Article Text

Statistics from Altmetric.com
Information and communication technology (ICT) has been reported as a useful tool in providing better and cheaper health care, but evidence supporting this statement is scarce. The Editor's choice in this issue of Heart is a randomized trial by Varnfield and colleagues (see page 1770) showing that an ICT-based strategy can improve the use and the efficacy of cardiac rehabilitation (CR) programs after myocardial infarction (MI). CR is a well-established therapy in post-MI patients and reduces both morbidity and mortality, but it is typically underused (<20% of patients). Logistic challenges (lack of time, transportation or geographical access) and competing life demands (as return to work) are the main causes of low CR usage. The ICT-based strategy used to overcome these barriers allows both health and exercise monitoring and delivery of motivational and educational material, using smart phones and a web portal. Their results are impressive: beyond providing similar improvements in 6-minute walk-test performance, the ICT-based strategy showed superior results in terms of weight reduction and quality of life, with higher uptake (80 vs 62%), adherence (94 vs 68%) and completion (80 vs 47%) rates than traditional CR (see figure 1).

(A) Line graphs showing changes in mean±SD for 6 Minute Walk Test, low-density lipoprotein and high-density lipoprotein over 6 months for traditional cardiac rehabilitation (TCR) and Care Assessment Platform-cardiac rehabilitation (CAP-CR), intervention cardiac rehabilitation participants. (B) Box plots of EQ5D-index (median values) and Kessler 10 scores for TCR and CAP-CR, intervention cardiac rehabilitation participants.
In a companion editorial, Drs Turk-Adawi and Grace (see page 1737) conclude that “the study by Varnfield and colleagues provides more compelling, initial evidence that smartphone-based CR can improve utilisation, and results in health outcomes similar to supervised CR programmes.” However, they caution that while this approach might be particularly useful in low resource or remote settings, feasibility studies are needed, followed by randomized controlled clinical trials with a primary endpoint of mortality to establish the benefit of this approach.
Despite robust evidence showing that beta-blocker therapy significantly reduces mortality after myocardial infarction, there is little data on the potential benefit of beta-blockers in patients with stable coronary disease. In a prospective cohort study of 4184 outpatients with stable coronary disease, Professor Bauters and colleagues (see page 1757) found a 1.9% absolute reduction in the risk of cardiovascular mortality at 2 year followup in those on beta-blocker therapy, when adjusted using propensity score (see figure 2).

Cumulative incidence curves for the risk of cardiovascular mortality by ß-blocker use in the propensity-matched cohort.
This observational study is put into context in the editorial by Dr. James Floyd (see page 1741) first by comparison to other observational studies on beta-blocker use in stable coronary disease patients, which have not shown benefit, and then in relation to possible confounding and selection biases that may occur in an observational study. He concludes that: “For now, recommendations from guidelines to consider β-blocker therapy for secondary prevention in this population are appropriately cautious, and clinicians should weigh the potential benefits and harms of β-blocker therapy for each patient individually.”
Also in this issue of Heart is the first description in five patients from two families of globotriaosylceramide-associated cardiomyopathy with a phenotype similar to Fabry disease (see page 1793). Identification of the cause and genotype-phenotype correlates in newly recognized conditions, such as this one, are important not only for the affected individuals, but also for the insights they provide into the mechanisms of myocardial dysfunction.
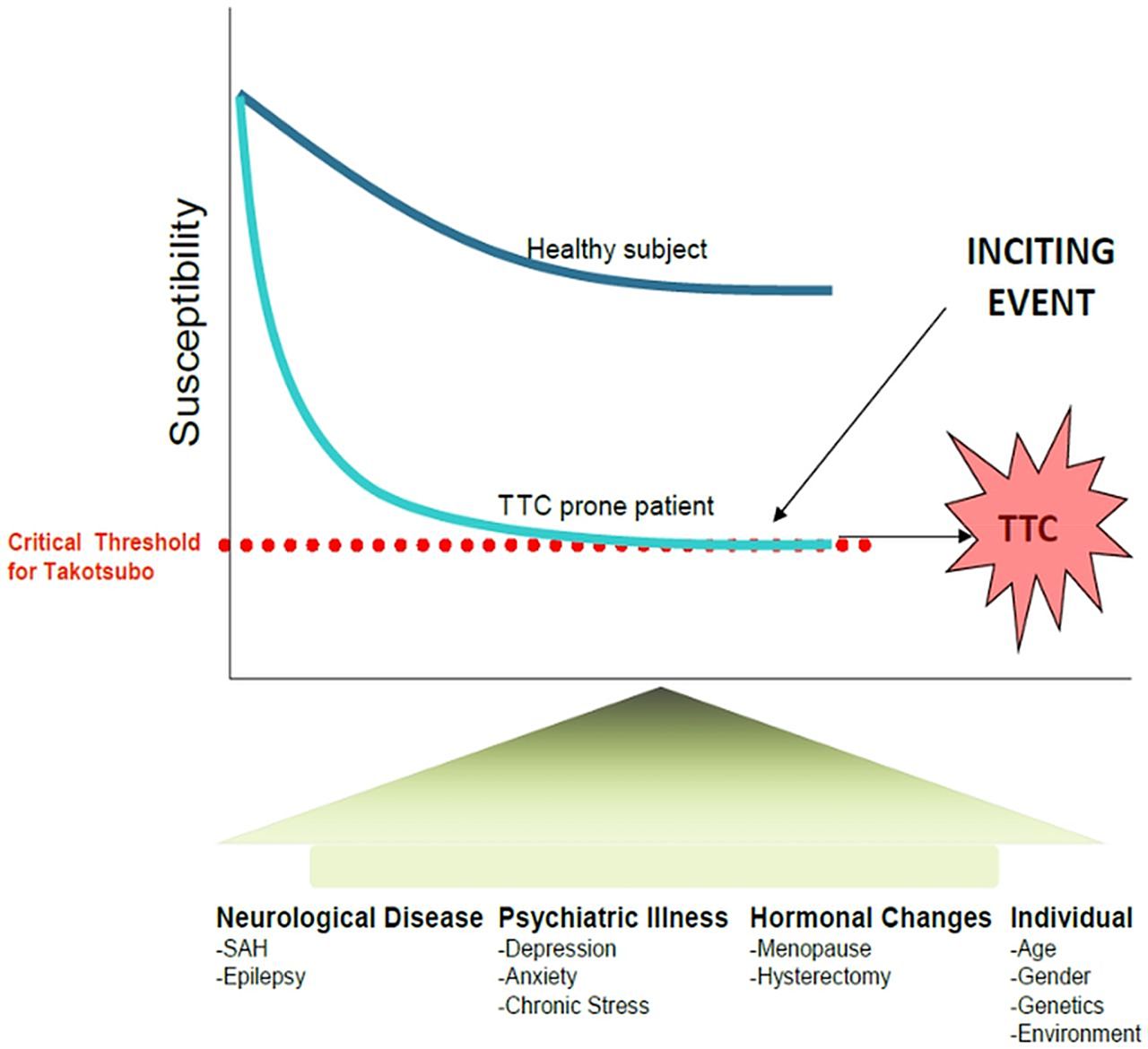
The Education in Heart article on takotsubo cardiomyopathy (see page 1804) discusses the definition, trigger factors, cardiac biomarkers and imaging findings as well as the prognosis and outcomes of this intriguing condition. Unfortunately, the mechanism of disease remains unknown and treatment is largely supportive (see figure 3).
{kind=link}
{kind=link}
{kind=link}
A critical threshold needs to be reached to initiate a cascade of biochemical events causing a takotsubo cardiomyopathy (TTC) event. The susceptibility traits comprise neurologic and psychiatric disease, hormonal changes, age, female gender, genetics, and stressful life events. SAH, subarachnoid haemorrhage.
The first of several state-of-the-art review articles on coronary artery disease appears in this issue with Drs Pilgrim and Windecker (see page 1750) addressing the issue of anti-platelet therapy for secondary prevention of coronary artery disease (CAD). They conclude with the recommendation: “Dual antiplatelet therapy should be continued for a minimum of 1 year among patients with acute coronary syndrome irrespective of stent type; among patients with stable CAD treated with new generation drug-eluting stents, available data suggest no benefit to prolong antiplatelet treatment beyond 6 months.” Tables, graphs and an online supplement provide detailed information on the evidence for benefit for each of the currently available anti-platelet agents.
Try the Image Challenge (see page 1769) question about a finding on coronary angiography with additional interesting images in the explanation of the correct answer.
Linked Articles
- Cardiac risk factors and prevention
- Editorial
- Heart failure and cardiomyopathies
- Editorial
- Education in Heart
- Image challenge
- Coronary artery disease
- Review