Article Text

Statistics from Altmetric.com
Patients with acute myocardial infarction (AMI) may benefit from highly specialized services and interventions, most notably early coronary angiography and revascularization by percutaneous coronary intervention (PCI). These specialized services are not universally available among hospitals, and inter-hospital transfer is the primary means for accessing these services for many AMI patients. Although there is evidence that inter-hospital transfer for the treatment of AMI can reduce cardiac mortality for ST-elevation AMI, the long term benefit of this strategy is controversial, as well as whether this advantage extends to non-ST elevation acute AMI patients.
In order to address these questions, Ranasinghe and colleagues, (see page 1032) from the The George Institute in Sydney, conducted an investigation to assess whether hospitalized AMI patients who are transferred for specialized care during their AMI event have lower long-term mortality, compared to similar patients solely treated at the presenting hospital, evaluating the consistency of findings in transferred patients with different risk profile and among various population subgroups. The authors used a database of over 40 thousand patients with a diagnosis of AMI linked with the register of deaths of the State of New South Wales and matched transferred (25% of total) and non-transferred patients using propensity score matching, as well as performing several sensitivity analyses. They found that transferred patients were about 4 times more likely to undergo coronary revascularization and had lower long-term mortality, compared with patients treated solely at the presenting hospital. This survival advantage was observed in most subgroups analyzed, including non-ST elevation acute coronary syndrome patients (figure 1).

Subgroup analysis of long-term mortality between transferred and non-transferred patients. †P for statistical interaction with IHT, *No interaction term calculated as in-hospital death directly affects long-term mortality. AMI, acute myocardial infarction; IHT, interhospital transfer; STEMI, ST-elevation myocardial infarction; NSTEMI, non-ST-elevation myocardial infarction.
In the companion editorial, Prof Gale and colleagues (see page 998), briefly summarize the previous literature before pointing out the potential limitations of the current study and then concluding: “There is no doubt that improved, harmonised systems of care are needed, which are flexible to the patient's cardiovascular and bleeding risk, estimated reperfusion time, mode of presentation, availability of specialist services and methods of delivery of reperfusion. For NSTEMI, until now, the evidence for inter-hospital transfer was less clear. Ranasinghe and colleagues help alleviate the uncertainty around inter-hospital transfer for NSTEMI, but the best course of action for the individual patient remains difficult to determine in a real-world situation due to the imbalance between transferred and non-transferred patients”.
Overcrowding of emergency departments (ED) is a worldwide issue that can impact on the quality of care and patient satisfaction, with clinical, administrative and financial implications. Missing cases of acute coronary syndrome that presents with a non-specific ECG is also a problem, which can lead to a loss of opportunity for effectively treating diseased patients, and can ultimately lead to a preventable death. In this context, Dr Carlton and colleagues (see page 1041) investigated the ability of a novel accelerated diagnostic protocol (ADP) for suspected acute coronary syndrome in successfully identifying low-risk patients suitable for discharge at the emergency department. The proposed ADP, which included high-sensitivity troponin, clinical and ECG data, was effective in ruling out an acute coronary syndrome (figure 2) with a sensitivity of 98.8% and a negative predictive value of 99.7%, and was superior to a stand-alone single measurement of high-sensitivity troponin result in guiding discharge decisions. They conclude that this protocol has the potential to allow early discharge in 40% of patients with suspected ACS, but it has to be tested in a multicenter randomized controlled trial before being used in clinical practice.

Participant recruitment flow chart. The 132 patients who missed the consent process were similar in age, gender, risk factors and m-Goldman scores (p>0.05 for all). ADP, accelerated diagnostic protocol; AMI, acute myocardial infarction; TRUST, Triage Rule-out Using high-Sensitivity Troponin.
In the companion editorial, Prof Hall and colleagues (see page 1000) discuss these results and argue that currently society and health care providers must choose between “the expectation that all patients should be correctly and rapidly diagnosed 100% of the time and never experience adverse consequences” versus “the need to balance competing healthcare needs, financial and practical considerations”, i.e. to do “the greatest good of the greatest number”, an unsolved dilemma.
This issue of Heart also includes what is sure to become a landmark paper by Dr Dahl and colleagues (see page 1015) about low-flow low-gradient (LFLG) severe aortic stenosis (AS) with normal left ventricular ejection fraction (EF). In a retrospective review of the Mayo Clinic echocardiographic database over an 11 year period, 78 patients were identified with LFLG severe AS, defined as an aortic valve area<1.0 cm2, stroke volume index<35 mL/m2, mean aortic gradient<40 mm Hg and an EF ≥50%, in whom there was at least 1 other echo in the prior 5 years. Contradicting our preconceived notions, only 5% of these patients had evidence for high gradient severe AS before developing LFLG severe AS. Instead, over the preceding 5 years there was evidence for gradually increasing LV wall thickness and decreasing chamber size with hemodynamics characterized by a reduction in stroke volume and valve area without ever going through a phase of high gradient AS (figure 3).

Serial changes in (A) aortic valve area, p<0.001 for low-flow, low-gradient severe aortic stenosis (LFLG-sAS) vs normal-flow, high-gradient (NFHG)-sAS and for LFLG-sAS vs normal-flow, low-gradient (NFLG)-sAS; (B) aortic valve area index, p<0.001 for LFLG-sAS vs NFHG-sAS and p=0.02 for LFLG-sAS vs NFLG-sAS; (C) aortic valve maximum velocity, p<0.001 for LFLG-sAS vs NFHG-sAS and p=0.52 for LFLG-sAS vs NFLG-sAS; and (D) aortic valve mean gradient, p<0.001 for LFLG-sAS vs NFHG-sAS and p=0.02 for LFLG-sAS vs NFLG-sAS, as a function of time, according to the AS group. Bars represent 95% CI for estimate at each time point. Time 0 indicates the index echocardiogram. The percentages of patients with echocardiograms at the various time intervals are tabulated below the figure.
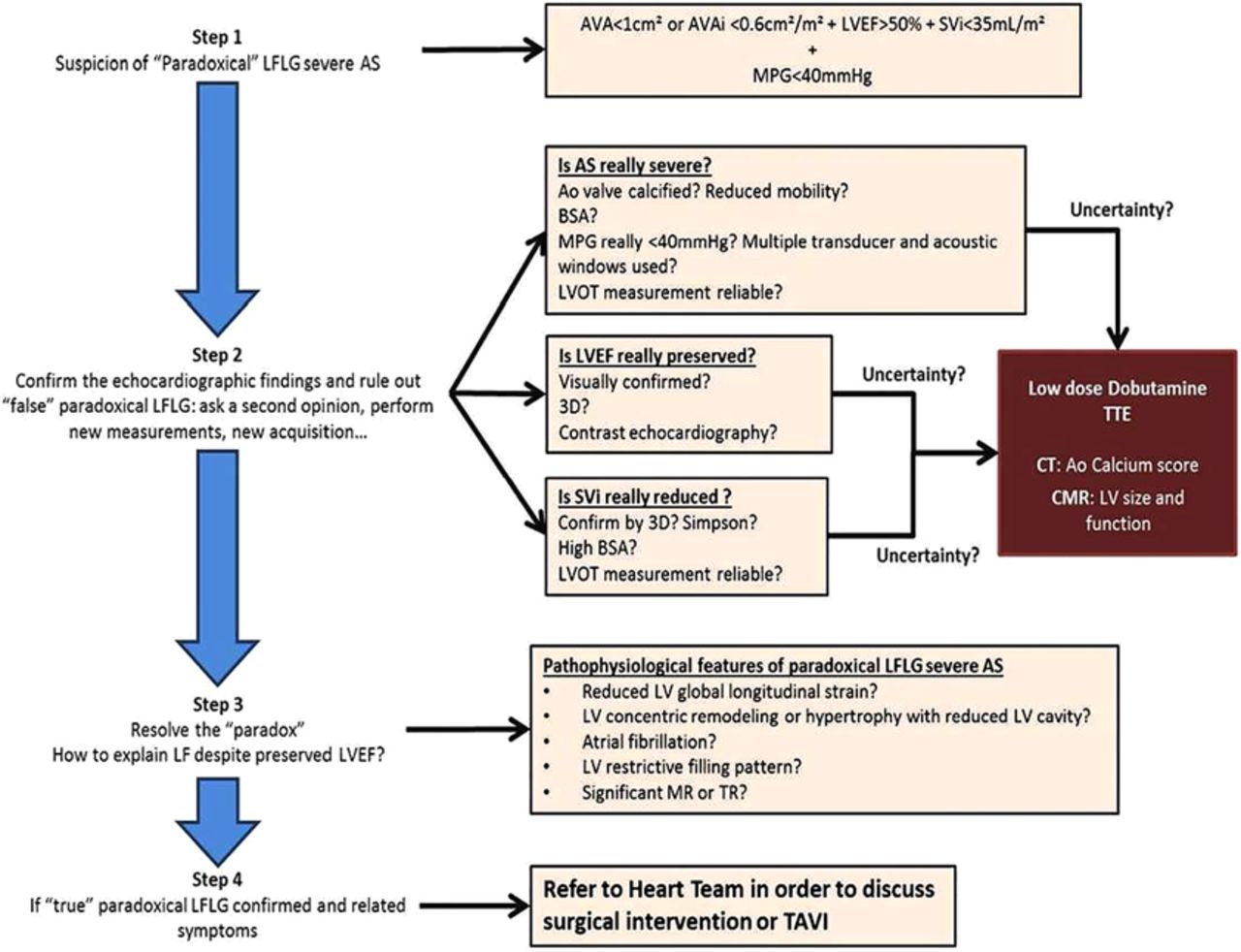
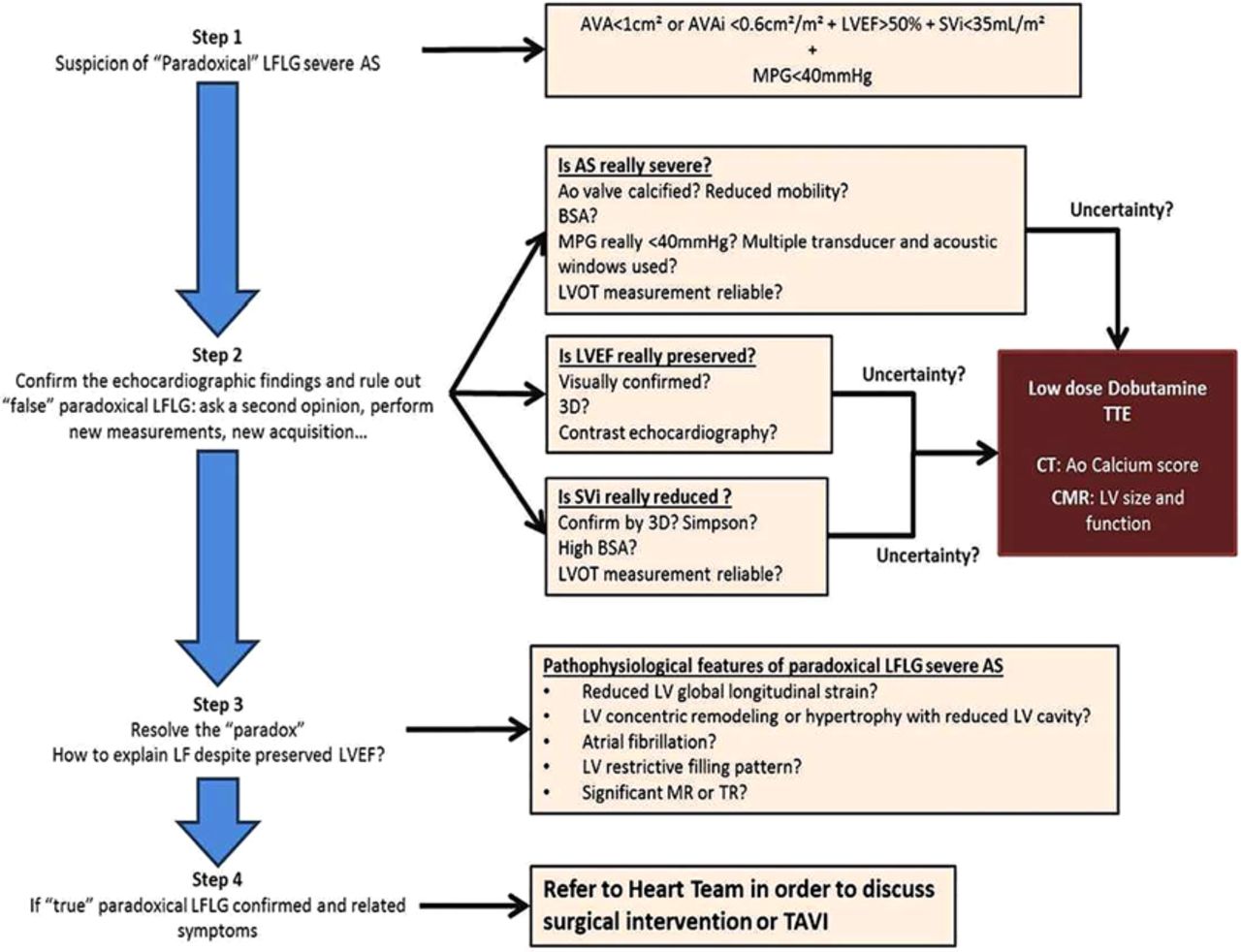
In the accompanying editorial, Drs Magne and Mohty refine the concept of LFLG severe AS with normal EF, often called “paradoxical” LFLG severe AS. They suggest that: “this study supports the concept that paradoxical LFLG is not necessarily a more advanced stage of the valvular disease (ie, stenosis severity) but rather a more advanced stage of the ventricular disease”. A practical clinical approach to these patients is summarized in figure 4.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Practical algorithm describing the daily clinical practice diagnosis of ‘true’ paradoxical low-flow, low-gradient (LFLG) severe aortic stenosis (AS). In the presence of echocardiographic findings suspecting (Step 1) the presence of paradoxical LFLG, all values should be meticulously confirmed and validated using alternative methodologies (Step 2) in order to address the three questions in boxes. In case of doubt or inconclusive echocardiographic results, other imaging modalities such as low dose dobutamine transthoracic echocardiography (TTE), CT with aortic valve calcium score assessment or cardiac magnetic resonance (CMR) may be used. When all findings are concordant, the apparent ‘paradox’ should be explained by concomitant pathophysiological features (Step 3). Ultimately, in case of obvious symptomatic ‘true’ paradoxical LFLG, we should refer to current practice guidelines and surgical intervention or transcatheter valve intervention (TAVI) should be discussed by the ‘Heart Team’. AVA, aortic valve area; AVAi, indexed aortic valve area; LVOT, LV outflow tract; MPG, mean pressure gradient; MR, mitral regurgitation; SVi, stroke volume index; TR, tricuspid regurgitation.
The Education in Heart article in this issue explains the concept of myocardial reperfusion injury and suggests that ischemic preconditioning has been neglected as potential therapy to protect against myocardial damage during cardiac surgery or with ST segment elevation myocardial infarction. (see page 1067) As with all Education in Heart articles, CPD/CME credits are available if you answer the accompanying multiple choice questions.
The Image Challenge case (see page 1031) in this issue shows a rare condition that was mistaken for a more common diagnosis, showing how imaging provided the definitive information needed for clinical management.
Linked Articles
- Editorial
- Image challenge
- Coronary artery disease
- Education in Heart
- Coronary artery disease
- Editorial
- Valvular heart disease