Article Text

Statistics from Altmetric.com
This issue of Heart includes an editorial from the British Cardiac Society proposing a cardiac catheterization patient safety checklist (see page 91). As Dr Cahill and colleagues note, the use of safety checklists in clinical practice “improves the reliability of a process and sets out an expected standard for practice. Perhaps more importantly, checklists modify team behaviour, bringing a focus to patient safety and communication and empowering junior members”. This checklist includes relevant patient data, pre-procedure checks, a team brief and post-procedure checks and allows content to be customized to local practice. The stand-alone and integrated versions of the checklist are available for download at http://www.bcs.com/checklist.
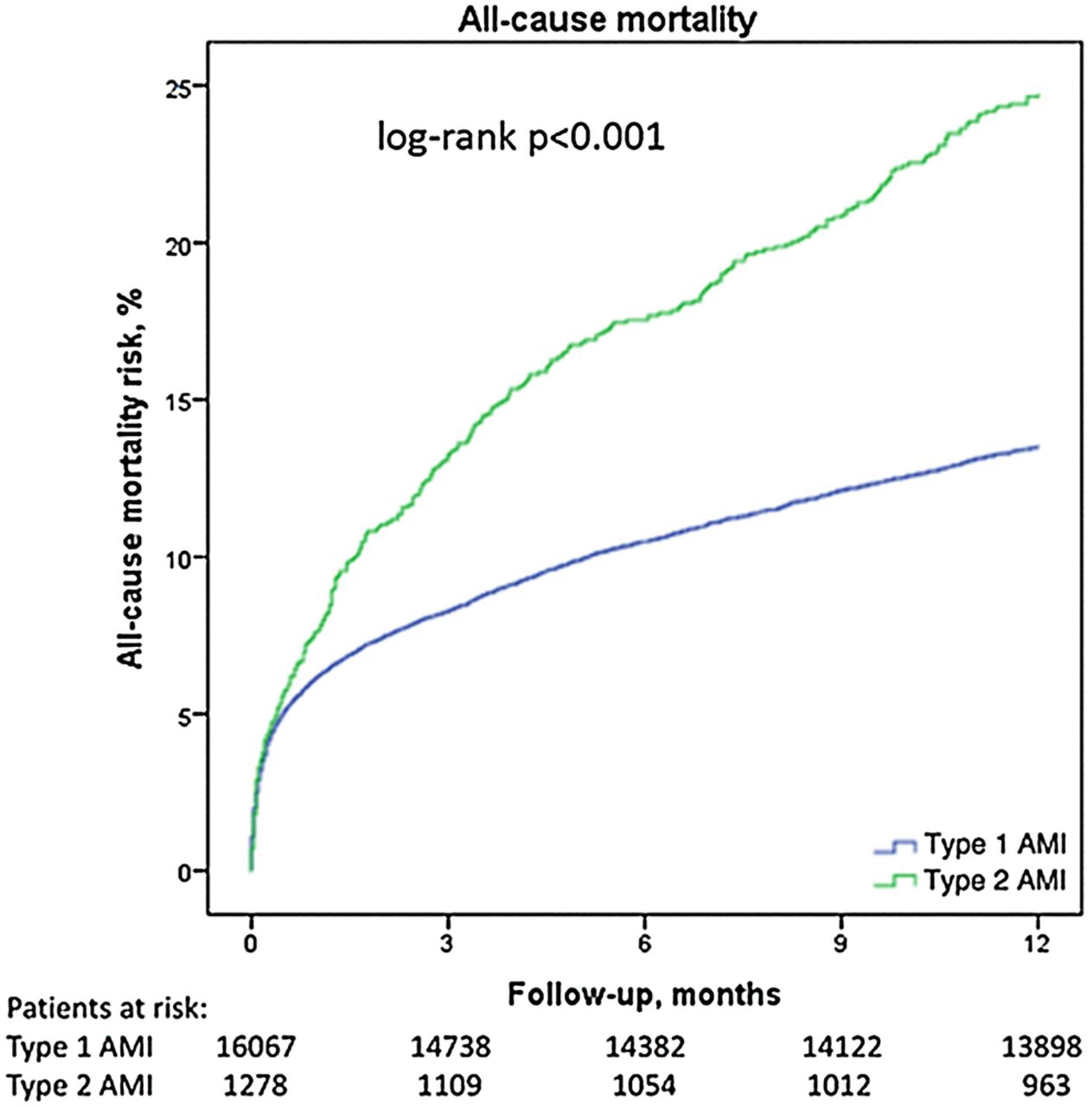
The clinical presentation and management of acute myocardial infarction (AMI) due an acute atherothrombotic occlusion of an epicardial coronary artery, defined as Type-1 myocardial infarction in the universal definition of myocardial infarction, has been addressed in numerous large clinical trials. Secondary (Type-2) AMI, defined as myocardial injury due to an acute imbalance in myocardial oxygen supply and demand, has been less well studied. In this issue of Heart, Dr. Tomasz Baron and colleagues (see page 101) found that Type-2 AMI accounted for 7.1% of myocardial infarctions in a registry of over 20,000 AMI patients in Sweden. In general, Type-2 AMI patients were older, more often female and had more comorbidities, including renal impairment and anemia. Although crude mortality at 1-year was higher in Type-2 compared to Type-1 AMI, there was no significant difference in outcome when adjusted for baseline clinical characteristics and treatment, suggesting that adverse outcomes in Type-2 AMI patients are related to their noncardiac conditions, with the elevated serum troponin simply being a marker of increased risk (figure 1).
In the accompanying editorial, Dr. Paul Collinson (see page 89) points out that diagnosis of Type-2 AMI is somewhat subjective with etiologies of oxygen supply-demand imbalance that include coronary endothelial dysfunction, embolism or spasm, as well as tachy/bradyarrhythmias, anemia, hypertension, and respiratory failure. In contrast to the current registry report, a previous single center study found that Type-2 AMI accounted for almost ¼ of AMI patients and was a predictor of adverse outcomes, even after correction for other clinical factors. These contradictory findings suggest that further research is needed into the causes and treatment of troponin elevations in conditions other than Type-1 AMI.
In patients undergoing cardiac surgery, pre-operative anemia is a predictor of adverse outcomes including increased length of stay, renal failure and mortality. Anemia may be due to depletion of whole body iron stores (absolute iron deficiency) or due to restricted availability of iron for erythrocytosis (functional iron deficiency), which is related to hepcidin levels, a protein that controls the absorption and distribution of iron. In a prospective study of 200 anemic surgical patients, Dr. Hung and colleagues (see page 107) found that although functional iron deficiency was the most common cause of anemia, hepcidin level was the only hematologic variable predictive of clinical outcome.
In putting this novel finding into perspective, Prof. Gavin Murphy (see page 87) notes that there is wide variation in the preoperative assessment and treatment of anemia, despite the high prevalence of this condition (about ½ of cardiac surgical patients) and known association with adverse outcomes. The current study raises the question whether preoperative treatment of functional iron deficiency with intravenous iron might provide clinical benefit, a concern that should be addressed in future clinical trials. If the relationship between elevated hepcidin levels and outcomes is validated in other studies, this biomarker might help identify patients at higher risk, although how this might influence clinical management is not yet clear.

Crude cumulative risk of death (Kaplan–Meier) in patients with type 1 and type 2 acute myocardial infarction (AMI).
{kind=link}
{kind=link}
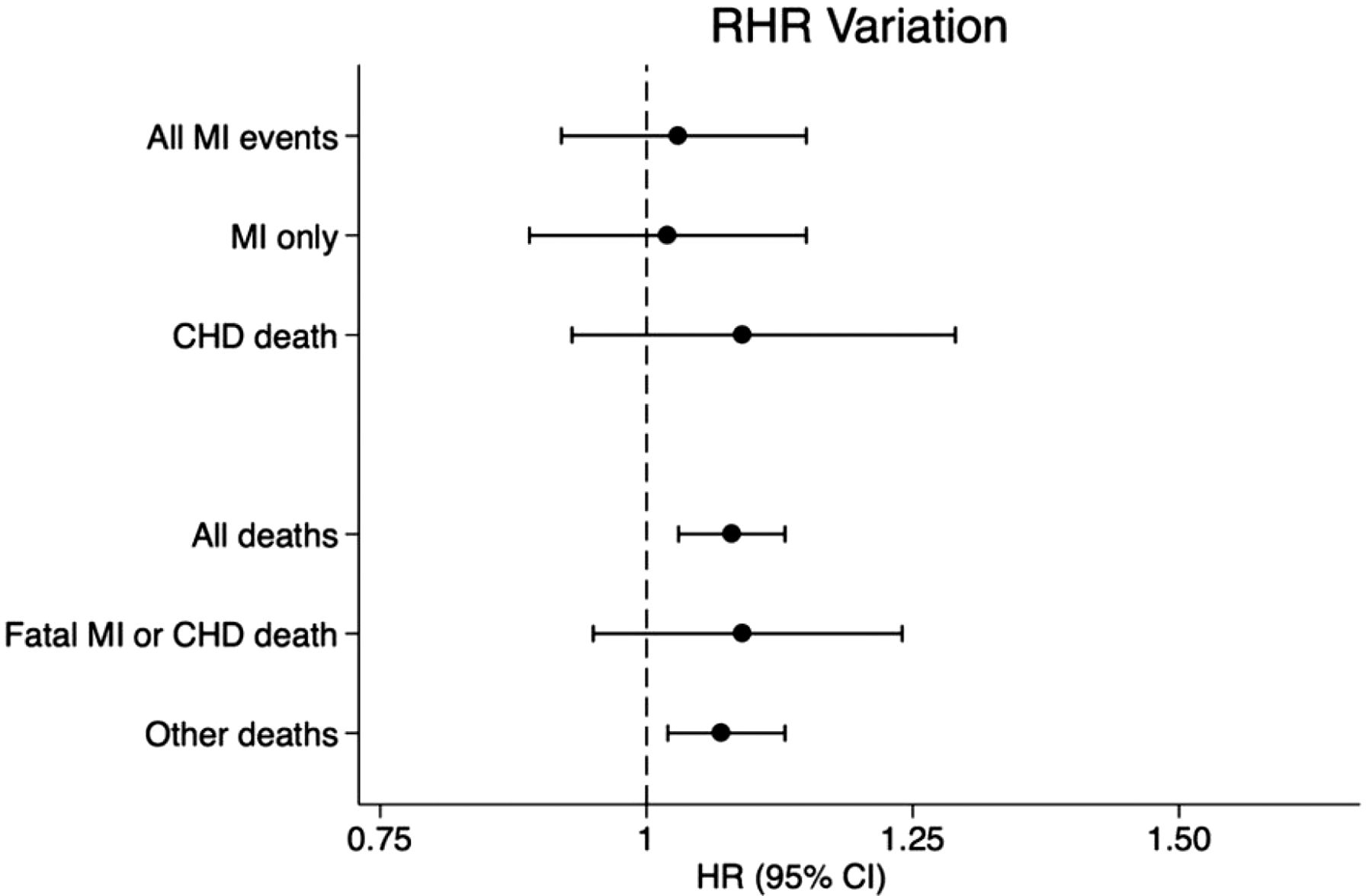
Forest plots of hazard rations for resting heart rate variation associations with outcomes. RHR, resting heart rate; CHD, coronary heart disease; MI, myocardial infarction.
Another interesting study in this issue of Heart, by Dr. James Floyd (see page 132) and colleagues examined the relationship between variation in resting heart rate at each of 5 annual visits and health outcomes in 1991 patients with no cardiovascular disease at study entry. Resting heart rate is an established predictor of myocardial infarction and mortality; this study took the next step to see if variation in resting heart rate over several years is an even better predictor of long-term outcomes (figure 2).
The authors conclude: “In this prospective cohort study of older adults free of cardiovascular disease, we found that the mean and long-term variation in resting heart rate, but not the trend, were associated with the risk of death”. If these findings are replicated in other populations, it may be helpful to integrate the simple measurement of resting heart rate at each annual visit into standard approaches to risk assessment.
The Education in Heart articles in this issue address quantification of mitral regurgitation by echocardiography (see page 146) and infarct size reduction in acute myocardial infarction (see page 155). Remember that you can earn CPD/CME credits for reading these articles and completing the BMJ Learning module.
The Image Challenge (see page 161) case asks you recognize the diagnosis on a CT image in a middle-aged man with progressive breathlessness and choose the next step in management of this patient.
We hope you find this issue of Heart informative and interesting. We encourage you to interact with authors by sending an e-letter or using social media to discuss articles with controversial or novel findings. Heart also now encourages authors to submit video abstracts to provide further information about their original research study. These videos can be found on the Heart website by clicking on the icon in the social media box.
Linked Articles
- Editorial
- Education in Heart
- Editorial
- Cardiac risk factors and prevention
- Coronary artery disease
- PostScript
- Editorial
- Education in Heart
- Coronary artery disease