Article Text

Statistics from Altmetric.com
In heart failure patients with an indication for cardiac resynchronization therapy (CRT) or an implantable cardiac defibrillator (ICD), it remains a difficult clinical decision to choose the optimal device in an individual patient, many of whom do not match the clinical characteristics of patient groups studied in randomized clinical trials. To evaluate the effects of age and comorbidities on the relative effectiveness of different types of implanted electric cardiac devices, Wood and colleagues (see page 1800) performed a meta-analysis, including almost 13,000 patients, comparing the survival benefit of CRT alone, ICD alone, CRT with a pacer (CRT-P) or CRT with a defibrillator (CRT-D). The patients included in these trials had a mean age of 62–65 years, mean left ventricular ejection fraction of 23%, NYHA functional was class II or III in 85–90%, and ischemic disease was present in about 50%. Compared to medical therapy, CRT-D had the greatest effect on mortality with a relative reduction of 42%, compared to 29% with ICD and 28% with CRT-P on unadjusted analysis. In the final adjusted model, the strongest predictors of benefit were QRS duration, left bundle branch block (LBBB) morphology, age and gender.
The main results of this meta-analysis are summarized in a elegant figure by Kramer and colleagues (see page 1773) which shows the interaction of gender, age, QRS duration and the presence on LBBB on the comparable effective of these 3 types of implanted cardiac devices (figure 1).

Estimated HRs and 95% CIs for each treatment (row) versus each contrast treatment (column). The subgroups on each panel''s x axis are defined by gender, age (<60 years, 60+ years), QRS duration (<120 ms, 120–149 ms, 150+ ms) and LBBB (Y=yes, N=no). The colours indicate results from two different samples: the full sample and the reduced sample that omits patients with QRS <120 ms and NYHA class I. This figure reproduces the main results from table 2 and the sensitivity results from table S5 of the Woods et al article. CRT-D, cardiac resynchronisation therapy-defibrillator; CRT-P, CRT-pacemaker; ICD, implantable cardioverter defibrillator; LBBB, left bundle branch block; MT, medical therapy; NYHA, New York Heart Association.
As these authors note: “The greatest reduction in mortality [with CRT-D] was seen in women ≥60 years old with QRS duration ≥150 ms and LBBB”. In contrast, men and patients<60 years of age benefited more from ICD. Although this large meta-analysis provides robust evidence for clinical decision-making, limitations of the data include a relatively short followup interval (averaging 2.5 years), absence of data on atrial fibrillation and chronic kidney disease, and advances in device programming algorithms over the publication window of these studies. Wood and colleagues conclude: “Ultimately, however, given the heterogeneity of effect across patient groups and the extraordinary costs of these therapies, the real test of progress in this field will be whether clinicians can move towards these more elusive, but essential, estimates of what this device will mean for this patient at this time”.
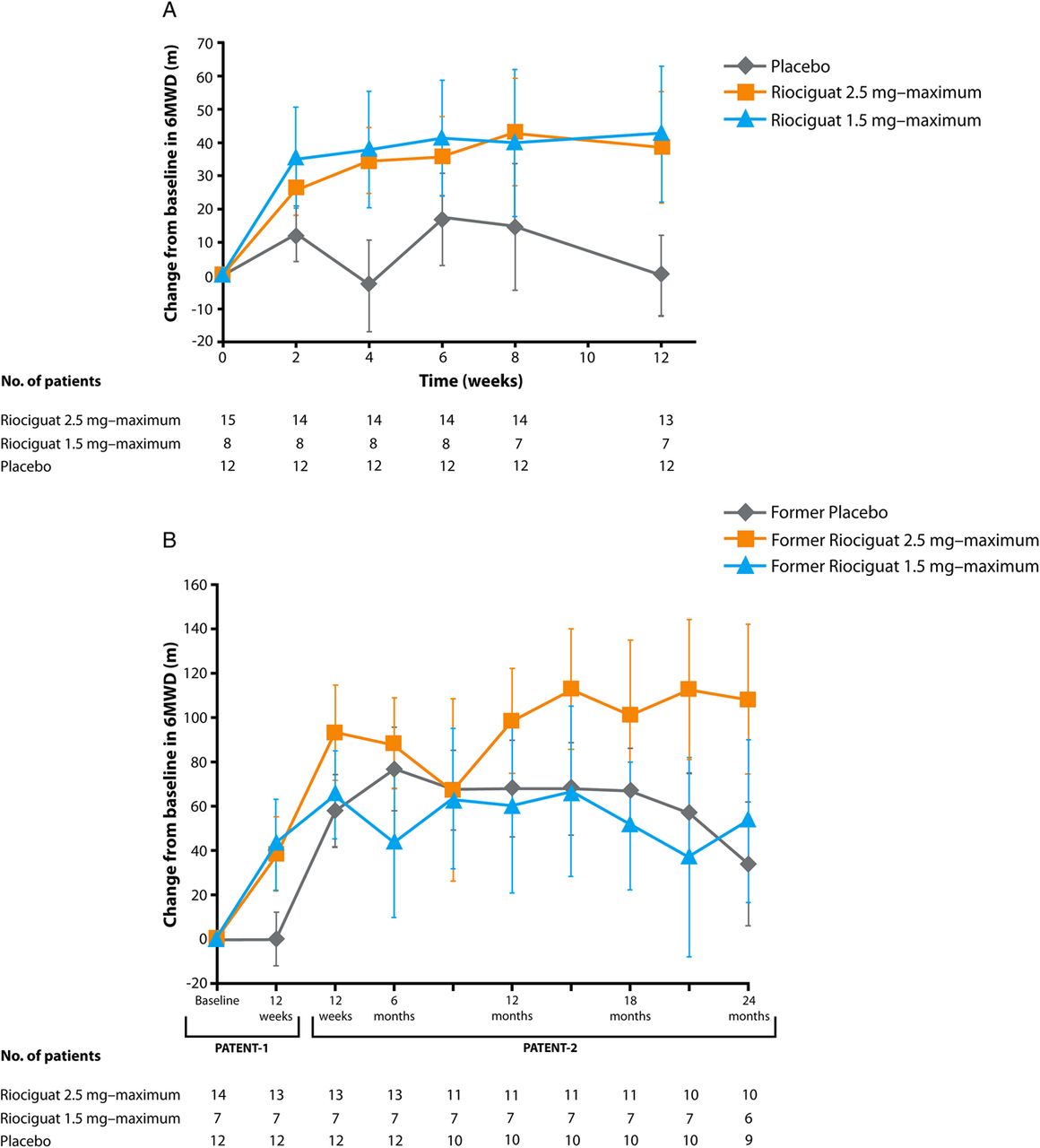
Pulmonary arterial hypertension (PAH) often complicates management of adults with congenital heart disease. Riociguat, a novel pulmonary vasodilator, increases cGMP production both by stabilizing nitric oxide-soluble guanylate cyclase (sGC) binding and by direct sGC stimulation via a non-nitric oxide dependent pathway. The Pulmonary Arterial hyperTENsion sGC-stimulator Trial-1 (PATENT-1) and PATENT-2 studies demonstrated that riociguat was well tolerated with a sustained improvement in exercise capacity and functional class in adult patients with PAH related to various underlying cardiac conditions. In this issue of Heart, Rosenkranz and colleagues direct our attention to PAH in adults with congenital heart disease (CHD) (see page 1792). In this exploratory post-hoc analysis, the beneficial effects and tolerability of riociguat were confirmed in this small subgroup of 35 patients with persistent or recurrent PAH after complete repair of CHD (figure 2).

Change from baseline in 6-min walking distance (6MWD) in the subgroup of patients with pulmonary arterial hypertension associated with congenital heart disease in Pulmonary Arterial hyperTENsion sGC-stimulator Trial-1 (PATENT-1; A) and PATENT-2 (B). Data are observed values (mean±SEM).
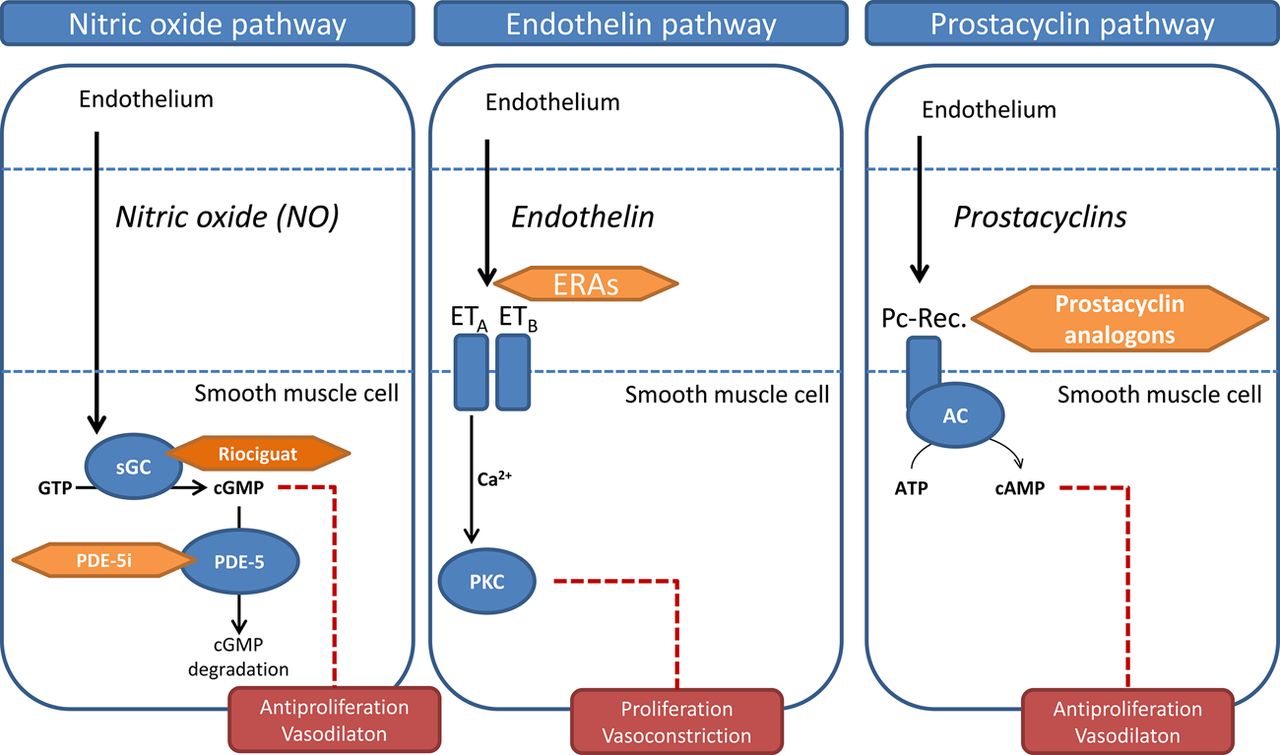
In the accompanying editorial, Lammers and Diller (see page 1771) emphasize the importance of treating PAH in adult patients with CHD to improve longevity and quality of life. The three pathophysiologic pathways currently targeted by medical therapy for PAH are compared (figure 3) and the potential value of riociguat in adult patients with CHD is discussed. However, they also caution: “Further studies of riociguat using state-of-the-art morbidity and mortality endpoints in CHD-PAH and in the setting of Eisenmenger syndrome are, however, desirable to further improve outcome and prognosis in this challenging group”.

{kind=link}
{kind=link}
{kind=link}
Main mediator pathways amenable to current standard therapy in pulmonary hypertension. AC, adenylate cyclase; cAMP, cyclic AMP; cGMP, cyclic guanylate monophosphate; GTP, guanylate triphosphate; ERA, endothelin receptor antagonists; ET, endothelin; PC-Rec, prostacyclin receptor; PDE-5i, phosphodiesterase 5-inhibitor; PKC, protein kinase C; sGC, soluble guanylate cyclase.
An interesting association between persistent left ventricular (LV) hypertrophy and an increased risk of allograft failure in kidney transplant recipients in reported in a study from Korea of 3373 kidney transplant recipients who underwent echocardiography before and after kidney transplantation (see page 1826). The pathophysiologic mechanism for this association between persistent LV hypertrophy and allograft failure deserves further study (see page 1776). It is possible that pre-transplant cardiac dysfunction with myocardial fibrosis and reduced longitudinal shortening results in persistent abnormal cardiac function after renal transplantation, which might affect renal blood flow. Other possible explanations include post-transplant hypertension or common comorbidities, such as diabetes and anemia that might lead to both persistent LV hypertrophy and allograft failure. However, even if we do not understand the mechanism of this association, it may be prudent to monitor cardiac function and LV hypertrophy after renal transplantation, in addition to optimizing medical therapy for control of blood pressure.
The Eduction in Heart article in this issue focuses on tricuspid valve disease (see page 1840) with the educational objective covering an understanding of the pathophysiology, role of diagnostic imaging and indications for intervention for this often-neglected form of valvular heart disease.
The Image Challenge question (see page 1785) asks you to predict the physical examination findings based on the Doppler echocardiographic findings in a 32 year old women with a dyspnea and a history of cancer. Learn about the value of tissue Doppler velocities in fine tuning your differential diagnosis.
Linked Articles
- Image challenge
- Special populations
- Editorial
- Heart failure and cardiomyopathies
- Editorial
- Editorial
- Education in Heart
- Pulmonary vascular disease