there was little variation in CHD risk between the 2001 NCEP ATP III definition, the 2005 revised NCEP ATP III definition or the IDF definition in the current study.
The current study suggests that the association of the MetS with CHD was stronger for fatal than non-fatal CHD events. The inclusion of revascularisation in the definition of non-fatal events may have reduced their association with the MetS. However, excluding revascularisation from the definition of non-fatal events did not change this pattern of association (not shown). Moreover, this may reflect a particular association with sudden arrhythmic death as previously shown in middle-aged men.17 The possibility that subjects with the MetS have more severe coronary artery lesions (which may increase their risk of CHD death) is not currently supported by angiographic findings.18 19
We found a stronger association between the MetS and CHD in women compared to men with a highly significant gender interaction. This has been previously observed in the middle-aged population and has been confirmed in two recent meta-analyses.3 4 More conflicting results on this issue has been reported in the elderly.6–9 The putative reasons for this gender interaction remain unclear. The stronger association between type 2 diabetes and CHD in women compared to men has been advocated.20 21 In the current study however, this gender interaction persisted after the exclusion of subjects with type 2 diabetes at baseline. Second, abdominal adiposity may contribute to this gender interaction as it was predictive of CHD in women and inversely associated with CHD in men. While this intriguing inverse association between abdominal adiposity and CHD risk in men may be due to chance, a comparable finding was recently reported for Alzheimer's disease risk.22 Interestingly, in the current study, the gender interaction was no longer observed when the study population was stratified by abdominal adiposity level, the p values for interaction being 0.31 and 0.77 respectively in the obese and the non-obese subjects (not shown). Finally, there may be biological interactions between the individual components of the MetS in women and not or of less importance in men. In the current study, the likelihood ratio of a model predicting CHD and including individual MetS components plus two by two interaction terms was significantly better than the model without interactions in women but not in men (data not shown).
The respective contribution of the MetS and of its individual components for CHD risk remains a matter of debate.23–25 In the current study, several findings argue against the potential clinical usefulness of the MetS to predict the risk of CHD. First, the association between the MetS and CHD events was of lower magnitude than that between elevated fasting glycaemia—the most significant component- and CHD. Second, the MetS was no longer associated with CHD after adjustment for its components. Similar observations have been recently reported in a limited sample of 1221 Swedish men over 70 years for total and cardiovascular mortality, but CHD morbidity was not investigated in that study.26 By contrast, in the Cardiovascular Health Study, the MetS as defined by the 2001 NCEP-ATP III criteria remained predictive of CHD and stroke even after adjustment for its components, although this adjustment attenuated substantially its HR.27 Third, our study shows that the MetS failed to improve in a clinically relevant manner discrimination for CHD risk beyond baseline confounders not including the MetS components. By contrast, discrimination was substantially improved by the addition of the components of the MetS. This latter finding re-emphasises that the classical risk factors remain the cornerstone for CHD risk stratification purposes.
The current study has some limitations. Analysis was based on a single measurement of the MetS. The thresholds currently used for the definition of the MetS may not be suitable for an older population. Residual confounding cannot be excluded and in particular, socioeconomic position from across the life-course has been suggested to be an important confounder, at least in British elderly women.9 The current study includes well-functioning, highly educated subjects and mostly Caucasians, needing caution before extrapolating these results to the frailest and other ethnic groups.
Conclusion
In summary, in this large prospective study of non-institutionalised elderly men and women, the MetS was an independent risk marker of CHD events especially in women. However, while the individual components of the MetS improved significantly discrimination for CHD risk beyond baseline confounders, the MetS did not. Therefore, a systematic assessment of the MetS may not be suitable for CHD risk stratification purposes in the elderly.
Acknowledgments
Marie-Cécile Périer for statistical support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Funding The Three-City Study was conducted under a partnership agreement between the Institut National de la Santé et de la Recherche Médicale (INSERM), the Victor Segalen–Bordeaux II University, and Sanofi-Aventis. The Fondation pour la Recherche Médicale funded the preparation and initiation of the study. The 3C Study was also supported by the Caisse Nationale Maladie des Travailleurs Salariés, Direction Générale de la Santé, MGEN, Institut de la Longévité, Conseils Régionaux of Aquitaine and Bourgogne, Fondation de France, and Ministry of Research–INSERM Programme “Cohortes et collections de données biologiques.” Researchers were independent of funding organisations.
Competing interests None.
Patient consent As mentioned in the manuscript, each participant had signed a french local informed consent.
Ethics approval The ethics approval was provided by Ethical Committee of the University Hospital of Kremlin-Bicêtre.
Provenance and peer review Not commissioned; externally peer reviewed.