Article Text

Statistics from Altmetric.com
Almost everyone likes drinking coffee! Thus, data suggesting that coffee might actually be good for us is always greeted with enthusiasm—the study by Dr Yosoo Chang and colleagues (see page 686) in this issue of Heart has the highest Altmetric score of any paper we have published, reflecting everyone's interest in this topic. In this cross-sectional study, over 25 thousand young and middle aged asymptomatic healthy men and women provided food frequency data using a validated questionnaire and also underwent health screening and computed tomographic measurement of coronary artery calcium (CAC). When adjusted for potential confounders, moderate coffee consumption (3 to 4 cups a day) was associated with a lower prevalence of detectable CAC as shown in figure 1. Although CAC is only a surrogate for coronary disease, it does allow detection of very early subclinical disease, making is useful for population based association studies, as reported here. Despite disparate data on the effects of coffee consumption on cardiovascular disease (CV) disease risk in the past, the findings in the current study are congruent with a recent meta-analysis. In addition, this association is biologically plausible based on improved endothelial function, a reduced risk of diabetes, improved insulin sensitivity, and possible prevention of low-density lipoprotein oxidation with chronic coffee consumption. On the other hand, this is a cross-sectional association study so we cannot ascertain whether or not there is a cause-effect relationship between coffee consumption and CAC. Most importantly, this study did not include outcome data and we do not know if a lower CAC score will translate into actual health benefit. Hopefully, this research group will provide CV outcomes data for this cohort at some future date. In the meanwhile, I (for one) will keep drinking coffee.

Odds ratio of detectable coronary artery calcium scores (CAC score >0) by coffee consumption. The curves represent the adjusted OR of detectable CAC scores (>0 Agatston unit) and coffee consumption. The dose response association of coffee consumption was estimated by using a linear and a quadratic term for coffee consumption in the multivariable logistic regression. The model adjusted for age, sex, centre, and year of screening examination, education level (high school graduate or less, community college or university graduate, graduate school or higher, and unknown), physical activity level (inactive, minimally active, health enhancing physically active, and unknown), smoking status (never, former, and current), body mass index (kg/m2), parental history of coronary heart disease (yes vs no), alcohol consumption (none, <5, 5–<20, ≥20 g/day, and unknown), total energy consumption (kcal/day), and consumption of fruits, vegetables, and red and processed meats (quartiles, g/day). A similar trend was observed in robust Tobit regression models of CAC ratios.
In adults with prior closure of an atrial septal defect (ASD) there often is a long-term concern for risk of atrial fibrillation (AF) and stroke. Indeed, in a study of 1168 Danish patients with ASD closure as an adult and a median follow-up of 9.6 years, Dr Camilla Nyboe and colleagues (see page 706) found new AF in 11% of patients with a closed ASD compared to 2% of control subjects, for an adjusted hazard ratio of 8.2 (95% CI 6.6 to 10.2). There was no difference between transcatheter and surgical ASD closure. Importantly, the risk of stroke was similar in ASD patients with or without closure and the use of medications for anticoagulation or control of AF was not reduced after ASD closure (figure 2).

Proportion of patients with atrial septal defect with closure and prevalent atrial fibrillation using anticoagulation medicine and antiarrhythmic medicine per 100 patient-years from 5 years before closure to 5 years after closure.
The data in this paper raise several important issues. Over the past 55 years, the authors document a dramatic increase in the number of ASD closures in the Danish population and in the age at which closure is performed. However, these changes are not paralleled by any evidence of improved outcomes or a reduced need for anticoagulation for AF. As Dr Sing-Chien Yap comments (see page 661) “The main message of their analysis is that despite closure, individuals with ASD remain vulnerable to AF and stroke. This has several important clinical implications. This specific patient population may warrant regular follow-up after closure for early detection and management of AF. To reduce the thromboembolic risk, patients with AF should receive oral anticoagulation. As the access to the left atrium is restricted after ASD device closure, patients with paroxysmal or persistent AF may be considered for left-sided catheter ablation before closure. In patients with pre-existing AF undergoing surgery, maze procedure should be performed. Finally, ASD closure in adults using current indications does not seem to prevent or reduce late AT after closure. Early recognition and repair of an ASD is important to restore haemodynamic abnormalities as soon as possible, maintain sinus rhythm and prevent paradoxical embolism.”
What does allopurinol and prevention of gout have to do with CV disease? It turns out that the inhibition of xanthine oxidase by allopurinol reduces generation of superoxide anions and other oxidative free radicals and, in theory, might reduce oxidative stress in a clinically meaningful way. In a population-based case-control study of 18,325 controls and 3171 cases of non-fatal myocardial infarction, treatment with allopurinol was associated with about a 50% lower risk of myocardial infarction, predominantly in men, dependent on both dose and duration of treatment (see page 679) (table 1).
Risk of non-fatal acute myocardial infarction associated with allopurinol
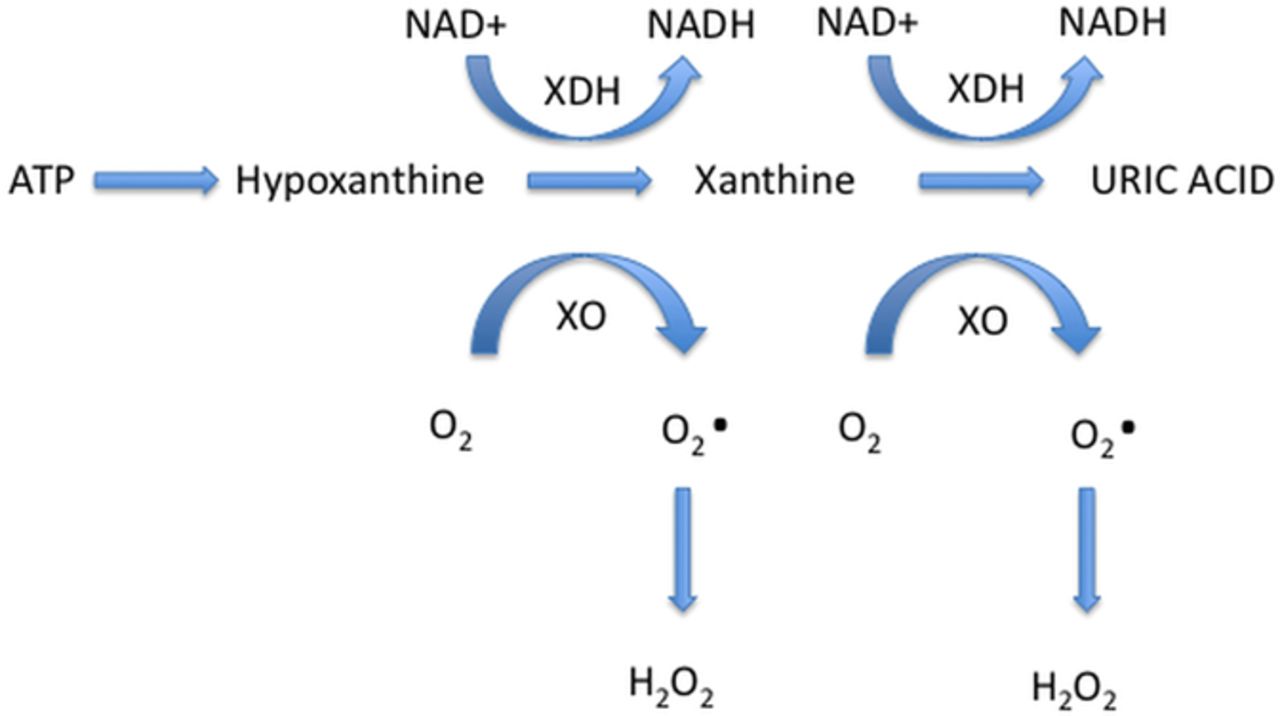
In the accompanying editorial Prof Pascal Richette (see page 659) illustrates the relevant molecular pathways (figure 3) and discusses other potential mechanisms linking gout and cardiovascular (CV) disease such as direct effects on endothelial function, low-grade inflammation, and regulation of signaling pathways in vascular smooth muscle cells. He also notes that patients with gout often have comorbidities that put them at higher risk of cardiovascular (CV) disease, including hypertension, diabetes and obesity.
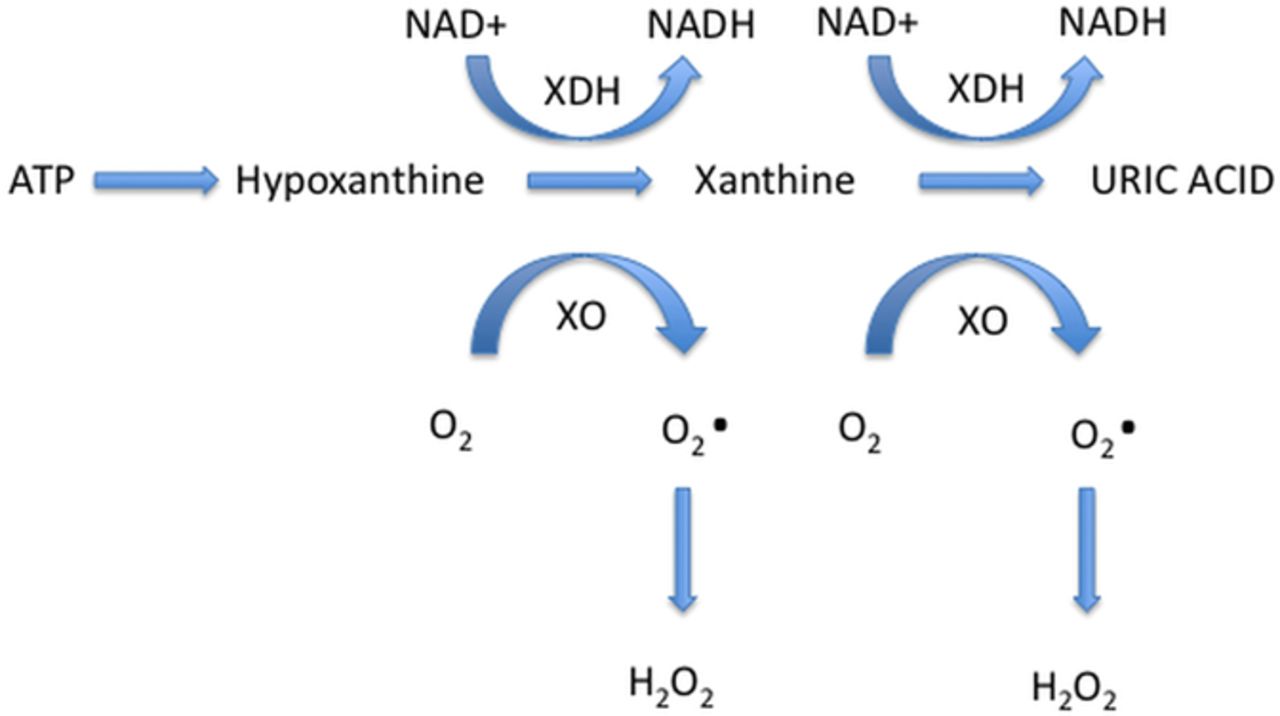
Xanthine oxidoreductase exists in two interconvertible forms: xanthine dehydrogenase (XDH), the constitutive form and xanthine oxidase (XO), the oxidised form, which uses oxygen as the terminal electron acceptor. NAD, nicotinamide adenine dinucleotide; NADH, nicotinamide adenine dinucleotide -hydrogen.
Prof. Richette concludes: “The mechanisms whereby gout and increased serum uric acid levels can lead to CV events are presumably multifactorial, implicating a low-grade inflammatory state, XO activity and the deleterious impact of hyperuricaemia itself.”
The Education in Heart article (see page 727) in this issue discusses how to assess aortic annular size before transcatheter aortic valve implantation (TAVI). This practical and informative discussion will be helpful for all clinicians to understand the anatomic issues that affect the choice of type and size valve and whether this procedure is even possible in an individual patient (figure 4). Although a simple annular diameter is adequate for Doppler calculation of aortic valve area, more complex descriptors of the elliptical annulus are needed before TAVI, including 3D echocardiographic or computed tomographic measurements of annular area and perimeter, to ensure correct valve sizing and decrease the likelihood of paravalvular regurgitation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Model of the coronet shaped aortic valve annulus. (B) Diagram of the aortic valve complex illustrating relevant measurements made by 3D imaging modalities. LMS, left main stem; LVOT, left ventricular outflow tract.
The Image Challenge this week (see page 719) shows a 2D and 3D echocardiographic image of the aortic valve in a 59-year-old woman who presented with a cerebrovascular event. This case nicely illustrates the art of differential diagnosis in interpretation of imaging studies.
Linked Articles
- Editorial
- Arrhythmias and sudden death
- Editorial
- Congenital heart disease
- Coronary artery disease
- Coronary artery disease
- Education in Heart